
Abstract
Purpose:
Pelvic arteriovenous malformations (pAVMs) are congenital or acquired vascular anomalies, presenting with hematuria, menometrorrhagia, pelvic pain, and varices; they can be life-threatening in case of rupture. Surgical therapies have been proposed but endovascular embolization has been recognized as the primary modality. The aim of this article was to report a retrospective multicenter experience concerning embolization of pelvic AVMs and provide literature overview.
Materials and Methods:
We describe 18 patients (14 female and 4 male) diagnosed with pAVM and treated with minimally invasive methods. The pre-procedural imaging evaluation was based on transpelvic and/or transvaginal color Doppler ultrasound, contrast-enhanced computed tomography, and/or magnetic resonance. In 3 cases, the malformation was congenital and in other 15, acquired. Most common symptoms were menometrorrhagia, hematuria, pelvic pain and pressure, and heaviness in the lower abdominal region. In 10 cases (56%), only 1 procedure was required. Eight patients underwent multistage treatment.
Results:
Complete occlusion of the lesion in post-procedural angiography was observed in 12 patients (67%). No major periprocedural complications were observed. In 14 cases (78%), both satisfactory embolization and significant clinical improvement was achieved in long-term follow-up. Sixteen patients (88%) were at least satisfied with the clinical outcome. One patient reported subsequent successful pregnancy 5 years after the treatment.
Conclusion:
Hemodynamics of pAVM are variable and thorough understanding of the vessel anatomy is crucial in planning and choosing proper treatment. Both transarterial and percutaneous direct puncture embolization strategies appear safe, technically feasible, and clinically effective.
Clinical Impact
In this manuscript, we discuss the role of interventional radiology methods in the treatment of pelvic arteriovenous malformations along with its advantages, limitations and possible complications. In addition to this, we review the current literature and confront our findings with those made by other authors. We believe that modern endovascular methods offer safe and reliable alternative for traditional surgical therapy and should be therefore considered during multidisciplinary treatment of these patients.
Introduction
Pelvic arteriovenous malformation (pAVM) is a rare condition defined by an abnormal direct communication between arterial and venous districts, without interposing capillary bed, inducing blood-flow diversion, and increase of the pressure gradient in the venous system; the estimated prevalence in general population is less than 1%.1,2 Whereas acquired pAVMs arise from trauma, surgery, or delivery, congenital lesions are caused by abnormal endothelial cell proliferation.3,4 Pelvic AVMs most commonly present with abnormal vaginal bleeding, ranging from spotting to life-threatening bleedings, pelvic pain or pressure, venous insufficiency, hematuria, and recurrent abortions. 5 As far as the diagnosis is concerned, ultrasonography, especially color Doppler with evidence of enlarged pelvic vessels with turbulent high-velocity blood flow is often the initial imaging modality in the setting of suspected pAVM. 6 Both pelvic computed tomography angiography (CTA) and magnetic resonance angiography (MRA) might be useful modalities in delineating the vascular anatomy and evaluation of involvement of adjacent organs and structures; nonetheless, digital subtraction angiography (DSA) remains the gold standard in the diagnosis of pAVMs. Traditional surgical treatment of pAVMs included surgical ligation of the feeding arteries and excision of the aneurysmal tissue, but it was associated with poor clinical results 7 and high rates of relapse.
Therefore, many centers refer patients with pAVMs for endovascular embolization, which proved to be a safe and feasable method.8–10 However, due to the rarity of pAVM prevalence, the available literature on endovascular therapy is scarce and limited mainly to case reports.5,8,9
The aim of this article is to present a multicenter experience with minimally invasive treatment for patients with pAVM and to review currently available literature.
Materials and Methods
Study Participants
This retrospective study was designed to evaluate the procedural and clinical outcome of minimally invasive treatment in patients diagnosed with pAVMs from 2010 to 2022. The study was approved by the local institutional review boards and was conducted in compliance with the Declaration of Helsinki. Written informed consent for the procedure was acquired the day before it commenced from each patient. Inclusion criteria were (1) age ≥18 years; (2) pAVM diagnosis based on clinical history and transvaginal ultrasound (TVUS), CTA, MRA, and/or DSA; and (3) follow-up at least 6 months after the final procedure. Exclusion criteria were (1) ruptured pAVM treated in emergency and (2) previous surgical treatments of the lesion. Demographic and clinical information were collected from electronic records and interviews.
