
Abstract
Keywords
Introduction
More than 200,000 femoropopliteal stents are implanted in the United States each year. 1 Despite improved devices and reduced rates of postprocedure complications, femoropopliteal in-stent restenosis (FP-ISR) remains a common problem, with an incidence up to 37% for lesion lengths of <150 mm and 60% for longer lesions. 2 Angiographic characteristics of FP-ISR are also an important determinant of subsequent outcome. 3 Class I (≤50-mm lesion) and class II (>50-mm lesion) FP-ISR are associated with reasonable patency after reintervention, whereas class III (total in-stent occlusion) FP-ISR is an independent predictor of recurrent restenosis (85% at 1 year) and reocclusion (65% at 1 year) when treated with balloon angioplasty. 4
Multiple modalities are available to treat FP-ISR, including laser and excisional atherectomy, repeat stenting with self-expanding covered stents, drug-eluting balloons and stents, and combinations of these therapies.5 –27 However, the optimal approach to endovascular treatment of FP-ISR remains controversial. One recent study showed high rates of restenosis and recurrent occlusion for class II and III FP-ISR even with the use of adjunctive devices and provisional stenting, thus raising concern that currently available technologies may not improve outcomes of FP-ISR compared with balloon angioplasty alone. 28
Given that in-stent occlusion contains both neointima and thrombus, laser atherectomy, by debulking the neointima and thrombus and inhibiting platelet aggregation, offers a potentially promising therapeutic avenue for treatment of FP-ISR. 16 Several studies have examined the use of laser atherectomy for treatment of FP-ISR, but those studies did not specifically analyze the association of angiographic characteristics with outcomes.6,29 In this study, patients with FP-ISR treated at two centers with laser atherectomy and standard balloon angioplasty were compared with patients treated with standard balloon angioplasty alone.
Methods
Study Design and Patient Population
This retrospective study, which was approved by the Institutional Review Boards of the University of California Davis and the University of Colorado, included patients who underwent endovascular treatment of FP-ISR between 2006 and 2013. Baseline patient data were collected from review of electronic medical databases; procedure details were gathered from medical records and procedure logs. Two physicians reviewed all angiographic images for lesion morphology and characteristics, TransAtlantic InterSociety Consensus (TASC) II classification, and distal runoff. 30 FP-ISR was categorized using the Tosaka classification 4 as class I (focal, lesion length ≤50 mm), class II (diffuse, >50 mm long), or class III (chronic total occlusion of the stent). Unsubtracted digital images were examined to identify the presence of stent fractures. 30
Ankle-brachial index (ABI) and duplex ultrasound were performed before treatment and routinely at 30 days post procedure with a concomitant assessment of clinical improvement. Subsequent follow-up included clinical and serial duplex examination and was conducted every 3 months during the first postoperative year and every 6 to 12 months thereafter.
During the study period, 135 patients (mean age 71 years; 76 men) underwent endovascular intervention for treatment of FP-ISR. Of these, 54 (40%) were treated with laser atherectomy (Table 1) and the remaining 81 patients with balloon angioplasty alone. The majority of patients in both groups presented with claudication as the indication for intervention, although a significant percentage (35% vs 46%) presented with recurrent critical limb ischemia. The majority of patients were treated with aspirin, statin, and clopidogrel at baseline, and all patients were treated with aspirin for life and clopidogrel for at least 1 month post procedure.
Patient and Angiographic Characteristics. a
Abbreviations: ABI, ankle-brachial index; BMI, body mass index; CLI, critical limb ischemia; ISR, in-stent restenosis; SFA, superficial femoral artery; TASC, TransAtlantic Inter-Society Consensus; TBI, toe-brachial index.
Continuous data are presented as the means ± standard deviations; categorical data are presented as the counts (percentage).
