
Abstract
Objective:
The purpose of this retrospective cohort study is to report outcomes of endovascular aortic repair (EVAR) with the novel endograft, Ankura (Lifetech Scientific, Shenzen, China).
Methods:
We identified all patients who underwent elective EVAR with Ankura stent graft in a tertiary unit from January 2015 to November 2021. Patients with ruptured infrarenal and juxtarenal aortic aneurysms were excluded from the study. All patients were anatomically suitable according to the instructions for use (IFU). Follow-up (FU) included computed tomography angiography (CTA) at 1 month, 12 months, and yearly thereafter if endoleak (EL) was not present. Primary outcomes included technical success (primary and secondary) and 30-day overall mortality and morbidity. Secondary outcomes included late overall and aneurysm-related mortality as well as influence of suprarenal fixation of the endograft on renal function at 12 months using eGFR (CKI-EPI formula).
Results:
The Ankura endograft was successfully implanted in 116 patients (mean age=71.1 years, 96.5% male). Mean aneurysm diameter was 62.3 mm. Median FU was 34 months (2-72 months). Primary and secondary technical success were 95.7% and 100%, respectively. Overall type I EL was 5% (2 proximal, 3 distal) and type II EL was 13%. Thirty days mortality and morbidity were 0% and 5.2%, respectively. All-cause mortality during FU was 13.9% (n=16); aneurysm-related mortality was 2.6% (n=3). Limb endograft patency was 100%. Freedom from reintervention was 98.2% at 2 years, and 97.4% at 4 and 6 years respectively. There was a statistically significant difference between preoperative (73.69 mL/min/1.73 m2) and postoperative (66.66 mL/min/1.73 m2) eGFR at 12 months (p<0.001).
Conclusion:
Ankura endograft has demonstrated an efficacious durability with low aneurysm-related mortality and high iliac limb patency rate. Elective EVAR is associated with significant decline in renal function at 12 months in our study. Larger series studies are necessary to evaluate long-term safety and efficacy of Ankura endograft.
Clinical Impact
Ankura stent graft is a novel PTFE endograft with suprarenal fixation for infrarenal aneurysm repair. This retrospective cohort study of 116 patients provide a first “picture” of Ankura safety and efficacy in a European tertiary vascular center. High technical success rate, low aneurysm related mortality and high limb patency rate are the main findings of the study with a negative impact of suprarenal fixation on kidney function during follow up.
Introduction
Abdominal endovascular aneurysm repair has spread all over the world and become the primary treatment modality in patients with suitable aneurysm anatomy and acceptable life expectancy. 1 Randomized clinical trials (RCTs) have established the benefits of endovascular aortic repair (EVAR) against open surgery regarding early morbidity and mortality with no significant differences in long-term outcome.2–4 It has evolved the last 2 decades with progressive improvement in materials, delivery mechanism profile, fixation mechanisms, conformability in challenging aortic anatomy’s preventing endoleaks (ELs), migration or limb thrombosis with subsequent reduction of secondary interventions, improving aneurysm-related morbidity and mortality. One of the novel stent grafts that has been introduced in the European market is Ankura endograft (Lifetech Scientific, Shenzhen, China), which is CE marked since 2014, and the first European case was in Greece in 2015. The aim of this study is to report outcomes of Ankura stent graft over the last 6 years in a tertiary vascular center.
