
Abstract
Keywords
Introduction
Prevention of spinal cord injury (SCI) remains one of the main concerns during open and endovascular repair of descending thoracic aneurysm (DTA) and thoracoabdominal aortic aneurysms (TAAAs). Paraplegia is a devastating complication for the patient, family, and medical team and has been associated with significantly shortened survival. 1 Although the etiology of SCI is multifactorial, arterial embolization, coverage of large aortic segments, insufficient collaterals, and systemic hypotension are the main predisposing factors during endovascular TAAA repair.2,3 The importance of an extensive spinal collateral network that includes the carotid, subclavian, vertebral, intercostal, lumbar, hypogastric, and deep femoral arteries has been recently emphasized in experimental and clinical studies.3–5 These studies have shown that a staged repair with segmental coverage of the aorta allows rapid recruitment of the spinal collateral networks, decreasing mortality and SCI during endovascular TAAA repair.4,6,7
Neuromonitoring with continuous motor-evoked potential (MEP) and somatosensory-evoked potential (SSEP) has been widely applied during open TAAA repair to guide reimplantation of intercostal arteries and to optimize distal aortic perfusion.8,9 In contrast to open repair, endovascular incorporation of intercostal arteries is not feasible. Several authors have advocated neuromonitoring during endovascular repair as a means to optimize spinal cord perfusion.10,11 We hypothesized that immediate recognition of ischemia using neuromonitoring may allow the use of maneuvers to optimize spinal cord and lower extremity perfusion and decrease the rate of SCI. The aim of this study was to review the clinical utility and outcomes of a standardized protocol of continuous intraoperative MEP/SSEP monitoring, cerebrospinal fluid (CSF) drainage, hemodynamic augmentation, and selective use of temporary iliac or femoral conduits in patients undergoing endovascular repair of DTA and TAAAs.
Methods
Study Design
The clinical data and outcomes of consecutive patients treated for type C DTA (from subclavian artery to celiac axis) and types I to IV TAAAs between July 1, 2011, and August 30, 2014, were reviewed in a study approved by the Institutional Review Board of the Mayo Clinic. All patients consented to participation in minimal-risk clinical research protocols. Patients treated by fenestrated/branched endografts were participants in a prospective physician-sponsored Investigational Device Exemption protocol registered at ClinicalTrials.gov (NCT1937949 and NCT02089607).
Data Collection and Definitions
Patient demographics, clinical characteristics, and radiologic and procedural data were reviewed. Clinical risk assessment was determined using standardized scoring systems including the Society of Vascular Surgery cardiac, pulmonary, renal, hypertension, and age scores and the American Society of Anesthesiologists physical status classification.
Technical success was defined by successful placement of aortic stent-graft and target vessel stents. Early and late outcomes were noted. Early outcome was defined as occurring in the hospital stay without regard to the number of days after the procedure or within the first 30 days after stent placement. Late outcome was obtained from the medical records, office visits, correspondence with referring physicians, and patient questionnaire or telephone interview. Follow-up include clinical examination, computed tomography angiography, and visceral artery duplex ultrasound performed prior to discharge, at 6 to 8 weeks, at 6 months, and annually thereafter.
Patient Population
In the observation period, there were 49 patients (mean age 75±8 years, range 47–86; 38 men) with type C DTA (n=5) or TAAA (n=44: 23 type IV, 11 type III, 8 type II, and 2 with type I; Table 1). Mean aneurysm diameter was 65±10 mm. Five patients had symptomatic aneurysms and one had ruptured acute type B aortic dissection complicated by intramural hematoma and acute aneurysm expansion. Aneurysm etiology was degenerative in 42 (86%) patients and dissection in 7 (14%). Twenty-seven (55%) patients had prior aortic repair (infrarenal aorta in 15 patients, thoracic aorta in 11, and aortic arch in 3). Forty-four (92%) patients had patent bilateral internal iliac arteries, with high-grade stenosis (>50%) in at least one side in 15. Five patients had occlusion of one or both internal iliac arteries. Length of aortic coverage averaged 286±89 mm (range 138–492), which corresponded to 64%±18% (range 33%–100%) of the estimated length from the subclavian artery to the aortic bifurcation.
Demographic, Clinical, and Anatomical Characteristics of 49 Patients Treated for Descending Thoracic or Thoracoabdominal Aortic Aneurysms. a
Abbreviations: DTA, descending thoracic aorta; TAAA, thoracoabdominal aortic aneurysms; TEVAR, thoracic endovascular aortic repair; TIA, transient ischemic attack.
Continuous data are presented as the means ± standard deviation; categorical data are given as the counts (percentage).
Spinal Cord Ischemia Prevention
All procedures were performed by a single surgical service (G.S.O.) with a dedicated endovascular team under total intravenous general endotracheal anesthesia using fixed imaging in a hybrid endovascular suite. The anesthetic consisted of propofol and fentanyl or sufentanil infusion at the discretion of the anesthesiologist with avoidance of nondepolarizing muscle relaxants. Succinylcholine was used as the muscle relaxant of choice for induction of anesthesia. A predefined standardized protocol was used to prevent spinal cord ischemia.
Blood Pressure Management
Calcium channel blockers and angiotensin inhibitors were discontinued or decreased in dose a week prior to the operation and up to 4 to 6 weeks after whenever possible. Mean arterial pressure (MAP) was targeted at ≥80 mm Hg intraoperatively and for the first 72 hours after the operation. If there were changes in neuromonitoring detected during the operation or neurological changes observed on postoperative physical examination, MAP goals were incrementally raised up to 100 mm Hg. In addition, transfusion of blood products was indicated in the first 48 hours after the procedure to keep a target hemoglobin ≥10 mg/dL and normal coagulation profile prior to removal of the spinal drain.
Cerebrospinal Fluid Drainage
Routine prophylactic CSF drainage was used in all patients with ≥4-cm stent-graft coverage (or 2 sealing stents) above the celiac axis, which was the minimum extent of coverage used for all type IV TAAAs. Spinal fluid pressure was set in a closed, pressure-controlled system at a baseline of 10 mm Hg. The spinal drain was opened for 15 minutes every hour with a maximum drainage of 20 mL per hour, after which the drain was clamped for the remainder of the hour. If there were changes in neuromonitoring or the neurological examination, CSF pressure was decreased to 5 or 0 mm Hg. CSF pressure was raised to 10 mm Hg once neuromonitoring or the neurological examination improved. Spinal fluid drainage was continued for 24 hours in patients with type IV TAAA and for 48 to 72 hours in those with types I–III TAAAs. The CSF drain was removed in patients who had stable hemodynamics and neurological examination after a 6-hour clamping trial.