Endovascular Treatment
The treatment strategy generally involved crossing of the FP-ISR segment with a 0.035-inch guidewire, followed by the laser catheter [2.0 or 2.3-mm Turbo Elite (Spectranetics Inc, Colorado Springs, CO, USA) or the Turbo-Tandem device] advanced at 1 to 2 mm/s. The use of distal embolic protection and the number of passes and energy delivered by the laser were at the operator’s discretion. After laser atherectomy, balloon angioplasty was routinely performed with a balloon matched to the reference vessel diameter. In cases of flow-limiting dissection, intrastent filling defects, or other suboptimal angiographic result, adjunctive therapy including repeat stenting was performed at the operator’s discretion.
Outcomes and Definitions
The primary endpoint was recurrent restenosis, which was defined as the presence of >50% stenosis at the treatment site (based on peak systolic velocity ratio >2.4) or by target lesion revascularization (TLR), which included any repeat endovascular intervention or surgical bypass to the target vessel. Secondary outcomes included stent reocclusion, TLR, and major amputation (above the ankle joint). Clinical improvement referred to improvement in Rutherford category by ≥1 level with a concomitant increase in ABI by ≥0.15 and no need for TLR.
Statistical Analysis
Mean values with standard deviation were used to describe continuous variables, while numerical values (percentages) were given for categorical data. Continuous variables were compared using the Wilcoxon rank sum test; categorical data were compared using the chi-square or Fisher exact test. Freedom from recurrent restenosis and freedom from occlusion were estimated using Kaplan-Meier survival analysis; groups were compared with the log-rank test. All tests were 2-sided, and the p value for statistical significance was <0.05. Analyses were conducted using STATA software (version 13.1; STATA Corporation, College Station, TX, USA).
Univariate analysis was used to identify predictors of recurrent restenosis. Relationships between laser atherectomy and outcomes of FP-ISR were examined with Cox regression analysis; outcomes are reported as the hazard ratio (HR) and 95% confidence interval (CI).
Results
Group Comparison
The groups were well matched in terms of baseline characteristics, with similar baseline ABIs (0.70 vs 0.65, p=0.3), TBI (0.33 vs 0.37, p=0.4), and below-knee runoff. Among the lesion characteristics (Table 1), patients treated with laser atherectomy had significantly longer ISR lengths (222 vs 114 mm, p<0.001) but similar reference vessel diameters. In addition to longer overall lesion length, there was a higher incidence of Tosaka class III FP-ISR (in-stent occlusion, 69% vs 20%, p=0.001) in patients treated with laser atherectomy. Consistent with longer segment disease, patients treated with laser atherectomy also had more FP-ISR extending from the superficial femoral artery (SFA) into the popliteal artery (57% vs 27%, p=0.001). The rates of stent fracture (10% vs 11%) were not significantly different between groups.
Procedure Outcomes
The majority of laser catheters utilized (n=44) were the Turbo Elite model, with a minority of cases (n=10) utilizing the Turbo-Tandem device; the mean maximum fluency was 48±7 mJ/mm2, and the mean maximum rate was 30±10 Hz. Distal embolic protection was used more frequently in patients treated with laser atherectomy (22/54) than patients treated with balloon angioplasty (12/81).
Procedure success was 100% in the laser group and 98% in the group treated with only balloon dilation (Table 2). Rates of distal embolization requiring treatment were low but higher in the laser group (9% vs 1%, p=0.01). The rate of provisional stenting was 59% in the laser atherectomy group vs 37% in the balloon angioplasty group (p=0.01). When stratified by angiographic presentation, the rates of provisional stenting were similar for class I/II FP-ISR (41% vs 34%, p=0.6) and class III FP-ISR (68% vs 47%, p=0.2). The postprocedure ABI was similar in both groups (0.93±0.2 vs. 0.91±0.2), as was the clinical improvement at 30 days (89% vs 81%, p=0.2). No patients required a major amputation, and the overall mortality was similar between groups at 2 years (17% vs 11%, p=0.3).
Procedure Outcomes. a
Abbreviations: ABI, ankle-brachial index; TBI, toe-brachial index.
Continuous data are presented as the means ± standard deviations; categorical data are presented as the counts (percentage).
