
Abstract
Keywords
Introduction
Critical limb ischemia (CLI), characterized by chronic pain and tissue loss, is an increasingly common problem in elderly individuals. The annual incidence of CLI is 50 to 100 cases per 100,000, and mortality rates are 20% at 6 months after onset. 1 An endovascular strategy for revascularization of the ischemic limb has become increasingly popular 2 and is often used as the first-line approach in preference to open surgery. 3 Endovascular therapy is suitable for multivessel, multilevel revascularization and is well tolerated in CLI patients, who often present with advanced comorbidities. Advancements in endovascular technology and technique have led to high technical success rates; however, failure may occur due to the absence of distal target vessels, severe calcification, and heavy plaque burden that results in elastic recoil and early restenosis after angioplasty. Advanced disease with occlusion of the pedal arteries commonly used for distal bypass or angioplasty targets (the “desert foot”) also represents an end-stage pathology that commonly leads to failure of all conventional revascularization attempts and culminates in major amputation. This is termed no-option CLI (NOP-CLI).
Surgical arterialization of the deep veins to prevent limb loss has been performed since the early 20th century. Halstead and Vaughan 4 were the first to report their early results using healthy arterialized veins of the distal lower limb to deliver oxygenated blood in 1912. Several rationales have been suggested since then to explain the success that may be achieved with venous arterialization, including maximizing tissue perfusion through the capillary bed, improved venous return in the remaining vessels, and increased angiogenesis.5–7
A meta-analysis of 56 studies that evaluated surgical venous arterialization reported 71% limb salvage and 46% secondary patency at 12 months. 8 In addition, most patients avoided major amputation and serious adverse events (SAEs) and experienced successful wound healing and resolution of rest pain. This report concluded that venous arterialization may be considered before major amputation is undertaken in patients with inoperable CLI. A more recent publication compared the efficacy of surgical venous arterialization to conventional distal bypass. 9 In this retrospective study, 19 patients underwent conventional distal arterial bypass and 21 underwent open surgical venous arterialization to the great saphenous vein. Surgical venous arterialization was associated with 71% patency and 53% limb salvage at 12 months, which was comparable to the pedal bypass group (75% and 47%, respectively). Although these studies suggest a role for surgical venous arterialization in patients with NOP-CLI, no known studies have evaluated venous arterialization via percutaneous access in this patient population. This study reports an initial clinical experience with a novel method of totally percutaneous deep venous arterialization (PDVA) used for the treatment of limb-threatening CLI in patients without conventional surgical or endovascular options.
Methods
This prospective, open-label, single-arm study was performed at Changi General Hospital, Singapore, after extensive preliminary benchtop, animal, and cadaveric studies. The inclusion criteria allowed for enrollment of adult patients aged 21 to 100 years with CLI (Rutherford category 5 or 6) who were at risk of major amputation without revascularization, had at least 1 patent tibial vessel as an inflow vessel for PDVA, and had no conventional endovascular or surgical options for revascularization due to lesion recoil despite optimal balloon angioplasty and/or absence of a reasonable target foot vessel for bypass or angioplasty. Exclusion criteria included life expectancy <12 months, active life-threatening infection, aspirin and/or clopidogrel allergy, or contraindication to anticoagulation. All patients had undergone prior attempts at angioplasty. Angiograms were reviewed by at least 2 vascular interventionists, one of whom was not involved in the index procedure before PDVA. The SingHealth Centralised Institutional Review Board approved the study (reference 2013/828/C).
Device Description
The novel PDVA approach to treating CLI described in this report uses an endovascular method (LimFlow, Paris, France) to achieve venous arterialization. The system consists of 4 main components: an arterial catheter with a needle, a venous catheter (Figure 1), a covered nitinol stent in a 7-F delivery system, and an ultrasound alignment system with a laptop computer. The tips of the arterial and venous catheters have an ultrasound-emitting and ultrasound-receiving probe, respectively, which facilitates needle penetration from artery to vein. A nitinol stent is then used to create an arteriovenous fistula (AVF).