Neuromonitoring
Total intravenous anesthesia was used to allow intraoperative neurophysiologic monitoring of MEP and SSEPs. A ≥75% consistent reduction from baseline evoked potential amplitude was considered to be significant (Figure 1). Cadwell Elite machines and Cascade software were used to collect data (Cadwell Laboratories, Kennewick, WA, USA) by electromyography technologists using a technique described in detail elsewhere. 12 In brief, electrical charges sent to the motor cortex through C3/C4 scalp electrodes evoke MEPs through the motor pathway; values are recorded down the cord over multiple muscles in the upper and lower extremities for at least every 10 to 15 minutes. An upper extremity muscle (extensor digitorum communis) is recorded to help differentiate neurogenic impairment such as spinal and lower limb ischemia from nonspecific changes. Bilateral lower extremity muscles are recorded using subdermal electroencephalographic (EEG) electrodes placed in the hamstring, tibialis anterior, and abductor hallucis muscles. In addition, SSEPs consisting of electrical stimulus generated at the ulnar or tibial nerve that travels from the distal extremity are recorded over the neck and scalp. In patients where the lower extremity tibial SSEPs are not present at the ankle, subdermal EEG electrodes can be positioned behind the knee.
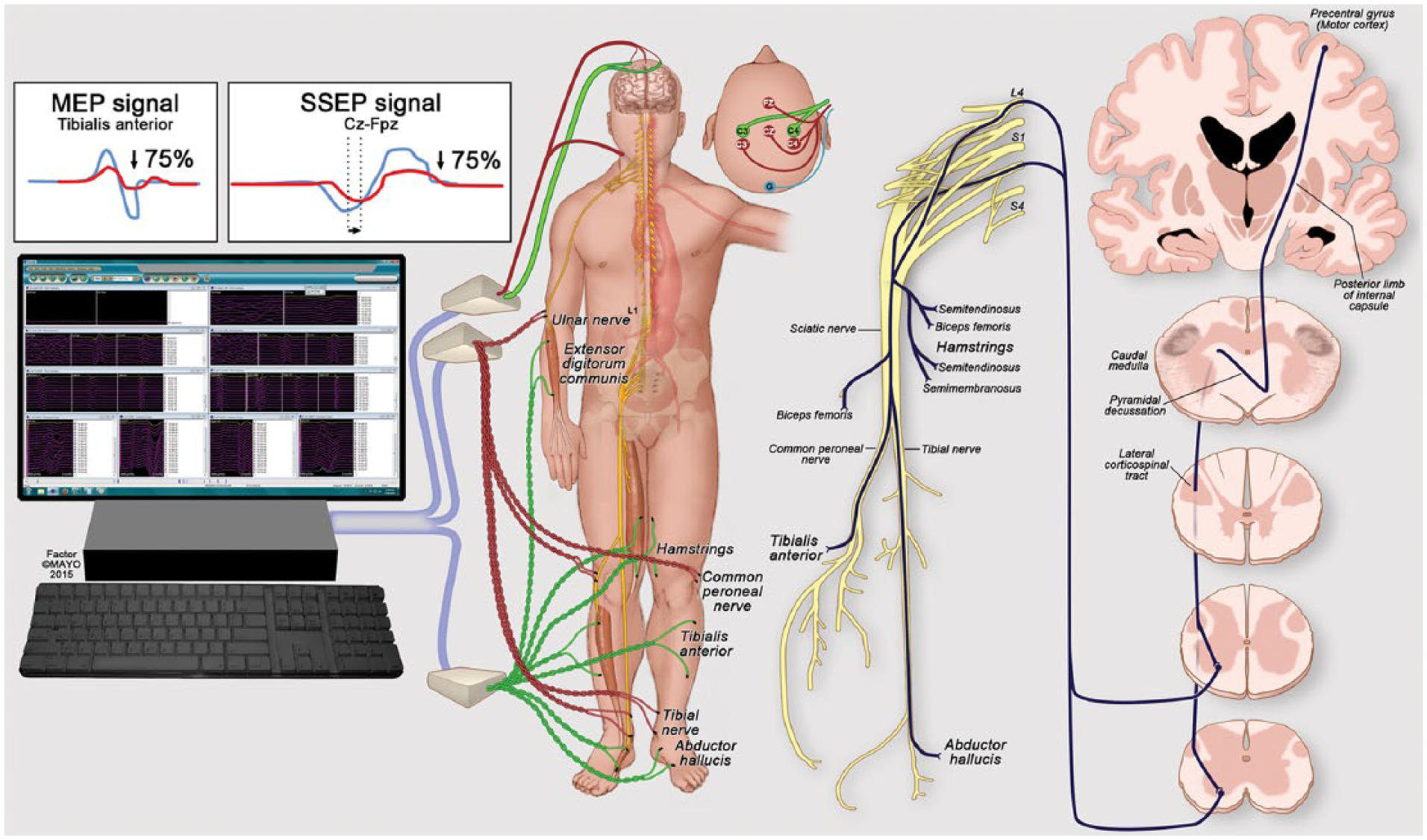
Illustration depicting placement of electrodes for monitoring of motor-evoked potentials (MEPs) and somatosensory-evoked potentials (SSEPs) during complex endovascular aortic repair. A significant change is defined by >75% decline in amplitude in MEPs or SSEPs.
Iliofemoral Conduits
Temporary iliac artery conduits were used in patients with small iliac arteries. A femoral conduit anastomosed end to side to the common femoral artery was indicated selectively to allow restoration of lower extremity flow in patients with challenging anatomy or severe hypogastric, profunda, and femoral artery disease. The use of a femoral conduit minimized lower extremity ischemia during visceral branch stenting by allowing the aortic device sheath to be retracted into the conduit (Figures 2 and 3).