Imaging protocol
The preprocedural imaging evaluation was based on transpelvic and/or transvaginal color Doppler ultrasound (CD-US); contrast-enhanced computed tomography (CTA) and/or magnetic resonance (MRA) were acquired subsequently in all cases.
After dismission, patients were checked by phone or chat at 2 weeks and then were visited at 30 days for clinical investigation and CD-US evaluation. A contrast-enhanced CT or MR was acquired at 3 months from intervention to detect eventual lesion residual; if patients did not present contraindications to MR scan (eg, claustrophobia, metallic implants), this was the preferred modality, especially in young subjects, to reduce x-ray exposure.
Endovascular Procedures
All interventions were performed by interventional radiologists having more than 5 years’ experience in endovascular embolization. Procedures were conducted in an inhospital regimen.
In angiosuite, through monolateral femoral access, first a panoramic aortoiliac DSA from the level of renal arteries was acquired to visualize arterial feeders. Afterward, selective injections were carried out, depending on feeders’ origin; endovascular strategy was accordingly customized case by case, based on the angioarchitecture. Superselective liquid embolizations were achieved: the type of microcatheters and embolics depended on local availability and operator preferences. In feasible cases, direct puncture technique was applied. Technical success was defined as complete exclusion of the malformation or occlusion of >75% of the lesion at last DSA run, with noticeably slower blood inflow (Figure 1).
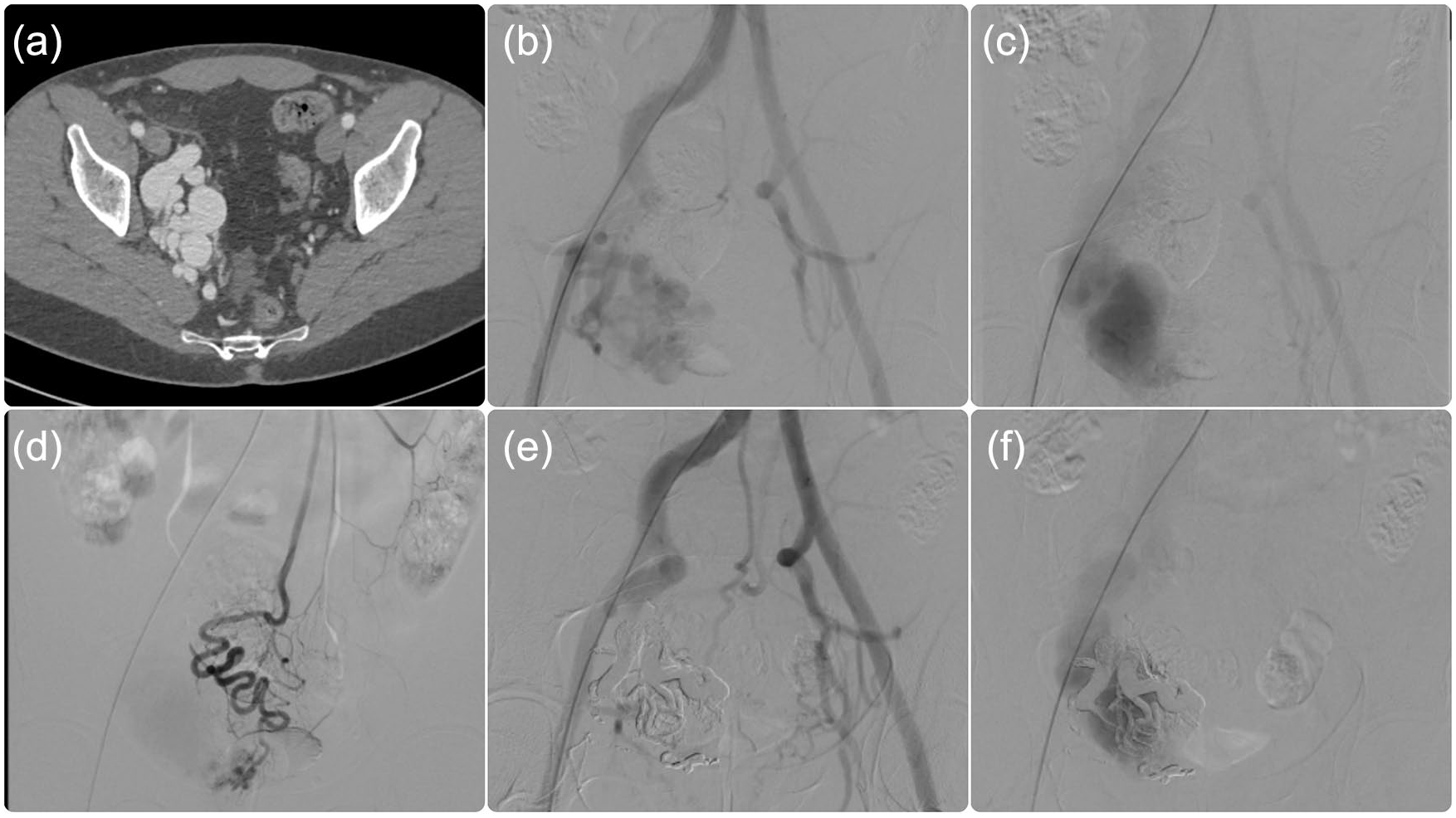
