
Abstract
Objective:
The comparisons between thoracic endovascular aortic repair for ruptured thoracic aorta (TEVAR) and open surgery (OS) have not been well documented, although both procedures have been widely utilized. We performed a systematic review and meta-analysis to investigate the effectiveness and safety between TEVAR and OS in the repair of ruptured descending thoracic aorta.
Methods:
PubMed, Embase, and Cochrane Library databases were searched to find relevant studies to assess TEVAR and OS outcomes. The comparative parameters were perioperative mortality (30 day/in-hospital), 1 year mortality, paraplegia or paraparesis, renal insufficiency, stroke, pulmonary embolism, re-intervention rate, pulmonary complications, and cardiac complications. A fixed-effects model was applied to calculate the odds ratio (OR) with a 95% confidence interval (CI) on pooled outcomes from different studies.
Results:
Eighteen observational trials involving 2088 patients were evaluated (TEVAR=560; OS=1528). Meta-analysis showed that TEVAR in repairing the ruptured descending thoracic aorta was associated with lower perioperative mortality (OR=0.47; 95% CI: 0.34–0.66; p<0.01), 1 year mortality (OR=0.46; 95% CI: 0.29–0.75; p<0.01), renal insufficiency incidence (OR=0.56; 95% CI: 0.33–0.93; p=0.03), and pulmonary complications (OR=0.69; 95% CI: 0.52–0.92; p=0.01) when compared with OS. There was no significant difference between TEVAR and OS in terms of paraplegia, stroke, pulmonary embolism, cardiac complications, and early re-intervention rates. However, the late re-intervention rate was higher in the TEVAR group than that in the OS group.
Conclusions:
When repairing the ruptured descending thoracic aorta, TEVAR may be performed rapidly and safely. TEVAR is associated with lower rates of perioperative morbidity and early postoperative complications than OS.
Introduction
An acute thoracic aortic rupture consists of a plethora of disease profiles, including thoracic aneurysm ruptures, acute type B dissection, blunt thoracic injury, and progressive penetrating aortic ulcers.1-3 It is generally considered as a life-threatening circumstance, which may lead to a rapid cardiovascular collapse onset. 4 The mortality of patients with thoracic aortic ruptures was approximately as high as 57% to 94% prior to hospitalization.5,6 Immediate open surgical or endovascular intervention is mandatory for survival. Traditional open surgery (OS) primarily consists of thoracotomy and aortic replacement, which often require deep hypothermia, circulatory arrest, systemic heparinization, and sometimes selective cerebral perfusion. It has been documented that OS is effective in controlling active bleeding, although it is associated with high postoperative mortality and morbidity. 7 In 1997, Semba and co-workers first reported thoracic endovascular aortic repair (TEVAR) for thoracic aortic ruptures. 8 In the past 20 years, TEVAR became increasingly popular because of its relatively low invasiveness. 9 TEVAR allows the timely closing of the aortic rupture and helps maintain patient circulation and stability,10,11 though complete bleeding sealing following TEVAR in patients with difficult aortic anatomy has concerning. Although numerous studies have assessed the applications of TEVAR and OS in acute thoracic aortic rupture, the overall safety and efficacy between the two procedures have not been sufficiently investigated.2,12-21 The Society for Vascular Surgery clinical practice guidelines recommend TEVAR as the preferred approach to treat elective descending thoracic aortic aneurysms, and should be the primary method of repair in both elective and emergent settings for isolated lesions of the descending thoracic aorta. 22 There is no consensus on which procedure should be considered as the first treatment choice for ruptured descending thoracic aortas. Therefore, we performed this systematic review and meta-analysis to compare the clinical outcomes between TEVAR and OS in ruptured descending thoracic aortas.
Materials and Methods
Search Strategy
A systematic search of published studies comparing TEVAR and OS in treating acute thoracic aortic ruptures was performed using the databases of PubMed, Embase, and Cochrane Library (from January 2001 to January 2019). A combination of the following relevant medical terms was used along with the MeSH terms “aorta, thoracic,” and “rupture” to search these databases: (1) “stentgraft” OR “endograft”, (2) “open surgery” OR “open repair,” (3) “thoracic aortic,” and (4) “rupture.” All references from retrieved studies were reviewed manually, and subsequently downloaded for consolidation, duplicate elimination, and further analyses.
Study Selection and Data Extraction
We included studies comparing outcomes of TEVAR and OS that discussed at least one outcome of interest, such as patients with descending thoracic aortic rupture due to blunt trauma or no trauma (aortic dissection, aortic aneurysm) requiring intervention. The exclusion criteria were as follows: (1) Lack of open surgical repair cohort comparison (2) Duplicate publications or patient cohorts. (3) Patients who died before arrival at the hospital or in the emergency department. The systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement standards. 23 A standard form was used to extract the data from all relevant articles, including study design characteristics, study population, demographics, intervention type, related mortality (perioperative mortality (in-hospital or within 30 days) and 1 year mortality), and early complications including paraplegia or paraparesis, stroke, pulmonary embolism, pulmonary complications (including pneumonia, acute respiratory distress syndrome, and respiratory failure), cardiac complications (including arrhythmias, myocardial infarction, and cardiac arrest) and re-intervention rates. The re-intervention in our study (within the total follow-up time) was divided into early re-intervention (we define the following statements as perioperative re-intervention: postoperative re-interventions during hospital and re-interventions within postoperative 30 days; in addition, to distinguish it from late intervention, perioperative re-intervention also described as “early intervention” in this study) and late re-intervention (from hospital discharge to 3 years). In the TEVAR group, aortic re-interventions were required during follow-up because of type one endoleak, migration, aortoesophageal fistula, and aneurysmal dilatation of the thoracic aorta. In the open surgery group, aortic re-interventions were required during follow-up to repair a distal anastomosis leak and evacuate an abscess around the aortic graft. All data were extracted and verified by two independent investigators, and any disagreements were resolved by reaching a consensus with a third investigator.
