
Abstract
Keywords
Introduction
Over the past decade, radial access has been established as a safer access site for coronary interventions. In fact, as compared with femoral access, radial access is associated with a drastic reduction in bleeding risk and, as a result, a reduction in both short- and long-term mortality.1–3 Femoral access is expected to have a higher complication rate in patients with peripheral artery disease. Yet, the limited lengths of currently available guidewires and devices, the reduced support, and the difficulty in advancing long sheaths through the radial artery have hampered the adoption of radial access for peripheral interventions, more specifically, superficial femoral artery (SFA) procedures.
Tibiopedal access may be used as a standalone access in patients unable to tolerate femoral access. 4 However, tibiopedal access is mainly reported in patients with infrapopliteal disease rather than SFA disease, and SFA stenting is rarely reported through the tibiopedal access.5,6 We describe a radial-pedal access strategy, including radial-pedal rendezvous, for revascularization of long total SFA occlusions unsuitable for transfemoral recanalization.
Technique
Patients are selected for this strategy when a duplex ultrasound scan or a prior angiogram suggests a long total SFA occlusion involving multiple segments with absent ostial stump or severely diseased and calcified distal reconstitution. These patients must have ischemia classified as Rutherford category 3 to 6; category 3 patients must have incapacitating symptoms and must have failed a period of conservative management (walking, smoking cessation attempt, cilostazol if appropriate).
Step 1
Blood pressure is checked in both arms to screen for left subclavian artery stenosis. A plethysmo-oximetric Barbeau test is performed at the left radial artery. In the absence of a type D Barbeau result or left subclavian stenosis, the left radial area is prepped. In addition, both groins and the ankle of interest are prepped and draped; note that 1% lidocaine cream is applied over the ankle 30 to 60 minutes prior to the procedure.
Step 2
A left radial access is obtained, and a 6-F, 25-cm Glidesheath (Terumo, Tokyo, Japan) is inserted. A 125-cm pigtail catheter (Performa; Merit Medical, South Jordan, UT, USA) is advanced into the abdominal aorta for aortoiliac angiography (the left subclavian artery often directs the devices toward the descending aorta). Afterward, selective cannulation and imaging of the limb of interest are performed using a 125-cm vertebral or multipurpose catheter (Performa; Merit Medical), which can reach the proximal external iliac artery even in patients who are up to 188 cm in height.
Step 3
Patients with a ≥10-cm SFA occlusion and one of the following conditions are eligible for a tibiopedal access: (1) unfavorable aortoiliac anatomy (prior aortofemoral graft or aortoiliac stent, aortic or iliac aneurysm, or severe tortuosity, calcification, and atherosclerosis with a steep aortoiliac angle); (2) ostial SFA occlusion without any stump (not even a small “nipple”) or blunt SFA occlusion with large bridging collaterals arising at the occlusion site without any stump, while a clear stump is present at the distal reconstitution; or (3) severely diseased, small and calcified distal SFA reconstitution or extension of the occlusion into the distal popliteal artery. Patients without these features undergo a crossover femoral access, which is our first-choice strategy.
Step 4
The anterior tibial artery (ATA) or posterior tibial artery (PTA), whichever is patent, is accessed under ultrasound guidance using a 13-MHz probe with color Doppler capability. If both arteries are patent, the less robust artery is selected for access (should a complication happen, the more robust artery is preserved). A 21-G echogenic needle and a 0.018-inch micropuncture guidewire are used for pedal access (Terumo), followed by the insertion of a 4-F Terumo Precision sheath; ~80 U/kg of unfractionated heparin and 400 µg of nitroglycerin are administered locally through the pedal access. Subsequently, a 0.035-inch angled Navicross catheter and an angled, stiff-shaft Glidewire (Terumo) are advanced through the 4-F Precision sheath. Alternatively, a 0.035-inch Seeker (Bard Peripheral Vascular, Tempe, AZ, USA) or Quickcross (Vascular Solutions, Minneapolis, MN, USA) catheter may be used; however, these catheters do not go through the Precision sheath and are advanced without a sheath.
Step 5
The SFA is crossed retrogradely with the 0.035-inch system, and the common femoral artery (CFA) is cannulated. The selective iliac catheter, which is positioned through the radial access, is used for imaging guidance. If the SFA is crossed subintimally (Figure 1) and reentry into the true lumen at the patent proximal site is not possible, the radial access is used for controlled antegrade-retrograde subintimal tracking (CART). A 6-F, 125-cm multipurpose guiding catheter (Cordis Corporation, Bridgewater, NJ, USA) is advanced through the radial access, followed by advancement of a 260-cm, 0.035-inch, angled, stiff-shaft Glidewire and a 150-cm straight or angled support catheter. The ostium of the SFA is then cannulated from the antegrade direction. Even if no ostial stump is originally present, the retrograde guidewire and dissection plane provide guidance for ostial probing. The antegrade catheter and Glidewire are then advanced in the mid-SFA, overlapping with the retrograde catheter, which often creates a communication between the retrograde subintima and the antegrade plane (rendezvous). The antegrade catheter is then pulled back, and the retrograde devices are pulled back and readvanced into the CFA, intraluminally, through this subintimal communication. If the 2 subintimal planes fail to communicate with catheter advancement, the antegrade radial wire is exchanged for a 0.014- or 0.018-inch guidewire, and a 0.014- or 0.018-inch balloon (150-cm shaft, 4- to 5-mm diameter) is advanced through the radial guiding catheter to dilate the subintima antegradely, overlapping with the retrograde catheter. This allows retrograde wire crossing (reverse CART). A 0.014-inch, 200-cm shaft monorail balloon (Bard Peripheral Vascular) may be used in tall patients to improve distal accessibility.