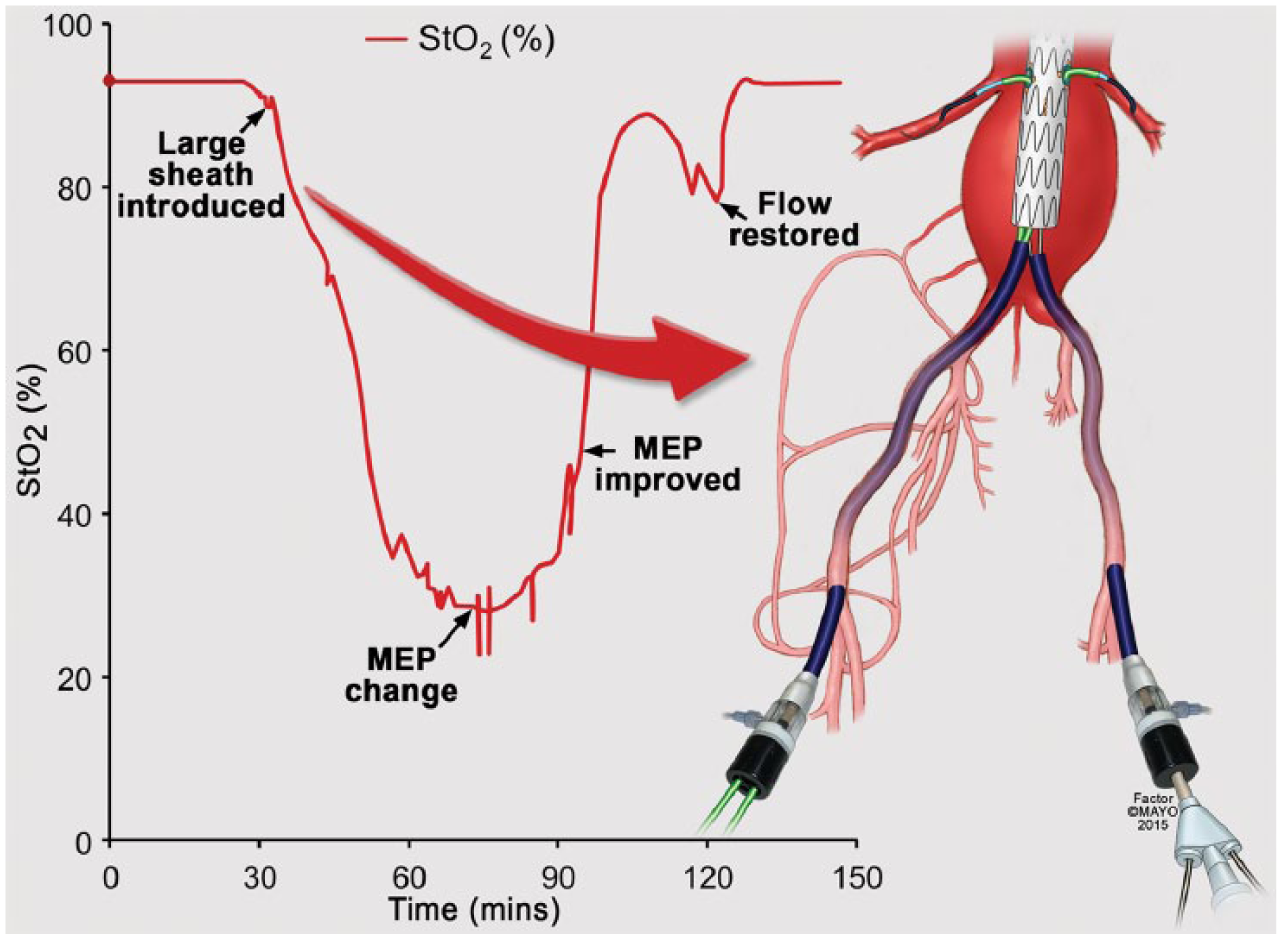
Graph demonstrates the correlation between a decline in lower extremity transcutaneous oxygen saturation (StO2) with placement of large diameter sheaths in the iliofemoral arteries during complex endovascular aortic repair. Note that the drop in StO2 starts immediately after the sheath is introduced, reaching its nadir within 60 minutes. Once changes in motor-evoked potential (MEP) are noted, maneuvers to optimize flow were started. An increase in StO2 and improvement in MEP were then identified. After flow is restored to the lower extremity, StO2 returns to baseline values.
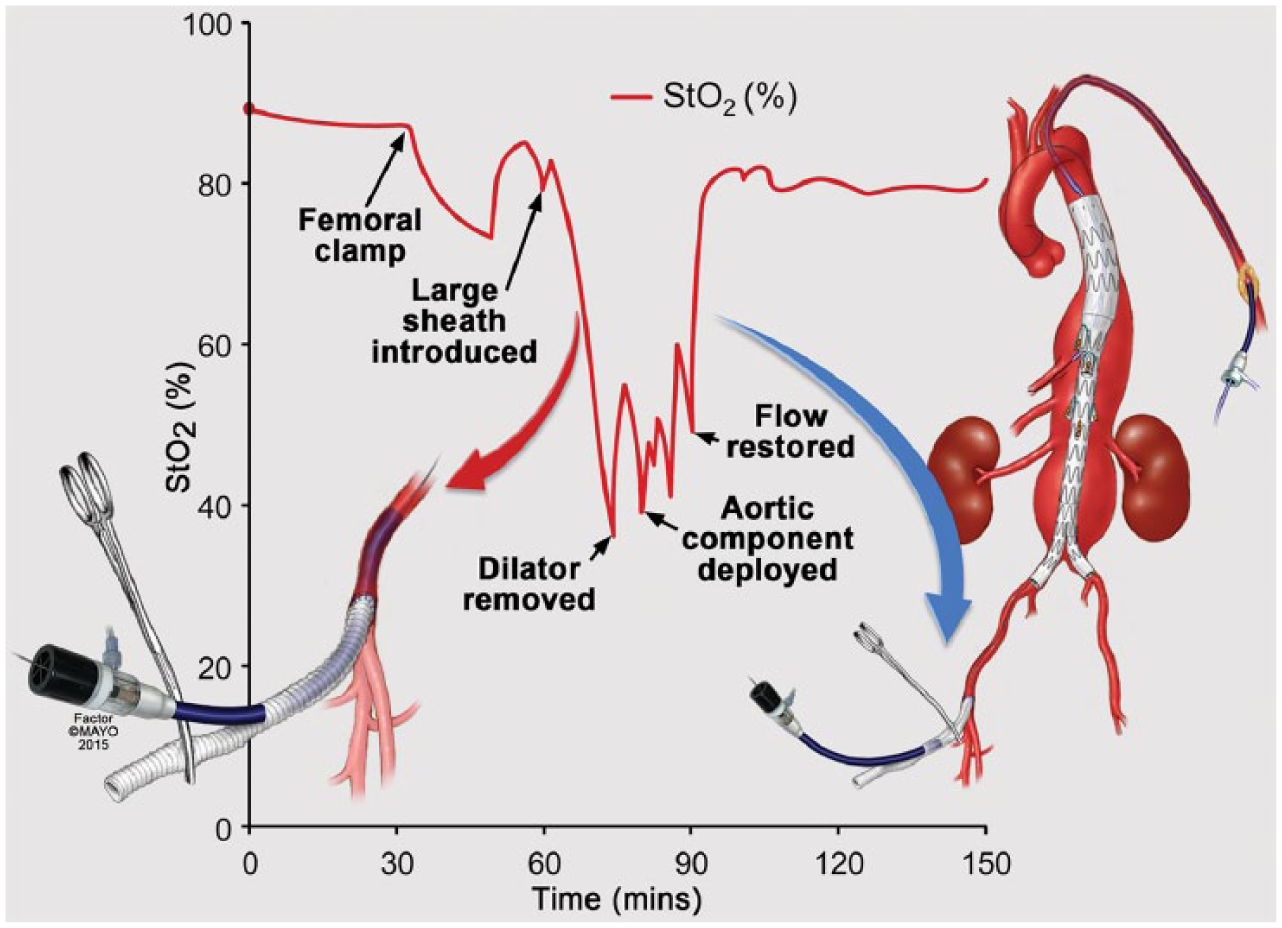
Temporary femoral conduits anastomosed end to side to the common femoral artery were used selectively as an adjunct to optimize lower extremity flow during difficult cases. These conduits were used more frequently in patients with very extensive aneurysms who had severe occlusive disease of the internal iliac and profunda femoris arteries. This graph illustrates the decline in lower extremity transcutaneous oxygen saturation (StO2) with placement of large diameter sheaths in the iliofemoral arteries. After the dilator is retracted to the femoral conduit, StO2 returns to baseline values. In this patient there were no changes observed in neuromonitoring despite the anticipated complex anatomy.