Materials and Methods
Study Design and Patient Population
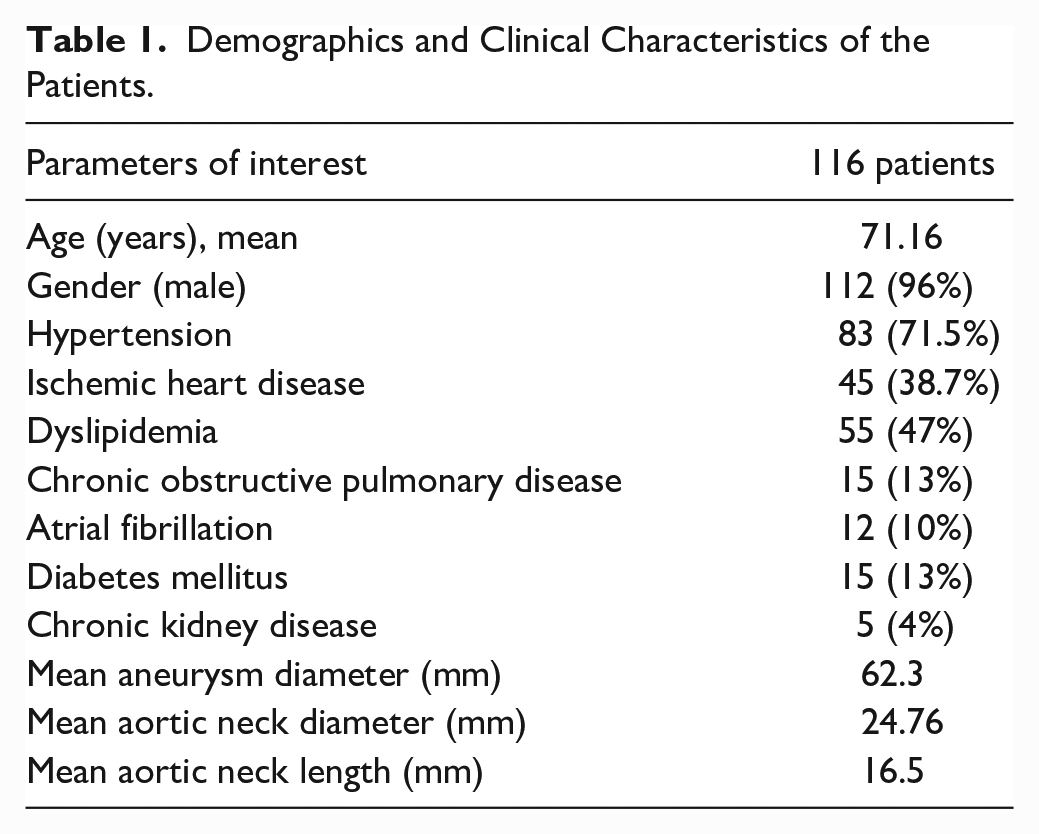
All records of patients who underwent elective EVAR with Ankura stent from January 2015 to November 2021 at a tertiary vascular unit of Northern Greece were evaluated using a prospectively collected database. Thirty-six patients with contained/free rupture of abdominal aortic aneurysm (AAA) and juxtarenal aneurysm treated by chimney technique were excluded, leaving 116 patients for analysis. The demographics and clinical characteristics of the patients are presented in Table 1. The primary indication for EVAR was an AAA with transverse diameter >55 mm in men and >50 mm in women, and saccular aneurysm >30 mm in diameter according to our clinic protocol. All patients treated with Ankura stent graft fulfilled the instructions for use (IFU) criteria, including proximal aortic neck length >15 mm long, aortic neck diameter of 18 to 32 mm, aortic neck angulation <60°, distal iliac artery sealing zone >15 mm, and distal iliac artery diameter 8 to 22 mm. Life expectancy >2 years in the presence of concomitant neoplasia was an inclusion criterion in our study after oncology consultation. Preoperative planning with computed tomography angiography (CTA) at 5 mm slice thickness was performed using Radiant Dicom viewer (Medixant, Poland) and Endosize (Therenva, France). Primary outcomes of the study included technical success (primary and secondary) and 30-day overall mortality and morbidity. Secondary outcomes included late overall and aneurysm-related mortality as well as influence of suprarenal fixation of the device on renal function at 12 months using eGFR (CKI-EPI formula) according to the Kidney Disease Improving Global Outcomes guidelines. The endograft was oversized 15% to 20% based on luminal diameter of the aortic neck. A protocol was approved by the institutional review board of our hospital. The study was not funded externally. All patients provided written informed consent before operation. The study was carried out according to the declaration of Helsinki.
Demographics and Clinical Characteristics of the Patients.