Outcomes in Follow-up
At 1 year, 101 of the 135 patients had adequate data for patency analysis (34 patients were censored due to lack of data); at 2 years, 86 were included in the patency analysis. There was no difference in the rates of follow-up between groups.
Cox regression analysis demonstrated a significant interaction between laser atherectomy and Tosaka class III FP-ISR (HR for interaction 0.25, p=0.01). Based on this interaction, the outcomes of laser atherectomy were stratified by Tosaka class I/II (restenosis) vs Tosaka class III FP-ISR (stent occlusion). Among patients with class I/II FP-ISR, there was no significant benefit of laser atherectomy on rates of recurrent restenosis at 2 years (69% vs 46%, p=0.2) or stent occlusion (26% vs 12%, p=0.2). However, patients with class I/II FP-ISR who were treated with laser atherectomy had significantly lower rates of TLR at 2 years (14% vs 44%, p=0.05; Figure 1). Notably, patients with class I/II FP-ISR who were treated with laser atherectomy had lengthier restenotic lesions (129±86 vs 89±86 mm, p=0.09), suggesting that laser atherectomy was preferentially used for more complex FP-ISR even in the absence of stent occlusion.
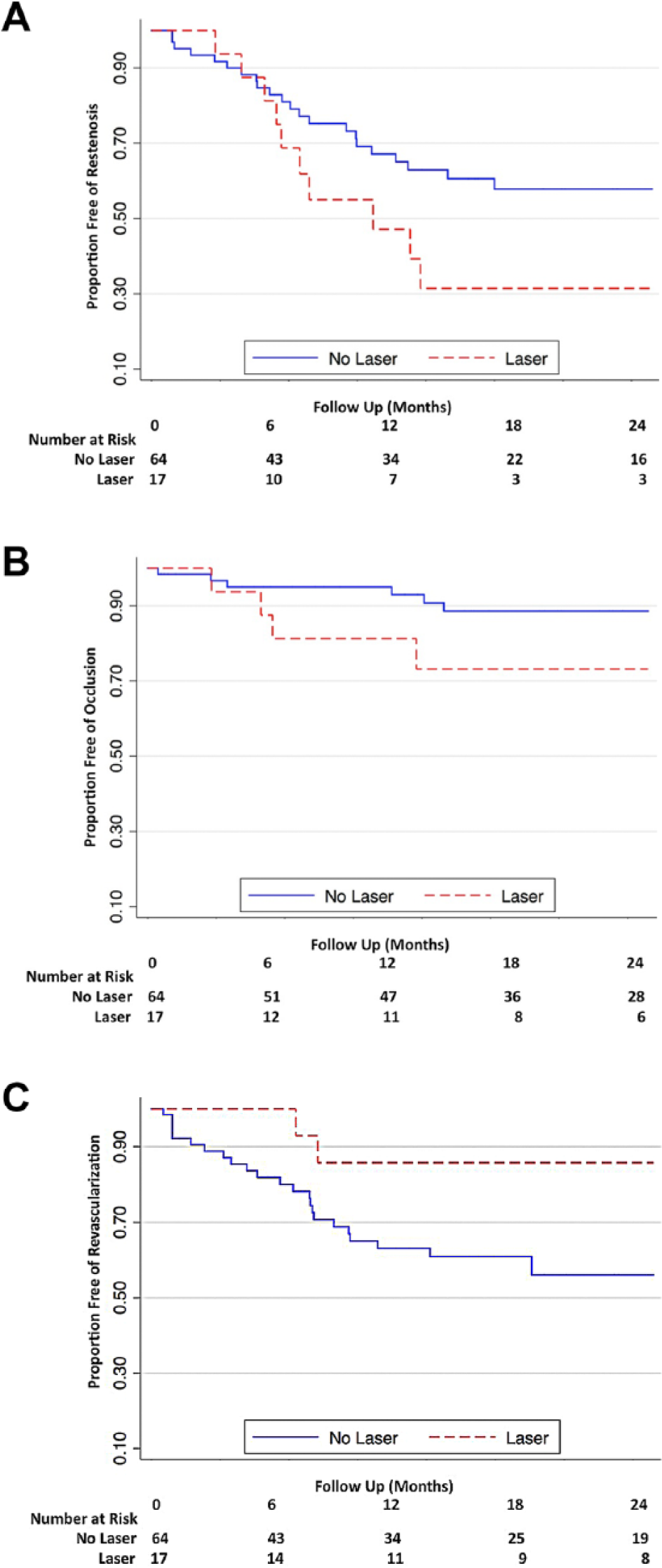
Use of laser atherectomy with adjunctive balloon angioplasty for the treatment of class I/II femoropopliteal in-stent restenosis is not associated with reduced rates of (A) recurrent stenosis or (B) occlusion but was associated with reduced rates of (C) target lesion revascularization. The standard error did not exceed 10% at each time point for either group.
