
Abstract
Five factors (gender, handedness, some aspects of general health, family history, and intelligence) that could assist speech–language pathologists in identification of children who stutter (CWS) in 42 CWS and 34 fluent control children (children who do not stutter [CWNS]) were investigated. The data reported here were obtained from assessments made within 1 year of the reported onset of stuttering. The results from the initial assessments showed significant differences between CWS and CWNS on the five factors considered. Although there were some differences on intelligence scores, it is emphasized that the scores of all CWS were within normal limits, and in fact, both groups scored higher than the population average. These factors are important for the initial assessment of stuttering and may be useful for establishing what intervention is appropriate.
Introduction
Previous work has shown that stuttering usually begins in early childhood and that onset occurs most often between 2 and 5 years, with 90% of cases of stuttering starting before 5 years of age (Andrews & Harris, 1964; Howell, Davis & Williams, 2008; Johnson et al., 1959; Månsson, 2000; Yairi & Ambrose, 2005). Stuttering is a relatively common disorder in childhood with an incidence of around 5% in the pre-school population (Månsson, 2000; Yairi & Ambrose, 2005), although a more recent study has put the rate higher than this at around 9% (Reilly et al., 2009).
The chance of spontaneous recovery is considered to be high for cases that were diagnosed during childhood: Thus, longitudinal studies have reported recovery rates of 65% in the age range 2 to 5 years 10 months (Ryan, 2001), 74% in the age range 2 to 4 years 11 months (Yairi & Ambrose, 1999), and 79% in the age range 2 to 16 years (Andrews & Harris, 1964). Recovery after teenage is rare (Andrews & Harris, 1964). Based on these recovery statistics, at least 20% of children who begin to stutter will persist. One fifth of the 5% of cases in the pre-school population corresponds with the figure of 1% who stutter in the adult population (Bloodstein, 1995).
The difficulty experienced by speech–language pathologists in the identification of stuttering is highlighted in a wide-ranging survey by Ham (1990). He found people could not agree on a definition or description of stuttering. Clinically, a definition of stuttering is also considered difficult and, often, the simplest option is to describe the overt symptoms (Starkweather, 1987). The World Health Organisation (1992; International Statistical Classification of Diseases and Related Health Problems, 10th Revision [ICD-10]) did attempt a definition based on symptoms. They classified stuttering as
speech that is characterized by frequent repetition or prolongation of sounds or syllables or words, or by frequent hesitations or pauses that disrupt the rhythmic flow of speech. It should be classified as a disorder only if its severity is such as to markedly disturb the fluency of speech. World Health Organisation ICD-10 F98.5
Van Riper (1982) provided an inventory of the core behaviors of stuttering, which comprised a list of different types of speech symptoms (repetitions, prolongations, blocks), as well as escape and avoidance behaviors. All the items on Van Riper’s inventory were speech related, as were those on Cooper and Cooper’s (1985) Chronicity Checklist and Wingate’s (1964) widely cited multipart definition. Some definitions of stuttering give lists of symptoms that are subgrouped into core and secondary behaviors. The core behaviors are usually a list of speech symptoms and the secondary behaviors contain items such as feelings and emotions (Shames & Florence, 1980). The U.K.’s Royal College of Speech Language Therapists (RCSLT) advise that “published scales or questionnaires should be used to evaluate the child’s perceptions, attitudes and sequelae of stammering” (Taylor-Goh, 2005 p. 75), but in reality, this can be very difficult in young children. Obtaining estimates of secondary behaviors from young children is a time-consuming and subjective process and this may account for the reticence to include them into definitions of stuttering for assessment used with clinical referrals. It is evident from this brief and selective review that the majority of definitions of stuttering that are available in the research and clinical literature focus on overt speech symptoms. Simply listing symptoms relating to speech performance as a method of identifying stuttering in children is problematic due to the cyclical nature of the disorder, and the fact that many children go through a transient period of normal non-fluency (Bloodstein, 1970; Kadi-Hanifi & Howell, 1992) where they tend to repeat whole words effortlessly.
This overlap between normal non-fluency and stuttering makes definition based on speech symptoms difficult. As a consequence of this difficulty, identification and diagnosis also become problematic—a condition cannot be identified or diagnosed if it cannot be defined. Consequently, the current research set out to establish which factors may aid a speech–language pathologist’s clinical assessment of those factors that may influence the persistence of dysfluency as opposed to normal, transient non-fluency at initial assessment, which is the time when it may be most difficult to distinguish the overt symptoms of stuttering from normal non-fluency. Speech–language pathologists often report difficulty in obtaining viable speech samples from young children in clinic, so other indicators could be useful in aiding a diagnosis of stuttering.