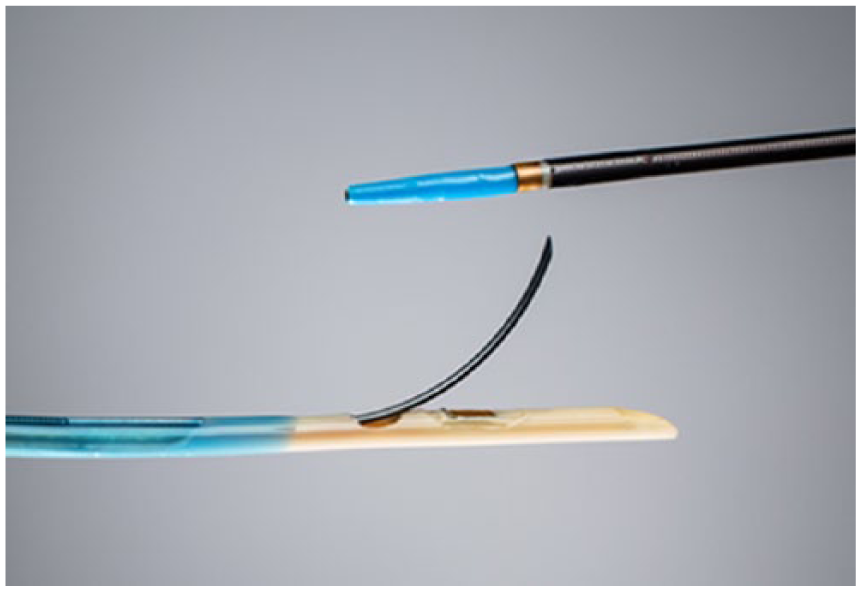
Arterial catheter with needle aligned next to venous catheter. Image courtesy of LimFlow SA.
Procedure
The target inflow vessel was accessed via an antegrade 7-F femoral sheath. A suitable inflow vessel below the knee was selected based on its caliber as well as the affected angiosome. An ultrasound-emitting arterial catheter with an embedded hollow crossing needle was placed over a standard 0.014-inch guidewire using a monorail system.
Venous access was achieved by percutaneous ultrasound-guided puncture of the corresponding target tibial vein near the ankle, chosen based on size and the location of the wound according to the angiosome/venosome concept. The venous catheter was placed over a standard 0.014-inch guidewire via a 5-F sheath in an over-the-wire system. The venous catheter was advanced proximally to the intended point of crossing, which was selected based on simultaneous digital subtraction venography and arteriography (ie, double injection) to determine where both vessels were in closest proximity.
The venous “receive” catheter was initially placed at the selected crossing point. The arterial “send” catheter was then adjusted to achieve optimal alignment between the two as confirmed by maximum peak ultrasound signals. This allowed both catheters to be aligned at the same transverse level with the probes rotated toward each other (Figure 2A). The crossing needle was driven across the artery into the vein (Figure 2B) using the pusher ring at the handle of the arterial catheter. A 0.014-inch Spartacore guidewire (Abbott Vascular, Santa Clara, CA, USA) was then advanced through the needle into the vein.
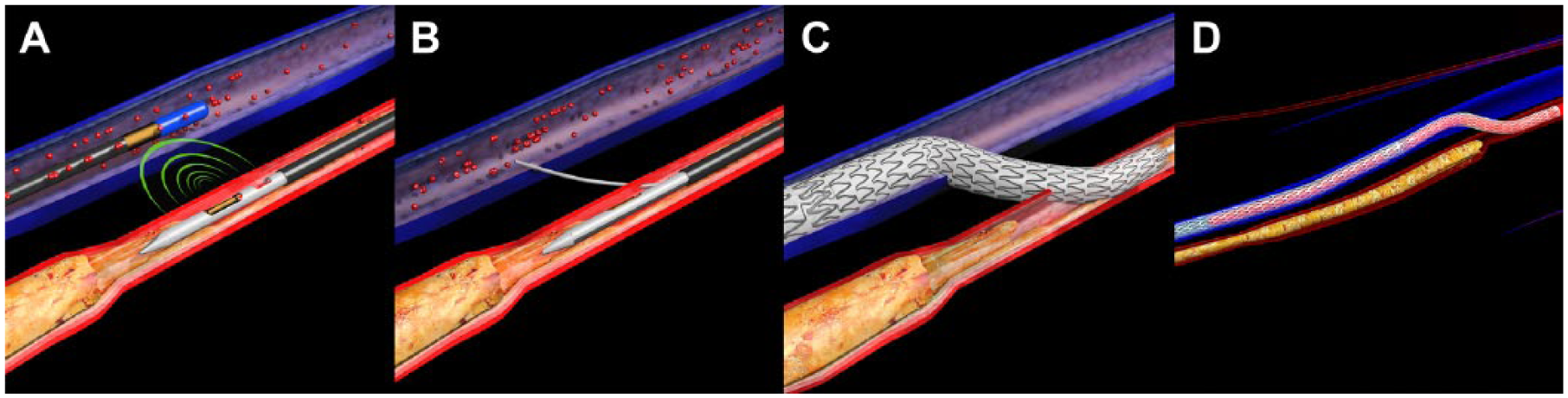
Step-by-step illustration of percutaneous deep vein arterialization. (A) The venous “receive” catheter is initially placed at the selected crossing point, and the arterial “send” catheter transmits a signal to optimally align the devices. (B) The send catheter crossing needle is driven into the vein after the receive catheter is withdrawn. (C) A 0.014-inch guidewire is advanced through the needle into the vein. A self-expanding covered stent is deployed after predilation across the vein and artery. (D) Multiple extension stent-grafts are deployed in the vein down to the ankle to serve as a conduit. Image courtesy of LimFlow SA.
