
Abstract
Purpose:
Patients with arteriovenous malformations (AVMs) have a lower health-related quality of life (QoL) than the general population. QoL assessment of patients with peripheral AVMs after endovascular treatment is scarce in the literature. Radiologic and clinical outcomes are not always correlated in vascular malformation treatment. This study aimed to investigate the relationship between clinical outcomes, QoL, and angiographic outcomes.
Materials and Methods:
Patients with peripheral AVM that underwent endovascular treatment between January 2009 and December 2021 in a single center were retrospectively evaluated. Patients’ characteristics (age, sex), AVM characteristics (Schobinger classification, location, angiographic architecture), previous treatment, treatment characteristics (type of endovascular approach, embolizing agent and number of sessions), percentages of angiographic response, complications, and recurrence were evaluated. The angiographic architecture was evaluated according to the Yakes classification. The questionnaire was applied for evaluation of clinical response and QoL. Patients older than 12 years and those who can be contacted were included in clinical and QoL analysis. Clinical response was defined as improvement in the patient’s most important pretreatment symptom. Treatment response was defined as clinical response plus >50% angiographic response.
Results:
Eighty-six patients (41 males [47.7%], 45 females [52.3%]) were included in angiographic analysis. The mean age was 28.44±12.99 years (range=5–61). Forty-three patients (50%) had previous treatment. The median number of sessions was 2 (range 1–15, InterQuartile Range [IOR]=2). Sixty-one patients (30 males [49.2%], 31 females [50.8%]) were included in clinical analysis. The clinical response rate was 73.8%, 95% confidence interval (CI) [0.60, 0.84]. The treatment response rate was 45.9%, 95% CI [0.33, 0.59]. The complication rate was 8.2%. Before treatment, 48 patients (78.7%) reported a negative impact on their QoL. Thirty-three of 48 patients (68.8%) reported improvement on their QoL after treatment. Higher Schobinger stages were related to a negative impact on QoL before treatment (p<0.01). Yakes types were not related to QoL (p=0.065). Clinical response was related to improvement on QoL after treatment (p<0.01). Angiographic and treatment responses were not related to improved QoL after treatment (p=0.52 and p=0.055, respectively).
Conclusion:
Angiographic architecture and outcomes were not always reflected in QoL after endovascular treatment.
Clinical Impact
This study’s findings will help clinicians with what to focus on in AVM treatment and how to monitor patients with peripheral AVM after endovascular treatment. Rather than relying too much on the angiographic response, patients should be checked for symptoms and quality of life improvement. No clear data in the literature regarding the applicability of the Yakes Classification in patients with previous treatment. This study questioned the applicability of the Yakes Classification in patients with previous treatments. In this study, type 4 AVMs were more common in patients with previous treatment.
Introduction
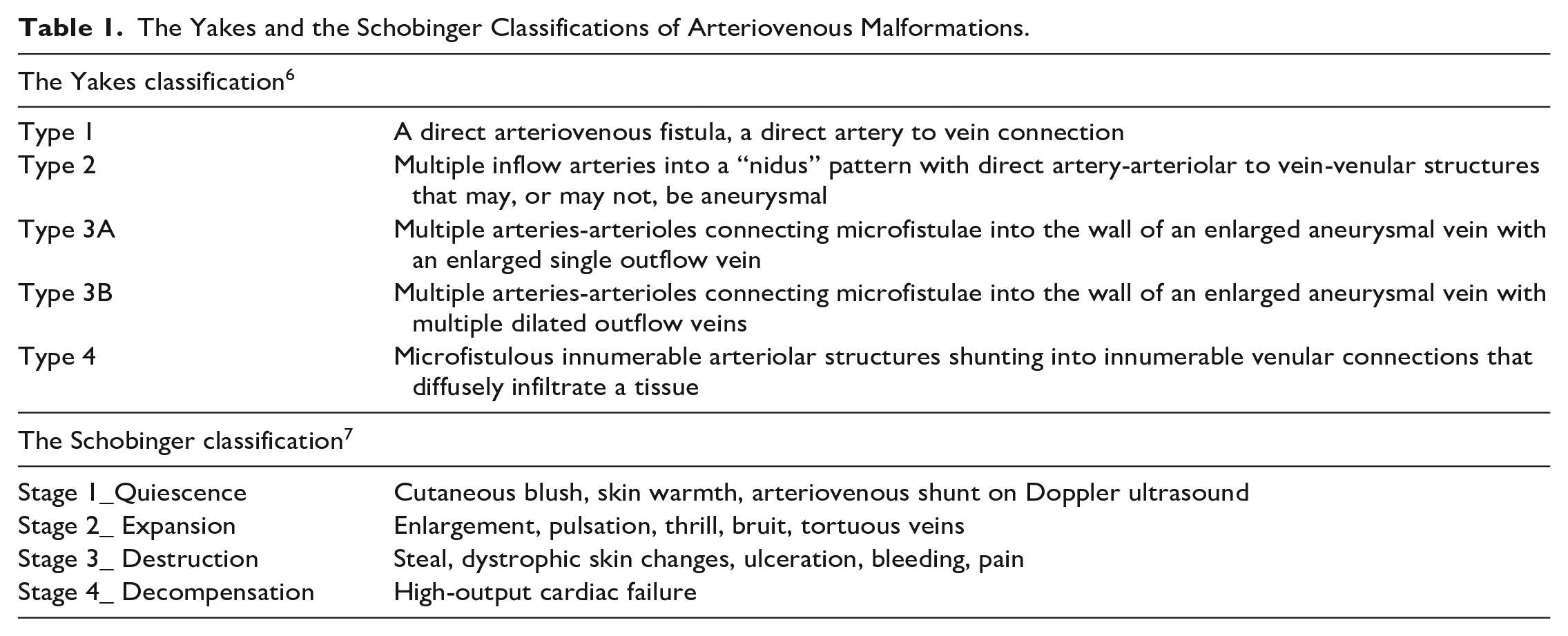
Arteriovenous malformations (AVMs) are lesions with direct fistulous connections between arteries and veins of various sizes without intervening normal capillary bed. The main purpose of AVM treatment is to eliminate such fistulous connections. 1 Over time, the number of patients undergoing primary endovascular treatment for peripheral AVM has increased. 2 For the endovascular management of AVMs, different systems of classification were devised according to AVM’s angiographic architecture.3–5 A relatively new one, the Yakes classification system, contains 5 different types of AVM and is used to determine the best endovascular approach according to AVM’s angiographic architecture. 6 The Yakes classifications of AVMs are listed in Table 1.1,6,7 Angiographic architecture types of AVM have been previously shown to influence the angiographic outcomes, the number of procedures, and the rate of complications.8–10 However, angiographic and clinical outcomes in AVM treatment were not always found to be correlated.9,11
The Yakes and the Schobinger Classifications of Arteriovenous Malformations.