A 31-year-old male patient with no history of surgery or pelvic trauma was admitted to the hospital due to hematuria. Pelvic contrast-enhanced CT disclosed the presence of enlarged vessels in the arterial phase (A). Pre-procedural aortoiliac DSA showed AVM refurnished from the feeders originating from the right internal iliac artery with early venous drainage in right internal iliac vein (B, C). Additional blood supply from the superior rectal artery was noted (D). Superselective embolization with Onyx was performed using a 2.4 microcatheter (E). Final DSA disclosed massive reduction of the arterial component and persistent venous outflow (F). The patient is seen regularly in an outpatient setting. AVM, arteriovenous malformation; CT, computed tomography; DSA, digital subtraction angiography.
Procedural complications were evaluated according to the CIRSE classification system. 11
Mechanical closure device or manual compression of the site of puncture was applied based on the center experience and patient’s anatomy. Based on clinical-radiological follow-up, subsequent procedures were scheduled.
Procedures were performed with anesthesiologic support for analgosedation; antibiotic prophylaxis was provided in all cases.
At dismission, anti-inflammatory and painkillers were prescribed for 1 week.
Follow-up Protocol
Embolization outcomes were assessed on the postoperative imaging examinations (CD-US after 1 month, CT/MR at 3 months follow-up). Information on clinical results, long-term complications, and fertility rate was collected. Clinical success was defined as a complete resolution or significant improvement of symptoms without additional therapies. Patients’ clinical outcomes were objectively evaluated with a visual analogue scale (VAS) when available.
Results
Patients’ Demographics and Clinical Characteristics
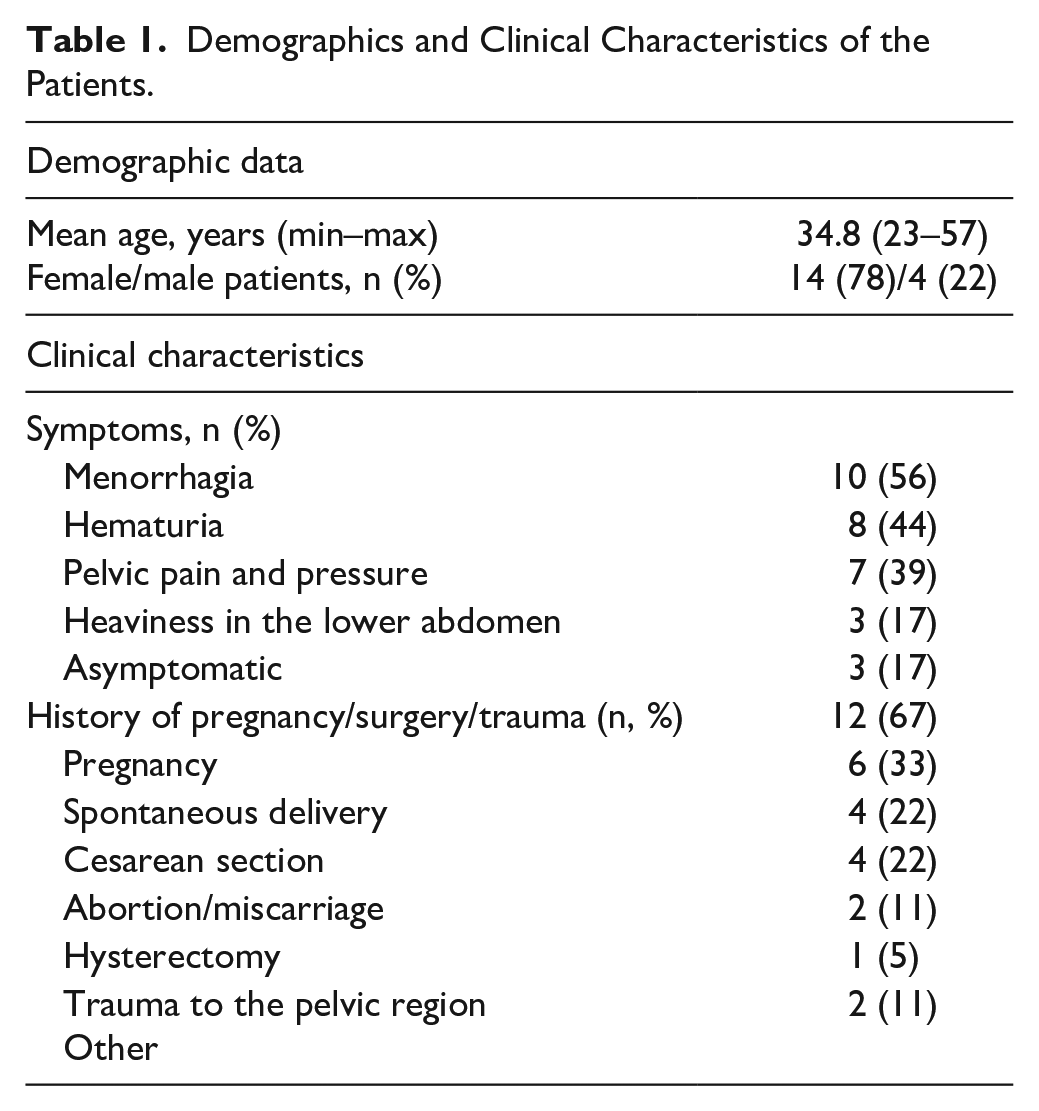