The data from the assessments reported here describe the differences between a group of children identified as stuttering (CWS) and a control group of children (CWNS) who had been confirmed by a speech–language pathologist as not stuttering. This comparison was carried out to (a) establish whether the factors measured differentiated between the groups and (b) that if they do differ, they will be used to investigate persistence and recovery from stuttering in a follow-up study. Five factors were chosen based on previous research that indicated differences between CWS and CWNS. The factors were (a) gender, (b) handedness, (c) health, (d) family history of stuttering, and (e) intelligence. A brief review of the literature that supports the selection of each of these factors is given below:
Gender
Research studies report consistently that stuttering affects boys more often than it does girls. Reported male/female ratios in early childhood range from 1.6:1 (Kloth, Janssen, Kraaimaat, & Brutten, 1995; Månsson, 2000) to 2:1 (Yairi & Ambrose 1992) in children aged 2 to 5 years. In older children, the ratio reported is higher still at around 5.3:1 (Howell et al., 2008) and 4:1 (Bloodstein, 1995). The increase in the gender ratio with age may be attributable to a higher recovery rate among girls than boys (Ambrose, Cox, & Yairi, 1997). Yairi and Ambrose (1992) reported boys started to stutter 5 months later than girls (which was statistically significant). Månsson (2000) reported that the difference in age at onset for the two genders was lower (M age at onset was 34 months for boys and 31 months for girls).
Handedness
One reason for ascertaining handedness is that it can be useful in indicating atypical cerebral laterality, which has been hypothesized as being linked to stuttering. In the population at large, 90% are right-handed and 10% are left-handed (McManus, 2002). Earlier research found that CWS were similar to the general population in terms of handedness (Andrews & Harris, 1964; Foundas, 2003; Johnson et al., 1959). Howell and Davis (2011) reported that 19% of their sample was left-handed, which was significantly higher than that expected in the general population (McManus, 2002). To date, there has been little recording of handedness near to the age of onset of stuttering, which is the time when hand preferences are being established.
General Health
Health factors in relation to stuttering are not well documented in the literature although they often form part of a clinician’s case-history taking. One study by Rustin and Purser (1991) reviewed 209 case histories taken from parents attending a specialist clinic for developmental stuttering. The study reported that 11% of the children had been diagnosed as asthmatic, and one third of the boys and one fifth of the girls were reported as having significant sleep problems relative to their siblings. These figures are comparable with those of the general population with 8% of girls and 10% of boys in the United Kingdom being diagnosed as asthmatic (Soriano, Kiri, Maier, & Strachan, 2003), and incidences of sleep disorders in children are around 20% (Dahl, 1996; Mindell, Owens, & Carskadon, 1999). The Rustin and Purser review also reported that 50% of boys and 29% of girls had been admitted to hospital as in-patients. This compares with 7% to 10% of all children in the United Kingdom who are admitted as in-patients to hospital (National Health Service UK, 2011). However, all the children were referred to the clinic by other speech–language pathologist so there may have been a tendency for them to be more complex cases. This is supported by the observation that reported birth and medical issues are not linked to stuttering (Andrews & Harris, 1964).
A correlation between head injury and the onset of stuttering has been reported in two studies. Segalowitz and Brown (1991) administered a self-report questionnaire to 616 high school students. Nine of the respondents (6 boys and 3 girls) reported that they had a diagnosis of stuttering and 8 of these reported closed head injury. This was the case for all 6 boys, each of whom also reported loss of consciousness due to the insult. No such association was found with other speech and language impairments, but there was a strong correlation between head injury and hyperactivity, mixed handedness, and dislike of mathematics. In a later study by Alm and Risberg (2007), 17 out of 32 people who stuttered reported pre-onset events that might be associated with neurological lesions. These were mostly perinatal complications and head injury.
Family History
It is known that stuttering is highly heritable. In studies on reported family incidence of stuttering, figures for stuttering in first-degree relatives (parents or siblings) are around 50% (Buck, Lees, & Cook, 2002; Riaz et al., 2005; Yairi & Ambrose, 1992) rising to 60% to 70% when second- and third-degree relatives are included (Månsson, 2000, Yairi & Ambrose, 2005). This is significantly higher than the incidence of stuttering reported in families of normally fluent controls. It should be noted, however, that reports of stuttering in families tend to increase once stuttering has been identified (Reilly et al., 2009). Twin studies suggest more about how a disorder might be passed on through family members (either by genetics or environmental influences). These types of studies have shown that stuttering is more prevalent in twins whose DNA is identical (monozygotic) than dizygotic twins who only share 50% of their DNA (Andrews, Morris-Yates, Howie, & Martin, 1991; Felsenfield et al., 2000; Howie, 1981), confirming that a large part of stuttering inheritance is due to genetics.
In recent years, the genetic basis of stuttering has been explored using more modern approaches such as linkage analysis and association studies. These approaches have revealed potential genes that are implicated in the inheritance of stuttering. Kraft and Yairi’s (2012) summary of the recent developments in the genetics of stuttering acknowledges the importance of genetics as an alternative to the “top-down” approach to diagnosis of stuttering. However, the summary also acknowledges the role of environmental factors in stuttering successful treatment implies some malleability in behavior.