Device Characteristics
Ankura is a 3-piece components endograft. It consists of bilayer e-PTFE membrane cover supported by nitinol stents. The membrane offers durability, biocompatibility, and low permeability. 5 The endograft has spiral woven connecting bar on the limb and a connecting bar for the last 2 waves of the main body between PTFE layers offering flexibility and preventing shortening of the stent graft. 5 The number of nitinol stents ranges from 4 to 5 in the main body, depending on the size of the endograft, which, in conjunction with smaller waves in size, provides high radial force and flexibility. 5 A bare stent with 6 barbs is located in the proximal part of the main body. Anchors are 3.5 mm in size and have 30° to 45° to the outer side of the bare stent. A part of the bare stent is incorporated in the membrane providing additional radial support. The delivery system has a tip capture mechanism for precise deployment. 5 There are no sutures in the main body, nor on the limbs; the stents are nipped between the e-PTFE membranes and attached to them under thermal treatment that minimizes pinhole leakage (Figure 1). The sheath is hydrophilic-coated. The main body delivery system ranges from 21 to 23 Fr and iliac in 18 Fr. Iliac stent grafts range in size from 14 to 28 mm in tube and tapered configurations. There are 7 radiopaque markers to aid accurate placement and deployment of the endograft. Proximally an “O-shaped” and an “8-shaped” markers are found, corresponding to the ipsilateral and contralateral limb, respectively. The contralateral limb has 3 markers, an “e-shaped” an “o-shaped” and a “v-shaped” in downward direction. The limb must be deployed at the level of the “e-shaped” marker. The ipsilateral limb has 2 “v-shaped” markers.
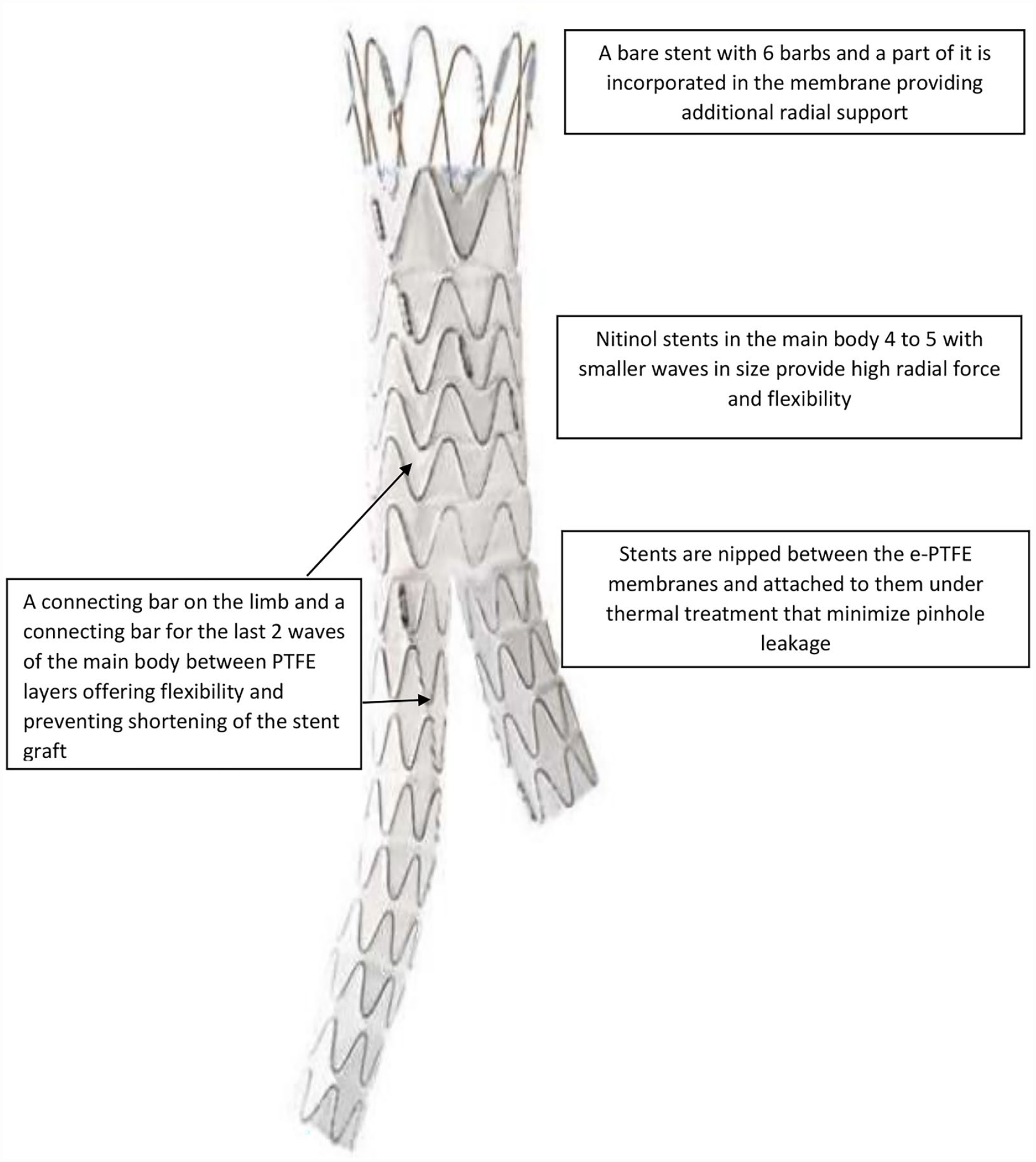
Device characteristics of the Ankura stent graft.