Among patients with class III FP-ISR, laser atherectomy was associated with significantly lower rates of recurrent restenosis at 1 year (54% vs 91%, p=0.05) and 2 years of follow-up (69% vs 100%, p=0.05). The overall rates of TLR were similar between the groups (43% vs 48%), but laser atherectomy was also associated with significantly lower rates of recurrent in-stent occlusion at 2 years (33% vs 71%, p=0.04; Figure 2).
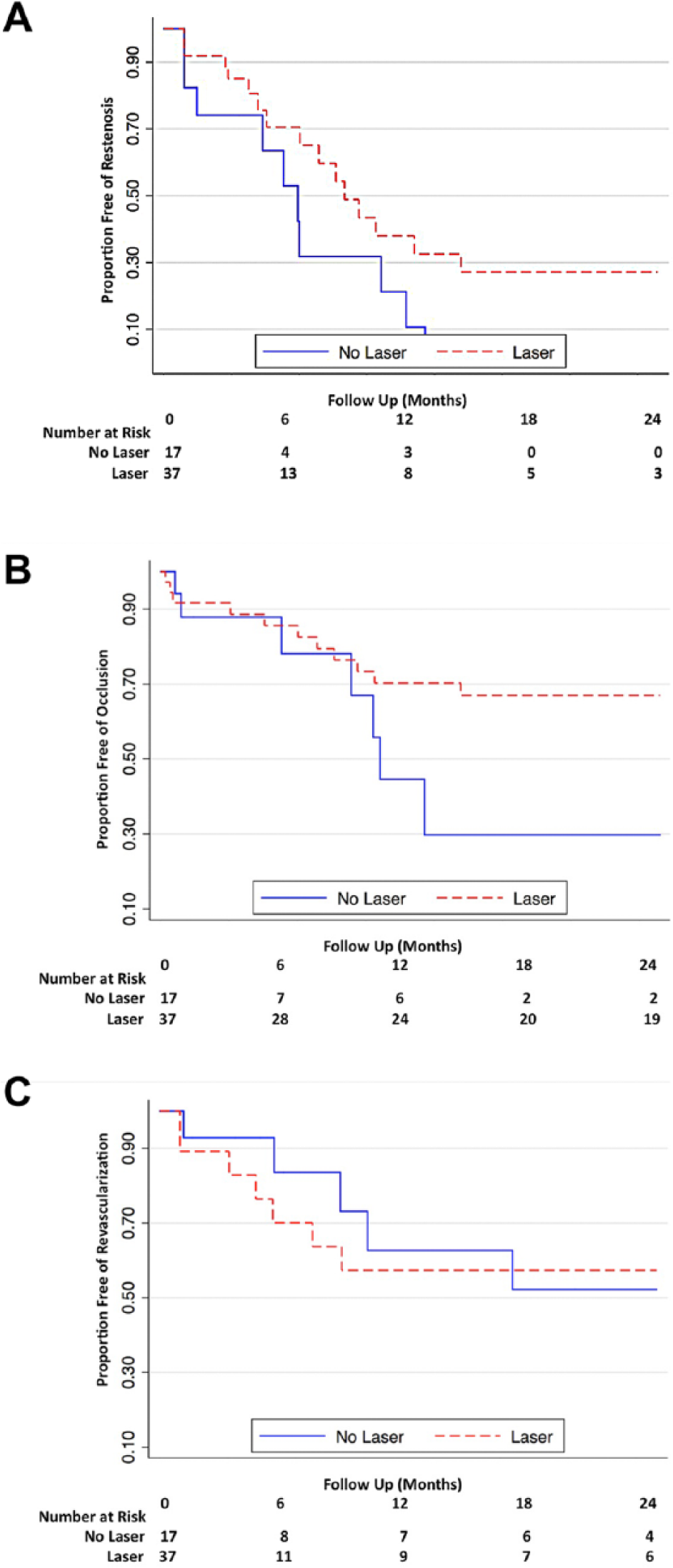
Use of laser atherectomy with adjunctive balloon angioplasty for the treatment of class III femoropopliteal in-stent restenosis is associated with reduced rates of (A) recurrent stenosis and (B) occlusion but no difference in rates of (C) target lesion revascularization. The standard error was <10% for both groups at 18 months but exceeded 10% for both groups at 24 months.
Discussion
The effectiveness of laser atherectomy in the treatment of FP-ISR is related to debulking of neointima and thrombus as well as suppression of platelet aggregation. By vaporizing plaque, laser atherectomy can also promote better stent expansion. Additionally, laser atherectomy can improve cross-sectional area prior to placement of a covered stent, allowing better stent-graft expansion, limiting stent-graft infolding, and thus reducing the risk of thrombosis within the stented area.2,31 This plaque modification can also potentially create micropores in the endothelium and enhance the clinical effectiveness of drug-coated balloons. 32 Together, these mechanisms may improve the outcomes after endovascular treatment of FP-ISR when compared with standard balloon angioplasty. This more extensive plaque modification could also explain the lower rates of TLR that we observed in patients with class I/II FP-ISR who were treated with laser atherectomy.
The recently published EXCITE-ISR trial, 1 which was a prospective, multicenter, randomized study evaluating excimer Turbo-Tandem laser atherectomy with adjunctive balloon angioplasty vs angioplasty alone for treatment of FP-ISR, showed similar results to our study, with procedure success higher in the laser with dilation group (93.5% vs 82.7% with dilation alone). Their overall rates of distal embolization were also low and consistent with results from prior studies.33,34 