Patients with vascular malformation have lower health-related quality of life (QoL) compared with the general population.12–14 Hence, one should set the improvement of the patient’s QoL as a point of focus when dealing with AVM. QoL assessments conducted on patients with peripheral AVM after endovascular treatment remain scarce in the literature. In this study, the QoL of patients with peripheral AVM was evaluated before and after they were treated endovascularly. The angiographic outcomes were assessed according to the Yakes classification system and an analysis of the relationship between angiographic outcomes, clinical outcomes, and QoL was performed.
Materials and Method
For this study, an approval from the Institutional review board was obtained. Patients with peripheral AVM that underwent endovascular treatment between January 2009 and December 2021 in a single medical center were retrospectively evaluated. Patients with pulmonary and uterine AVMs were not included in this study. Patients’ characteristics (age, sex), AVM characteristics (clinical stage, location, Yakes classification), previous treatments, treatment characteristics (type of endovascular approach, embolizing agent and the number of sessions), complications, and recurrences were evaluated. Early postoperative (up to 1 week) swelling and pain were not accepted as a complication. The clinical stage of AVMs was determined according to the Schobinger classification. The Schobinger classifications of AVMs are listed in Table 1.1,6,7 The type of endovascular approach used was categorized as trans-arterial, percutaneous (nidus and/or venous), and combined (trans-arterial + percutaneous). Agents used for treatment were categorized as sclerosants (polidocanol and/or ethanol), liquid embolizing agents (EVOH [ethylene vinyl alcohol copolymer] and/or n-BCA [n-Butyl cyanoacrylate]) and combined (sclerosants + liquid embolizing agents). Patients were contacted by phone call. After obtaining their verbal consent, patients (or the patient’s legal guardian, in cases where the patient was a minor) were asked whether they had any specific pretreatment symptoms (such as pain, swelling, function loss, cosmetic disfigurement or bleeding, and focal ulceration) 15 and if they had any negative impact caused by AVM on their daily lives or not. The patients were also asked to assign a rating to change in their symptoms and the improvements they observed in their daily lives after the treatment. A 5 point scale was used for grading: 1 (worsening), 2 (no change), 3 (minor improvement), 4 (major improvement), and 5 (complete relief). 11 Clinical response was defined as improvement in the patient’s most important pretreatment symptom (which disturb them the most) with a grade of 3 to 5. In cases with more than one most important symptom, improvement was sought in all of their most important symptoms for clinical response. Cases with improvement in their symptoms other than the most important one were not accepted as a clinical response. Yakes classifications and angiographic results were evaluated by two experienced interventional radiologists. Examples of each type of Yakes classification are shown in the Supplementary Figure. Percentages of shunt reduction were graded under four categories: (1) <50% shunt reduction, (2) 50–75% shunt reduction, (3) 76–90% shunt reduction, and (4) >90% shunt reduction. The percentage of shunt reduction was calculated between the last and first angiographic examinations performed in the study period. In other terms, angiographic results were analyzed per patient, not per procedure. Treatment response was defined as a clinical response plus >50% shunt reduction.
Patients with Schobinger stage 2 or higher were offered the option of treatment. In the study time period, 86 patients with peripheral AVM underwent the endovascular treatment process. Twenty patients could not be contacted by phone call. These patients were excluded from the clinical analysis, but included in the angiographic analysis. In this cohort, there were 2 cases of exitus. One of them was AVM related. This patient had a large head and neck AVM that involved the airway. The other patient died from an unrelated cause. These 2 patients were included in the angiographic analysis, but were excluded from the clinical analysis. Five patients that were under the age of 12 were also excluded from the clinical analysis and the QoL assessment, as they may not be able to clearly state the impact of AVMs on their lives.
Endovascular Procedure
Written informed consent was obtained from the patients (or their legal guardian, if the patient was a minor) before the procedure. Under deep sedation, femoral artery access was obtained with ultrasound guidance and a 4F vascular sheath was inserted. Diagnostic angiograms with different projections were obtained in pertinent body parts containing the AVM to evaluate feeders of AVM, the architecture of AVM, the outflow veins and the surrounding normal arterial anatomy. After delineating the feeders of AVM, each feeder was catheterized superselectively with 2.0 to 2.4F microcatheters. Microcatheters were advanced to the nidus or pre-nidus artery for embolization. A superselective angiogram was performed with microcatheters to demonstrate the nidus stain, the outflow pattern and the absence of normal arteries of surrounding tissues. Next, a test angiogram with a 2 mL syringe was performed to determine the injection rate of the agent. The choice of embolic/sclerosant agents was made based on performing physicians’ discretion and the availability of agents. In fast flowing lesions, outflow vein or proximal arterial manual compression was applied in order to extend the dwelling time of the agent in the nidus.