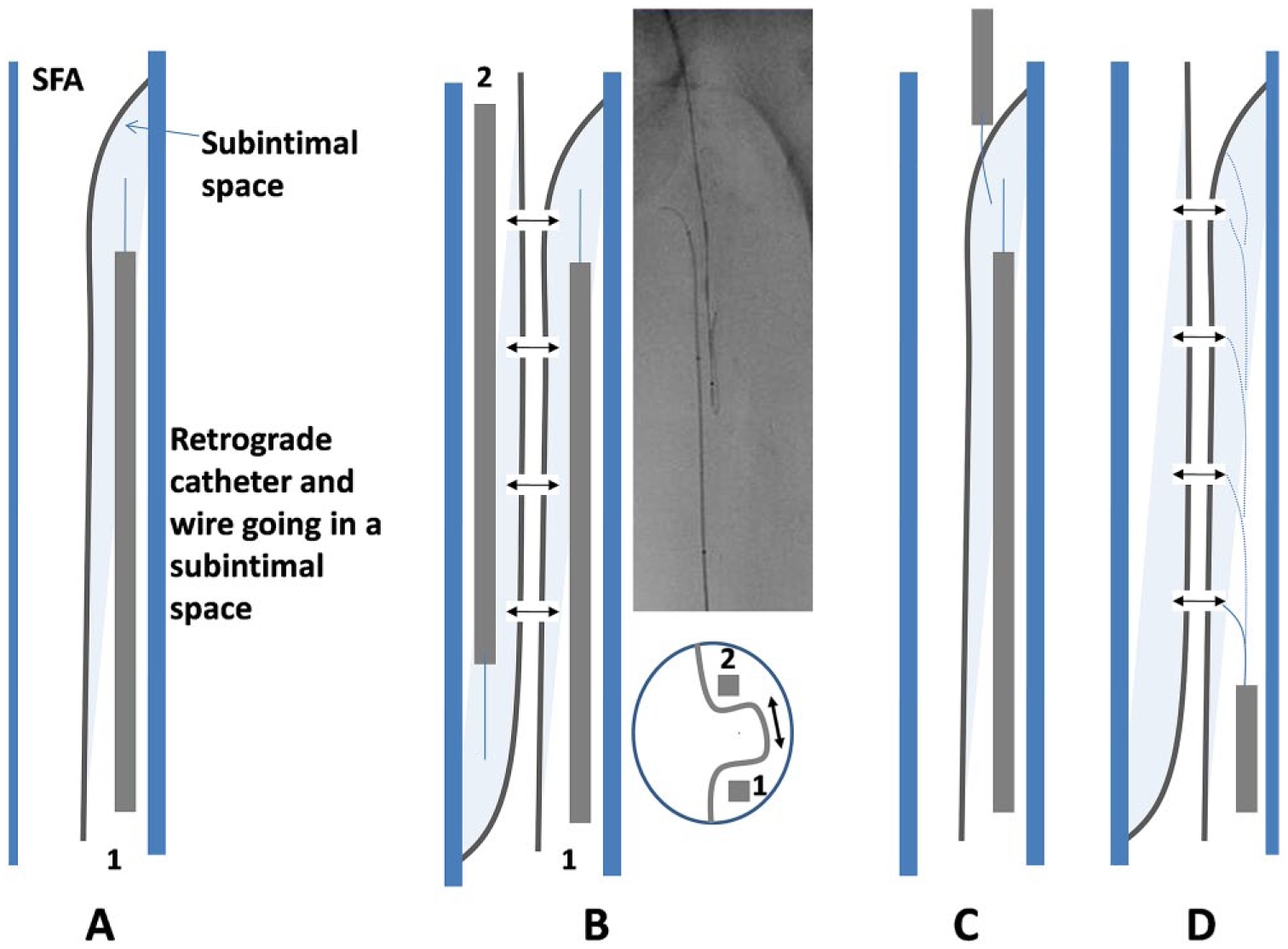
(A) The catheter and guidewire are advanced retrogradely into a subintimal superficial femoral artery (SFA) space (1). (B) Another catheter and guidewire are advanced antegradely through the radial access into another subintimal space (2). With and sometimes without antegrade balloon dilation, the subintimal spaces (1 and 2) communicate at various points (double arrows). The axial cut shows a level where the 2 subintimal spaces communicate. (C) Alternatively, since the radial access provides suboptimal support, the antegrade devices tend to fall into the path of least resistance, which is the retrogradely created subintimal plane. This establishes a communication between the retrograde subintimal space and the common femoral true lumen. (D) The antegrade catheter is pulled back. The retrograde devices are pulled back and reoriented. They eventually fall into one of the communications between the 2 subintimal spaces (interrupted lines) and reach the true lumen of the common femoral artery.
Step 6
After the transtibial Glidewire crosses the SFA into the CFA true lumen, it is exchanged for a long, 300-cm, 0.018-inch guidewire. Between device exchanges, 200 to 400 µg of nitroglycerin is readministered through the Precision sheath. Also, 1000 to 2500 units of heparin are administered locally between exchanges to keep the activated clotting time ≥300 seconds.
The SFA is dilated using 0.018-inch balloons advanced though the 4-F Precision sheath. Residual areas of recoil or dissection are treated with one or more self-expanding stent(s) (generally 6-mm diameter) advanced without a sheath through the pedal access after the 0.018-inch wire is reexchanged for a 0.035-inch wire.
Step 7
In cases where a drug-coated balloon (DCB) is used, the 4-F pedal Precision sheath is exchanged for a 5-F Glidesheath through which the balloon can be advanced.