Twelve patients who were initially suspected for pAVM and were eventually diagnosed with other vascular lesions were excluded from the study. Eighteen patients (14 women and 4 men; mean age of 35 years, range = 23–57 years) were finally included. Most common symptoms were menometrorrhagia, hematuria, pelvic pain and pressure, and heaviness in the lower abdominal region. Two male patients were asymptomatic and the lesions were incidentally found during urologic US examination. Thirteen out of 14 female patients (93%) had a history of pregnancy or some kind of gynecologic intervention (cesarean section, hysterectomy, or intrauterine ablation). Patients’ demographics are presented in Table 1.
Demographics and Clinical Characteristics of the Patients.
Pre-procedural Imaging Findings and Endovascular Treatment
All patients underwent imaging examinations that included TVUS and CTA, and/or MRA. All pAVMs were then confirmed in DSA. A majority of the lesions was supplied by both uterine arteries (11/18, 61%). Other blood supply originated from unilateral uterine arteries, inferior mesenteric artery, main hypogastric trunk, and median sacral artery. All arteriovenous malformations were classified according to the Yakes AVM classification system. 12 Seven pAVMs were type IIIA or IIIB, 5 were type II, and 3 were types I and IV. In addition to this, in 2 cases, secondary procedures were performed using direct puncture technique. Most commonly used embolic materials included Onyx, cyanoacrylate glue, ethanol, and coils. Used microcatheters’ sizes ranged from 2.8 to 1.5 French. No periprocedural major (grade >3) complications were observed. In 2 patients, inguinal hematoma occurred (grade I). The number of required endovascular procedures ranged from 1 to 6. The final DSA run disclosed complete or near complete embolization in 12 cases (67%). Pre-procedural imaging findings and endovascular treatment details are shown in Table 2.
Pre-procedural Findings and Procedural Details of the Patients.