Procedural Technique
All procedures were performed under general or regional anesthesia. Bilateral femoral exposure was performed via surgical cutdown. After systemic heparinization, the delivery system is loaded over an extra stiff guidewire (Lunderquist; Cook Medical, Bloomington, Indiana). An angiography is performed at the level of renal arteries. The delivery system is slowly turned in order the contralateral “8-shaped” marker appears as a straight line. The endograft is partially deployed until the contralateral limb is released. Catheterization of the limb is then followed. After exchange of the stiff with an extra stiff guidewire, the contralateral iliac endograft is advanced and deployed. The main delivery system is then fully deployed followed by deployment of the ipsilateral limb. Balloon molding of the iliac limbs from the level of flow divider is subsequently performed. A final aortography confirms exclusion of the aneurysm and absence of EL I and III. All patients are discharged under lifelong single antiplatelet therapy or antithrombotic regimen (warfarin, novel oral anticoagulants [NOACs]) in case of mechanical heart valve or atrial fibrillation.
Follow-up
According to our EVAR protocol, patients underwent CTA at 1 month, 12 months, and then yearly thereafter for the first 4 years and then every 2 years. In the case of EL at 1 month, an additional CTA examination was performed at 6 months. Patients with renal insufficiency (stage 3-5 chronic kidney disease [CKD]) underwent unenhanced CT of abdomen and/or ultrasound. If there was an increase of sac diameter >5 m, a CTA was performed with primary assessment of sac diameter, the presence of EL, device migration, and limb thrombosis. Evaluation of decline of renal function during FU was performed using eGFR values at 12 months compared with preoperative eGFR values.
Definitions
All definitions and reporting relating to co-morbidities, cardiovascular events, and clinical outcomes were based on the Society for Vascular Surgery reporting guidelines (standards) for patients undergoing endovascular procedures for EVAR. 6 Perioperative morbidity and mortality were defined as complications and death within 30 days of operation. ELs were classified according to the White-May definitions. 7 Contrast-induced nephropathy was defined as impaired renal function indicated by either a 25% increase in serum creatinine from baseline or a 0.5 mg/dL increase in absolute value within 48 to 72 hours after intravenous contrast administration. 8 The estimated glomerular filtration rate (eGFR) was determined using the abbreviated Modification of Diet in Renal Disease study equation. 9
Statistical Analysis
Statistical analysis was performed using SPSS for Windows (version 27; IBM Corporation, Armonk, New York). Continuous variables are presented as mean and standard deviation (SD). Mann-Whitney U test, χ2 test, and Fisher exact test were used to compare outcomes as necessary, based on normality of distributions. Discrete variables are presented as absolute values and proportions. Freedom from reinterventions and survival were estimated using Kaplan-Meier method. The level of statistical significance is set at a=0.05.
Results
The Ankura stent graft was successfully implanted in 116 patients (mean age=71.1 years, 96.5% men). Mean aneurysm diameter was 62.3 mm (range=46-99 mm). Mean aneurysm neck diameter and neck length were 24.76 mm (range=21-32 mm) and 16.5 mm (range=15-22 mm), respectively. Two ELIa and 3 ELIb on final angiography were managed by deployment of a cuff proximally and iliac limb extensions distally. Primary and secondary technical success were 95.7% and 100%, respectively. No open conversions occurred. Common femoral endarterectomy was performed in 2 patients due to rupture of calcified plaque at the femoral bifurcation; 2 patients underwent external iliac artery stenting with bare self-expandable stents due to local dissection. Type II EL due to patent lumbar arteries was noticed in 13 patients (13%). The inferior mesenteric artery was occluded in all patients, verified by CTA preoperatively. Eleven patients developed contrast-induced nephropathy postoperatively. All patients were successfully managed with intravenous hydration. Temporary hemodialysis was not required in any patient. Perioperative mortality and morbidity were 0% and 5.2%, respectively.