A proprietary, tapered bare metal stent or a self-expanding covered stent (iCAST; Atrium Maquet Getinge Group, Hudson, NH, USA) with diameters of 3.5 mm at the proximal aspect and 5 mm at the distal aspect was deployed after predilation across the vein and artery to create an AVF (Figure 2C). The crossover stent is critical because it prevents leakage at the crossover point and also redirects blood distally, preventing it from immediately following the flow of the normal venous return back to the heart. The crossover stent was extended with multiple 5-mm Viabahn stent-grafts (W. L. Gore & Associates, Flagstaff, AZ, USA) to the ankle to serve as a conduit (Figure 2D). Apart from destroying the valves in the tibial vein by stenting, the reasonably large caliber ensured adequate flow down to the foot. These stent-grafts also covered multiple venous collaterals that could reduce flow to the forefoot.
Ancillary procedures were also performed to render the valves in the foot veins incompetent. Balloon angioplasty was used initially, with interwoven 4-mm nitinol stents (Supera; Abbott Vascular) implanted as needed after suboptimal distal vein angioplasty. Later, a proprietary, over-the-wire, forward-cutting 4-F valvulotome became available, which lysed the valves distal to the extension stents, some as far distal as the midfoot, in contrast to a conventional surgical valvulotome that is pulled rather then pushed.
Assessments
Transcutaneous partial pressure of O2 (TcPO2) at the level of the capillary bed was recorded with the Periflux System 5000 (Perimed, Jarfalla, Sweden) in a room with constant temperature of 24°C; each measurement lasted ~25 minutes. Patients were supine, clinically well, and not on supplementary oxygen. Two readings were taken in every instance, one probe near the wound and another further from the wound. Probes were placed in the same locations at every measurement. TcPO2 values ≥40 mm Hg are predictive of wound healing. 10 TcPO2 measurements were done every 2 weeks for the first 2 months and monthly thereafter until wound healing was achieved or the leg was amputated.
Thermography was performed using an infrared camera (FLIR E30; FLIR Systems, FLIR Systems Co, Ltd, Hong Kong, China) and was interpreted subjectively. Thermography was done before the procedure and not more than 72 hours after the procedure by pointing the infrared camera at the foot in the anteroposterior, medial, and lateral projections. Areas of the foot that were detected as cool were visualized as yellow or blue, while warm areas were orange or red. A reduction in the cool areas by >50% after PDVA was considered an improvement in perfusion. Patient follow-up with duplex ultrasound to measure volume flow rate in particular was performed at 4 to 6 weeks and at 6 and 12 months; examinations were performed more often as clinically necessary.
Patient Enrollment
The study enrolled 7 patients (median age 85 years; 5 women) between September 2013 and November 2014. All patients were diabetic (Table 1); 4 presented with Rutherford category 6 ischemia (including 1 with heel gangrene). Six patients were classified at high risk of amputation based on the Society for Vascular Surgery WIfI (wound, ischemia, and foot infection) classification. 11 Five were treated with the LimFlow procedure and 2 underwent the procedure with off-the-shelf devices before the LimFlow system was developed. The main difference was that an Outback reentry catheter (Cordis Corporation, a Cardinal Health company, Milpitas, CA, USA) was used to puncture an inflated balloon catheter in the target vein after both catheters were visually aligned. Subsequent steps were identical to the LimFlow cases.