Statistical Analyses
We conducted a meta-analysis of the summary statistics from all individual studies. All analyses were performed using the Review Manager, version 5.3 (available from http://tech.cochrane.org/Revman). For each study, pooled odds ratios (ORs), with a 95% confidence interval (CI), were calculated to compare the outcomes between TEVAR and OS groups. The mean difference (MD), with a 95% CI, was applied to all continuous variables. Between-study heterogeneity was analyzed by means of the I2 index, with values in the order of 25%, 50%, and 75% considered as low, moderate, and high, respectively. A funnel plot asymmetry was assessed mathematically using an adjusted rank-correlation Begg and Mazumder test.
Results
Study Selection and Characteristics
The search was carried out from literature written in English. Initially, a total of 3821 publications were identified. After eliminating any duplicated studies, 2618 reports were subsequently selected for further analyses. The title and abstract of all selected publication were reviewed, leading to an exclusion of 2491 articles. The full text of the remaining 124 studies was retrieved and thoroughly analyzed, which further excluded 106 publications. In total, 18 original papers were enrolled for further analyses (Table 1, Figure 1).
Patients’ Baseline Characteristics and Description Included in Each Study.
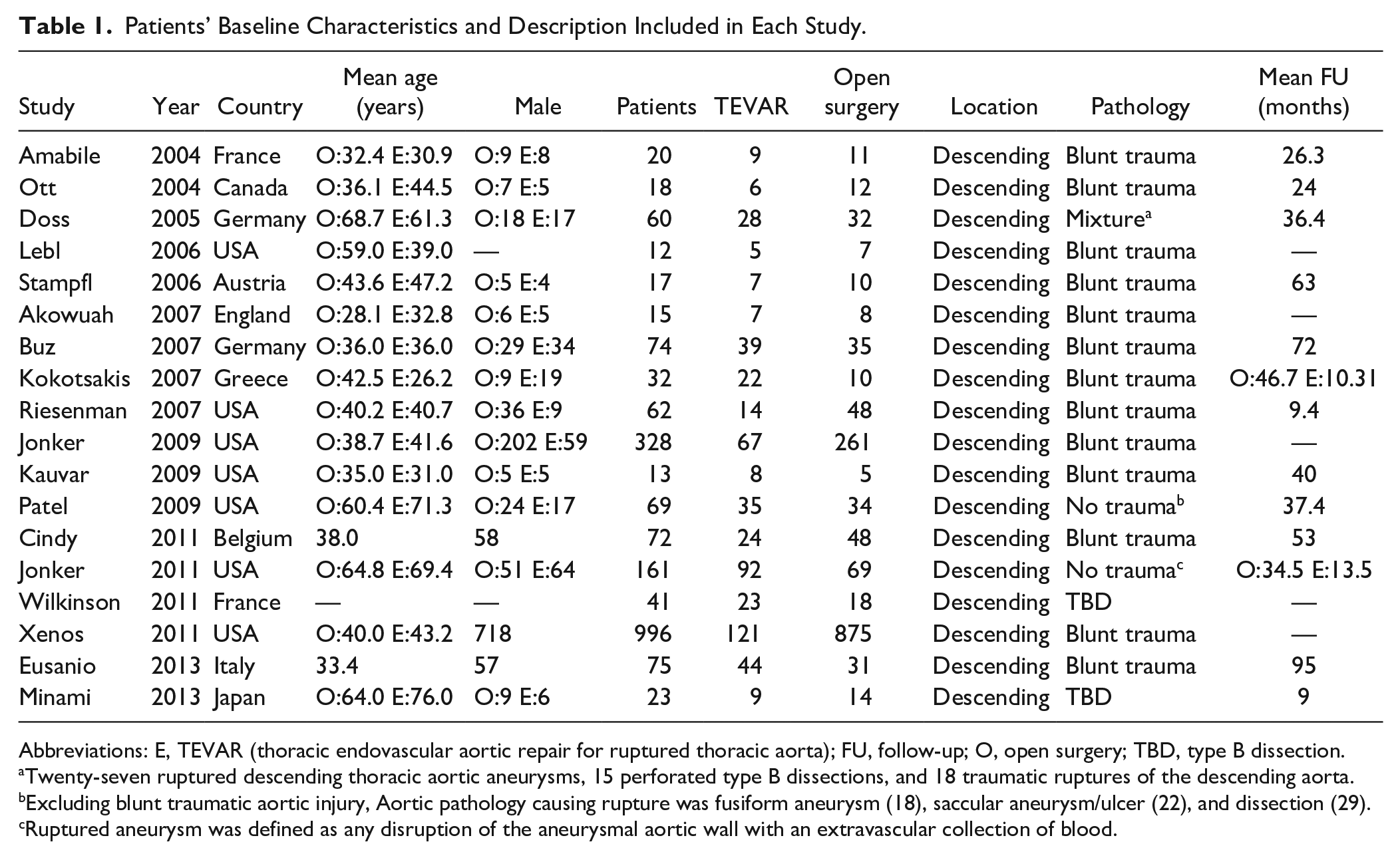
Abbreviations: E, TEVAR (thoracic endovascular aortic repair for ruptured thoracic aorta); FU, follow-up; O, open surgery; TBD, type B dissection.
Twenty-seven ruptured descending thoracic aortic aneurysms, 15 perforated type B dissections, and 18 traumatic ruptures of the descending aorta.
Excluding blunt traumatic aortic injury, Aortic pathology causing rupture was fusiform aneurysm (18), saccular aneurysm/ulcer (22), and dissection (29).
Ruptured aneurysm was defined as any disruption of the aneurysmal aortic wall with an extravascular collection of blood.