Step 8
Before pedal sheath removal, retrograde angiography is performed through the sheath to ensure no dissection or thrombosis has occurred across the accessed tibial artery. Hemostasis at the tibial access is achieved immediately at the end of the procedure with gentle manual compression for 10 to 20 minutes or with the use of a transradial band and patent hemostasis for 20 to 60 minutes (Doppler flow is documented below the applied band). After releasing pressure, the pulse downstream of the compressed artery is checked manually and by Doppler.
Clinical Experience
Between March and July 2015, all patients referred to the authors with a long and complex SFA occlusion on ultrasound imaging or prior angiography initially received a left transradial access (17 patients). Fifteen of the 17 patients were found to have the complex angiographic characteristics described earlier under step 3 and eventually underwent a successful tibiopedal access (Table 1). The remaining 2 patients had SFA occlusions without any of the complex features and were treated successfully using a standard transfemoral technique. Three-quarters of the patients had Rutherford category 3 disease (with failure of a trial of conservative management). Four patients had critical limb ischemia: 3 with rest pain and 1 with a 3-cm gangrenous ulcer. The majority of patients had at least 2 of the 3 unfavorable anatomic features, and most patients had an absent ostial SFA stump and a small and diseased distal SFA reconstitution.
Clinical and Angiographic Characteristics of the 15 Patients Undergoing a Radial-Pedal Strategy. a
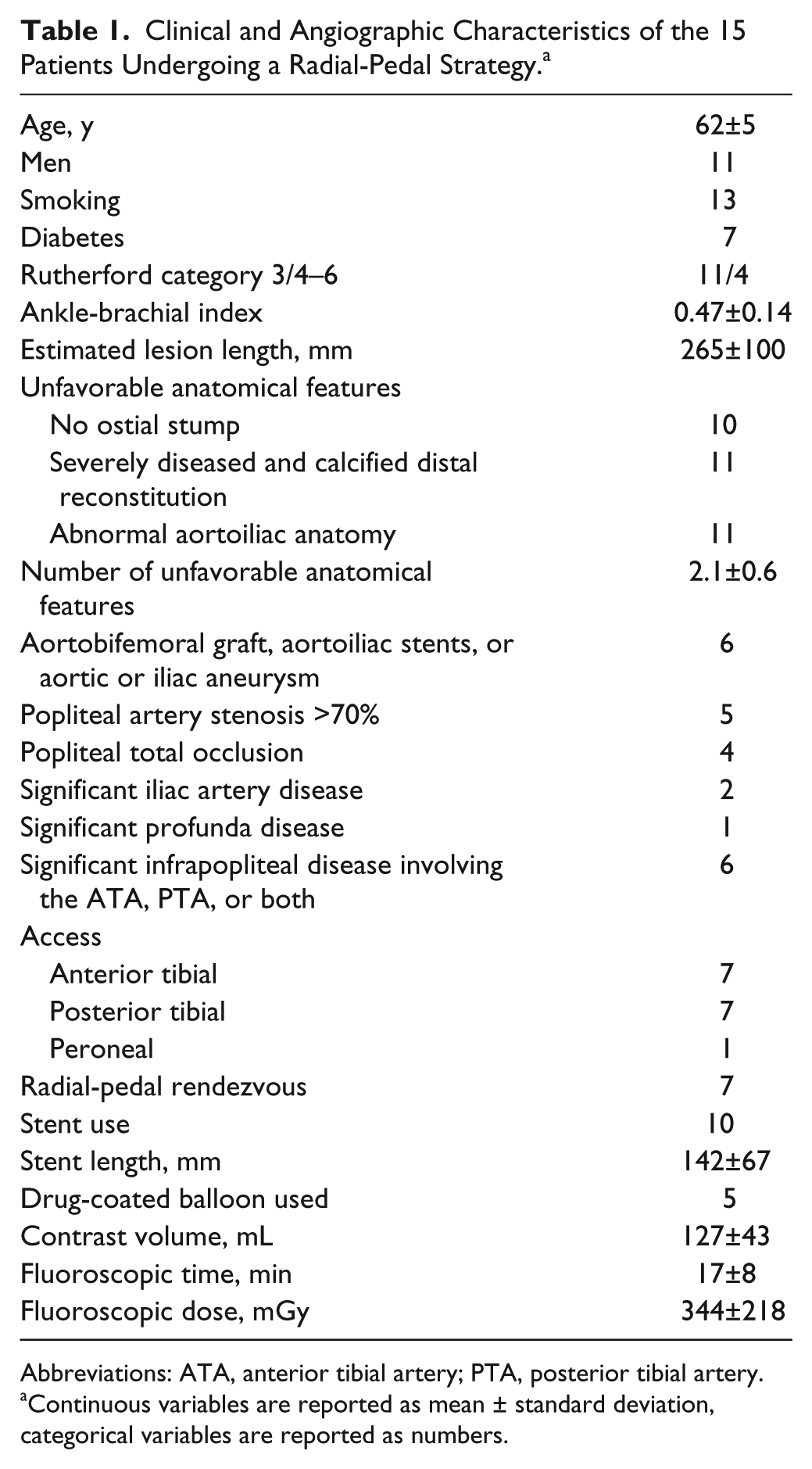
Abbreviations: ATA, anterior tibial artery; PTA, posterior tibial artery.
Continuous variables are reported as mean ± standard deviation, categorical variables are reported as numbers.