Patient and Procedure Characteristics. a
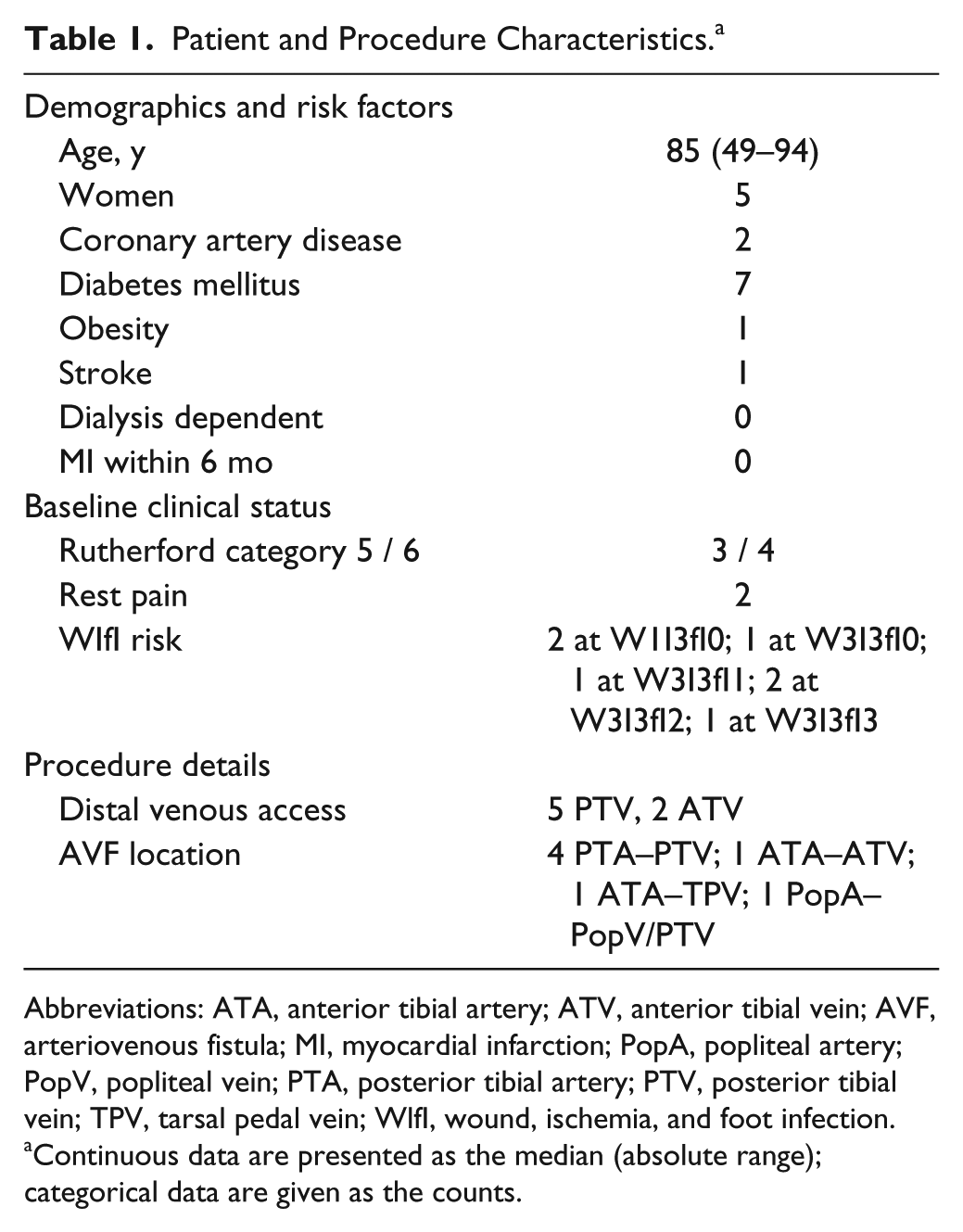
Abbreviations: ATA, anterior tibial artery; ATV, anterior tibial vein; AVF, arteriovenous fistula; MI, myocardial infarction; PopA, popliteal artery; PopV, popliteal vein; PTA, posterior tibial artery; PTV, posterior tibial vein; TPV, tarsal pedal vein; WlfI, wound, ischemia, and foot infection.
Continuous data are presented as the median (absolute range); categorical data are given as the counts.
Outcomes
Safety endpoints were a major adverse limb event (MALE) and major adverse coronary event (MACE) through 30 days and SAEs through 6 months. A MALE was defined as major amputation (transtibial or above) or major vascular reintervention (bypass graft, thrombectomy, or thrombolysis) in the index limb but not including percutaneous reinterventions. A MACE included cardiac-related death, ST-elevation myocardial infarction (MI), or myocardial ischemia confirmed biochemically regardless of the need for percutaneous or open myocardial revascularization. SAE referred to any life-threatening event that resulted in death, persistent or significant disability/incapacity, or required/prolonged inpatient hospitalization.
Secondary objectives were technical success (the ability to position the artery and venous catheters and deploy the stent); clinical improvement (visible formation of granulation tissue, resolution of rest pain, or both) within 6 months; limb oxygenation assessed by TcPO2; amputation-free survival; limb salvage at 1 year; and wound status of the index limb, including time to wound healing (complete epithelialization of the index wound or successful incorporation of a split skin graft) and thermography of the affected limb.
Statistical Analysis
Patient data were collected on standardized case report forms. Device performance was evaluated by the principal investigator and treating physician. Descriptive data are presented as the number for categorical data and the median [interquartile range (IQR)] for continuous data. Differences between TcPO2 levels were compared using the Wilcoxon signed rank test.
Results
Technical success was 100%, with flow to the plantar venous arch achieved in 5 of 7 cases. A tapered bare metal stent was used to create the AVF in 6 of 7 patients. Six patients had prior or simultaneous inflow treatment and received extension stent-grafts. Five patients also had interventions to the foot veins (1 balloon dilation, 3 dilation + stent, and 1 valvulotome + dilation). The immediate angiographic appearance was dramatic (Figure 3A-D). One patient who had prior lumbar sympathectomy and was on high doses of opioids for chronic pain had a dramatic resolution of her pain within 48 hours and was opioid free. Negative pressure therapy was used to augment wound healing in 5 of 7 patients, and split skin grafting was used for wound closure in 3 of 7 patients.