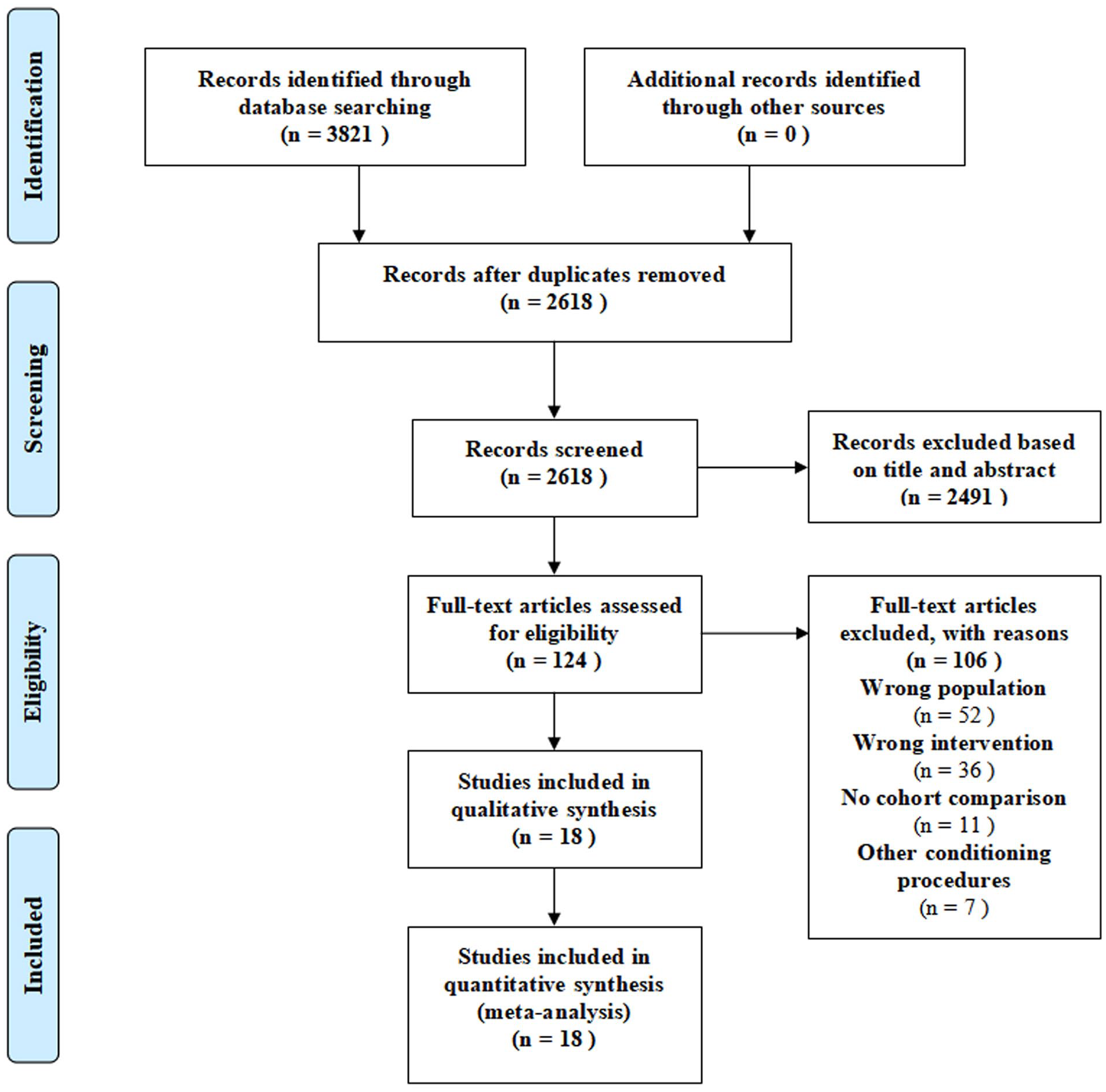
Study selection flow diagram.
Sensitivity and Bias Analyses
Sensitivity analyses were performed by comparing both fixed- and random-effects model outputs. Studies with relatively large differences in the 95% CI distribution from the overall sample were excluded until a fixed-effect model was available (ie, I2≤25% and p≥0.1). The number of remaining data samples after the sensitivity analysis was ensured to be at least 3 to obtain more accurate meta-analysis results. Generally, the exclusion of any single relative-risk estimate from the primary meta-analysis had no major effect on the overall outcomes. Risk of bias was assessed for cohort and case-control studies independently by two authors, using the Newcastle-Ottawa scale (NOS). Discrepancies were resolved by consensus. Publication bias was mainly judged by the inverted funnel plot method, which is generally used to discuss the outcome indicators of the included data with the number of samples (after sensitivity analysis) ≥10.
Outcomes
A total of 2088 patients were included from 18 studies to compare the clinical outcomes of TEVAR and OS for acute thoracic aortic rupture treatment between January 2001 and January 2019. There were 560 patients in the TEVAR group and 1528 patients in the OS group. In addition, in 335 cases (TEVAR: 180 and OS: 155) thoracic aortic rupture was caused by degeneration; in 1753 cases (TEVAR: 380 and OS: 1373), rupture was caused by blunt trauma. All included studies were published in peer-reviewed English journals. Relevant study characteristics are presented in Table 1. The time trend chart of utilization of OS and TEVAR in each center showed that the utilization of TEVAR showed a fluctuating and increased trend, whereas OS showed a fluctuating and decreased trend (Supplementary Figure 1).
Short-term Mortality
Of the 18 publications, 17 publications were identified as including short-term data for subsequent analysis. Data pooled from these studies revealed a statistically significant difference between the TEVAR and OS groups in terms of perioperative mortality (Figure 2A, OR=0.47; 95% CI: 0.34–0.66; p<0.01) with zero heterogeneity (I2=0.0%). Furthermore, 1 year mortality was also lower in TEVAR group than in the OS group (OR=0.46; 95% CI 0.29–0.75; p<0.01; Figure 2B) and no significant publication bias was detected (Supplementary Figure 1A and B). In addition, in both blunt trauma and degenerative patients, the perioperative mortality of TEVAR group was significantly lower than that of OS group (Figure 3A). Similarly, the 1 year mortality rate of blunt trauma patients with in the TEVAR group was lower than that in the OS group; however, there was no significant difference between the two groups in the degenerative cases (Figure 3B). To sum up, stratified analysis showed that the TEVAR group had lower perioperative mortality rates in patients with ruptured descending thoracic aorta (Figure 2) than the OS group. Similarly, TEVAR group had lower 1 year mortality rates in patients with ruptured descending thoracic aorta by blunt trauma (Figure 3) than the OS group. The difference was statistically significant.