In this cohort, 13 patients (15.1%) were only treated with sclerotherapy, 20 patients (23.3%) were only treated with liquid embolization, 2 (2.3%) patients were only treated with coil embolization, and 51 patients (59.3%) were treated with both sclerotherapy and liquid embolization. Four patients had additional embolization for large shunt occlusion, which was performed with coils in 3 patients and with an amplatzer vascular plug in 1 patient. Polidocanol and ethanol were used as sclerosant agents. Volumes of 2 mL/kg of polidocanol and 0.14 mL/kg of ethanol were not exceeded per session. EVOH and n-BCA were used as liquid embolic agents.
Treatment sessions were scheduled at 4 to 6 week intervals. Treatment sessions were performed until there was no reachable AVM component left or until alleviation of clinical symptoms was achieved.
Statistical Analysis
For statistical analysis, SPSS 25.0 (IBM Corp, Armonk, NY, USA) was used. Continuous data were presented as mean±SD or median (IOR) and categorical data were displayed as percentages. Continuous data were compared with the Mann-Whitney U test. Categorical variables were compared using the Chi-square test or the Fisher exact test. Variables with a p value less than 0.1 in the univariate analysis for QoL improvement after treatment were included in the multivariate analysis. Kaplan-Meier curve analysis was performed to assess recurrence-free time after endovascular treatment. Statistical significance was set to p<0.05.
Results
Angiographic Outcomes
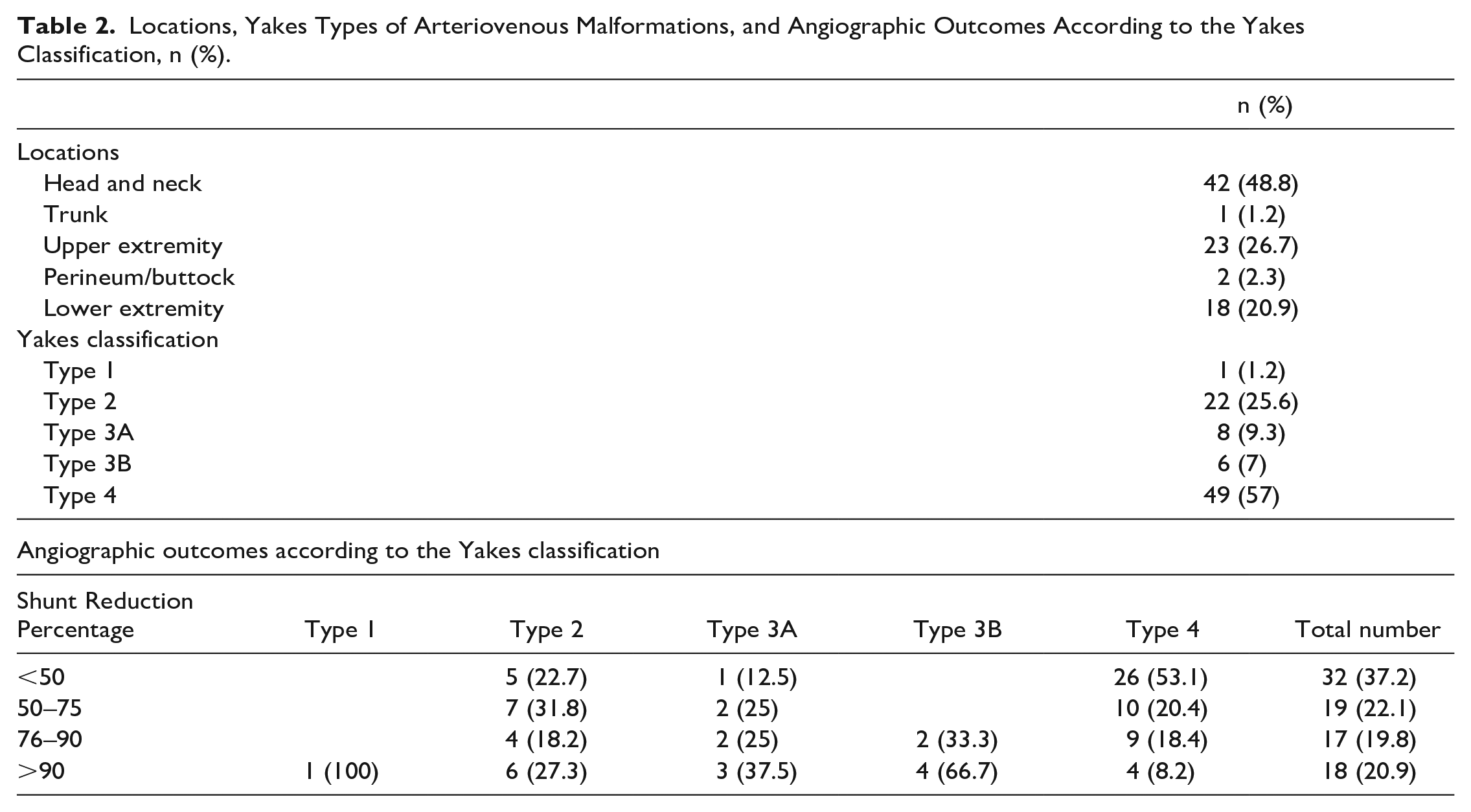
Eighty-six patients (41 males [47.7%], 45 females [52.3%]) were included in the angiographic analysis. The mean age was 28.44±12.99 years (range=5–61). Forty-three patients (50%) had previous treatment (20 patients with surgery, 15 patients with endovascular treatment, 6 patients with surgery and endovascular treatment, 1 patient with radiotherapy, and 1 patient with laser treatment). Locations, Yakes types of AVMs, and shunt reduction percentages according to the Yakes classification were listed in Table 2. The median number of the sessions was 2 (range=1–15, IOR=2).