Access was immediately successful in 14 patients; 1 patient had initial failure related to tibiopedal spasm and was brought back 1 week later, at which time the tibiopedal access and the recanalization were successful. A radial-pedal subintimal rendezvous was required to cross the SFA in 7 of the 15 patients (Figures 2 and 3), and reverse CART with subintimal angioplasty was required in 3 of those patients (Figure 4). In the remaining 8 patients, the radial access was used for initial imaging and for interventional guidance. Two patients had concomitant external iliac artery stenoses that were stented in the same setting using the radial access. Five patients had concomitant popliteal disease that was treated during the procedure. All procedures were successful with no residual stenosis (≤30%) or flow-limiting dissection, and no access site thrombosis or complication. All patients had palpable pulses across the accessed tibial artery and biphasic or triphasic flow documented by Doppler. Ipsilateral claudication resolved in all patients at 2 to 4 weeks of follow-up. Three-month follow-up was available in 12 of the 15 patients and found them free of recurrent claudication or rest pain; the patient with gangrenous ulcer had full healing of his ulcer.
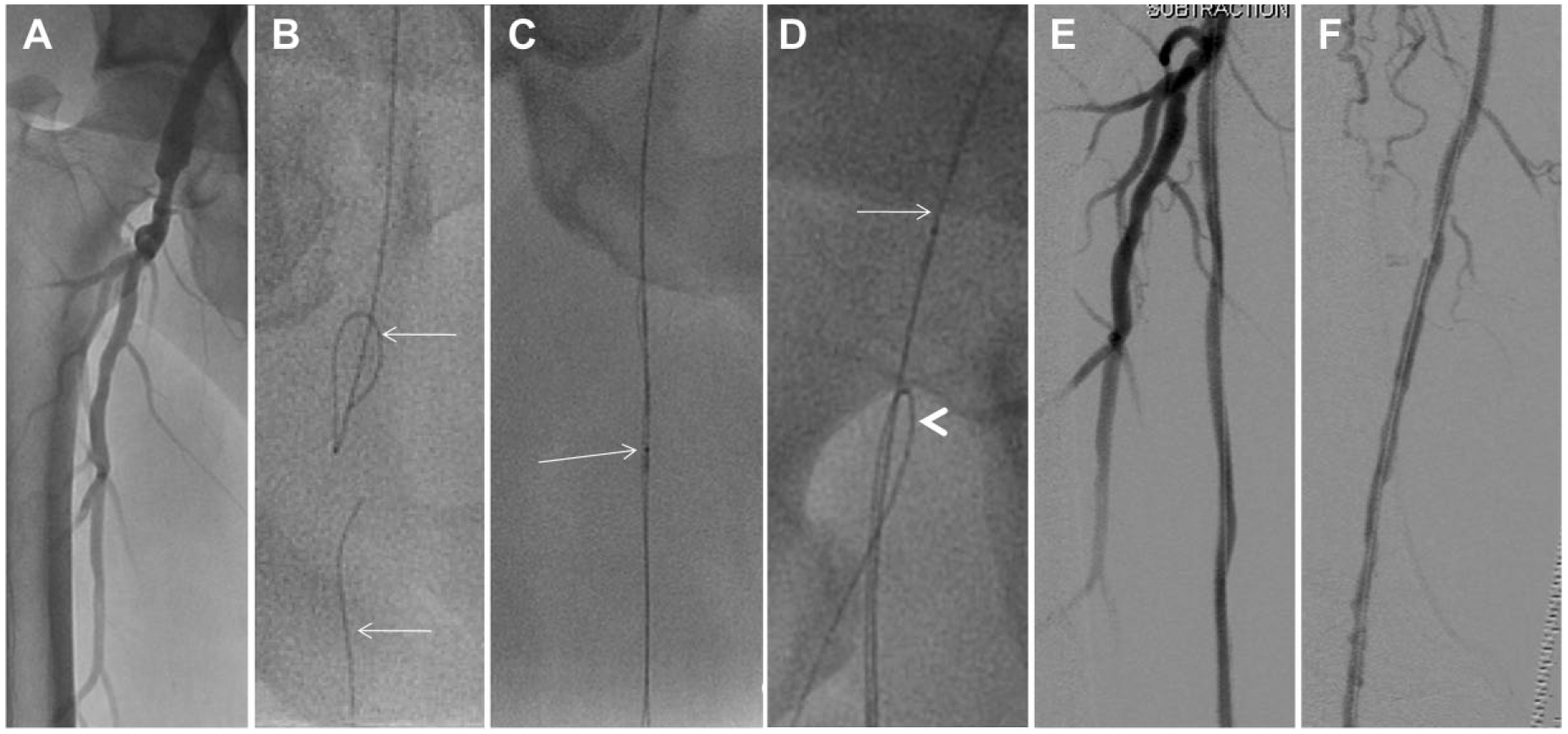
A 53-year-old man, 183 cm in height, presented with lifestyle-limiting claudication of the right limb and uncontrolled diabetes. An aortogram through the left radial access revealed an aortic aneurysm (~3.5 cm), a right common iliac aneurysm (~2 cm), and (A) a long ostial occlusion of the right superficial femoral artery (SFA) without a stump. The anterior tibial artery was used for distal access. (B) A Seeker catheter and a 0.035-inch Glidewire were advanced retrogradely through the SFA occlusion subintimally (lower arrow) without reentry at the distal common femoral artery. Subsequently, a 150-cm Seeker catheter and an angled stiff Glidewire (top arrow) were advanced from a radial access subintimally into the proximal-to-mid SFA. (C) The antegrade and retrograde catheters overlapped (arrow), and the 2 subintimal spaces communicated (rendezvous). (D) The antegrade catheter was pulled back (arrow). The retrograde Glidewire was pulled back then readvanced into the subintimal communication, eventually entering the true lumen of the distal common femoral and the profunda (arrowhead). The SFA was dilated through the tibial access then stented with two 6×150-mm self-expanding stents. (E, F) Final result.