For the purpose of the current study, family history was chosen as a key factor to be considered in identifying stuttering. The only viable way a clinician can collect information about family history is through a questionnaire asking parents to report all known incidences of stuttering in first- and second-degree relatives. This was therefore the method chosen in the current study.
Intelligence
Models of stuttering often incorporate cognitive elements (e.g., De Nil, 1999; Smith & Kelly, 1997; Starkweather, Gottwald, & Halfond, 1990), yet broad testing of intelligence has not been investigated in groups of young CWS. Intelligence was included as a potential factor to investigate as older research found that school-aged CWS scored lower on IQ tests than those who did not stutter in both the verbal and non-verbal components of the intelligence tests (Andrews & Harris, 1964; Johnson, 1955; Okasha, Bishry, Kamel, & Moustafa, 1974). Although IQ testing has not been carried out on young CWS, there is a body of research on children with specific and non-specific language impairment that has shown these children have deficits in area of cognitive ability apart from language (e.g., Rice, Tomblin, Hoffman, Richman, & Marquis, 2004). It is also known that there is a higher incidence of fluency disorders in adults with significant learning difficulties (Stansfield, 1990). Young children presenting with deficits in cognitive development may therefore be more at risk of developing a stutter and as such, it is an area worthy of further investigation.
Method
Participants
Data were obtained from 42 CWS and 34 CWNS. The CWS were recruited through speech and language therapy departments, nurseries, and schools in Norfolk and Suffolk in the United Kingdom and through referrals by health visitors and general practitioners. Some CWS were also recruited from one of the author’s (S.C.) caseload and from advertisements placed on the British Stammering Association website (http://www.stammering.org/) and in local newspapers. The CWNS were recruited from nurseries and schools in the same geographical region. Five of the CWNS were relatives or friends of children in the CWS group. The selection criterion for inclusion in the CWS group was age 5 years or under at the time of first assessment and reporting no other developmental disorder. All children referred to the study spoke English as their first language so this was de facto a selection criterion (although it was not a requirement for inclusion). The children also had to meet the following criteria (based on those employed by Yairi & Ambrose, 1992) for stuttering at initial assessment:
Classified as stuttering by a qualified speech–language pathologist (S.C.), as well as by the child’s speech–language pathologist (if applicable)
Rated by parents at 2 or higher on a 10-point scale where 0 represented no stuttering and 9 represented very severe stuttering
Analysis of a 20-min speech sample indicated 3% or higher stuttered syllables (SS)
A score of 18 (moderate stuttering) or higher on the Stuttering Severity Instrument–Third Edition (SSI-3; Riley, 1994)
The criteria for inclusion in the CWNS group were as follows: (a) aged 5 years or under at the time of first assessment; (b) English was the first language (so as to match the CWS); (c) no other developmental disorders; and (d) no evidence of stuttering. Speech samples from the CWNS were checked to confirm that there was no evidence of blocks or prolongations and both part word and whole word repetitions were below 2% SS.
There were 27 boys and 15 girls in the CWS group. All the children were first assessed within 1 year of reported onset. The age range at first assessment was 2 years 6 months to 5 years 10 months with a mean age of 3 years 11 months and a standard deviation of 10 months. The parent’s rating of stuttering severity at first interview was in a range 2 to 9 on the 10-point scale with a mean of 4.5 and a standard deviation of 1.9. Analysis of speech samples at first interview indicated a stuttering rate in the range 3.9% to 17.0% with a mean of 7.3% and a standard deviation of 3.6%. SSI-3 scores at first interview were in the range 18 to 30 with a mean of 22.1 and standard deviation of 3.9. In the CWNS group, there were 19 boys and 15 girls. The age range at first assessment was 2 years 6 months to 4 years 11 months with a mean age of 4 years 2 months and a standard deviation of 1 year and 1 month. The gender distribution did not differ significantly between the CWS and CWNS groups, χ2(1) = 0.79, p = .37. The mean ages of the CWS and CWNS did not differ significantly, t = 0.09, df = 76, p = .92. Due to time and financial constraints and difficulty in recruiting control children, it was not possible to have equal numbers in the groups or to match on gender. Other studies have also reported imbalance between CWS and controls (e.g., Anderson & Wagovich, 2010; Yairi & Ambrose, 1999).
Assessments
Five assessments were used in this study to establish baseline measurements for the CWS and CWNS for the longitudinal study. These were
Speech recordings
Questionnaire 1: Family History of stuttering (Janssen, Kloth, Kraaimaat, & Brutten, 1996, modified by Howell et al., 2008)
Questionnaire 2: Child Health Questionnaire (CHQ; Landgraf, Abetz, & Ware, 1996)
Questionnaire 3: Child Development Questionnaire (CDQ)
Wechsler Pre-School and Primary Scale of Intelligence, Third U.K. Edition (WPPSI III-UK; Wechsler, 2003)
Speech recordings
Most of the children were seen in their own homes, but some were assessed at their school or nursery. During the first visit, a digital audio recording of the child’s spontaneous speech of approximately 20-min duration was made during free play with the researcher or parent. The speech samples were recorded on a Sony Digital Audio Tape (DAT) recorder using a Sennheiser K6 microphone. The recordings were transferred to a PC and uploaded for analysis using Speech Filing System (SFS) software (freeware available at http://www.phon.ucl.ac.uk/resource/sfs/). This recording was used to establish stuttering by measuring percent syllables stuttered. As part of the longitudinal study, children were followed up at 6-monthly intervals over a 3-year period and 20-min speech recordings were made at each visit. The follow-up data from these recordings will be used to establish persistence or recovery from stuttering in the group of CWS and will be reported in papers currently being prepared.