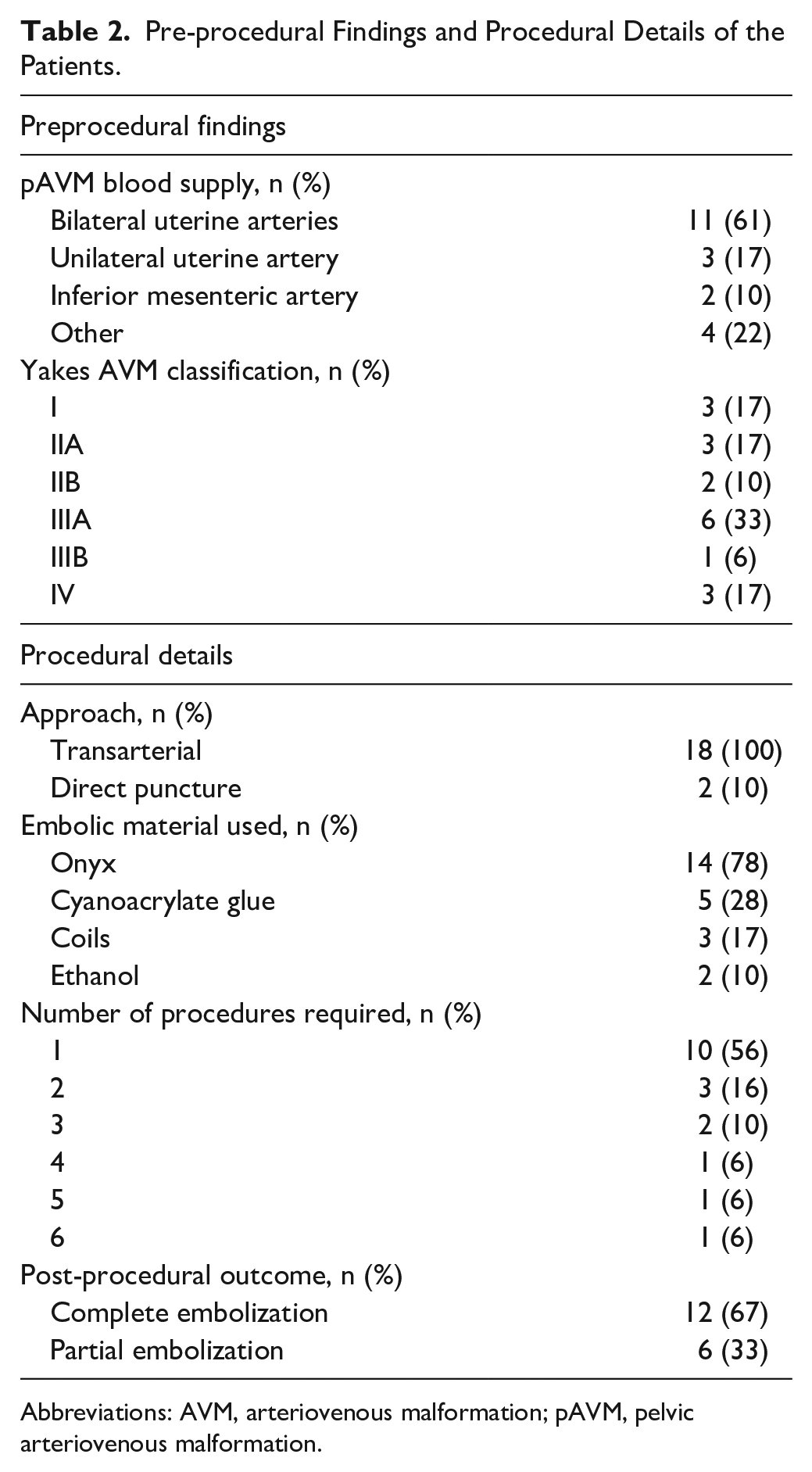
Abbreviations: AVM, arteriovenous malformation; pAVM, pelvic arteriovenous malformation.