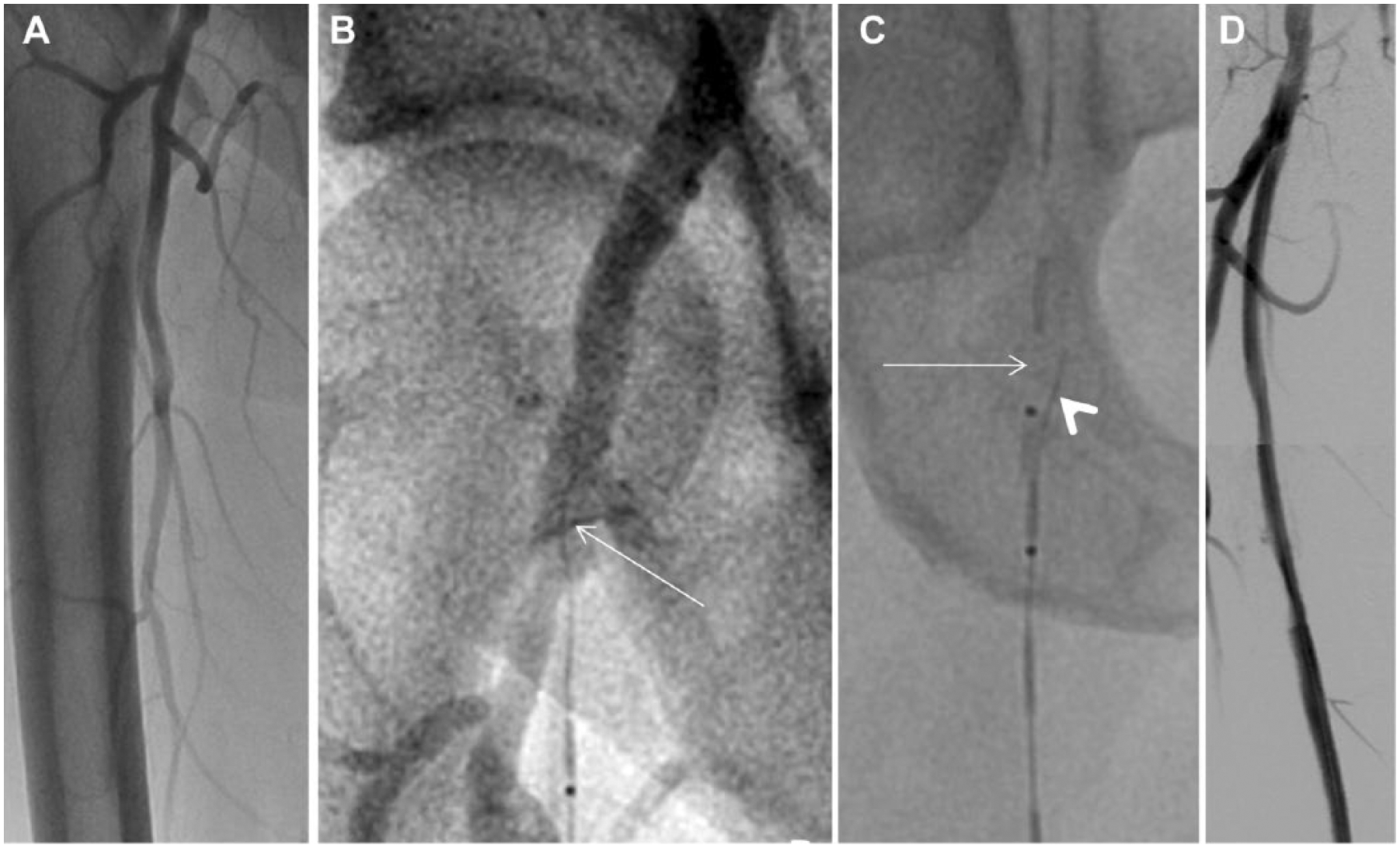
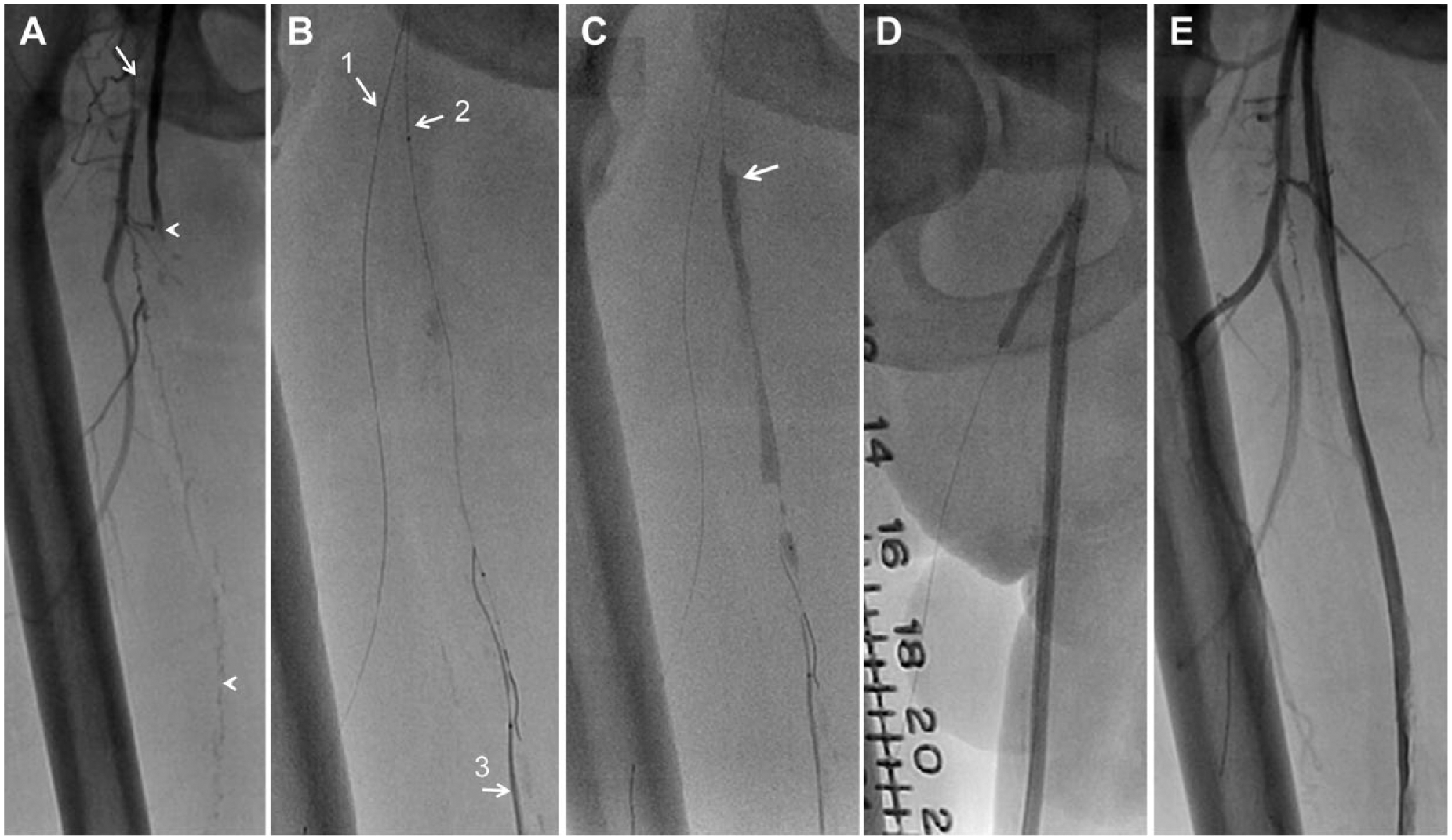
A 67-year-old man presented with severe right limb claudication and uncontrolled diabetes. (A) An angiogram through a left radial access showed a 70% ulcerated right external iliac artery stenosis and a long superficial femoral artery (SFA) ostial occlusion without a clear stump. The SFA reconstitution was heavily diseased and calcified. A 6-F, 125-cm multipurpose guiding catheter was advanced through the radial access and positioned in the right iliac artery. (B) The posterior tibial artery was accessed, and a 0.035-inch Seeker catheter and an angled, stiff-shaft Glidewire were navigated into the SFA. The devices went partially in the subintimal plane (arrow). (C) Through the 6-F multipurpose guiding catheter, a Seeker catheter and a Glidewire were delivered antegradely (arrow) into the proximal-to-mid SFA, subintimally, creating a communication of the 2 subintimal spaces. Afterward, the transtibial Glidewire (arrowhead) was pulled then readvanced, and fell into the true lumen of the common femoral artery. (D) Final angiographic result after proximal angioplasty and mid-to-distal stenting of the SFA through the posterior tibial access.
A 65-year-old man with a history of aortobifemoral bypass presented with right limb rest pain and 3-cm gangrenous ulcer of the anterior shin. (A) An angiogram through a left radial access showed total occlusion of the right profunda (arrow) past the aortofemoral graft (~4 cm ostial occlusion) and proximal SFA occlusion (~30 cm) with a heavily calcified track (arrowheads). The popliteal reconstitution was heavily calcified, and the