
Abstract
Objectives:
Aortic diameters may differ significantly between patients with different gender and body size. The aim of this study was to relate absolute aortic diameters to age, sex, height, and weight of the patients and to correct for these factors by calculating the ratio between the infrarenal and the suprarenal aortic diameters.
Methods:
A total of 458 patients who underwent elective endovascular aneurysm repair (EVAR) between 2004 and 2018 were included. The aortic anatomy in this group of elective EVAR patients was compared with a control group of 75 patients without an abdominal aortic aneurysm (AAA). The aortic diameter was measured at 4 suprarenal points and 4 infrarenal points. Ratios were calculated by dividing the mean infrarenal neck diameter by 4 suprarenal measurements.
Results:
Patients in the aneurysm group had significantly larger suprarenal and infrarenal aortic diameters. The ratios between the mean infrarenal neck diameter and all 4 suprarenal measurements were larger in the AAA group than in the control group. In both groups, there was a significant correlation between the mean infrarenal neck diameter and sex, height, weight, and body surface area (BSA). However, in both groups, all 4 ratios between the mean infrarenal neck diameter and suprarenal aortic diameters were not correlated with age, sex, height, weight, or BSA, except for the ratio between the mean infrarenal neck diameter and the aortic diameter measurement proximal to the upper renal artery, which was correlated to weight and BSA in the control group.
Conclusion:
The mean infrarenal neck diameter is correlated with sex, height, weight, and BSA. However, when the suprarenal aortic diameter was used as an internal control for the mean infrarenal neck diameter, we were able to correct for these variations in aortic diameters due to sex and body size. The clinical relevance of this ratio in patients treated by EVAR has yet to be assessed in future research.
Clinical Impact
In the assessment for EVAR suitability the absolute diameter of the aneurysm neck is taken into account. We believe that using absolute diameters is not the appropriate way to assess this suitability, but that patient characteristics such as age, gender and body size, should be factored into this assessment. In this paper, we show that suprarenal and infrarenal aortic diameters are both significantly increased in patients with an aneurysm compared with patients without an aneurysm. Besides, we found that mean infrarenal aortic diameter is correlated with sex, height, weight, and body surface area. Finally, we propose a new ratio system, using suprarenal diameters as an internal control, to correct for aortic diameter variations due to sex and body size.
Keywords
Introduction
Endovascular aneurysm repair (EVAR) has nowadays evolved into the primary treatment of abdominal aortic aneurysm (AAA). Nevertheless, several studies have shown inferior results in patients treated with large infrarenal aortic neck diameters (IADs), as shown by a recent meta-analysis. 1 A large IAD is defined as a diameter of ≥28 mm.2 –4 A large IAD may be an indication that the proximal neck is already dilated and that, in these patients, significant aortic neck dilatation may occur after EVAR, with an increased risk for type IA endoleaks and proximal neck-related reinterventions.5,6 However, because aortic diameters may vary substantially due to sex, race, and body size,7,8 an absolute IAD may not be the best risk factor to predict a durable proximal seal in all patients. To correct for variations in IAD between people, the suprarenal aortic diameter may serve as an internal control. If a ratio between the infrarenal and suprarenal aortic diameter corrects for sex, race, and body size, it may be a better indicator for infrarenal aortic enlargement than the absolute diameter.
The aim of this study was to relate absolute aortic diameters to age, sex, height, and weight of the patients and to correct for these different diameters by calculating the ratio between the infrarenal and the suprarenal aortic diameters.
Patients and Methods
All patients who underwent EVAR between 2004 and 2018 in a single vascular referral center were included. Patients were identified by their operation codes, and medical records were reviewed. Patients were excluded if the preoperative computed tomography angiography (CTA) was not available and if they were treated for a ruptured AAA. These patients were compared with a control group of 75 patients without an AAA. Patients with a pulmonary malignancy and/or peripheral arterial occlusive disease (PAOD) without aneurysmal disease were handpicked, based on age and sex, to create a control group that was comparable to the aneurysm group with regard to risk factors and comorbidity.