Intraoperative Maneuvers
A decrease in MEP/SSEPs triggered the introduction of sequential standardized maneuvers to optimize lower extremity and spinal cord perfusion (Figure 4), including incremental changes in MAP and CSF pressure as previously described. The MAP was raised from 80 up to 100 mm Hg with norepinephrine and/or vasopressin infusions along with simultaneous decrease in CSF drain pressure from 10 to 5 or 0 mm Hg. Response to these maneuvers was recorded, and the MAP and CSF pressure parameters were readjusted accordingly. In patients with improvement after maneuvers, the procedure was completed in standard fashion. In those with no change or deterioration in neuromonitoring, flow was restored to the pelvis and lower extremities as fast as possible by changing the sequence of target vessel stenting as depicted in Figure 4. In patients with normalization of MEP/SSEPs after lower extremity flow was restored, the procedure was completed. If changes persisted, the procedure was left incomplete with flow into the sac via the celiac branch or contralateral iliac limb whenever possible.
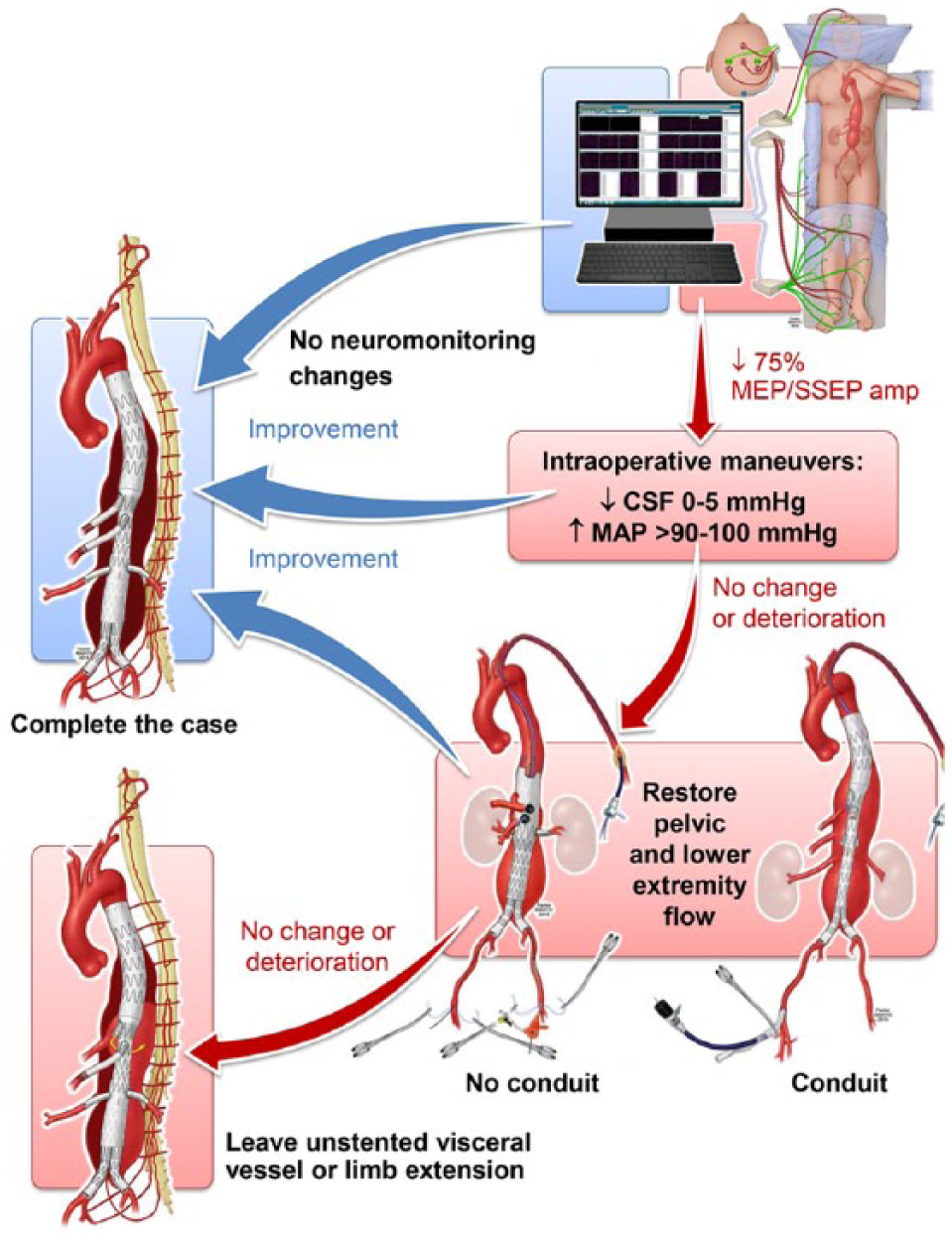
Standardized maneuvers and protocol triggered by changes in motor-evoked potentials (MEPs) and somatosensory-evoked potentials (SSEPs). CSF, cerebrospinal fluid; MAP, mean arterial pressure.
Staged Procedures
A staged endovascular approach was used in all patients with type I or II TAAAs (Figure 5). Two strategies were utilized for staged coverage of the aorta. In 5 patients, sac perfusion was maintained using perfusion branches or via the celiac branch, which was left unstented. Perfusion branches were intentionally occluded or stented in 10 to 14 days, respectively. Since 2012, this technique evolved to sequential aortic coverage using initial placement of thoracic stent-grafts from the proximal landing zone, distal to the subclavian artery, to the celiac axis. This was followed by completion endovascular repair using a patient-specific fenestrated/branched stent-graft 6 to 8 weeks later.