Outcomes in Follow-up
Median follow-up (FU) was 34 months (range=2-72 months). No patient was lost during FU. Type Ia EL was detected in 3 patients, the first at 21 months, the second at 47 months, and the third at 12 months (2.6%). Etiology was progression of the aneurysmal disease at the aortic neck despite optimal endograft oversize. All patients presented with rupture of AAA and significant hemodynamic instability. Open conversion with endograft explantation and aorto-aortic tubular graft anastomosis was performed to the first 2 patients, who eventually died at intensive care unit postoperatively. Endovascular bail out repair with double chimney technique and proximal cuff extension was performed to the third patient in another facility. His postoperative recovery was uneventful and discharged the fifth postoperative day. An aorto-enteric fistula was noticed in one patient at 63 months. He presented with abdominal pain, loss of appetite, and upper gastrointestinal hemorrhage. The patient underwent an axillo-bifemoral bypass, endograft explantation, and aortic stump ligation. He died the 10th postoperative day due to multisystem organ failure. Type II EL was depicted in 10 patients during FU (8.6%); 7 of the leaks eventually subsided within 24 months and the rest remain without increase in sac diameter. No type III EL or limb graft thrombosis was noticed during FU. Long-term aneurysm-related mortality was 2.6% (n=3). The Kaplan-Meier estimates of freedom from reintervention were 98% at 24 months, and 97.4% at 4 and 6 years (Figure 2). Overall, all-cause mortality was 13.9% (n=16) at 6 years. Five patients died due to cancer, 5 patients due to ischemic heart disease, and 3 patients due to respiratory failure from Covid-19 infection. The Kaplan-Meier estimates of patient’s survival with all-cause mortality and aneurysm-related mortality are presented in Figures 3(A)-(B).
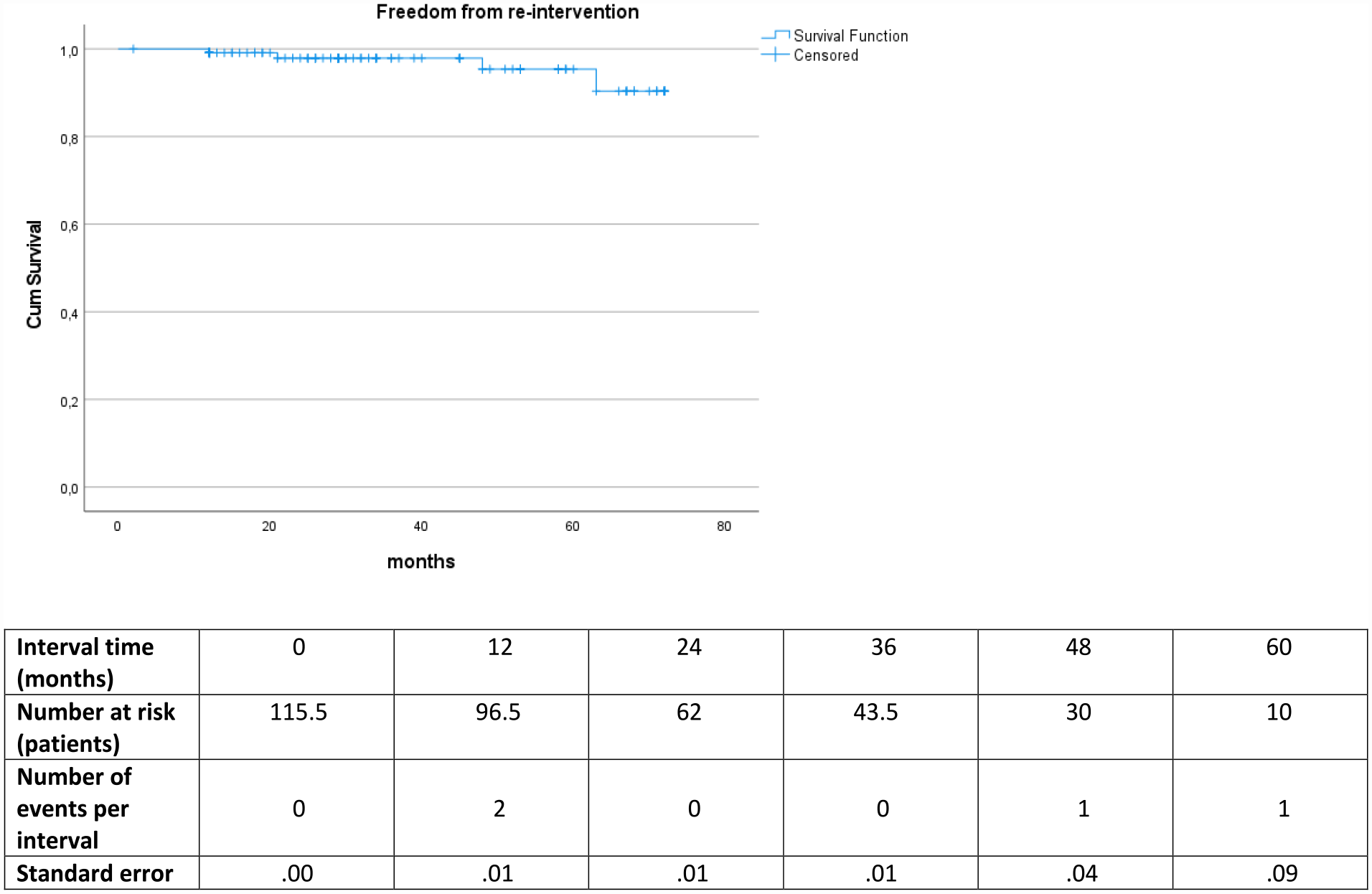
Kaplan-Meier analysis of freedom from re-intervention.
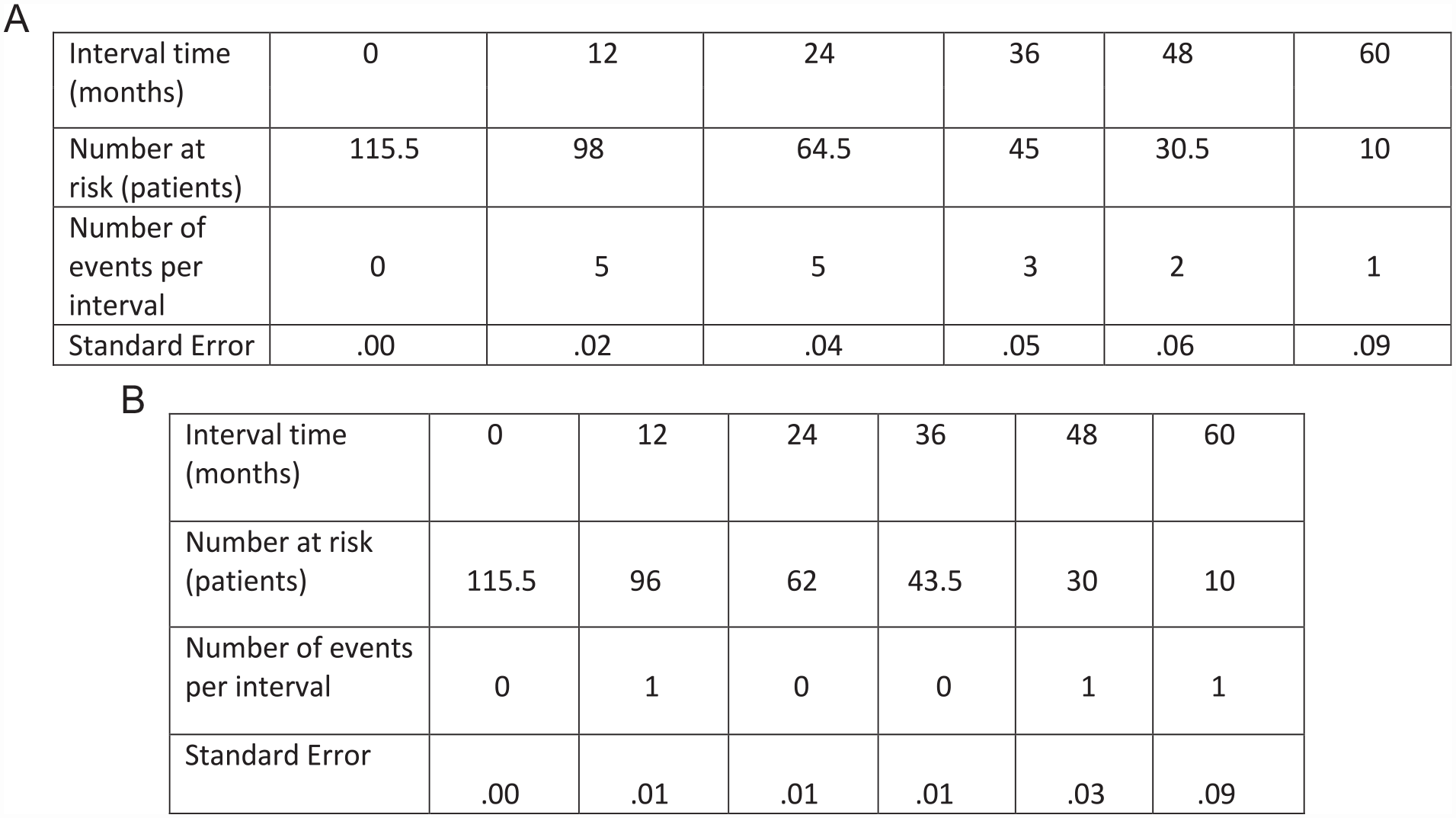
(A) Kaplan-Meier analysis of aneurysm-related mortality. (B) Kaplan-Meier analysis of all-cause mortality.