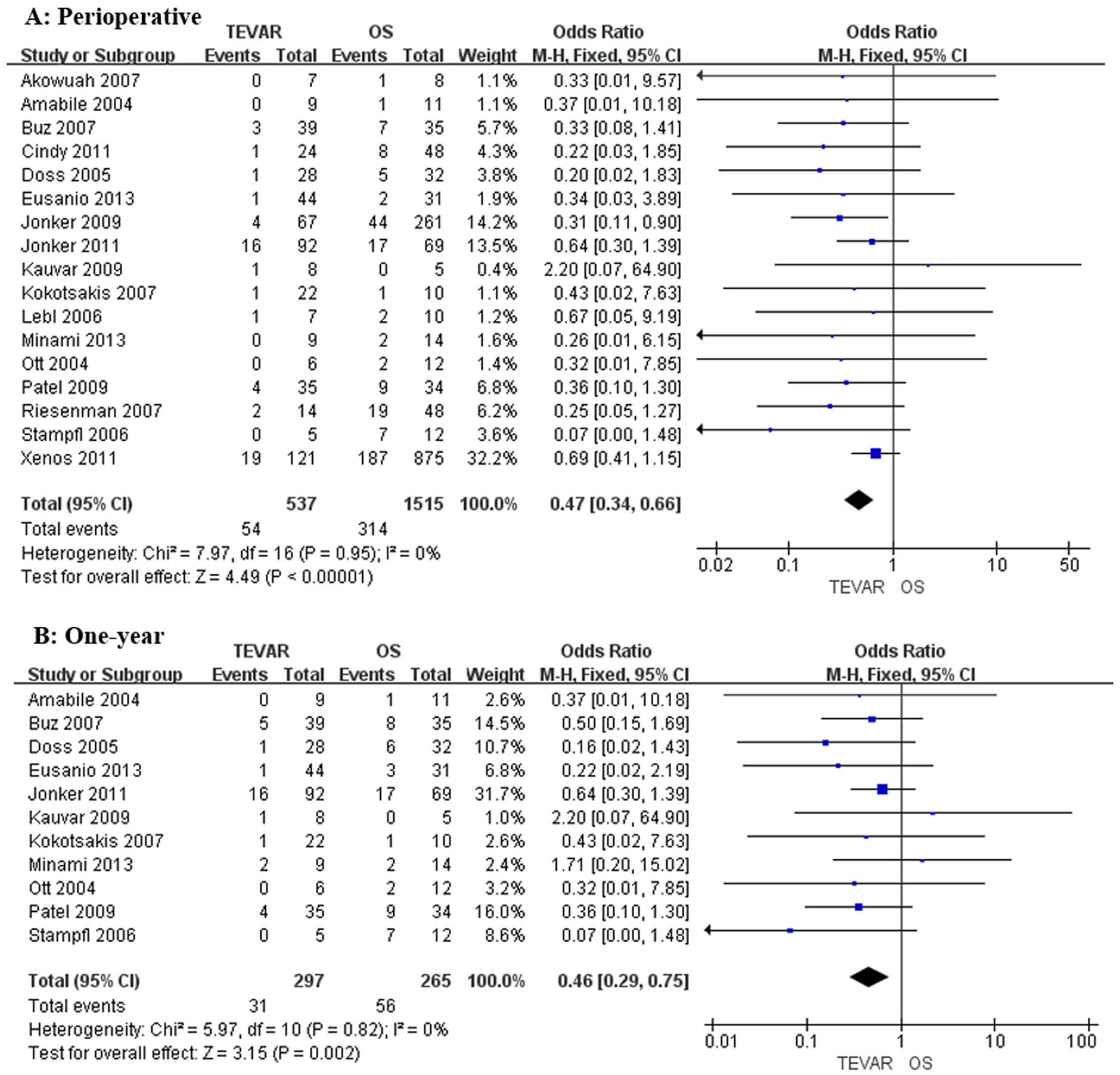
Forest plot of mortality: The effects of TEVAR and OS on mortality in each study are shown as odds ratio and 95% confidence intervals. The overall results indicate that the perioperative mortality (A) and 1 year mortality (B) of TEVAR group was significantly lower than that of OS group. TEVAR, thoracic endovascular aortic repair for ruptured thoracic aorta; OS, open surgery.