During 1-year follow-up, freedom from TLR, freedom from bailout stenting, and primary patency rates were higher with the use of laser atherectomy compared with dilation alone. In subgroup analysis, patients with more complicated lesions, as defined by either TASC D stenosis or total occlusion, appeared to benefit the most from laser atherectomy with dilation compared to angioplasty alone. The EXCITE trial also showed greater efficacy of the combined approach with longer lesion length, 1 similar to our study.
Several differences should be noted between our study and the EXCITE-ISR trial. 1 Compared to our patient population, subjects enrolled in EXCITE-ISR had higher rates of coronary artery disease but lower rates of diabetes and overall Rutherford classification. Additionally, subjects in that trial had lower rates of FP-ISR total occlusion and greater stent fracture rates than observed in our study. The mean lesion lengths in the 2 cohorts of the EXCITE-ISR trial were similar, unlike our patients, who had longer lesions in the laser treatment group. This likely reflects real-world treatment bias, where laser atherectomy is preferentially used for the treatment of more complex lesions. 35 Patients in EXCITE-ISR were treated with the Turbo-Tandem directional laser, which is a biased catheter that creates a larger lumen, whereas the majority of patients in our study were treated with the smaller caliber (Turbo Elite) excimer laser catheter that creates a pilot channel. 16 The PATENT study specifically examined the combination of a Turbo Elite catheter followed by a Turbo Booster directional laser for the treatment of FP-ISR, with a residual stenosis of only 32% after laser atherectomy and 7% after adjunctive balloon angioplasty. 36 This improved debulking capacity of a directional laser atherectomy catheter may provide some additional benefit compared to standard laser atherectomy, as has been studied in native femoropopliteal disease as well. 37 It is possible that the greater debulking performed in EXCITE-ISR and PATENT studies could account for the differences in provisional stenting rates; provisional stenting in our population was generally performed for treatment of residual stenosis after balloon angioplasty or for treatment of dissection.