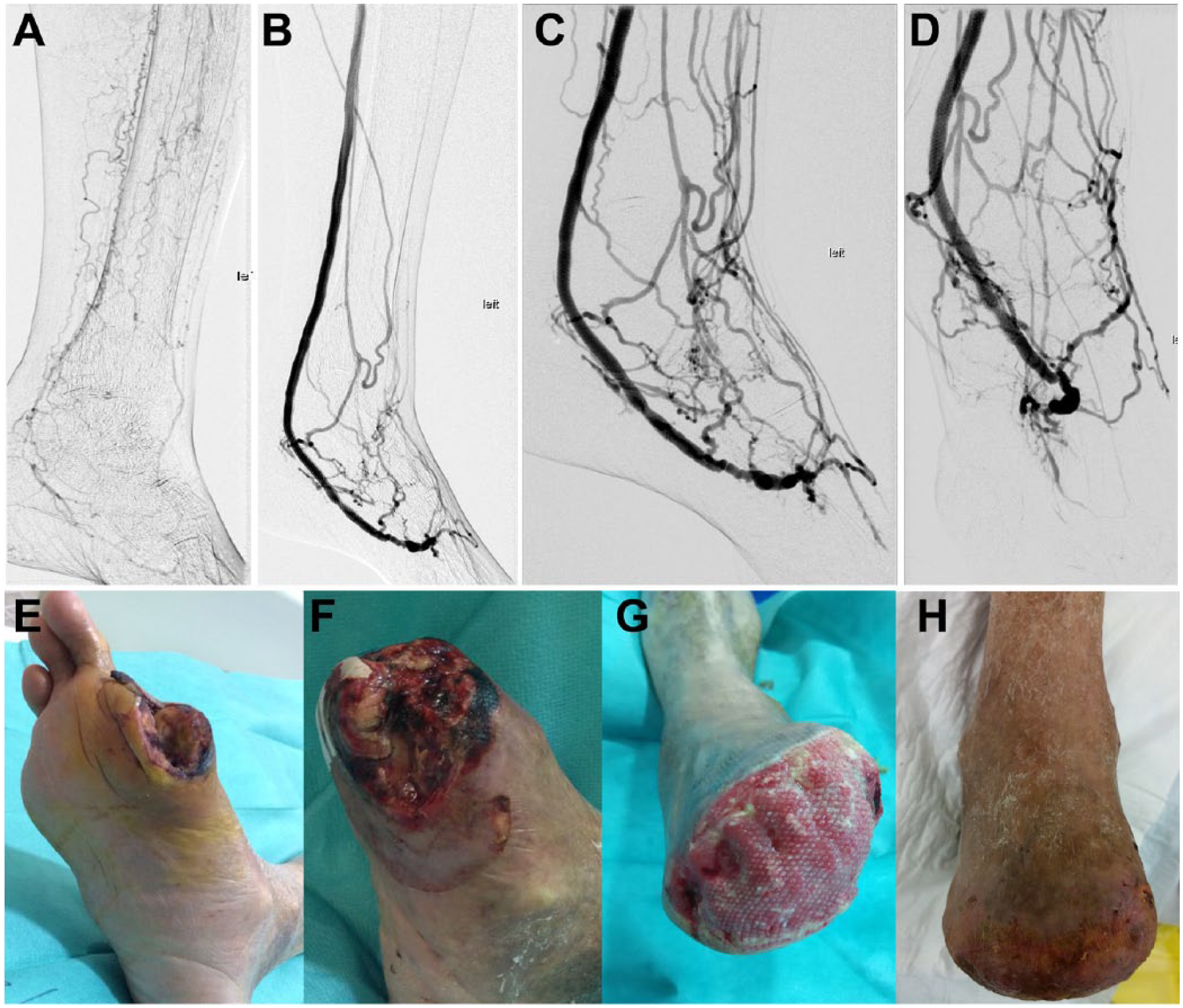
Angiograms before (A) and after (B-D) the procedure (C is magnified lateral, D is magnified anteroposterior). Wound status preoperatively (E) and after forefoot amputation at day 12 (F), day 91 (G), and day 164 (H, fully healed).
No MALE was reported through 30 days, but 2 patients were treated medically for non–ST-elevation MIs. One patient was known to have right coronary artery disease deemed too diffuse for coronary intervention or bypass. There were no perioperative deaths associated with the procedure. Spontaneous retroperitoneal bleeding developed in 1 patient 8 weeks after the procedure, probably from anticoagulation; she was managed conservatively after cessation of the anticoagulation.