popliteal artery was occluded at the mid-level. (B) The profunda was crossed transradially using a multipurpose guide, an angled Navicross catheter, and a 0.035-inch straight Glidewire followed by a 0.014-inch wire (arrow 1). Afterward, the anterior tibial artery was accessed. The popliteal and SFA were navigated retrogradely (arrow 3), but the devices went subintimally, so the transradial guiding catheter was used to advance a 0.014-inch Glidewire subintimally into the SFA (arrow 2) in an antegrade fashion. (C) The antegrade subintima was dilated using a 200-cm-shaft, 5×100-mm balloon (arrow), overlapping with the retrograde Navicross catheter, allowing the 2 subintimal planes to communicate. The retrograde Navicross/Glidewire combination was then readvanced from below the balloon inflation site directly into the true common femoral lumen (radial-pedal reverse controlled antegrade retrograde tracking). (D) The SFA was dilated, then kissing balloon dilation was performed of the ostial profunda (through the radial guide) and the ostial SFA (through the tibiopedal access; “radial-pedal kiss”). The popliteal and SFA were dilated using 3 drug-coated balloons. (E) Result across the SFA and profunda.
Discussion
Advantages and Pitfalls of the Transradial Access for Lower Extremity Arterial Interventions
For coronary interventions, the transradial access has been consistently shown to reduce major bleeding and local vascular complications, which has translated into mortality reduction in several studies.1–3 For lower extremity arterial interventions, transradial access has been reported in only a limited fashion for iliac 7 and selected SFA8,9 interventions.