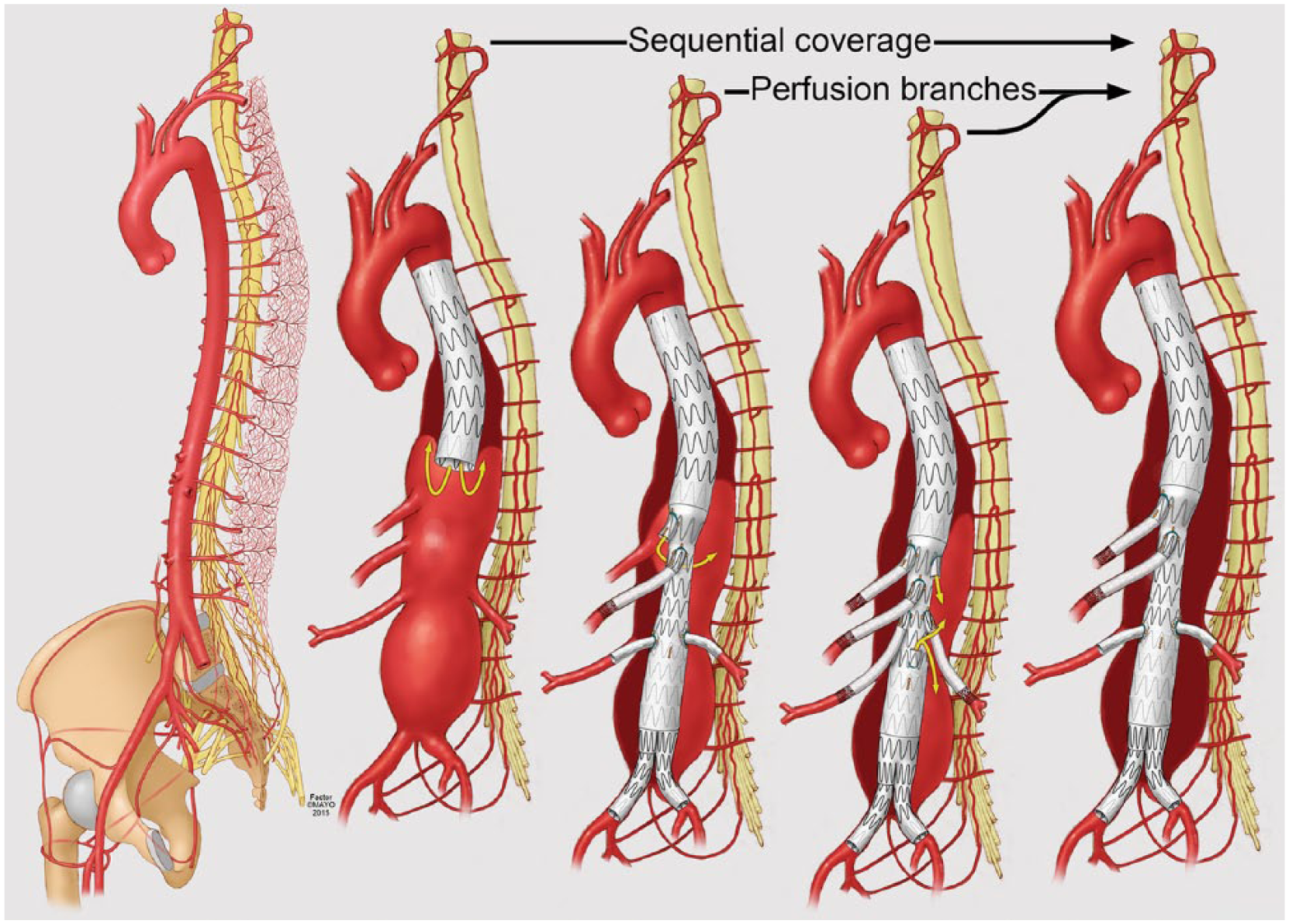
Optimization of the extensive spine collateral network, including vertebral, intercostal, lumbar and hypogastric arteries, forms the basis for staged endovascular repair of complex aneurysms. Strategies include coverage of the proximal thoracic aorta up to the celiac axis, followed by visceral branch stenting in a second stage. Alternatively the sac can be perfused via perfusion branches or unstented celiac axis or contralateral iliac limb. The addition of two perfusion branches is favored by some to improve hemodynamics and avoid hyperpressurization of the sac by single branches.
Statistical Analysis
Data were analyzed using definitions proposed by the Society for Vascular Surgery reporting standards for endovascular abdominal and thoracic aortic repairs. 13 Major adverse events were analyzed using the definition proposed by pivotal studies. 14 To evaluate the impact of changes in MAP and CSF drainage, the recorded changes in amplitude were analyzed, excluding other potential causes of technical concern such as anesthetic medication or artifact. Motor function, SCI, and stroke were assessed using the American Spinal Injury Association and Modified National Institutes of Health Stroke Scales.15,16 All patients with any weakness or symptoms suspicious of SCI had formal neurology consultation. Length of aortic coverage was estimated using centerline of flow measurements (Aquarius iNtuition; TeraRecon, Foster City, CA, USA) to determine the absolute and relative length of aortic coverage from the left subclavian artery to the aortic bifurcation. Results are reported as frequency (percentage) for categorical variables and mean ± standard deviation or median and interquartile range (IQR) for continuous variables. Fisher exact test or Pearson chi-squared test and 2-sample t test were used for comparing groups when appropriate. Univariate and multivariate logistic models were used to predict MEP and SSEP changes by extent of coverage, sheath sizes, and times. A value of p<0.05 indicated statistical significance. Data were analyzed by JMP (version 11-pro; SAS Institute Inc, Cary, NC, USA).
Results
All patients underwent successful endovascular repair under general endotracheal anesthesia. Preoperative CSF drainage was successful in 47 (96%) patients, but despite several attempts it was not possible in 2 patients. Technical success for visceral artery stenting was 98% (160/163), including stenting of 41 celiac axes, 42 superior mesenteric arteries, and 80 renal arteries, with a mean of 3.7±1.0 vessels per patient. In 5 patients with type C DTAs, endovascular repair was performed using commercially available thoracic stent-grafts. Revascularization of the left subclavian artery was performed routinely in 8 patients who required extension of the stent-graft to zone 2.
Temporary iliofemoral conduits were used in 16 limbs of 14 patients. Four patients with small iliac arteries underwent placement of iliac conduits anastomosed to the distal common iliac arteries via a flank retroperitoneal incision. Nine patients had 11 temporary common femoral artery conduits. Total endovascular operating time averaged 175±37 minutes, and total operating time averaged 290±94 minutes. Median blood loss was estimated to be 450 mL (IQR 200–1151 mL).
Neuromonitoring
A stable MEP/SSEP was achieved in all patients. Thirty-one (63%) patients had changes in MEP or SSEP affecting 50 limbs (Figure 6). Of these, 28 (90%) patients had simultaneous decline in MEP and SSEPs. Changes in SSEP and MEP occurred at 62±27 and 77±29 minutes, respectively, after vascular access was obtained. The most common pattern of SSEP changes was signal delay followed by amplitude reduction. All patients with MEP changes had decrease in amplitude, first noted in distal muscle groups. Only 2 (4%) patients had bilateral decline in MEPs at the thigh level. Intraoperative maneuvers restored neuromonitoring signals in 12 (39%) of the 31 patients. Following restoration of lower extremity perfusion, MEPs returned to near baseline values within 5 minutes in all but 1 patient who was found to have immediate SCI. Changes in SSEPs also improved but were partial in 7 patients.