Follow-up
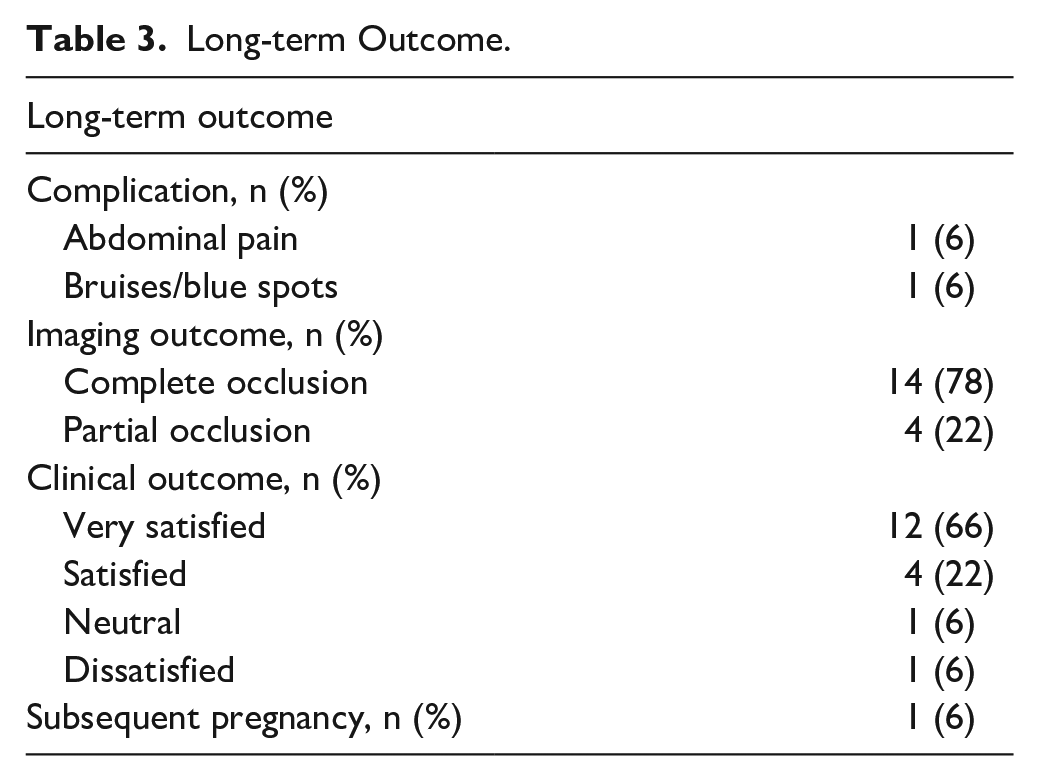
Clinical and imaging follow-up were performed at least 6 months after the final endovascular procedure. During this period, a patient reported abdominal pain and discomfort that started a few days after the treatment and were resolved within the week. Another patient observed bruises/blue spots on the lower abdominal area—they resolved within 2 weeks after the procedure. Imaging examinations disclosed complete or near-complete exclusion of the pAVM in 14 cases (78%). Residual was noted in 4 patients (22%). Sixteen patients were satisfied with the clinical outcome (12 were “very satisfied” and 4 were “satisfied”). One patient reported subsequent successful pregnancy 5 years after the treatment. Long-term results of the endovascular treatment are presented in Table 3.
Long-term Outcome.
Discussion
Minimally invasive endovascular methods are becoming first-line treatment modalities in many centers worldwide for the treatment of patients with pAVM. This study was designed to present a multicenter experience with pAVM patients presenting with a wide variety of symptoms and who underwent endovascular therapy with special attention to the methods used, procedural and clinical outcome, complications, and long-term results. A relatively high rate of complete occlusion (78%) was observed with only a few minor complications (2 cases). The use of embolic material was determined by the hemodynamical and anatomical conditions of the lesion and was individualized in every case. Technical development allows personalization of the treatment, thanks to the wide range of embolic agents (eg, coils, cohesive liquids, and glue). Overall, a vast majority of the patients (88%) reported to be at least satisfied after the treatment. Although only a few of them expressed their desire to become pregnant after the treatment, we noted a successful pregnancy following the procedure in 1 case.
Proper diagnosis in patients with pAVM remains challenging as the presenting symptoms are nonspecific and range from subtle (discomfort, pain) to serious (hematuria, venous insufficiency) or even fatal. They may also mimic other diseases, such as, for example, lumbar disk herniation. 8 Nonetheless, they are usually asymptomatic and are detected incidentally. 13 However, in our study, only 2 patients were asymptomatic and 16 reported some symptoms on admission.
A majority of pAVMs are acquired and arise from pelvic trauma, gynecological surgeries, gestational trophoblastic disease, or delivery. 1 Congenital lesions are rare and are characterized by rich vascularity and numerous anastomoses rather than fistulous communications patterns. 1 Only a limited number of publications on congenital pAVM are available in the current literature.14,15 Our findings are in line with these data—a majority of enrolled patients reported history of pregnancy, surgery, or trauma to the pelvic region.