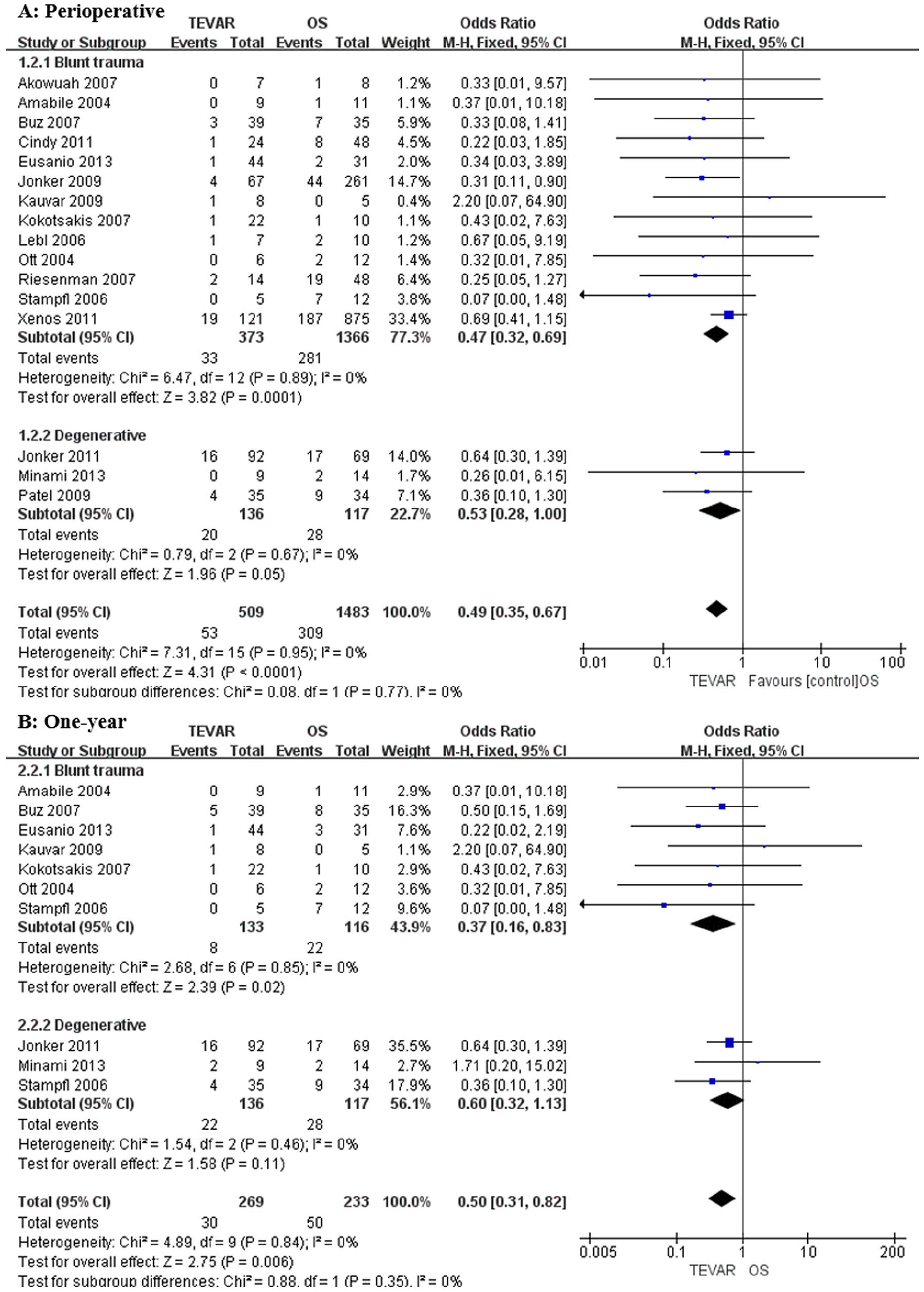
Forest plot of mortality associated with type of lesion: The effects of TEVAR and OS on mortality in each study are shown as odds ratio and 95% confidence intervals. (A) The perioperative mortality between the TEVAR group and OS group in blunt trauma and degenerative cases. (B) The 1 year mortality between the TEVAR group and OS group in blunt trauma and degenerative cases. TEVAR, thoracic endovascular aortic repair for ruptured thoracic aorta; OS, open surgery.
Short-term Complications
Clinical outcomes such as stroke, paraplegia, cardiac complications, pulmonary complications, re-intervention rate, pulmonary embolism, and renal insufficiency were compared between the TEVAR and OS groups. Pooled rates showed no significant differences in terms of stroke, paraplegia, cardiac complications, pulmonary embolism, sepsis, and wound infection, respectively (Figure 4A, B, C, and D and Supplementary Figure 2). However, our results showed that TEVAR tended to have a lower rate of wound infection than OS. Meanwhile, in Cindy et al’s study and Ott et al’s study, there were no patients with sepsis in the TEVAR group.13,24 There was no significant heterogeneity in these studies (I2=7%). However, fewer pulmonary complications (OR: 0.69; 95% CI: 0.52–0.92; p=0.01) and renal insufficiency (OR: 0.56; 95% CI: 0.33–0.93; p=0.03) were observed in the TEVAR group compared with OS group (Figure 4E and F) with almost no significant heterogeneity in these studies (I2≤18%). Our study showed that there was no statistically significant difference in early (perioperative) re-intervention rates between the TEVAR group and the OS group. However, the late re-intervention rate of descending aorta in the TEVAR group was higher than that in the OS group with the difference statistically significant (Figure 5A). In this study, the late re-intervention rate in the TEVAR group was higher than that in the OS group in the degenerative groups. However, there was no statistic difference between TEVAR and OS groups in the trauma group (Figure 5B).