Part of the reluctance to use a radial access is due to the available equipment. A 110-cm sheath is necessary to selectively cannulate the iliac arteries. In our experience, the attempt to advance this long sheath through the radial artery frequently leads to severe spasm and precludes full advancement of the sheath. Even if properly advanced, removal of the sheath may be problematic. Alternatively, a standard 25-cm Glidesheath may be used along with a 125-cm, 6-F multipurpose guiding catheter and is associated with a much lower risk of spasm. The 6-F guiding catheter accommodates 0.035-inch support catheters and 0.014- to 0.018-inch balloon catheters. Yet, despite the guiding catheter support, the long distance between the sheath and the SFA and the sharp subclavian-aortic angle strongly limit the support and pushability of devices through a complex SFA occlusion.
Except in patients with short stature (probably <160 cm), the 150-cm shaft length of the currently available support catheters (eg, Quickcross, Navicross) can reach only the proximal or mid-SFA. The 0.035-inch balloons are available only on 135-cm shafts, which prevent their use in any SFA intervention. The 0.014- and 0.018-inch balloons are available on 150-cm shafts, which limit their use to the proximal or mid-SFA. Longer 0.014-inch balloon shafts are available in the monorail system (200-cm balloon by Bard Peripheral Vascular). However, 0.014-inch wires may not provide enough support from the far away radial access, especially in complex cases. Moreover, bailout stenting, if required, remains problematic as the shaft length of the currently available self-expanding stents is 135 cm. On another note, the currently available guidewires (300 cm) are not long enough to allow easy balloon exchange through the radial artery.
Despite these disadvantages, the left radial access may be used as a standalone access strategy to cross and treat simple SFA lesions with the aid of a 6-F, 125-cm multipurpose guiding catheter and a 0.014-inch, 200-cm-shaft monorail balloon, without the possibility of bailout stenting. For complex SFA occlusions, our strategy is to use the left radial access as a supportive access for crossing and imaging, rather than a primary access for crossing, balloon dilation, or stenting. The short 25-cm Glidesheath is used along with a 6-F, 125-cm multipurpose guide, providing enough support for advancement of wires and support catheters, particularly after having disrupted a fibrotic or calcified SFA through the tibiopedal access. In fact, it is likely that the transradially advanced devices will follow the path of least resistance and probe the same subintimal plane created transtibially, allowing this subintimal plane to communicate with the CFA true lumen.
Advantages of the Tibiopedal Access
The proximal cap of a total SFA occlusion contains higher concentrations of collagen and calcium than the distal cap and frequently has a concave shape (looking from the proximal lumen). 10 Those characteristics tend to deflect the tip of an antegrade wire into the subintimal space; a diseased and calcified distal reconstitution would prevent a subintimal wire from reentering the true lumen. Conversely, the distal cap is softer and convex (looking from the distal lumen), potentially allowing easier retrograde probing with a wire. In addition, the proximity of the tibial artery to the SFA and the relatively straight line to the occlusion provides great support and pushability. Therefore, retrograde crossing of a long SFA occlusion seems a reasonable strategy in a patient with either a totally absent ostial stump or a severely diseased and calcified popliteal reconstitution. Conversely, patients with a robust and noncalcified distal SFA reconstitution who have a patent but diseased proximal SFA are better served by antegrade recanalization through a transfemoral approach: reentry at the distal reconstitution point is facilitated by the robust reconstitution size, while a retrograde transtibial wire will have difficulty reentering the small, diseased proximal SFA (Figure 5).
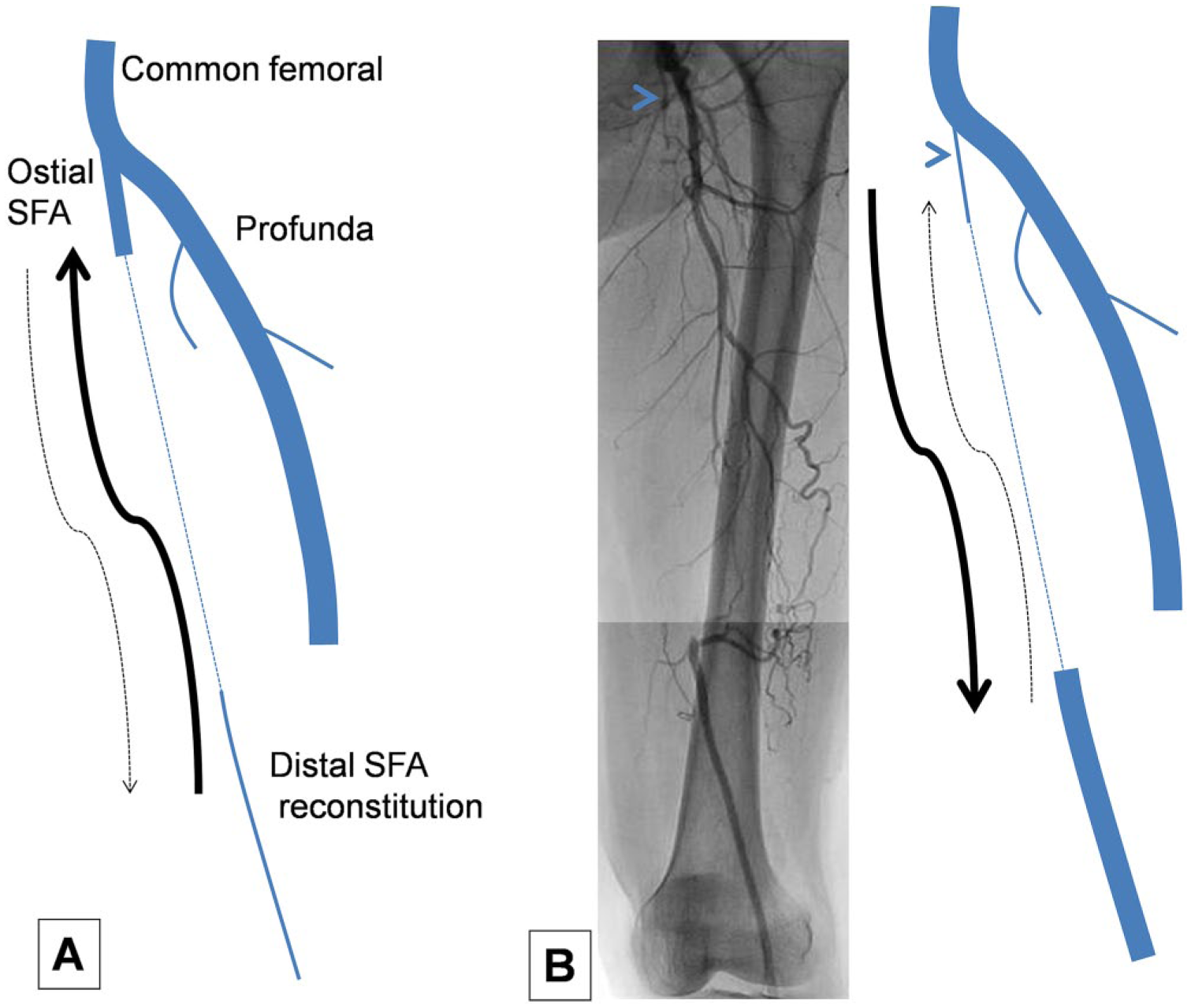