Ultrasonography (US) is often the initial tool in the setting of suspected pelvic AVM. Usually, the use of Doppler in abdominal or transvaginal examination shows the presence of enlarged uterine vessels with turbulent blood flow, but cases of successful diagnosis in transrectal US are reported.15,16 Although US is valuable for screening and might eliminate the need for intensive examinations in the majority of cases, further examinations, including CT, MR, and DSA are required to exclude other vascular lesions. In our cohort, 12 patients were excluded from the study after additional imaging, which ruled out the presence of arteriovenous malformation suspected in the US.
In terms of pAVM feeding vessels, the uterine arteries are the most common culprit arteries. In our cohort, we observed cases with involvement of other vessels (eg, inferior mesenteric artery, hypogastric artery, and median sacral artery) but indeed nearly 80% of lesions were supplied by the uterine arteries. Nonetheless, the presence of extrapelvic blood supply is more characteristic for congenital lesions that are more technically demanding and might require multi-session treatment. Hemodynamic conditions (feeding arteries, nidus, and draining veins) determine the treatment and, in case of endovascular approach, the use of embolic material. In our study, the most commonly used embolic material was Onyx that is a liquid embolic widely used in the treatment of peripheral and intracranial AVM.17,18 As far as the treatment of pAVM is concerned, Onyx has been used for more than 2 decades for both elective and emergency cases.19,20 Apart from Onyx, other liquid embolic agents (eg, PHIL) was reported to be successfully implemented in the treatment of pelvic AVM. 21 Other embolic materials included coils, glue, and ethanol. Murakami et al 13 observed that both glue and ethanol are suitable for filling the nidus in selected patients. Glue was also the most common agent in one of the biggest series available in the literature on endovascular treatment of pAVM published by Jacobowitz et al. 22 As far as the coil embolization technique in the treatment of arteriovenous malformations is concerned, the use of this embolic material is a matter of debate as it may result in proximal feeder embolization and non-complete exclusion of the nidus. Nonetheless, several authors reported successful treatment of uterine AVMs using this technique.23,24 In our experience, coils might be effective and safe in selected patients also in case of pAVM.
In case of complex pAVM, multistage treatment was conducted. In total, 8 patients (44%) underwent multiple endovascular procedures. In these challenging cases, a combination of various embolic agents and approaches (transarterial and direct puncture) was required. Worth mentioning is the fact, that 3 cases in which >3 procedures were needed were congenital lesions that are reported to be more complex and challenging to treat. 1 We did not try the transvenous approach that is reported to be successful in selected huge pelvic AVM associated with prominent outflow veins, but carries the potential risk of nidus rupture as a result of elevated intravenous pressure. 25 Apart from 2 groin hematomas, which did not require surgical interventions, no procedure-related complications were observed in our cohort.
As for all arteriovenous malformations, the goal of the endovascular treatment is the occlusion of the point of fistula or the exclusion of the nidus. The reported clinical and technical success rates range from 70% to more than 90%.26,27 Our results stay in line with these findings—although the post-procedural success rate was lower (68%); control imaging examination disclosed complete occlusion in 78%. In addition to this, a vast majority of the patients (88%) reported to be at least satisfied with the clinical outcome of the procedure.
A detailed overview of currently available literature presenting outcome of pAVM treatment is presented in Table 4.
Review of Currently Available Literature on Treatment of pAVM.