Outcomes of Renal Function
One hundred fifteen patients (99.1%) were available for evaluation of renal function using eGFR formula at 12 months. Four patients had preoperative higher creatinine levels than normal range (0.6-1.2 mg/dL) with stage 3A moderate CKD (GFR=45-59 mL/min). No patient had critical renal artery stenosis at preoperative CTA. There was not any deterioration of renal function during FU due to other causes (eg, medication, infection, heart failure, and dehydration). Mean preoperative eGFR was 73.68 mL/min/1.73 m2 (95% confidence interval [CI]=69.66-77.70) and postoperative eGFR was 66.66 mL/min/1.73 m2 (95% CI=62.07-71.25) (p<0.001). Of 4 patients with CKD, 2 progressed to end-stage renal disease during FU.
Discussion
Endovascular repair of AAA is steadily increasing over the last years and is considered the primary treatment modality in patients with suitable anatomy. 1 Decreased perioperative mortality and morbidity, decreased length of stay, and noninferior long-term mortality versus open repair are the main advantages of EVAR.2–4 Evolution of endovascular repair for AAA treatment has allowed many endografts to be designed and engineered. Ankura stent graft is one of the novel endografts that was launched in Europe in 2015. Outcomes with Ankura endograft in Western countries are limited, and the purpose of this current study was to explore the feasibility and safety of graft in AAA repair. Tumer et al 5 have published their experience with Ankura stent graft. A multicenter retrospective analysis with 100 patients who were electively treated from January 2018 and December 2019 was performed. All patients were compatible with IFU. Technical success was 100%. There was no early mortality or conversion to open repair. At 12 months no migration, no occlusion and migration were noticed. Two patients had El1b due to iliac artery dilatation who were successfully managed with iliac limb extension. Freedom from reintervention at 1 year was 98%. Albuquerque e Castro presented at LINC 2019 his experience with Ankura endograft. 10 Thirty patients were included in the study, where perioperative results were analyzed. Technical success was 100%. No early EL1-EL3 and migration were recorded. No surgical conversion, rupture, and in-hospital death occurred at 30 days.
Thirty-day mortality in our study was 0%, which is comparable with the major randomized trials.3,4,11,12 A major concern regarding durability of endografts is the fixation system and the progression of aneurysmal disease at the aortic neck. Ankura has a suprarenal fixation with a bare stent and active anchors providing active sealing at the aortic neck. In addition, a bare stent is incorporated in the dual PTFE membrane providing additional radial support. Aortic neck dilatation (AND) after EVAR has been reported in several studies in 10% to 36% of cases with subsequent loss of proximal fixation and increased susceptibility for ELIa and migration.13–15 Malach et al 14 have evaluated the effect of stent graft oversizing and the fixation type on AND. Three groups of patients with active suprarenal (SR), passive suprarenal, and active infrarenal fixation (IR) system as well as groups according to the degree of oversizing were included in the study. The study showed that infrarenal active fixation and oversizing of the endograft <10% had a minimum effect on AND. Active suprarenal fixation was associated with a significant change in suprarenal and infrarenal aortic diameter at 4 years FU. A systematic review by Kouvelos et al 16 encompassed 9721 patients (median age=71.8 years, 9439 men). The AND was noticed in 24.6% of patients (95% CI=18.6%-31.8%) for a period 15 months to 9 years after EVAR. The AND group was associated with higher incidence of adverse events (EL Ia, migration, and reintervention) (26% vs 2% in the group without AND). A recent single retrospective cohort study by Oliveira et al 17 evaluated risk factors and clinical relevance of AND after EVAR. Graft oversizing was 20% and 460 patients were included in the study. The AND was greater during the first year (5.2% [interquartile range (IQR) = 0%-11.7%]), which then decreased subsequently (2-4 years to 1.4%/year [IQR = 0.0%-4.5%], p=0.001), and was associated with suprarenal fixation endografts (t value = 7.9, p<0.001) and oversizing (t value = 4.4, p = 0.001). Authors concluded that baseline aortic diameter and suprarenal fixation system were associated with higher risk of AND post-EVAR. In our study, 3 patients were presented with ruptured AAA due to AND and subsequent ELIa. Conversion to open repair with eventually fatal outcome was performed in 2 patients, whereas the last one was managed successfully by endovascular double chimney bail out technique.