In addition to laser atherectomy, several other options exist for the treatment of FP-ISR. Covered stents have demonstrated lower rates of recurrent ISR and TLR compared with balloon angioplasty and were recently approved by the Food and Drug Administration for treatment of FP-ISR.11,16,17,19,21 –25 Drug-eluting stents, which elute paclitaxel, have also been associated with lower TLR and higher primary patency rates.12,20 The relatively few length options for drug-eluting stents, however, may limit their utility and cost-effectiveness.2,12,16
Excisional atherectomy can provide significant neointimal debulking, but its clinical benefit in the treatment of FP-ISR has been undermined by disappointing rates of restenosis at 1-year follow-up. 13 Further trials are necessary, especially those combining laser atherectomy with these and other devices, such as scoring or cutting balloons.7,8 In cases of multiple FP-ISR recurrences despite endovascular therapy, surgical femoropopliteal bypass should also be considered.
An alternative strategy in the treatment of FP-ISR is the use of drug-coated balloons (DCBs), which deliver paclitaxel at the site of angioplasty, thereby inhibiting microtubule formation and limiting cell replication, smooth muscle cell proliferation, and ingrowth post angioplasty. 2 Stabile and associates5,18 evaluated the use of DCBs in the treatment of FP-ISR and reported a primary patency rate of 92% at 1 year and 70% at 2 years. The DEBATE-ISR trial evaluated outcomes of DCBs in FP-ISR patients with diabetes showed improved patency rates compared to standard balloon angioplasty at 1 year. 9 It is important to note, however, that small sample sizes limit the power of these trials. The FAIR trial, a prospective randomized study of 119 patients with FP-ISR stenosis of 70% to 100%, also showed lower restenosis and TLR rates for DCBs compared with angioplasty alone at 6 and 12 months. 10
The combination of DCBs and atherectomy has also yielded encouraging results in the treatment of FP-ISR. Preliminary studies have shown improved restenosis and patency rates using excisional atherectomy in combination with DCB or angioplasty. 14 A study that randomized subjects with class III FP-ISR to laser atherectomy and DCB vs DCB alone also demonstrated a lower rate of TLR at 12 months with combination therapy, as well as a lower rate of major amputation. 15 The combination of laser atherectomy with DCB-angioplasty thus may be an important future treatment option for FP-ISR.
Limitations
This was a retrospective analysis and may therefore be subject to bias in the treatment decision to use laser atherectomy. Consistent with this, longer lengths of restenosis were more likely to be treated with laser atherectomy, suggesting a preference for the use of laser atherectomy when treating more complex lesions. Second, there was a high rate of provisional stent placement. However, this study represents a real-world cohort and provides analysis of all patients who have undergone treatment of this difficult clinical presentation. Third, the caliber of the laser used was at the discretion of the operator. It is possible that routine use of larger caliber laser atherectomy, such as in the EXCITE-ISR trial, could be associated with improved outcomes, especially for treatment of long segment (class II) FP-ISR.
Conclusion
Treatment of femoropopliteal ISR with laser atherectomy and adjunctive balloon angioplasty is associated with decreased rates of TLR in the treatment of class I/II FP-ISR and with decreased recurrent restenosis and occlusion when used to treat in-stent occlusion. Further studies should be performed to evaluate the additive benefit of laser atherectomy with emerging drug-eluting technologies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: John R. Laird is a consultant for Boston Scientific, Covidien, Abbott, Bard, and Medtronic; he receives research support from W.L. Gore. Ehrin J. Armstrong is a consultant for Abbott Vascular, Medtronic, Merck, and Spectranetics.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.