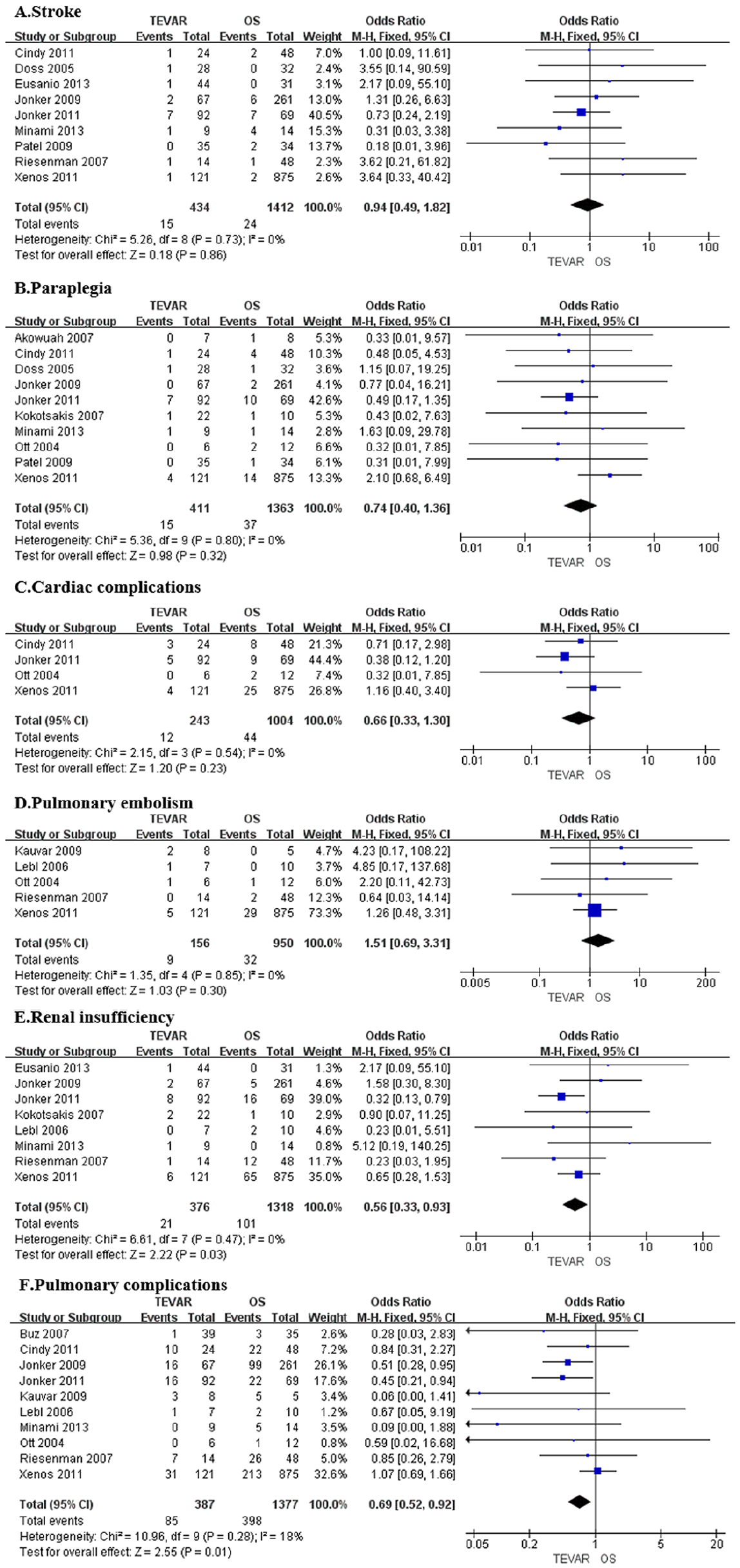
Forest plot of early complication rate: The effects of TEVAR and OS on early complications in each study are shown as odds ratio and 95% confidence intervals. Comparisons of early complications in the repair of thoracic aorta rupture included: (A) stroke; (B) paraplegia, (C) cardiac complications, (D) pulmonary embolism, (E) renal insufficiency, and (F) pulmonary complications. TEVAR, thoracic endovascular aortic repair for ruptured thoracic aorta; OS, open surgery.
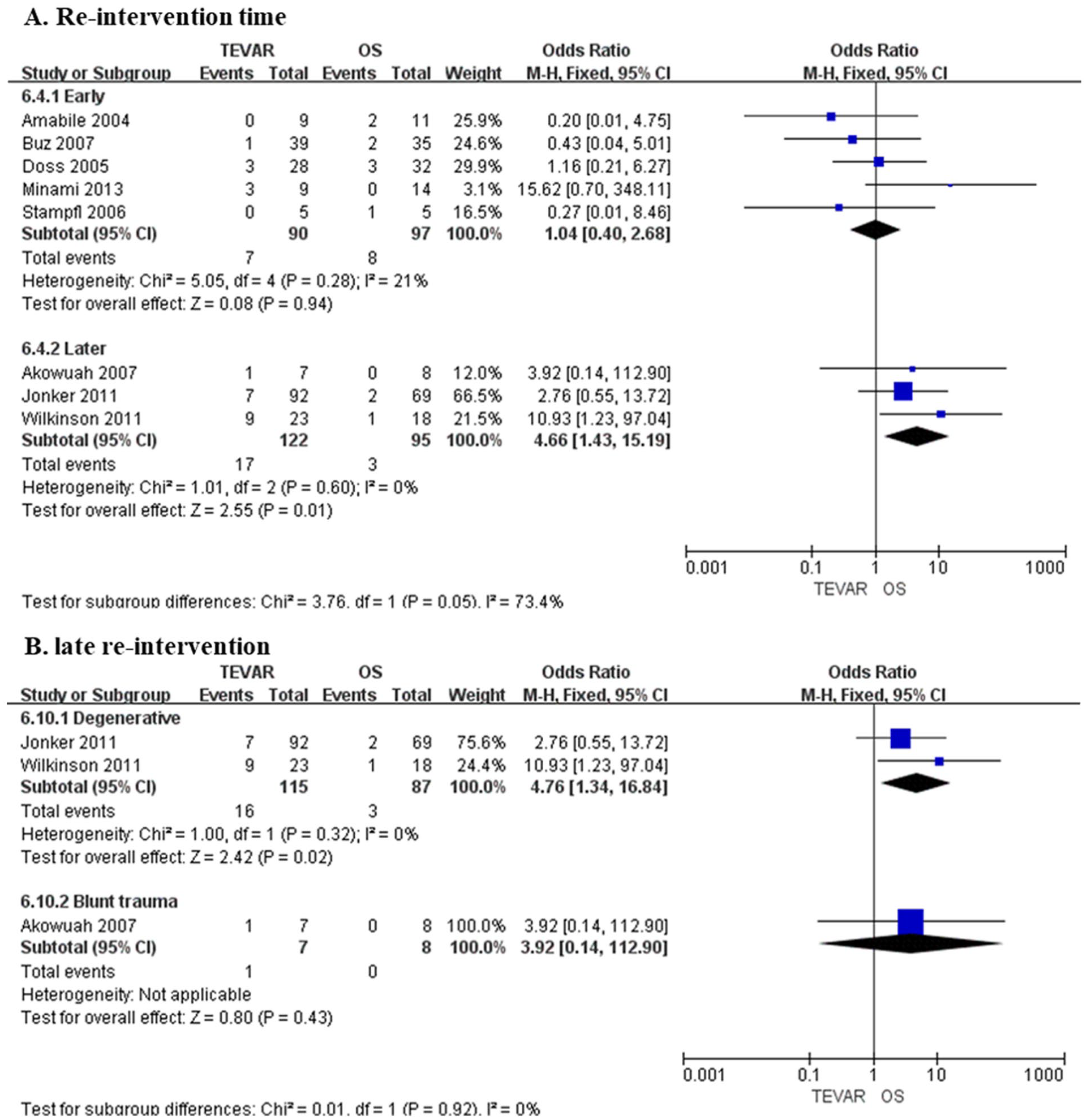
Forest plot of re-intervention rate: The effects of TEVAR and OS on re-interventions in each study are shown as odds ratio and 95% confidence intervals. Comparisons of early (perioperative) re-intervention rate and later re-intervention rate in the repair of thoracic aorta rupture between the TEVAR group and OS group. TEVAR, thoracic endovascular aortic repair for ruptured thoracic aorta; OS, open surgery.