The Family History of Stuttering Questionnaire (Questionnaire 1) and the CHQ (Landgraf et al., 1996; Questionnaire 2) were mailed to parents prior to the first visit to give them time to source the relevant information and these were collected at the first assessment. The researcher checked the forms with the parents at the time and assisted with completion if required.
Questionnaire 1: Family History of Stuttering Questionnaire
Family history of stuttering was based on Janssen et al.’s (1996) questionnaire as modified by Howell et al. (2008). The biological mother and the biological father completed the questionnaire independently. Parents were asked about whether any blood relatives of their child had ever (or still) stuttered. Information was also obtained about the degree of relationship of the child to the affected relative(s). The responses were designated as first-degree (parent or sibling), second-degree (grandparent), or third-degree (aunt/uncle, cousin) relative.
Questionnaire 2: CHQ
The CHQ Parent Form–50 (CHQ PF-50; Landgraf et al., 1996) is a 50-item, parental report questionnaire designed to measure two components of child health: physical and psycho-social well-being. The authors suggest that the CHQ is an ideal instrument for comparing the health of children in general as well as specified subgroups of children (Landgraf et al., 1998).
Questionnaire 3: CDQ
The CDQ is a series of questions designed to elicit information regarding the child’s birth and early development. This was devised specifically for this study to assess those factors that have been associated with the onset of stuttering. This questionnaire was administered during the first visit and included the following questions:
Were there any complications with the birth? (please give details)
Was your child born full-term?
What was your child’s birth weight?
Did your child require any special care? (please give details)
Is your child right- or left-handed?
WPPSI
The WPPSI III-UK is an intelligence test for children in two age bands—2 years 6 months to 3 years 11 months, and 4 years to 7 years 3 months. Children in the younger age band complete four subtests (information, receptive vocabulary, block design, and object assembly). Children in the older age band complete seven subtests (information, vocabulary, word reasoning, matrix reasoning, picture concepts, block design, and coding). The subtest and composite scores represent intellectual functioning in verbal and performance cognitive domains and they provide a composite score of the child’s general intellectual ability (full-scale IQ). This test was carried out by one of the authors (S.C.) under the supervision of the principal investigator (P.C.) who is a qualified clinical psychologist.
Results
Data were not available for all participants on some parts of the assessments. This was because some parents did not want to answer certain questions or to complete questionnaires. The numbers of participants who provided data on each variable are given in Table 1.
The Number of Participants for Each Variable Investigated.
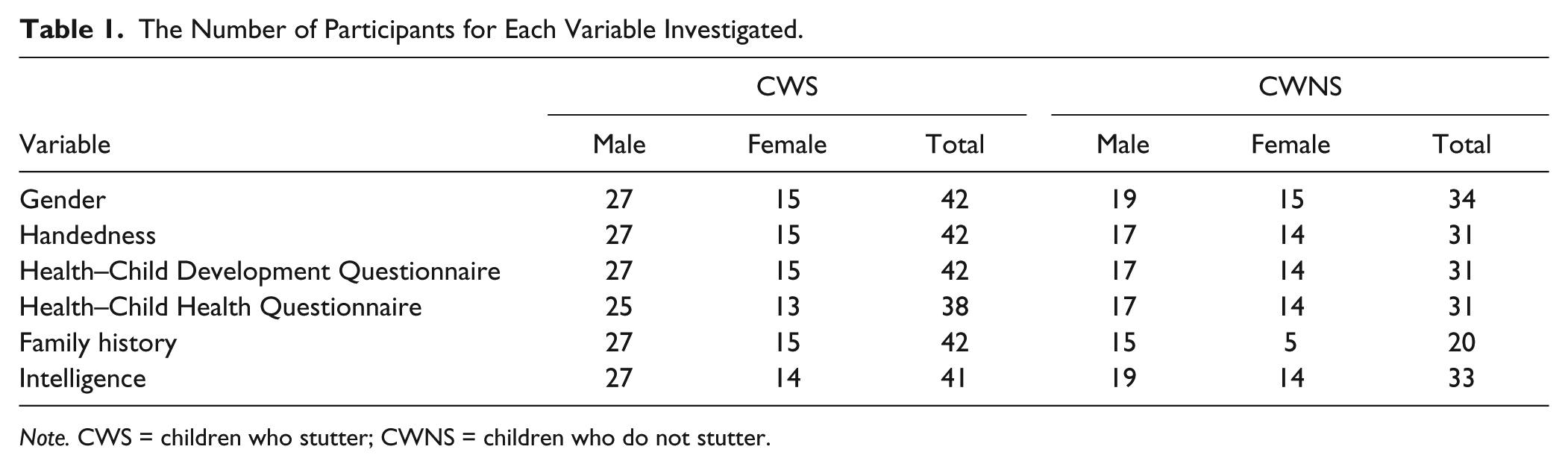
Note. CWS = children who stutter; CWNS = children who do not stutter.