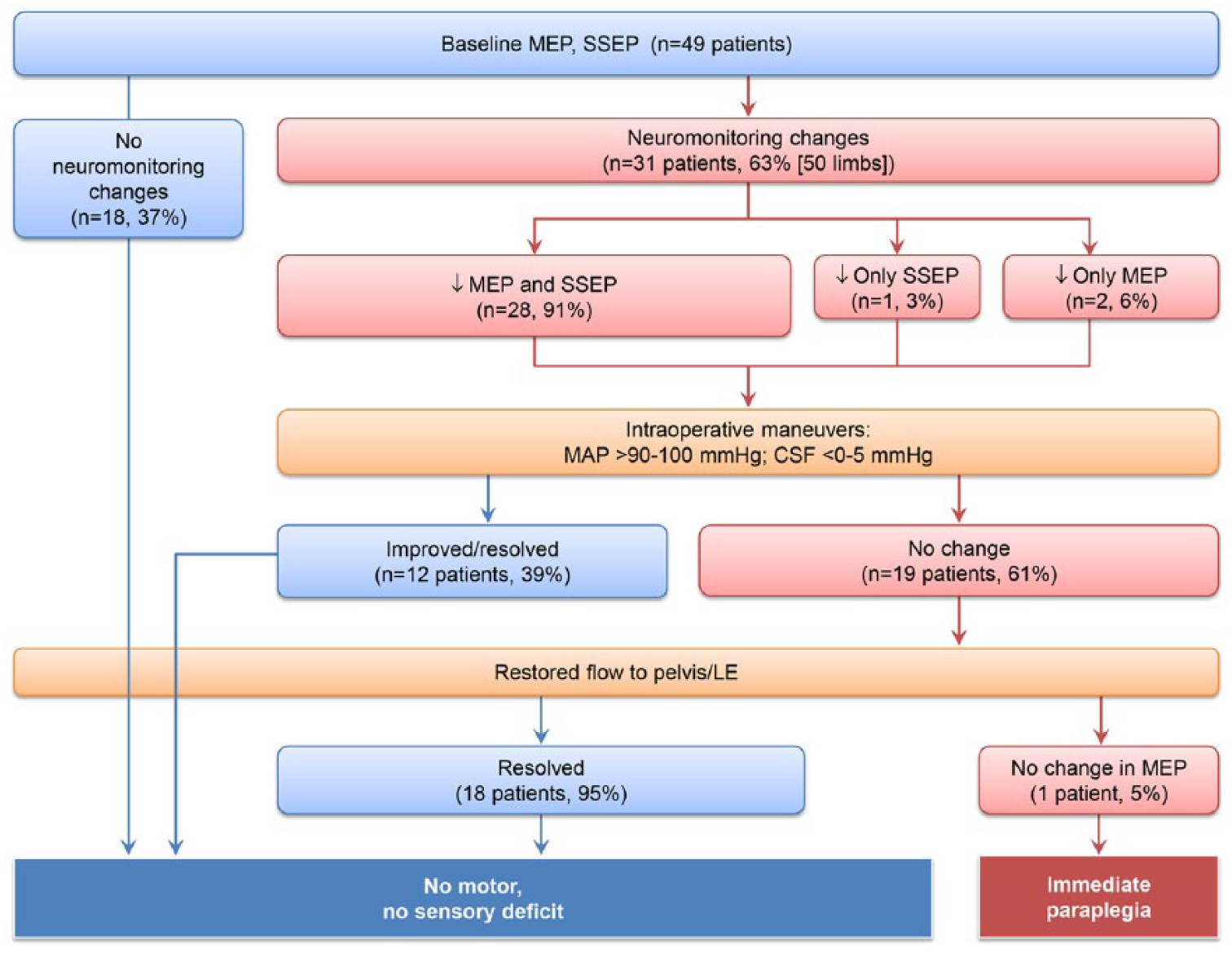
Description of changes in motor-evoked potentials (MEPs) and somatosensory-evoked potentials (SSEPs) during complex endovascular repair in 49 patients. Note changes in MEP and SSEP and response to maneuvers outlined in Figure 4. CSF, cerebrospinal fluid; MAP, mean arterial pressure.
The use of temporary iliac or femoral conduits was associated with faster recovery and shorter duration of changes in neuromonitoring (Figure 3) compared with no use of conduits (Figure 2), but this did not reach statistical significance (38.5±35 vs 86±81 minutes, respectively; p=0.272). By univariate analysis, gender, peripheral artery disease, internal iliac occlusion, prior aortic repair, use of conduits, and extent of aortic coverage were not associated with changes in neuromonitoring. None of the patients who had coverage of the thoracic aorta without visceral branch stenting developed changes in neuromonitoring [0/5 vs 31/44 (70%), p<0.01].
The 2 patients who had changes in thigh MEPs developed SCI. The first patient with type IV TAAA had MEP decline after release of the first 2 proximal sealing stents. At that time, MEP changes were noted despite aneurysm sac perfusion. The second patient treated for type II TAAA developed changes in MEP/SSEP in both lower extremities, which did not respond to maneuvers but reversed to baseline with restoration of lower limb flow. The patient had no evidence of SCI immediately after the operation. Two days after the operation, the patient had a cardiac arrest and was diagnosed with retrograde type A dissection. The patient was resuscitated and underwent emergent open repair of the type A dissection under cardiopulmonary bypass but was noted to be paraplegic after the procedure, which was uneventful with no specific periods of hypotension.
Mortality and Major Adverse Events
There were 2 (4%) 30-day or in-hospital deaths, both in patients treated urgently for symptomatic and ruptured aneurysms (Table 2). The first patient was an 81-year-old high-risk female patient with complicated acute type B dissection, intramural hematoma, and contained ruptured type C DTA. The patient underwent successful proximal coverage of the dissected thoracic aorta and intramural hematoma extending to the celiac axis but had persistent type Ib endoleak via reentry sites into the area of dissection; she died on postoperative day 2 from aortic rupture. The second patient was a 75-year-old high-risk male patient treated using a 4-vessel, physician-modified, fenestrated/branched stent-graft for rapidly enlarging type II TAAA. The patient’s postoperative course was complicated by myocardial infarction and multiple cerebral and cerebral infarcts, likely from atheroembolization from diseased aortic arch.