Data Collection and Definitions
In both groups, the following patient characteristics and comorbidities were collected: age, sex, height, weight (at the time of surgery), tobacco use, diabetes, hypertension, hyperlipidemia, ischemic heart disease, congestive heart failure (an ejection fraction of <40%), cerebrovascular incident, renal insufficiency (estimated glomerular filtration rate of <60 mL/min/1.73 m2), pulmonary oncology, chronic obstructive pulmonary disease, and PAOD. Body surface area (BSA) was automatically calculated using the Mosteller formula. 9
Preoperative aortic anatomy was assessed using 3Mensio (Medical Imaging BV, Bilthoven, the Netherlands). All measurements were performed according to St George’s Vascular Institute protocol. Because this protocol has been proven to be an accurate method for assessment of aneurysm morphology with high interobserver repeatability, the measurements of the aortic diameter in this study were performed by only 1 investigator (GJB). 10 A central lumen line was automatically created and adjusted manually. The aortic diameters were measured outer-to-outer at 4 standardized suprarenal locations (at the level of the upper diaphragm, proximal to the celiac trunk, proximal to the superior mesenteric artery, and proximal to the upper renal artery) and at 4 standardized infrarenal locations (directly infrarenal, 5 mm infrarenal, 10 mm infrarenal, and 15 mm infrarenal) (Figure 1). The mean infrarenal neck diameter was calculated by adding the 4 infrarenal measurements and dividing by 4. Neck length was defined as more than 10% growth compared with directly infrarenal. If the neck length was shorter than 15 mm, the neck diameter prior to the start of the aneurysm was used as the fourth measurement. If the neck was shorter than 10 mm, the third measurement was replaced by the neck diameter prior to the start of the aneurysm, and the sum was divided by 3. In all patients, 4 ratios were calculated by dividing the mean infrarenal neck diameter by each of the 4 suprarenal measurements.
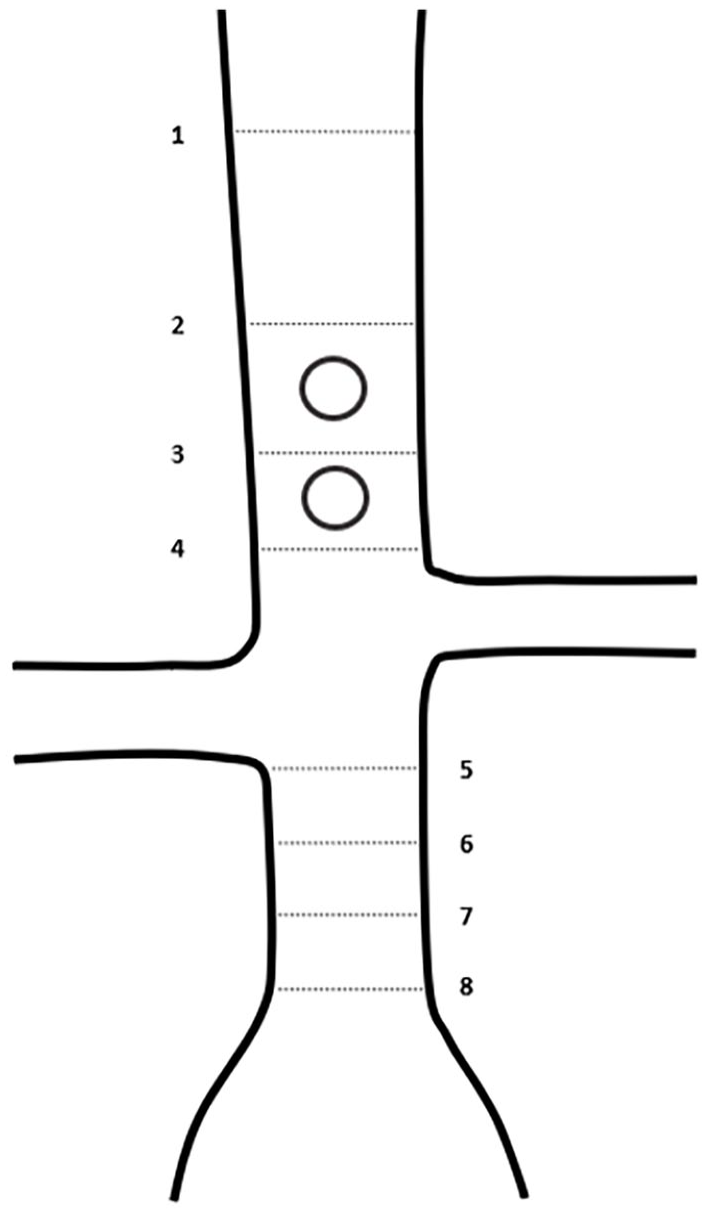