Gender
Of the 42 CWS, 27 were male and 15 female, giving a male-to-female ratio of 1.8:1. This is lower than the 2.1:1 ratio reported by Yairi and Ambrose (1992) in children up to the age of 6. The ratio is higher than the 1.6:1 reported by Månsson (2000) and Dworzynski, Remington, Rijsdijk, Howell, and Plomin (2007) in 3-year-old children and the same as that found by Dworzynski et al. for children aged 4 to 7 years. Although the male:female ratio found in this study is comparable with other studies, it should be noted that the data were obtained from a smaller and highly selective population.
Handedness
Responses were available for 42 CWS and 31 CWNS (handedness was asked as part of Questionnaire 3). Parents indicated that 5 (11.9%) of the CWS showed no preference in which hand they used for everyday tasks; 3 of these were boys and 2 were girls. Of the remaining 37 CWS, 28 (75.7%) were described as predominantly right-handed and 9 (24.3%) as predominantly left-handed. In the CWNS group, 2 boys and 1 girl indicated no hand preference (12%). Of the remaining 28 CWNS, 25 (89.3%) were described as predominantly right-handed and 4 (14.3%) as predominantly left-handed. Males and females had a different distribution of handedness. Fifteen (62.5%) of the 24 boys for whom data were available were right-handed compared with 12 (92.3%) of the 13 girls. The difference in distribution across the genders was significant (χ2 = 3.79, p = .05). Table 2 gives the distribution of participants across handedness. The difference in distribution of handedness between CWS and CWNS was not significant (χ2 = 1.28, p = .25).
The Distribution of Participants With Respect to Handedness.
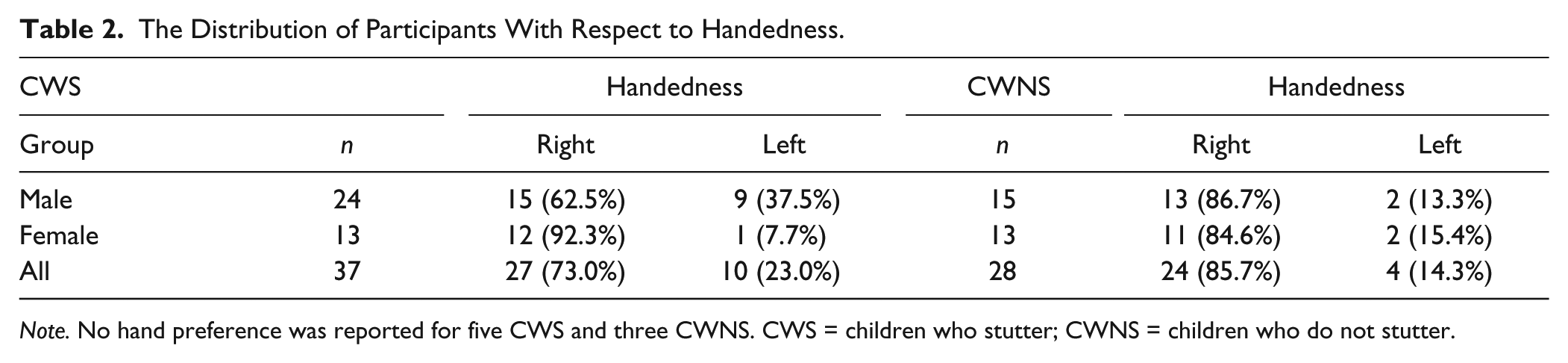
Note. No hand preference was reported for five CWS and three CWNS. CWS = children who stutter; CWNS = children who do not stutter.
Health and Head Injury
Results from the CDQ (Questionnaire 3) showed that 14 (33.3%) out of the 42 parents of CWS reported complications at birth. These comprised four emergency Caesarean sections, five ventouse-assisted deliveries, and five other types of complication (heart, breathing problems, etc.). No instance of forceps delivery was reported. In comparison, the parents of 14 (45.2%) of the 31 CWNS reported complications at birth. These comprised five emergency Caesarean sections, two ventouse-assisted deliveries, two forceps deliveries, and five other complications. A chi-square analysis on the contingency table of participant group (CWS/CWNS) and problems at birth (none/any of the types indicated) showed that there was no significant association between groups and birth problems. There were no reports of head injury from parents of either the CWS or the CWNS.
Information was also obtained regarding the child’s health and development from the CHQ (Questionnaire 2). Data from the CHQ (Landgraf et al., 1996) were supplied by parents of 38 CWS and 31 CWNS. Two of the CWS have dropped out without completing the CHQ, and the remaining parents have not completed it to date. In this study, the CHQ was used to investigate differences in health and emotional and social well-being between CWS and CWNS.