Early Outcomes in 49 Patients Treated for Descending Thoracic or Thoracoabdominal Aortic Aneurysms. a
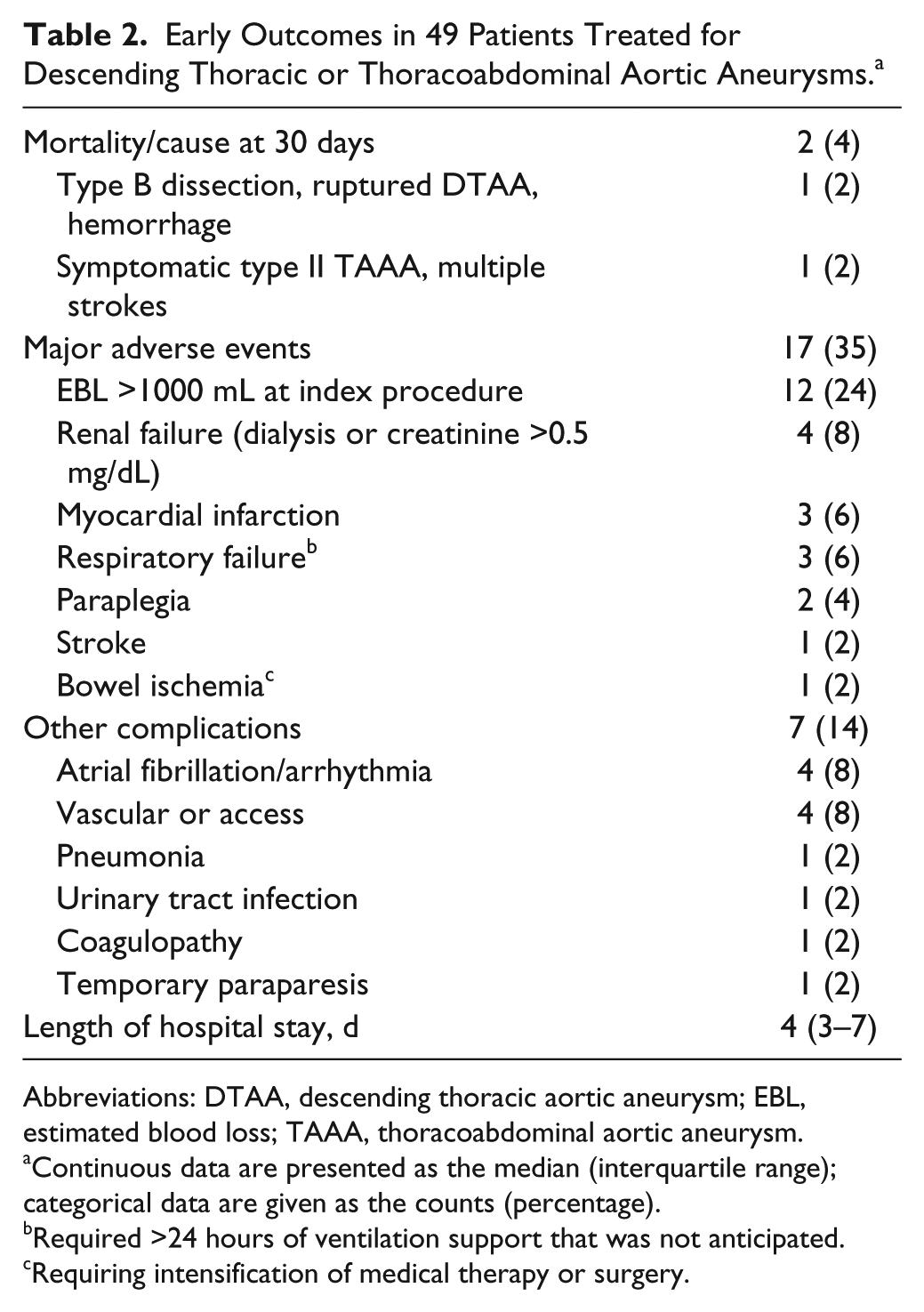
Abbreviations: DTAA, descending thoracic aortic aneurysm; EBL, estimated blood loss; TAAA, thoracoabdominal aortic aneurysm.
Continuous data are presented as the median (interquartile range); categorical data are given as the counts (percentage).
Required >24 hours of ventilation support that was not anticipated.
Requiring intensification of medical therapy or surgery.
Major adverse events occurred in 17 (35%) patients at 30 days; the most common event in 12 (24%) patients was estimated blood loss >1000 mL. Median length of stay was 4 days (IQR 3–7 days). Three (6%) patients developed any SCI, including the 2 patients previously mentioned (Table 3). The first patient who developed immediate paraplegia gradually improved motor function at 3-month follow-up but was diagnosed with advanced small cell lung cancer at 6 months and died from metastatic disease not related to the aortic procedure at 9 months. The second patient who had delayed paraplegia after emergency repair of retrograde type A aortic dissection was dismissed to a rehabilitation center at 25 days but died from aspiration pneumonia 38 days after the initial operation. One additional patient was readmitted on postoperative day 14 with a complaint of bilateral lower extremity weakness after restarting all his antihypertensive medications. The patient had complete resolution of symptoms immediately after placement of a CSF drain, intravenous hydration, and discontinuation of all the antihypertensive drugs. The drain was removed in 24 hours with no recurrent symptoms. There were no other patients with lower extremity weakness or SCI.
Clinical, Anatomical, and Follow-up Data on Patients Who Developed Spinal Cord Injury After Endovascular Repair of Descending Thoracic or Thoracoabdominal Aortic Aneurysms.
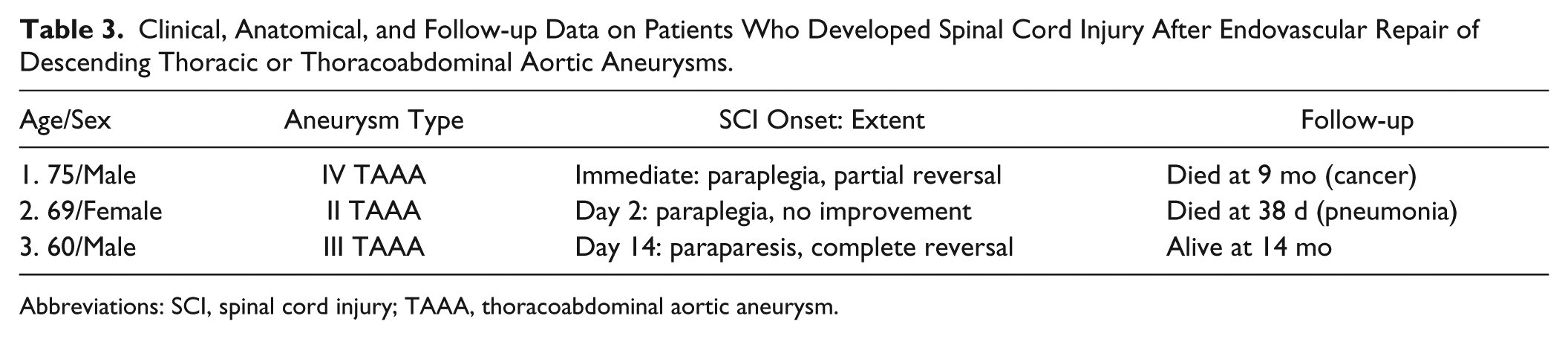
Abbreviations: SCI, spinal cord injury; TAAA, thoracoabdominal aortic aneurysm.