Discussion
Compared with traditional thoracotomy and open aortic repair, TEVAR avoids invasive anesthetic procedures, such as one-lung ventilation and left ventricular bypass, and reduces mortality and postoperative complications; however, TEVAR is often associated with paraplegia and stroke, as well as endoleak, stent displacement, stent folding, and other stent-related complications.25,26 Unfavorable anatomies, such as inadequate proximal or distal landing zones, usually exclude TEVAR from thoracic aortic repair, especially for ruptured aortas. When thoracic aortic disease involves the descending part, TEVAR is generally considered for treatment. The methods of reconstructing the superior aortic arch branches by TEVAR mainly include artificial blood vessel bypass technology, parallel stent technology, and fenestrated and branch stentgraft technologies. The emergence of these technologies makes it possible to repair the aortic arch by hybrid TEVAR, which requires branch vessel reconstruction. To our knowledge, no investigation has compared the outcomes between TEVAR and OS for ruptured descending thoracic aorta treatment. In Harky A et al’s study, patients with injuries extended to the aortic arch were also included in their analysis. 27 Given that TEVAR for ascending aortic pathology remains off-label, comparisons between TEVAR and open surgery should be interpreted with cautions. So, in our research, only the studies that clearly stated the lesion and injury site located in the descending aorta were included, while other studies that did not mention the lesion site were excluded. Our meta-analysis shows no significant differences in postoperative stroke, paraplegia, cardiac complications, early re-intervention rate, and pulmonary embolism between the TEVAR and OS groups. However, TEVAR is associated with lower rates of perioperative renal insufficiency, pulmonary complications, and early mortalities (30 day/in-hospital mortality and 1 year mortality) compared with OS. In addition, compared with the OS, TEVAR shows higher later re-intervention rate.
Our study showed that there was no statistical difference in the 1 year mortality between the two groups (TEVAR and OR) in the degenerative cases. Owing to the atherosclerotic pathogenesis of degenerative aneurysm, this group of patients usually accompanied by a higher proportion of multiple comorbidities. Due to the less invasion, we believe that TEVAR has an advantage over OS in reducing the perioperative morbidity and mortality of patients with poor general condition. However, the etiology of degenerative diseases may still exist after TEVAR. Therefore, once the ruptured aorta was repaired, the long-term influence of the surgical strategy was not obvious. However, we have to emphasize that the 1 year mortality about the degeneration was reported in only three studies, thus it should be interpreted with caution.
Ischemic stroke is one of the leading causes of postoperative death following TEVAR, with a reported incidence of 0% to 18.2%.28-30 A postoperative ischemic stroke is closely related to hemodynamic changes in patients before and after the operation. Buth et al’s study revealed that surgery duration may also be a risk factor for perioperative cerebral infarction. 28 TEVAR was associated with cerebral embolization from atheromatous plaque debris caused by the manipulation of guidewires, catheters, sheaths, or deploying stentgrafts, and possible air embolism. This was further supported by the observations published by Sullivan and co-workers, especially when atherosclerotic lesions existed in the aortic arch. 31 Several other studies documented similar stroke rates in open surgery and endoluminal repair.24,32,33 Our systematic review and meta-analysis did not reveal a difference in neurological complications between the TEVAR and OS groups.
The incidence of paraplegia reported in various literature ranged from 0% to 12.5%. 34 Due to technical limitations, such as the inability to reconstruct the intercostal artery, TEVAR, which is less invasive than OS, did not significantly reduce postoperative paraplegia rates. 35 Our meta-analysis also suggests that there is no statistical difference between TEVAR and OS in terms of postoperative paraplegia. Currently, the paraplegia mechanism is vague and is mainly related to spinal cord supply, artery coverage by stentgraft in the treated segment of the aorta, perioperative hemodynamic stability, and intercostal and lumbar arteries thrombosis or embolization. 36
Renal insufficiency after TEVAR is a common postoperative complication. It has been reported that the incidence of acute kidney injury after TEVAR ranges from 1.5% to 34%.37,38 Our findings indicate that the rate of renal insufficiency in TEVAR patients is lower than that in the OS group (21/376 vs 101/1318). One explanation for this matter is that TEVAR has less renal artery ischemia than OS. Although intravascular contrast may cause kidney injury, our study findings suggest that contrast-induced nephropathy following TEVAR might be temporary and less harmful than prolonged ischemia during OS.
The majority of the pulmonary complications in the OS group were related to thoracotomy and single lung ventilation. Poor respiratory function, resulting from postoperative pain and atelectasis, requires longer ventilation support and intensive care unit stay. These led to an increased postoperative pneumonia and sepsis incidence. 13 In the TEVAR group, most patients need open or even only percutaneous femoral artery access. Its less invasive nature significantly reduces respiratory complications, especially in patients who sustain traumatic aortic rupture with associated pulmonary injury.