Median follow-up was 20 months (IQR 6–32). Clinical improvement was demonstrated in all patients with granulation, resolution of rest pain, or both. Five of 7 patients underwent minor amputation of one or more toes. At 6 months, 4 of 7 patients had achieved complete wound healing (Figure 3E-H) and were symptom free. By 12 months, 5 of 7 patients achieved complete wound healing, with a median healing time of 4.6 months (95% confidence interval 84 to 192). Thermography was also improved in all cases (Figure 4).
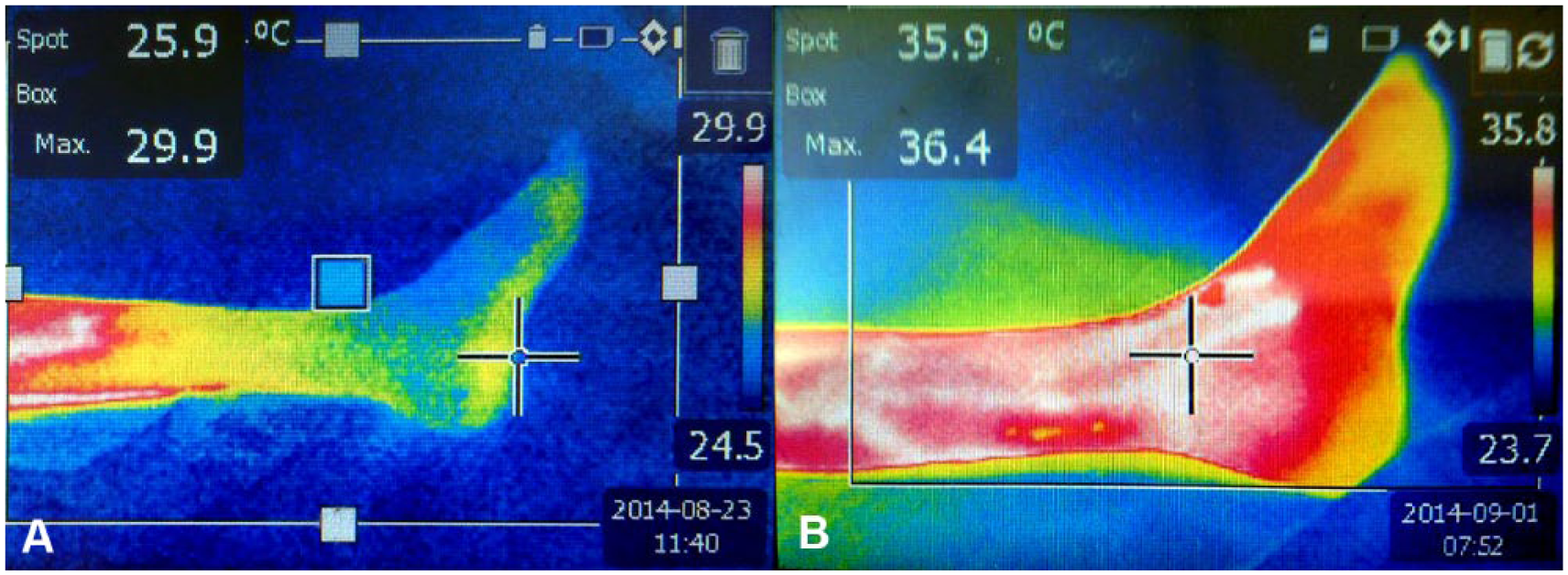
Improvement in thermography before (A) and after (B) percutaneous deep vein arterialization. Cool areas are blue and warm areas are red.
The median time to loss of primary patency was 3.3 months (IQR 1.9–6.8). Reinterventions were performed in 5 of 7 patients to maintain patency; occlusions were addressed using percutaneous mechanical thrombectomy (Rotarex; Straub Medical, Torrance, CA, USA) and drug-coated balloons to reestablish patency.
Two major amputations occurred within 12 months (limb salvage 71%). The first patient presented with Rutherford 6 heel gangrene and osteomyelitis, which was amputated at 61 days postprocedure owing to progressive symptoms of systemic infection. The PDVA was patent at the time of amputation. Bleeding of the heel wound was noted to be good in the preceding debridements. Another patient had severe ischemia with rest pain that resolved after the procedure. The PDVA occluded, and she required an above-knee amputation 7 months after the procedure. There were 3 deaths at 12 months, each unrelated to the device or procedure. Two patients died of pneumonia at 6 and 8 months, respectively. The previously mentioned patient with the above-knee amputation suffered a fatal MI 19 days after the amputation.
Tissue perfusion was recorded in 6 of 7 patients (Figure 5A). The median number of TcPO2 measurements per patient was 13 (IQR 4–17). Median values rose from 8 mm Hg (IQR 3–27) before the procedure to 61 mm Hg (IQR 50–76) after (p=0.046); in 5 of the 6 patients, the value was >40 mm Hg. The TcPO2 levels appeared to rise 2 to 4 weeks after treatment and were mostly >40 mm Hg at 6 to 8 weeks after treatment (Figure 5B). By the time of wound healing in 5 patients, the median TcPO2 was 59 mm Hg (IQR 36–67); 4 of these patients had values >40 mm Hg.