Locations, Yakes Types of Arteriovenous Malformations, and Angiographic Outcomes According to the Yakes Classification, n (%).
Clinical Outcomes and the QoL
Sixty-one patients (30 males [49.2%], 31 females [50.8%]) were included in the clinical analysis. The mean age was 30.18±12.71 (range=12–61) years. Patient-reported clinical outcomes are shown in Table 3. The clinical response rate was 73.8%, 95% confidence interval (CI) [0.60, 0.84]. Four patients with improvement in symptoms other than the most important one and 2 patients with improvement in one of their most important symptoms, but not all, were not included in the clinical response (Supplementary Table). The treatment response rate was 45.9%, 95% CI [0.33, 0.59]. The complication rate was 8.2%. There was no statistically significant difference seen between the type of endovascular treatment approaches and the complication rates (p=0.61). Complications occurred in 5 of 61 patients. Two patients had temporary paresthesia and 2 patients had minor wounds which were treated by dressing the wound without requiring reconstructive surgery. One patient experienced prolonged pain after the treatment. There was no permanent complication related to endovascular treatment in this cohort. Twenty patients (32.8%) reported recurrence of their symptoms during 43.96±29.61 months of the mean follow-up time. In Kaplan-Meier event-free survival curve analysis, the median recurrence-free time was 75 months, 95% CI [55.31, 94.68] (Figure 1). Four patients with AVM in their extremities underwent amputation (3 minor and 1 major amputation) during the follow-up.
Patient Reported Clinical Results, n (%).
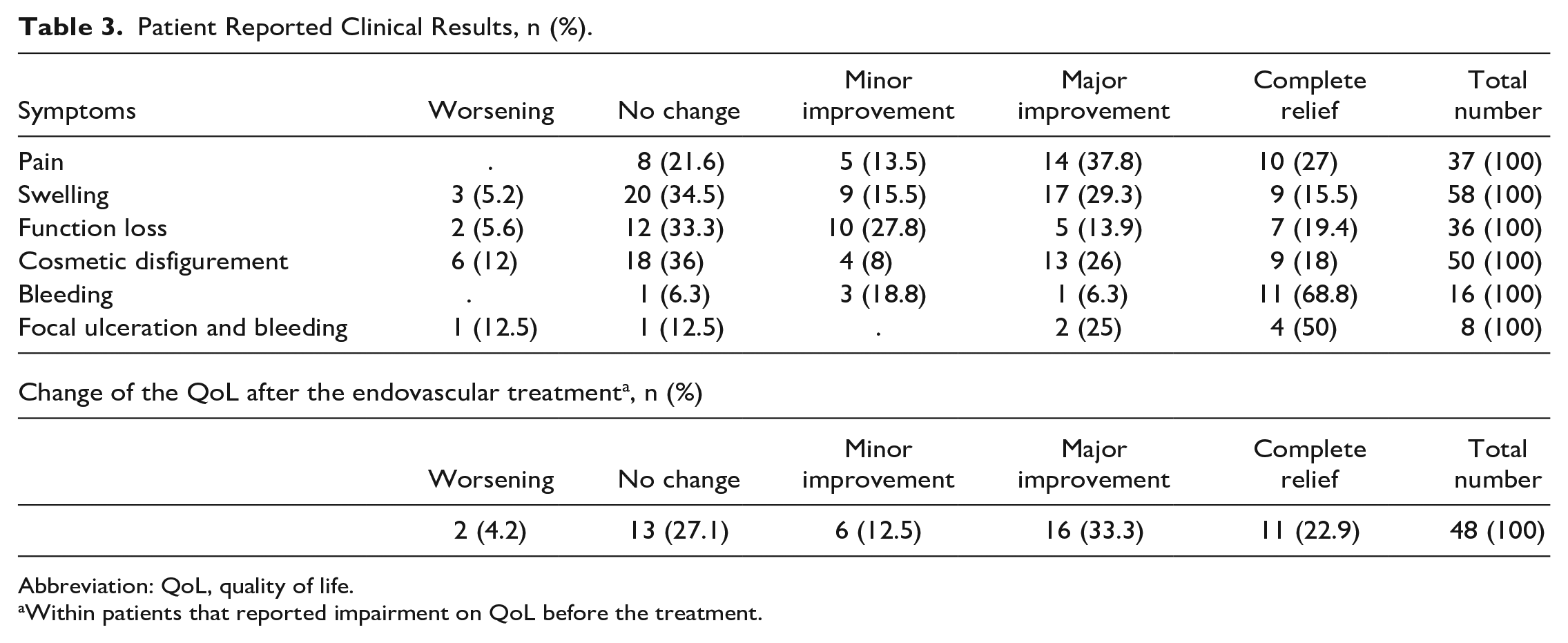
Abbreviation: QoL, quality of life.