TEVAR has been increasingly promoted as one of the preferred methods for thoracic aortic rupture due to its advantages of small trauma and good prognosis. However, studies have shown that the long-term efficacy of TEVAR remains controversial. 39 The incidence of complications such as endoleak, aortic aneurysm-like expansion, retrograde type A aortic dissection, and aortic rupture in the late stage of TEVAR is high, and the re-intervention rate is 8.1% to 32.4%40,41 More than 20% of patients required re-intervention at 1 year after TEVAR, and this proportion was as high as 54% at 6 years after TEVAR.42,43 Similarly, our study showed that there was no statistically significant difference in early re-intervention rates between the TEVAR group and the OS group after thoracic aortic rupture. However, for the late re-intervention rates, the TEVAR group was higher than the OS group with the difference statistically significant. This may be related to the occurrence of aortic aneurysmal dilatation, endoleak, and other related complications after TEVAR.
Thoracic aortic rupture treatment in emergency settings remains challenging. Associated severe comorbidity is common in thoracic aortic rupture patients. High rates of respiratory failure, acute renal insufficiency, and bleeding re-exploration are also common following emergency open procedures. In addition, there are some open surgery-related risks, such as lung injury and postoperative pneumothorax from thoracotomy, which may also contribute to high perioperative mortality. 44 Although Alric et al reported that stentgrafts failed to protect patients from abdominal aortic aneurysm–related deaths, 45 our study showed that TEVAR was associated with decreased perioperative mortality and 1 year mortality and the incidence of early complications in patients with ruptured thoracic aorta compared with OS.
Limitations
This study has several limitations. First, the major limitations of this study are its retrospective nature and the differences in baseline characteristics between the groups. However, a randomized study would be difficult to undertake. The differences between the groups may be due to selection bias, prioritizing patients with more complex complications to the TEVAR group. Some patients with severe conditions underwent TEVAR because they were unable to tolerate open surgery, which may result in a high mortality risk. Similarly, anatomic constraints limit patient selection for endovascular therapies. In addition, baseline pathological differences (ie, more frequent arch repair in DTAR) may also have contributed to the increased morbidity seen in the open surgery group. These factors may affect the outcomes. Second, the patients included in this study do not represent patients with ascending aorta rupture. The patients in the literature we included had lesions located in the descending aorta only. Publication bias should be considered, although heterogeneity analysis results are satisfied in the majority of the analyses. Third, due to the limited number of patients with thoracic aortic rupture caused by degeneration, it is difficult to conduct a deeper stratified analysis on this group of patients. Therefore, our study mainly analyzed and discussed the results by trauma and degeneration. To some extent, it can also explain the impact of trauma and degeneration factors on the clinical outcome by TEVAR or OS. Fourth, the short-term follow-up period varied, and there was a lack of data regarding long-term outcomes. This study spans a long time (18 years), during which both surgical technology and anesthetic trauma management improved significantly. When interpreting our results, it is also worth noting that some patients received early treatment. Despite this, the trends observed in the present study are clinically significant. We were able to identify the importance of TEVAR in reducing early morbidity.
Conclusion
In summary, our systematic review and meta-analysis demonstrate that TEVAR is associated with lower perioperative and 1 year morbidity and mortality in patients with acute descending thoracic aortic ruptures, compared with OS. TEVAR is safe and effective for treatment of ruptured descending thoracic aortic ruptures when the patient anatomy is suitable. Risk of re-intervention following TEVAR is not increased based on short-term follow-up. However, further studies are required to compare the long-term clinical outcomes between TEVAR and OS.
Supplemental Material
sj-jpg-1-jet-10.1177_15266028211057087 – Supplemental material for A Comparison of Clinical Outcomes of Endovascular Repair Versus Open Surgery for Ruptured Descending Thoracic Aorta
Supplemental material, sj-jpg-1-jet-10.1177_15266028211057087 for A Comparison of Clinical Outcomes of Endovascular Repair Versus Open Surgery for Ruptured Descending Thoracic Aorta by Xinsheng Xie, Xiaolong Shu, Wei Zhang, Daqiao Guo, Wayne W. Zhang, Lixin Wang and Weiguo Fu in Journal of Endovascular Therapy
Supplemental Material
sj-jpg-2-jet-10.1177_15266028211057087 – Supplemental material for A Comparison of Clinical Outcomes of Endovascular Repair Versus Open Surgery for Ruptured Descending Thoracic Aorta
Supplemental material, sj-jpg-2-jet-10.1177_15266028211057087 for A Comparison of Clinical Outcomes of Endovascular Repair Versus Open Surgery for Ruptured Descending Thoracic Aorta by Xinsheng Xie, Xiaolong Shu, Wei Zhang, Daqiao Guo, Wayne W. Zhang, Lixin Wang and Weiguo Fu in Journal of Endovascular Therapy
Supplemental Material
sj-jpg-3-jet-10.1177_15266028211057087 – Supplemental material for A Comparison of Clinical Outcomes of Endovascular Repair Versus Open Surgery for Ruptured Descending Thoracic Aorta
Supplemental material, sj-jpg-3-jet-10.1177_15266028211057087 for A Comparison of Clinical Outcomes of Endovascular Repair Versus Open Surgery for Ruptured Descending Thoracic Aorta by Xinsheng Xie, Xiaolong Shu, Wei Zhang, Daqiao Guo, Wayne W. Zhang, Lixin Wang and Weiguo Fu in Journal of Endovascular Therapy
Footnotes
Acknowledgements
The authors are grateful to all the institutions that were included in this study for providing data for this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (grant number: 81970412), Shanghai Municipal Science and Technology Commission Innovation Fund (grant number: 18441902400), Xiamen Municipal Health Science And Technology Program Fund (grant number: 3502Z20194034) and Zhongshan hospital’s Talents Supporting Plan (grant number: 2019ZSGG11).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.