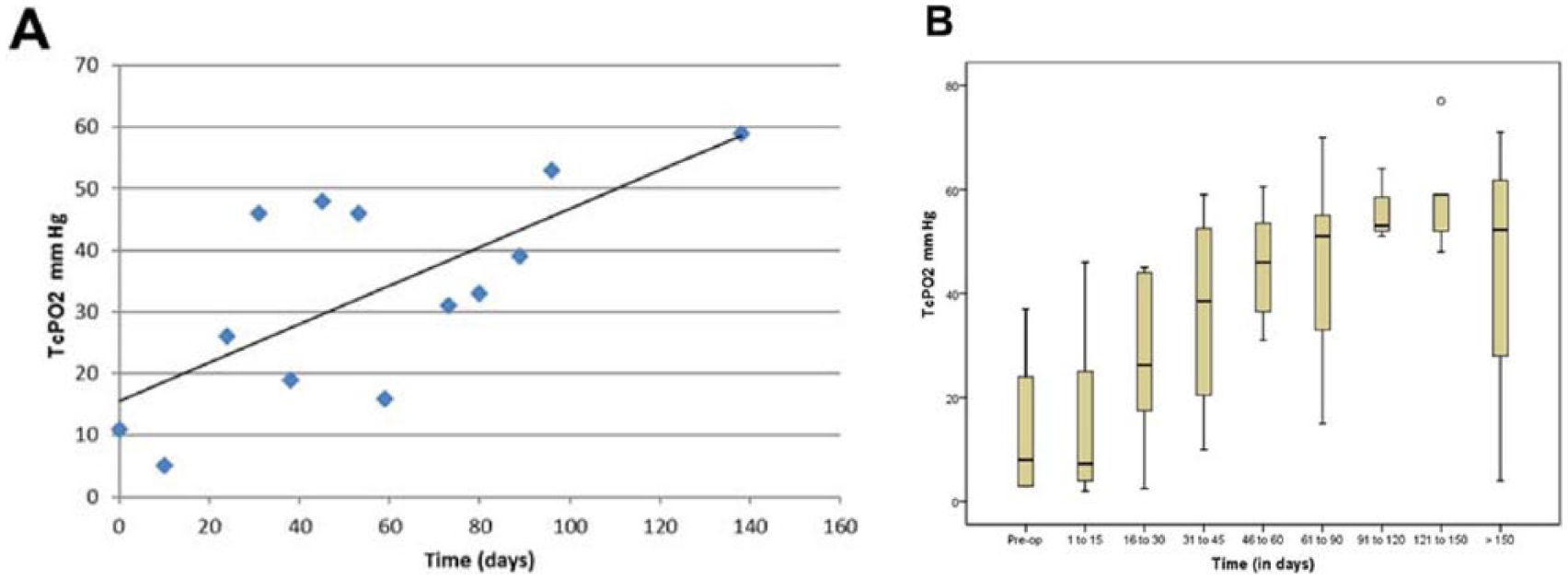
(A) Foot oxygenation against time in 1 patient from the day of the procedure. (B) Box-and-whisker plot of median transcutaneous pressure of oxygen (TcPO2) values of all patients obtained from the probe adjacent to the wound. The top and bottom borders of the box mark the 75th and 25th percentiles, respectively; the horizontal line in the middle is the median. The whiskers are the 90th and 10th percentiles. The circle indicates an outlier.
Discussion
Percutaneous revascularization represents a revolution in the treatment of CLI. Novel techniques have increased the number of limbs being salvaged. However, there are multiple challenges yet to overcome, as well as the lack of alternatives for restenosis in below-the-knee vessels. These shortcomings and better survival from optimization of comorbidities have resulted in an increasing number of patients with NOP-CLI.
Different alternatives have been suggested for these patients, including cell-based therapies, which have shown some promise. 12 Other possible treatments include spinal cord stimulation and sequential pneumatic compression. Some of the earliest reports of surgical proximal venous arterialization by Halstead and Vaughan 4 and Bernheim 13 yielded mixed results. Lengua 14 and Taylor et al 15 reported their experience with distal venous arterializations. More contemporary series of surgical DVA8,9 have been encouraging. The combination of interventional techniques to embolize the venous collaterals or to render valves incompetent16,17 have been employed to improve the results and drive the arterialized blood distally.