Within patients that reported impairment on QoL before the treatment.
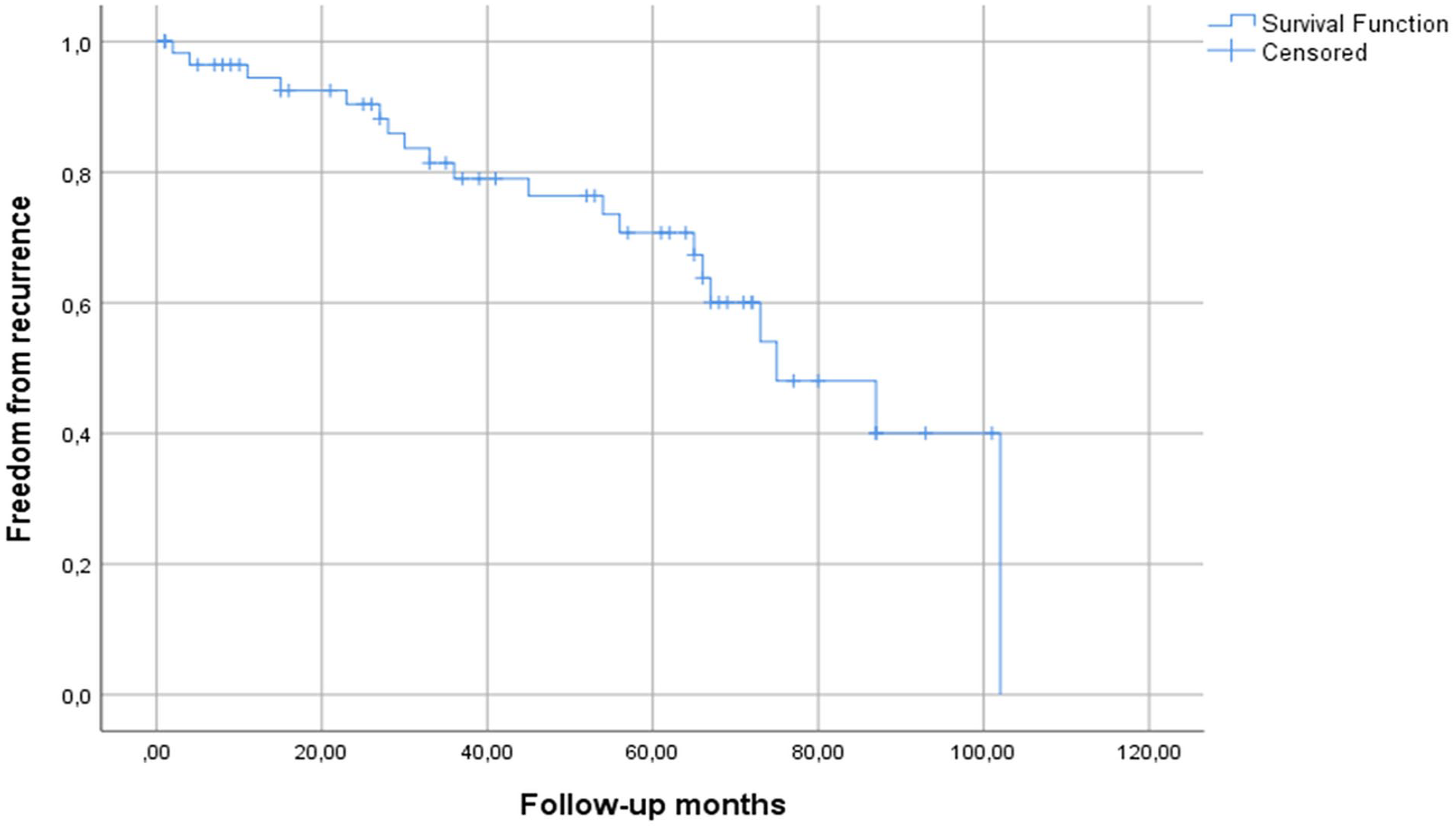
Kaplan-Meier event-free survival curve of recurrence-free rate after endovascular treatment.
Before treatment, 48 patients (78.7%) reported a negative impact on their QoL caused by AVM. Thirty-three of 48 patients (68.8%) reported improvement (minor, major improvements, and complete relief) on their QoL after the treatments. Analysis of variables between the patients with and without impaired QoL before the endovascular treatment are listed in Table 4. Only the Schobinger classification was related to the negative impact on QoL (p<0.01). Age, gender, AVM’s location, Yakes classification, and previous treatments were not found to be related to the negative impact on QoL. Table 5 shows an analysis of variables between patients with and without improvement on their QoL after the treatment. In univariate analysis, the angiographic response rate, complication, the type of agent used, Yakes classification, number of sessions, and recurrence were not found to be related to the improvement on QoL after the treatment (p>0.1). In univariate analysis, clinical response and treatment response had p value less than 0.1, and these variables were included in the multivariate analysis. In multivariate analysis, only clinical response was a predictor of improvement on QoL after the treatment (p=0.007) (Table 5). The key findings of the study are summarized in Figure 2.
Analysis of Variables Between Patients With and Without Impaired QoL Before the Treatment.