CHQ (Questionnaire 2)
Significant differences were reported on the emotional impact on the parents of their child’s health, behavior, and attention/learning difficulties, t(74) = −2.19, p = .03, and on the family’s cohesion as a unit, t(74) = −2.14, p = . 03. In the emotional impact section, parents were asked to rate how much emotional suffering or worry was experienced by the parents as a result of their child’s (a) physical health, (b) emotional well-being or behavior, and (c) attention or learning abilities. In the family cohesion section, parents were asked to respond to the following statement: Sometimes families may have difficulty in getting along with one another. They do not always agree and they may get angry. In general, how would you rate your family’s ability to get along with one another? There were no significant differences between CWS and CWNS groups for the concepts of global health, changes in health, physical functioning, role/social limitations due to emotional or behavioral difficulties, role/social limitations due to physical health, bodily pain and discomfort, behavior, mental health, self-esteem, time impact on parent, and family activities. In summary, parents of CWS were significantly more concerned than parents of CWNS about their child’s health, behavior, and attention/learning difficulties, and families of CWS were reported as having greater difficulty in getting along together than families of CWNS. Table 3 displays the mean raw scores for the concepts together with standard deviations and t-test values. Bearing in mind the subjectivity involved in responding to the types of question in the questionnaire together with the difference in the variance between the two groups, the results from this analysis should be treated with caution.
Raw Concept Scores and t-Test Results for Child Heath Questionnaire.
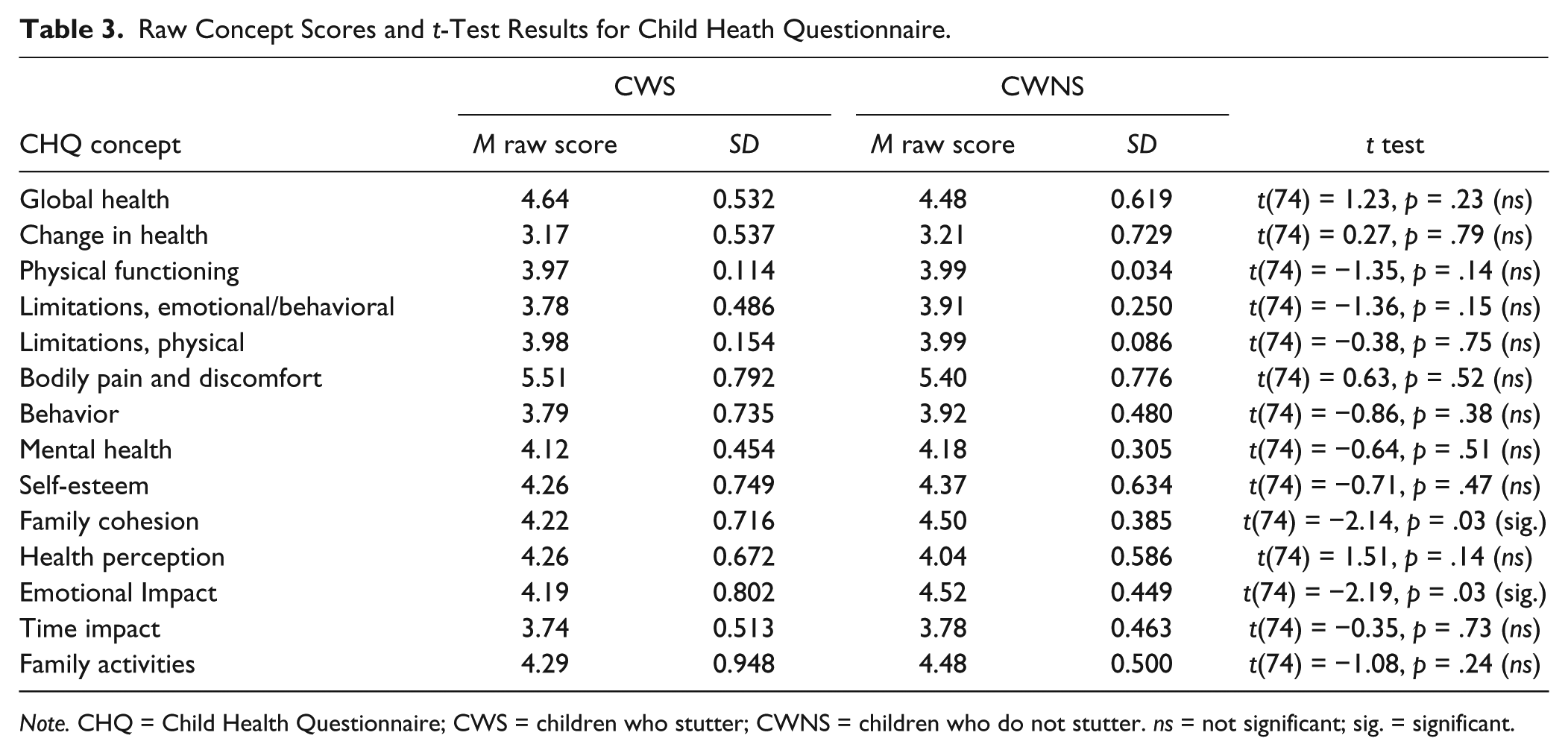
Note. CHQ = Child Health Questionnaire; CWS = children who stutter; CWNS = children who do not stutter. ns = not significant; sig. = significant.