Discussion
Endovascular treatment of thoracoabdominal aneurysms has evolved greatly in the last decade. Improvements in device design, techniques of implantation, adjunctive measures, and better perioperative care have resulted in substantial improvements in morbidity and mortality. 17 Contemporary reports by experienced operators indicate that 30-day mortality ranges from 5% to 9%, which compares favorably to the largest open surgical experiences in centers with thousands of repairs.3,5,17–19 Nonetheless, SCI continues to be the most devastating complication of these procedures, with rates reaching up to 35% in some series. 15 The current study outlines the evolution of our learning experience with a protocol designed to optimize spinal cord perfusion by hemodynamic augmentation, early restoration of pelvic and lower extremity blood flow, and reduction of CSF pressure in response to intraoperative changes in neuromonitoring during complex endovascular aortic repair.
Spinal cord ischemia can result from multiple insults, which may occur in combination or as isolated events.3,5 Although many reports have identified risk factors for SCI, the specific causes have not been well described. Some of the recognized factors are hemodynamic deterioration leading to spinal cord infarction secondary to loss of intercostal arteries coupled with an insufficient collateral network; reperfusion injury and spinal cord edema; and microembolization from catheter or device manipulations. 3 Traditionally, embolization has been considered a relatively uncommon cause. 3 However, since the widespread use of adjunctive measures to improve spinal cord perfusion during open aortic repair (eg, distal perfusion, intercostal reimplantation, hypothermia, and CFS drainage), microembolization has been increasingly recognized as a cause of spinal cord ischemia. 2 Tanaka and associates 2 reported the results of magnetic resonance imaging to evaluate mechanisms of spinal cord injury after aortic repair. In that study, diffuse infarction around the radicularis magna artery, which is consistent with hemodynamic deterioration, was observed in only 20% of patients with injury. The remaining 80% of patients had scattered or focal magnetic resonance imaging lesions corresponding to infarction from microembolization. 2 In our study, it is likely that our single case of immediate spinal cord injury was caused by microemboli, given that the aneurysm sac was perfused and there were no intercostal arteries covered by the stent when the patient developed MEP changes.
The main goal of neuromonitoring is to help identify ischemia in the anterior and lateral spinal columns, which are sensitive to a decrease in oxygen supply. 20 During open TAAA repair, this technique has helped guide selective intercostal artery reimplantation and intraoperative maneuvers designed to improve spinal cord perfusion.8,9 Because signal changes can result from dysfunction in any of the recorded pathways, including the brain, peripheral nerves, receptors, or muscles, as well as technical issues, interpretation requires correlation with the clinical scenario. During endovascular procedures, early detection of these changes may ultimately help identify patients at increased risk of spinal cord injury and in whom hemodynamic deterioration may be prevented or reversed by use of sequential maneuvers designed to optimize spinal cord perfusion pressure (SCPP) by augmentation of MAP and reduction of CSF pressure. These maneuvers raise traditional targets currently applied to endovascular procedures (MAP of 80 mm Hg; CSF pressure of 10 mm Hg or maintaining a SCPP >70 mm Hg) and include early restoration of flow to the pelvis and lower extremities. In this study we found changes in MEP in 63% of our patients, which correlated with prolonged periods of lower extremity ischemia, starting on average 77±29 minutes after iliofemoral access was obtained. These changes returned to normal in all except the single patient who sustained immediate injury. Because the benefit of neuromonitoring was noticed only during procedures associated with longer periods of lower extremity ischemia (>70 minutes) and TEVAR of thoracic aneurysms is often associated with shorter periods, we currently reserve neuromonitoring only for patients undergoing fenestrated and branched incorporation of TAAAs.
Other components of our protocol highlight the importance of preserving and optimizing collateral spinal networks, including use of staged repairs (Figure 5). This is based on experimental and clinical evidence that has challenged the concept that spinal cord perfusion primarily depends on critical segmental arteries, such as the artery of Adamkiewicz. 6 Although unquestionably this artery also plays an important role, the spinal circulation is part of a continuous network that includes vertebral, hypogastric, intercostal, lumbar, and paraspinal arteries.3,5,6 The collateral network spinal pressure corresponds to 75% of the MAP. 21 In experimental studies, coverage or sacrifice of all segmental arteries between T4 and L5 effectively decreases the collateral network pressure to <25% of the MAP for 24 hours, after which it progressively increases to baseline values by 72 to 120 hours. 21 Conversely, staged coverage or sacrifice of segmental arteries is associated with a rapid remodeling process and less pronounced decrease in collateral network pressure, with faster recovery to baseline values. 6
Bischoff and associates 7 reported no spinal cord injury in pigs randomized to staged coverage compared to a 50% rate of paraplegia in pigs treated in a single stage. The Cleveland Clinic group reported recently that internal iliac artery occlusion was an independent predictor of immediate spinal cord injury and lack of recovery, while staged thoracoabdominal aortic repair reduced early mortality and rates of paraplegia.3,4 The benefits of staged repair for TAAA may go beyond the optimization of collaterals. It is possible that a faster, simpler second stage procedure with earlier restoration of pelvic and lower extremity blood flow is associated with improved spinal cord perfusion or that prior stent-graft coverage of the proximal thoracic aorta results in lower rates of microembolization during the second stage procedure. Further clinical experiences and comparison of different strategies of staged aortic repair are needed to confirm these results.
Limitations
Although the clinical data on patients treated by fenestrated/branched endografts was collected prospectively, results of neuromonitoring were reviewed retrospectively, which makes it difficult to accurately assess the timing of changes in evoked potentials relative to specific steps of the procedure. This has been remediated by institution of a prospective protocol. The study included patients with a lower risk of SCI such as thoracic aortic aneurysms, dissections, and patients with type IV TAAAs. A larger study with higher risk groups is needed to validate this protocol. Because our sample size is small and the event rates have been fortunately low, we were not able to analyze predictive factors of spinal cord ischemia in this cohort.
Conclusion
This study outlines a protocol to identify spinal cord and lower extremity ischemia during complex endovascular aortic repair based on neuromonitoring. The experience reflects the evolution of complex aortic repair at our institution, incorporating several concepts, including routine CFS drainage, preservation of collateral networks, selective use of staged coverage, and early restoration of lower extremity blood flow. In this retrospective cohort study, two-thirds of the patients had changes in neuromonitoring, which allowed use of a protocol to optimize spinal cord and lower extremity perfusion by hemodynamic augmentation and reduction of CSF pressure. Although this study does not conclusively determine that our protocol is beneficial, increasing clinical experience may help identify exact mechanisms of SCI and the role of neuromonitoring during complex endovascular repair. Larger clinical experience with higher risk groups (type II TAAA) is needed to evaluate the efficacy of neuromonitoring to prevent SCI during complex endovascular aortic repair.
Footnotes
This work was presented at the 43rd Annual Symposium of the Society for Clinical Vascular Surgery; April 1, 2015, Miami, Florida, USA.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Gustavo S. Oderich is a consultant to W.L. Gore & Associates and Cook Medical (all fees paid to Mayo Clinic) and receives research grants from W.L. Gore & Associates and Cook Medical (all grants paid to Mayo Clinic).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.