Two different configurations of proximal and distal superficial femoral artery (SFA) reconstitution. The interrupted line represents the occluded SFA. (A) Diseased and small distal SFA reconstitution. After antegrade wire delivery ± subintimal tracking, reentry into the small distal SFA may prove difficult (dashed arrow). Retrograde transtibial recanalization and proximal reentry may prove more successful (solid arrow). (B) Robust distal SFA reconstitution. After antegrade wire delivery ± subintimal tracking, reentry into the distal artery is less difficult (solid arrow). Conversely, retrograde wire navigation and proximal reentry into the small proximal SFA (arrowhead) may prove difficult (dashed arrow).
A popliteal access, which may also be used for retrograde SFA crossing, is not feasible in patients with diseased popliteal reconstitution or SFA occlusion extending into the popliteal artery and is plagued by a high risk of local vascular and bleeding complications (arteriovenous fistula, pseudoaneurysm, popliteal thrombosis with acute limb ischemia, and compartment syndrome).11–13 Multiple series have suggested the safety of a tibiopedal access, making it an attractive revascularization strategy in select patients.4–6,11,14 With the experienced operators of these series, occlusion rates of the accessed tibial artery appeared very low (≤1%).
Advantages of a Combined Radial-Pedal Strategy
Prior studies of tibiopedal access have mainly focused on patients with infrapopliteal rather than SFA disease and have mandated the initial performance of transfemoral angiography. To avoid a femoral access and its inherent risks, we performed the initial angiography through a radial access and then used this access to facilitate SFA crossing and intraprocedural angiography.
The “radial-pedal rendezvous,” or assisted antegrade-retrograde recanalization using the radial access, was successfully used in 7 of our patients. Because of the transradial limitations described above, the transradial catheter and wire are used only to assist recanalization and retrograde reentry, while the procedure is finished through the tibiopedal access (angioplasty and stenting, as needed).
The “radial-pedal kiss,” which is a useful strategy in patients with SFA occlusion and ostial profunda disease, consists of simultaneous kissing balloon dilation of the profunda and the ostial SFA using a transtibially advanced balloon and a transradially advanced balloon (Figure 4).
An additional advantage of our strategy is that concomitant iliac disease may be treated during the same procedure using the radial access.
Caveats and Future Improvements
To achieve a very low complication rate, the tibial access must be performed only by operators experienced in tibial access, preferably ultrasound-guided access. We do not endorse the routine use of tibial access in patients with long SFA occlusions who can undergo transfemoral recanalization. Although our experience and that of other experienced centers suggest the safety of the tibial access, placement of a 4- or 5-F sheath across those small atherosclerotic and calcified arteries (~2–2.5 mm in diameter) may lead to thrombus formation, intimal flaps, and access site occlusion. Moreover, pushing 0.035-inch devices through the tibial artery into a calcified SFA occlusion may be hazardous to the tibial artery and may theoretically lead to intimal tears. Tibial access should be avoided in patients who can reasonably undergo transfemoral recanalization and should be used carefully and selectively in patients without critical limb ischemia.
A limitation of our strategy is the requirement for a 5-F tibiopedal sheath when DCBs are used (high profile). The future availability of smaller-profile DCBs (0.018-inch balloon catheters) may allow advancement of these devices through a 4-F pedal access. Also, the future availability of longer DCB shafts may allow advancement of these devices through the radial access once the SFA has been recanalized transtibially.
The future availability of longer 0.035-inch support catheters, longer 0.018-inch balloon shafts (to be used through the 6-F transradial guide), and longer SFA stent shafts may allow standalone transradial access for some complicated SFA occlusions. Yet, tibiopedal access may still be required in patients with an unfavorable proximal occlusion site or diseased distal reconstitution.
Conclusion
A radial-pedal strategy is a feasible recanalization strategy for long and complex SFA occlusions that are not amenable to transfemoral recanalization. Future availability of long balloon and stent shafts may allow treatment of some complex SFA occlusions through a standalone radial access.
Footnotes
Declaration of Conflicting Interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.