Family History
Twenty-eight (67.7%) of the 42 families of CWS reported a positive family history of stuttering. Further analysis showed that 12 (28.6%) of the families reported stuttering in first-degree relatives only and a further 5 (11.9%) families reported stuttering in both first- and/or second- and third-degree relatives. These two figures combined show that 40.5% of the families had a positive family history of stuttering in first-degree relatives. These figures are close to the 46.6% positive first-degree relatives and 66.3% positive family history overall reported by Yairi and Ambrose (1992) and the 45% and 64%, respectively, reported by Yairi (1983). A positive family history was reported more frequently for male CWS with 19 (76.0%) out of 25 males compared with 9 (52.9%) out of 17 females. A chi-square test showed that this difference was significant (χ2 = 4.08, p = .04).
Family history data were used from 20 CWNS. Although family history questionnaires were obtained from 28 CWNS, eight children were excluded because they were related to other participants in the study. Three of the CWNS had siblings in the CWS group, and five had other siblings present in the CWNS group (family history data were only included once per family). A positive family history was reported in five families (25%) of the subgroup of 20 CWNS. A positive family history was reported more often among families of CWS than CWNS. A chi-square test showed that this difference was significant (χ2 = 9.45, p = .01).
Intelligence
The WPPSI III-UK (Wechsler, 2003) was administered to 41 CWS and 33 CWNS. These data indicated that the mean scores for both groups fell within the high average range. Subsequent t tests indicated that CWS scored significantly lower than CWNS on the verbal, performance, and full composite scales. Scale scores and t-test results are listed in Table 4.
WPPSI-III Scores and t-Test Results.
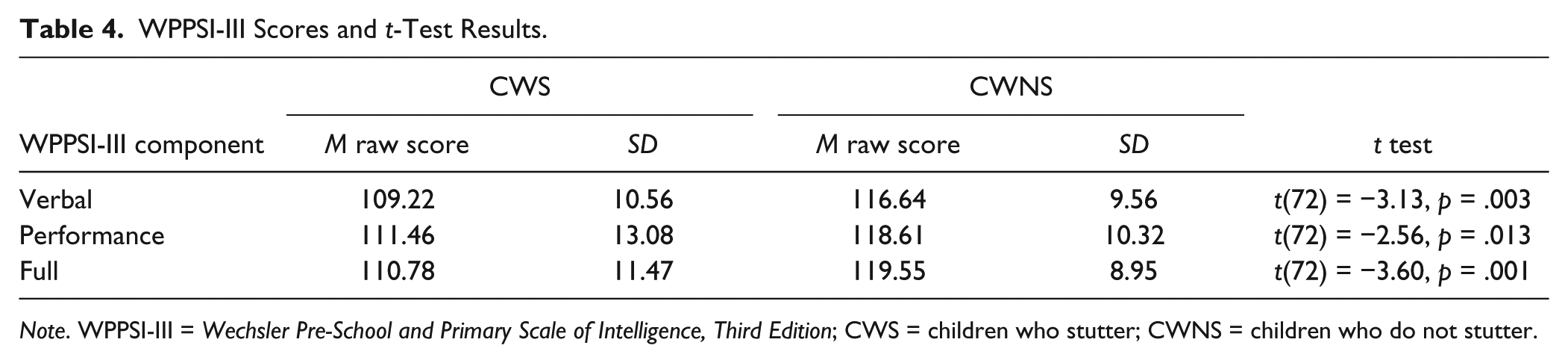
Note. WPPSI-III = Wechsler Pre-School and Primary Scale of Intelligence, Third Edition; CWS = children who stutter; CWNS = children who do not stutter.
Discussion
The data reported in this study were derived from baseline assessments made on CWS and controls. The data from the longitudinal study that investigates persistence and recovery of stuttering will be reported later. The five factors selected for investigation may have a bearing on a child’s propensity to stutter and thus have relevance for the assessment of stuttering and potentially for the likelihood of persistence of stuttering.
It is also possible that these factors may have implications for what intervention is appropriate for the children’s stuttering which, in turn, would have ramifications as to the most effective use of scarce health service resources.
The five factors investigated were gender, handedness, general health, family history of stuttering, and intelligence.
Gender
In this study, the reported male:female ratio in the CWS group was 1.8:1.This finding fits in with the range of values reported in previous research (Johnson et al., 1959, Månsson, 2000). The study confirmed that being male could be a risk factor to be taken into account in the diagnosis of stuttering and estimating the likelihood of its persistence.