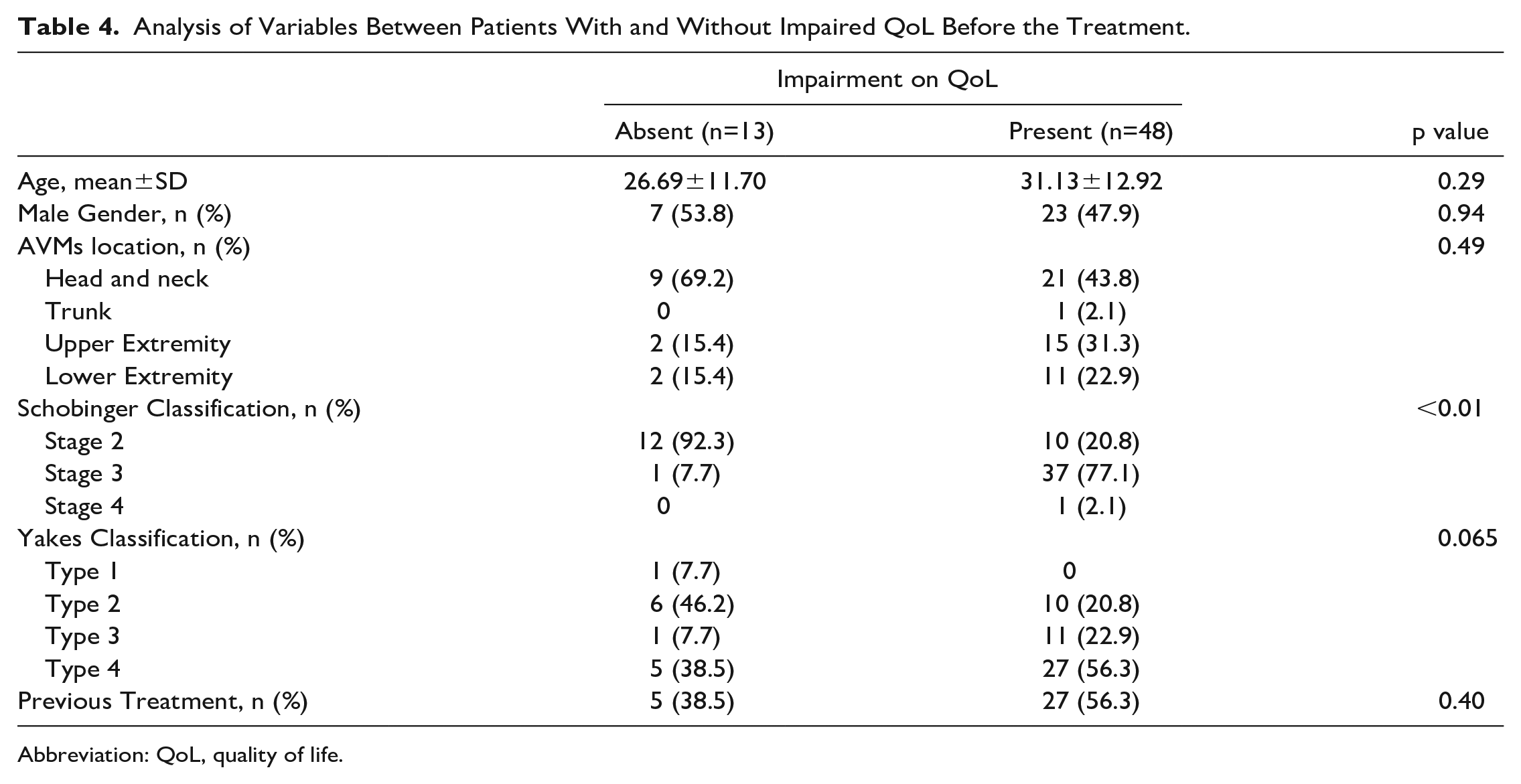
Abbreviation: QoL, quality of life.
Univariate and Multivariate Analyzes of Variables Between Patients With and Without Improvement on QoL After the Treatment.
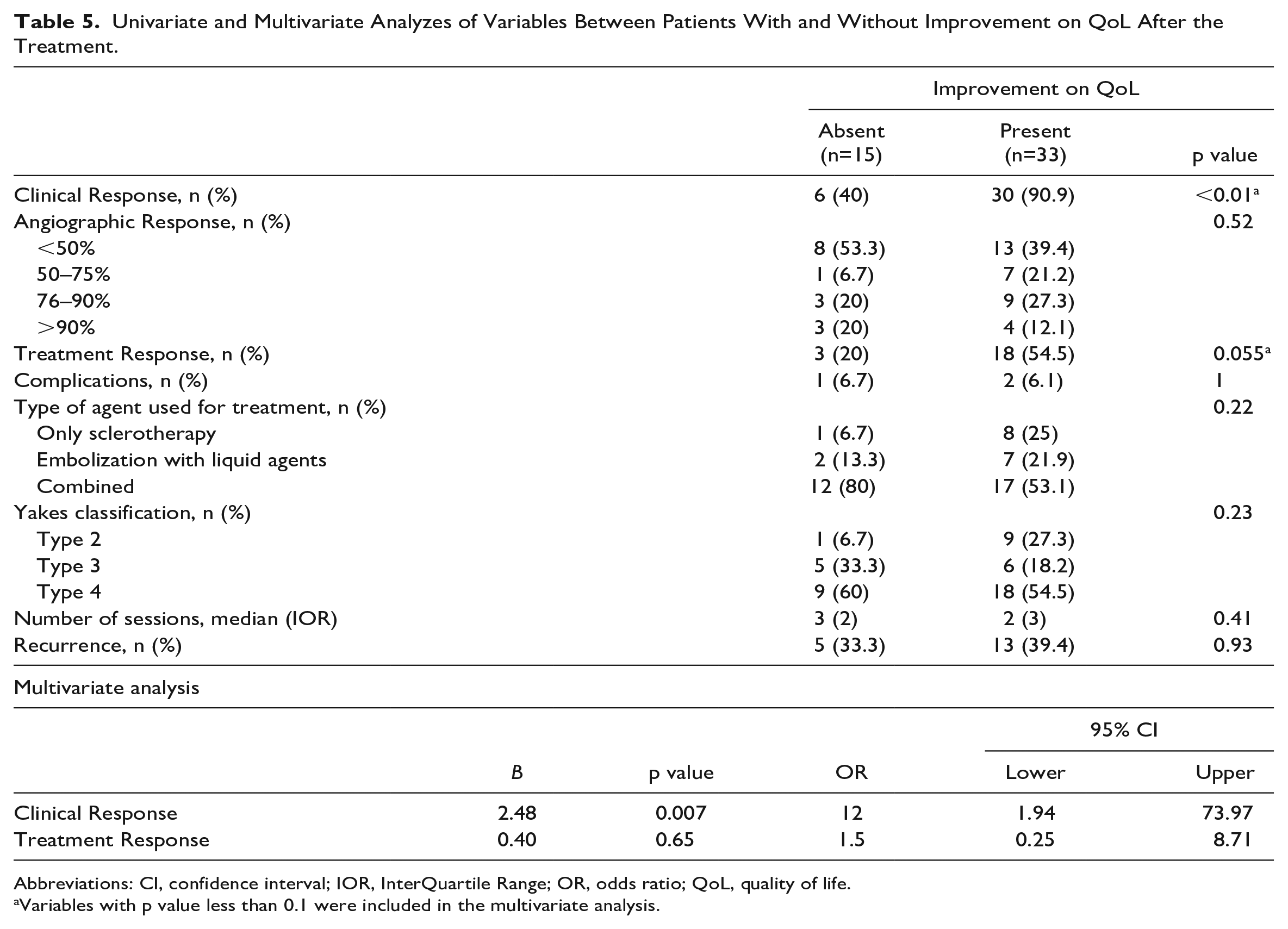