A great debate regarding the influence of fixation type to renal function has been raised in the last years. Several meta-analyses and multicenter retrospective cohort studies have been performed evaluating the impact of suprarenal fixation devices in renal function after EVAR18–23 with controversial results. The meta-analyses by Stather et al 19 identified a small but significant difference in patient’s outcome with SR fixation for renal function decline at the study end point compared with IF (SR 5.98% vs IR 4.83%; odds ratio [OR]=1.29, 95% CI=1.18-1.40 [p<0.001]). Renal artery stenosis (SR 2.4% vs IR 0.8%; OR=2.89, 95% CI=1.00-8.38 [p=0.05]), occlusion (SR 2.4% vs IR 0.8%; OR=2.89, 95% CI=1.00-8.38 [p=0.05]), and renal infarcts (SR 6.6% vs. IR 2.3%; OR=2.78, 95% CI=1.46-5.29 [p=0.002] opposed suprarenal fixation. Calderbank et al 18 performed a meta-analysis of renal injury after EVAR based on eGFR. The results did not show any significant difference in renal injury between SR and IR fixation systems at 12 months, OR=1.32 (95% CI=1.01e1.71, p=0.03, I 2 =28.4%); 5.1% for SR versus 4.6% for IR fixation. Zettervall et al 21 performed a retrospective analysis of patients who underwent EVAR with SR versus IR system from Vascular Study Group of New England. A total of 2574 patients were included in the study. Authors concluded that patients with SR fixation system endografts were associated with higher rates of renal function decline and longer length of hospitalization. However, the overall conclusion of all studies is that long-term data are necessary to establish and determine the effect of fixation system in renal function, and careful preoperative evaluation of patients with preexisting renal dysfunction is necessary. In our study, there was a statistically significant decline of renal function based on eGFR; mean preoperative eGFR was 73.68 mL/min/1.73 m2 (95% CI=69.66-77.70) and mean postoperative eGFR was 66.66 mL/min/1.73 m2 (95% CI=62.07-71.25) (p<0.001), with 2 of 4 patients with CKD progressed to hemodialysis during FU.
Iliac limb graft occlusion (ILGO) is a serious complication after EVAR with clinical presentation varying from asymptomatic to acute limb ischemia with severe sensory and motor deficits. 24 An incidence of 0% to 10.6% has been reported and several risk factors have been related to ILGO, including calcification, kinking and angulation of iliac arteries, limb graft oversizing, narrow aortoiliac bifurcation, external iliac artery distal landing zone, and endograft device type.24–28 Ankura stent graft has demonstrated 100% iliac limb patency rate in our study. Kissing balloon molding of iliac limbs from the flow divider, the absence of severe iliac artery calcification and stenosis in the distal landing zone, and the flexibility of the device could be associated with the absence of iliac limb thrombosis. Our study presents important limitations. It is a retrospective observational single-center study with not large number of patients, thus making comparison with results of other endografts difficult. However, it is a real non-industry-sponsored single-center study. The fact that it is a novel endograft arrived in Europe 7 years ago, our study provides a first “picture” of Ankura efficacy in elective repair of infrarenal AAA.
Conclusion
Ankura endograft has demonstrated an efficacious durability during FU with low aneurysm-related mortality and high limb patency rate. Suprarenal fixation system of the device significantly declines renal function at 12 months in our study. Long-term efficacy and safety of Ankura stent graft must be evaluated in larger series studies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.