Handedness
The percentage of left-handed CWS (24.3%) was higher than the 16% reported in adults who stutter (Records, Heimbuch, & Kidd, 1977) and the 19% of adolescents reported by Howell and Davis (2011).
A statistically significant difference was also found between male and female CWS in terms of handedness. Nine of the 24 male CWS (37.5%) were left-handed compared with 1 of the 13 girls (7.7%). The incidence of left-handedness in the female cohort was similar to the incidence of left-handedness reported in the general population: approximately 10% (McManus, 2002). However, the incidence of left-handedness in the male cohort (37.5%) was far higher than the population at large and significantly so. In the control group of CWNS, the incidence of left-handedness was similar in both males and females (13.3% and 15.4%, respectively) and only slightly higher than the incidence of 10% reported in the general population (McManus, 2002). This makes the 37.5% figure for left-handedness in the group of CWS all the more noteworthy and raises the inevitable question of whether left-handedness in males is associated with the onset and persistence of stuttering and whether, for each of these aspects, handedness differences result in, or are a result of, stuttering. The finding of this research raises the possibility of atypical cerebral laterality in males as manifested by a preference for left-handedness being related to the onset of stuttering. This could be confirmed by neurological investigations in high-risk children and by determining whether the CWS who started to stutter later were more likely to have atypical laterality prior to onset compared with CWNS. The high incidence of left-handedness in male CWS has also been reported to be significant in relation to the persistence of stuttering as Howell et al. (2008) noted that right-handedness was associated with an increased chance of recovery. Being a left-handed male could therefore be considered as a risk factor for stuttering and its persistence.
Family History
A further finding from this study pertaining to males was about positive family history of stuttering. For the CWS, 76% of males had a positive family history of stuttering compared with 52.9% of females and the difference was significant. A positive family history was more prevalent among families of CWS than CWNS. A chi-square test showed that the difference was significant, χ2(1) = 9.45, p = .01. Being a male with a positive family history may again be considered as a risk factor in the diagnosis of stuttering and its persistence.
General Health
There were no reports of head injury from parents of either CWS or CWNS.
The CDQ (Questionnaire 3) showed that complications at birth (which may be a cause of head injury) were not related to the onset of stuttering. Only 33.3% of the parents of the CWS reported complications at birth compared with 43.7% of the parents of the CWNS. This is in contrast to previous research, which linked head injury to the onset of stuttering (Alm & Risberg, 2007; Segalowitz & Brown, 1991).
CHQ
The CHQ (Questionnaire 2) yielded several interesting findings. There were no significant differences between groups in the parents’ perception of their child’s mental health or self-esteem. Parents of CWS were, however, significantly more concerned than parents of CWNS about their child’s health, behavior, and attention/learning difficulties, despite the finding that they reported no differences on the impact of these parameters on their own time as parents or on family activities. Families of CWS reported that they felt they were less cohesive as a unit than families of CWNS and the difference was again significant.
It is difficult to ascertain cause and effect from the above findings on health and social factors. Are parents of CWS more anxious about the health of their children because of their stutter or might anxiety have contributed to the onset of stuttering? Again, do families get on less well or are perceived to get on less well as a result of stuttering, or have perceived or real family dysfunction contributed to the onset of stuttering? The common factor behind these observations could perhaps be anxiety that manifests in concern for their child’s health and in the belief that the family does not get on that well. It could be speculated that this would be the result of higher expectations and higher levels of self-criticism. It certainly seems that family environment and levels of anxiety in the families of CWS are worth further investigation, and will be addressed in the ongoing longitudinal study that examined what factors may be involved in the persistence of stuttering.
It is difficult to identify a potential specific risk factor from these results although a careful exploration of family relationships and anxiety levels within the family may be helpful in this respect.
Intelligence
Administration of the WPPSI III-UK showed that CWS scored significantly lower than CWNS on the verbal, performance, and full composite scales, although both the CWS and CWNS groups fell within the high average range. This finding supports the evidence from older research (Andrews & Harris, 1964; Johnson, 1955) that CWS tend to have a lower IQ than controls.
Conclusion
The five factors investigated in this study differed significantly between CWS and CWNS. Although there are limitations to the study in terms of size of sample and possible reporting bias on measures used (e.g., the results of the CHQ relied on self-report, which can result in subjective bias), these factors could reasonably be argued to be potential “risk” factors in the identification of stuttering. A checklist of these factors may be a helpful “tool” for speech–language pathologists alongside speech measures to more confidently make a diagnosis of stuttering. The participants in this study will be followed up over a 3-year period, so that comparisons can be made between children who persist in stuttering and those who recover from stuttering in the factors being investigated.
The longitudinal nature of this study should allow these factors to be investigated with regard to their utility in providing a prognosis and the course of therapy required. This is of particular significance in the climate of the U.K.’s National Health Service today where increasingly scarce resources make it vital that they are targeted where they will be most effective.
Footnotes
Acknowledgements
The support of the Dominic Barker Trust is gratefully acknowledged.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.