Abbreviations: CI, confidence interval; IOR, InterQuartile Range; OR, odds ratio; QoL, quality of life.
Variables with p value less than 0.1 were included in the multivariate analysis.
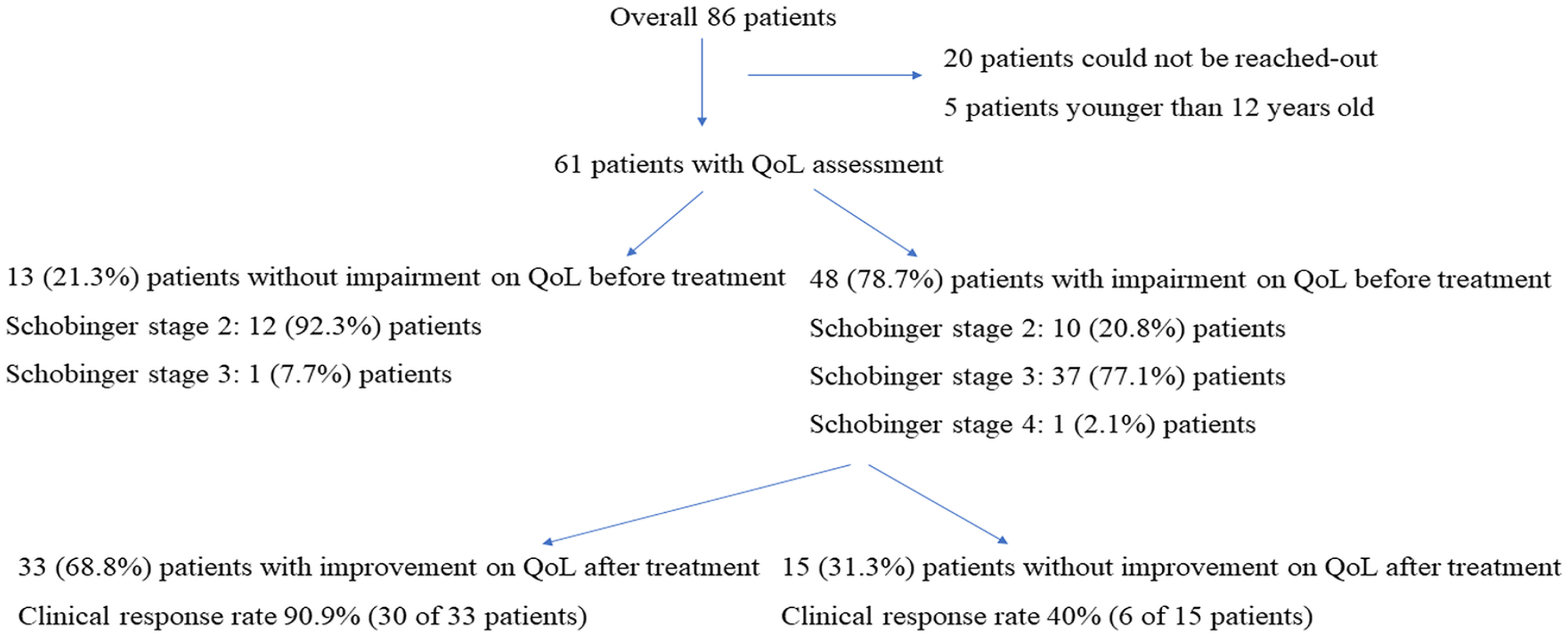
Summary of the key findings of the study.