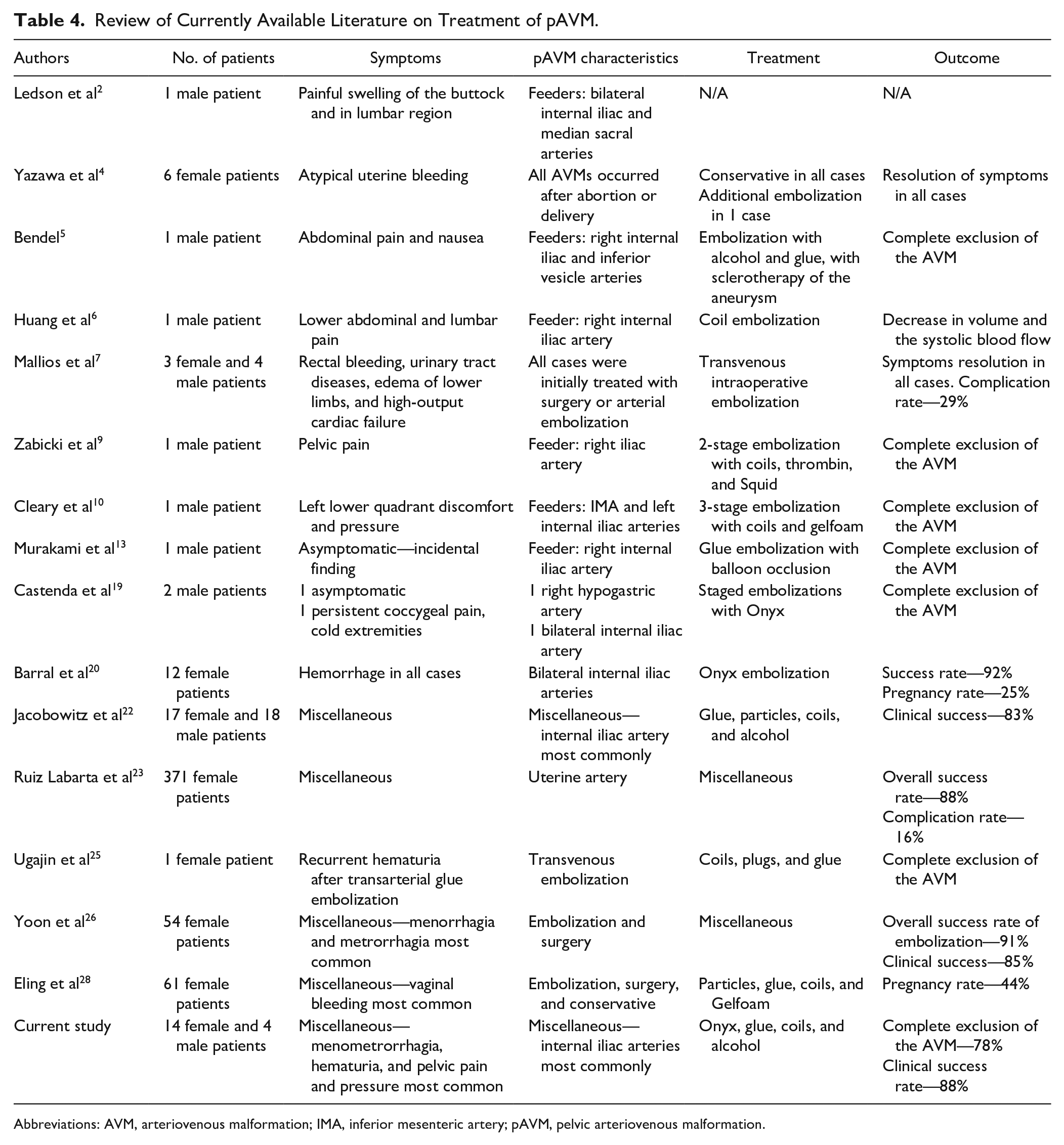
Abbreviations: AVM, arteriovenous malformation; IMA, inferior mesenteric artery; pAVM, pelvic arteriovenous malformation.
The question of fertility after endovascular pAVM treatment remains a matter of debate. There are several reports on successful pregnancies following the embolization.28,29 Thanks to novel embolic materials, the risk of nontarget embolization and ovarian failure is low. Similarly, the risk of uterus ischemia caused by bilateral uterine artery embolization is very low as the uterine collateral network is rich. 30 Consequently, no reports of uterine necrosis following the pAVM treatment are available in the literature.
Our study had several limitations. First, our sample size was small although the study was performed in a multi-tertiary center. Therefore, the significance of our results and of the conclusions requires further validation in future studies. However, data on larger groups of patients with pAVMs and their treatment have been lacking because the pathology is rare. Hence, our results may provide the pilot data for further study. Second, our study lacks the control arm that included the patients treated with other methods. Nonetheless, surgical treatment of pAVM was associated with poor clinical results and often hysterectomy was recommended. 31 Finally, we do not provide long-term follow-up that actually would detect eventual disease relapse at distance.
In conclusion, our study confirms that endovascular embolization is safe and effective in treatment of patients with pAVM regardless of the origin of the lesion. A wide range of available embolic materials enables personalized therapy that increases the chance of successful treatment of both relatively simple and complex AVM. It may also preserve the fertility; however, further studies are required to confirm these findings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.