To our knowledge, no one has yet reported a totally percutaneous approach to DVA. This pilot study indicates that the procedure is safe; none of the patients experienced perioperative mortality or significant morbidity other than 2 MIs not resulting in any significant sequelae. It is important to understand that these patients were of an advanced age and had multiple cardiovascular comorbidities, some of which were poorly controlled, and multiorgan dysfunction. In every sense, when they presented with NOP-CLI they were also “end-stage” patients with poor organ reserves. It is not surprising that 3 deaths occurred within 12 months despite best medical treatment. A recent meta-analysis of NOP-CLI studies 18 reported mortality ranging between 10% and 54% in the 886 patients; notably, the proportion of diabetic patients in these studies (19%–54%) was lower than in our small cohort (100%), which could have accounted for higher mortality.
All our patients experienced clinical improvement as seen by the formation of granulation; 2 patients even had immediate resolution of rest pain. Most (71%) had achieved complete wound healing and improvement in Rutherford class by 1 year. The loss of 2 target limbs, in our opinion, is not unexpected given that all patients were diabetic and had NOP-CLI. These figures are comparable to a meta-analysis of surgical DVA, 8 in which the foot preservation rate at 1 year was 71%.
One of the outcomes specifically documented was the change in serial TcPO2 measurements, which were systematically performed in a controlled environment. In our opinion, TcPO2 levels represent the best available objective measurement of perfusion, but it can be influenced by swelling and the presence of infection, which may falsely depress the measurements. Conversely, shunting at the arteriole–venule level may not reflect oxygen tension at a cellular level.
The TcPO2 readings increased dramatically in all patients, but it seemed to take >2 months for most of the patients to achieve the >40 mm Hg threshold, which seemed to lag behind clinical improvement. One possibility is that the swelling and edema commonly seen after the procedure may have falsely depressed the TcPO2 levels. In our opinion, a rise in TcPO2 represents an objective improvement in perfusion.
All of our patients experienced some degree of swelling, which was mostly managed conservatively with elevation and occasionally diuresis. Our impression is that the patient should be nursed with leg elevation and off-loading measures if significant swelling is seen. Subsequently, they can be nursed with legs down to allow the hydrostatic pressure to encourage further formation of venous collaterals, somewhat analogous to the maneuvers for the maturation of AVFs created in the arm.
Though the procedure was feasible in our early experience, challenges included the inconsistent vein anatomy, small vein diameters, and valve crossing in particular, which proved surprisingly difficult at times. We used a variety of 0.014-inch and 0.018-inch wires with dedicated support catheters to circumvent the valves. A combination of high-pressure balloon angioplasty and stents was also used as adjuncts to achieve flow to the foot. An over-the-wire reverse valvulotome that allows the operator to push and cut the valves after wire passage is now used routinely, obviating the need for high-pressure balloon angioplasty to address the valves. This represents a less traumatic approach to render the valves incompetent compared with the potentially damaging barotrauma associated with balloon angioplasty, which may ultimately lead to restenosis. In our opinion, the angiographic and clinical success of the procedure relies heavily on these measures to drive blood to the foot. Since these adjunctive interventions to address the valves were not available in the past, the limited success of early surgical series is not surprising.
The use of extension stent-grafts addresses not only the problem of venous bleed-offs via collaterals but also the valves in the calf. It allows a large-caliber shunt and is analogous to a polytetrafluoroethylene surgical bypass to the deep veins. Reintervention for an occluded PDVA was usually due to restenosis distal to the extension stent-grafts. The use of these covered stents made reintervention relatively easy with dedicated pharmaceutical and mechanical thrombectomy devices to clear the thrombus, followed by treating the restenosis in the distal veins. These stent-grafts have also been surveyed with intravascular and transcutaneous ultrasound, documenting nearly full expansion.
Limitations
The small number of patients reported limits the conclusions with regard to the technique’s general applicability. This pilot study, however, seems reasonable to demonstrate safety and feasibility.
Conclusion
PDVA, when applied to a cohort of patients with NOP-CLI, appears to be a safe and feasible procedure. The dual catheters, guided by ultrasound imaging, provide a reliable way to percutaneously create the AVF between a tibial artery and a deep tibial vein. Assisted by a percutaneously introduced valvulotome, arterial blood can now be directed to the veins of the foot. In this small cohort of patients, PDVA appears to be effective in improving limb oxygenation, encouraging wound healing and potentially avoiding major amputation. Although these initial results are promising, they need to be verified in larger studies, though it will remain challenging to prove the concept in this complex group of patients. Wound outcomes will continue to be important in future studies.
Footnotes
Authors’ Note
This technique was presented at the VEITHsymposium (November 19, 2013; New York, NY, USA) and at the Amputation Prevention (AMP) Symposium (August 11–12, 2016; Chicago, IL, USA).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Steven Kum is a consultant to Limflow and has received remuneration for travel expenses and consultancy services. Andrej Schmidt and Roberto Ferraresi are consultants to Limflow and have received remuneration for consultancy services. Yih Kai Tan and Jihad Mustapha are uncompensated consultants to Limflow.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.