Discussion
As inadequate treatment may lead to the exacerbation of symptoms and can be associated with worse treatment outcomes, AVM treatment requires meticulous planning by a multidisciplinary team.1,16 Endovascular treatment, surgery, radiotherapy, laser therapy, and a combination of these are therapeutic options for AVM treatment. Over time, the primary endovascular approach for the treatment of AVM has been used to treat an increasing number of patients. 2 Different endovascular approaches considering AVM architecture have been proposed to achieve the best angiographic response and lower complication rates. 6 However, the angiographic and clinical responses were not always correlated. Thus, the therapeutic goals of the treatments must be defined by clinical symptoms and not just by angiographic picture of the AVM.11,17
In this study, 78.7% of the patients reported a negative impact on their QoL caused by AVM. Only, pretreatment higher Schobinger stage was found to be related to a negative impact on QoL. Improvement on QoL after the treatment was reported by 68.8% of the patients who reported an AVM-related impairment before treatment. Clinical response was the only predictor of this improvement. These results underline the importance of the clinical aspects of AVMs both before and after treatment. In this study, there were 3 patients with more than 90% angiographic response and without improvement on QoL. This can be explained by procedural vasospasm and local edema which may have led to the overestimation of shunt reduction. 9 Furthermore, 2 of these patients were scheduled to have surgery after embolization for cosmetic concerns. However, as the main purpose of the study was an evaluation of primary endovascular treatment, all patients were asked to evaluate solely endovascular therapy.
To the best of our knowledge, there is only one publication with a limited number of patients with head and neck AVM that reports the QoL of patients after endovascular treatments. 11 In this article, the QoL of all 9 patients improved after the treatments. Our study is one of the first to evaluate the QoL of patients with peripheral AVM before and after endovascular treatment. The results of this study will help physicians to better inform their patients with AVM about what to be expected from the treatment. We believe proper patient consultation has imperative importance in patients’ compliance with treatment. Patient’s compliance is essential in the endovascular treatment which could necessitate multiple sessions.
Existing studies on peripheral AVM in the literature have heterogeneous patient populations, treatment strategies, and different treatment outcome definitions. This compromises the precise comparison of the treatment outcomes between studies. Improvement in pre-treatment symptoms was reported in a range of 54% to 91% in the literature.8,10,15,18,19 In line with the literature, the clinical response rate was 73.8% in this study.
In the literature, the angiographic architecture of AVM had an effect on the angiographic outcome, the number of procedures and complications.8–10 Yakes type 4 AVMs are hard-to-treat lesions and they are reported to have the worst angiographic outcome of all other Yakes types.1,9,20 Sheng et al 21 stated that no surgery other than amputation may be feasible in type 4 AVM. In line with the literature, the lowest shunt reduction rate was achieved in type 4 AVMs in this study. More than 50% shunt reduction was achieved in 100%, 77.3%, 92.9%, 46.9% for type 1, type 2, type 3, type 4, respectively.
An increasing number of studies report treatment results of peripheral AVMs according to the Yakes classification. However, the applicability of Yakes classification to patients with previous treatments is not well studied in the literature. There is no clear data in this regard. In this study, the percentage of type 4 AVM in patients with previous treatment was 69.8% which was statistically higher than other types (p=0.03). Hence, it can be speculated that the angiographic architecture of AVMs with previous treatment resembles type 4 AVM in the Yakes classification. Another explanation for this may be that most of these types of AVMs were referred to our center after incomplete treatments, as our center is a tertiary referral center for hard-to-treat lesions such as type 4 AVM. This finding should be evaluated in other studies for better understanding.
This study has its limitations such as the retrospective nature of it, the relatively high number of patients who were lost to clinical follow-up, the wide variety of embolic/sclerosant agents used and the heterogeneity of the treatment protocol. Also, as this study was a retrospective study in nature, the placebo effect could not be controlled. Thus, the placebo effect should be kept in mind when interpreting the results of this study.
Conclusion
In this study, the angiographic architecture and outcomes were not always reflected in the QoL of patients. Therefore, we believe the alleviation of symptoms and improvement of QoL should be the main focus of endovascular AVM treatments.
Supplemental Material
sj-pdf-1-jet-10.1177_15266028231166546 – Supplemental material for Endovascular Treatment of Peripheral Arteriovenous Malformations (AVMs): Do Angiographic Outcomes Relate to the Quality of Life?
Supplemental material, sj-pdf-1-jet-10.1177_15266028231166546 for Endovascular Treatment of Peripheral Arteriovenous Malformations (AVMs): Do Angiographic Outcomes Relate to the Quality of Life? by Ferdi Çay, Gonca Eldem, Gökçe Aybeniz Sevim, Kamil Çağan Özdemir, Barbaros Erhan Çil, İbrahim Vargel and Bora Peynircioğlu in Journal of Endovascular Therapy
Supplemental Material
sj-pdf-2-jet-10.1177_15266028231166546 – Supplemental material for Endovascular Treatment of Peripheral Arteriovenous Malformations (AVMs): Do Angiographic Outcomes Relate to the Quality of Life?
Supplemental material, sj-pdf-2-jet-10.1177_15266028231166546 for Endovascular Treatment of Peripheral Arteriovenous Malformations (AVMs): Do Angiographic Outcomes Relate to the Quality of Life? by Ferdi Çay, Gonca Eldem, Gökçe Aybeniz Sevim, Kamil Çağan Özdemir, Barbaros Erhan Çil, İbrahim Vargel and Bora Peynircioğlu in Journal of Endovascular Therapy
Footnotes
Authors’ Note
This work has not been presented in any meeting, congress, or similar event.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.