Schematic representation of the measurements: 1. Upper diaphragm. 2. Proximal to the celiac trunk. 3. Proximal to the superior mesenteric artery. 4. Proximal to the upper renal artery. 5. Directly infrarenal. 6. 5 mm infrarenal. 7. 10 mm infrarenal. 8. 15 mm infrarenal.
Statistical Analysis
Statistical analysis was performed using RStudio 3.6.1 software. 11 All numeric variables had skewed distribution, and therefore, only the Mann-Whitney U test was used. The Pearson χ2 test was used to evaluate categorical variables. Correlations between numeric variables were tested by the Pearson correlation coefficient statistic, based on the central limit theorem. Categorical variables were tested by analysis of variance. Significance was defined as a p value of <0.05.
Ethical Approval
This study was reviewed and approved by the Medical Research Ethics Committees United and the Maasstad Hospital Institutional Review Board. Informed consent was waived by the Maasstad Hospital Institutional Review Board.
Results
Endovascular aneurysm repair was performed in 529 patients between 2004 and 2018. We excluded 48 patients who were treated for a ruptured AAA and 23 patients who had no preoperative CTA, resulting in 458 eligible patients. The control group included 75 patients with pulmonary malignancy and/or PAOD with a CTA of the thoracic and abdominal aorta.
Patients’ characteristics were similar in both groups, except for an increased incidence of ischemic heart disease and renal insufficiency in the AAA group and more diabetes, pulmonary cancer, and PAOD in the control group (Table 1). However, the mean ratios between the infrarenal and suprarenal aortic diameter were not significantly different between diabetic and nondiabetic patients (0.901 vs 0.90; p=0.440), patients with or without ischemic heart disease (0.91 vs 0.90; p=0.441), patients with or without renal insufficiency (0.92 vs 0.90; p=0.261), patients with or without pulmonary cancer (0.90 vs 0.91; p=0.504), and patients with or without PAOD (0.89 vs 0.91; p=0.171).
Characteristics, Comorbidities, and Univariate Analysis.
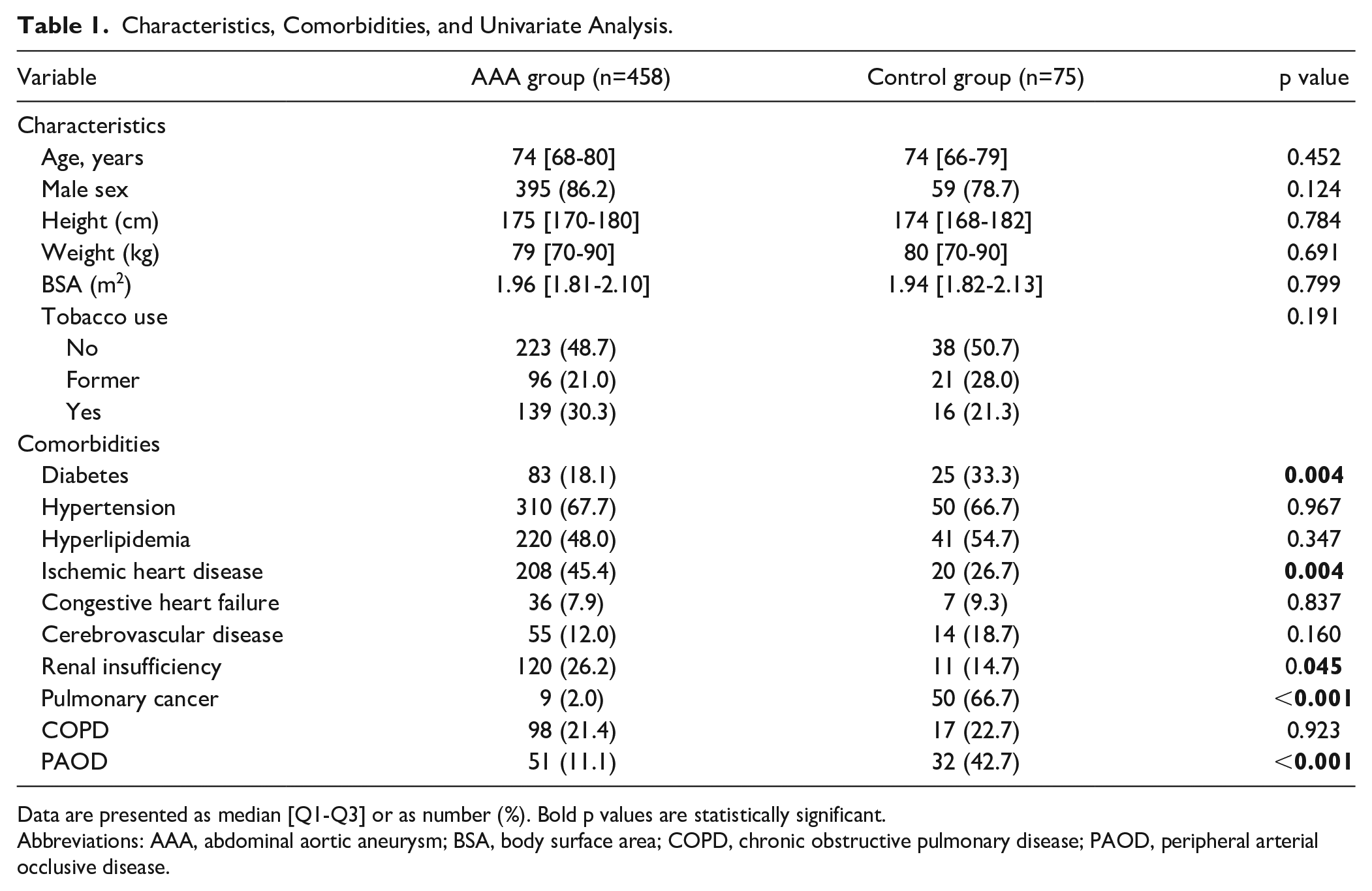
Data are presented as median [Q1-Q3] or as number (%). Bold p values are statistically significant.
Abbreviations: AAA, abdominal aortic aneurysm; BSA, body surface area; COPD, chronic obstructive pulmonary disease; PAOD, peripheral arterial occlusive disease.
Patients in the aneurysm group had significantly larger diameters of their suprarenal and infrarenal aorta compared with patients in the control group at all points that were measured. In addition, the ratios between the mean infrarenal neck diameter and all 4 suprarenal measurements were larger in the AAA group than in the control group. In both the AAA and control groups, the absolute suprarenal diameter measurements decreased toward the distal aorta, and consequently, the ratio between the mean infrarenal neck diameter and the suprarenal diameter measurements increased toward the distal aorta. In the control group, all 4 infrarenal diameter measurements were similar, but in the AAA group, the infrarenal neck diameter measurements increased toward the distal aorta (Table 2, Figures 2 and 3).
Aortic Diameter Measurements and Ratios.
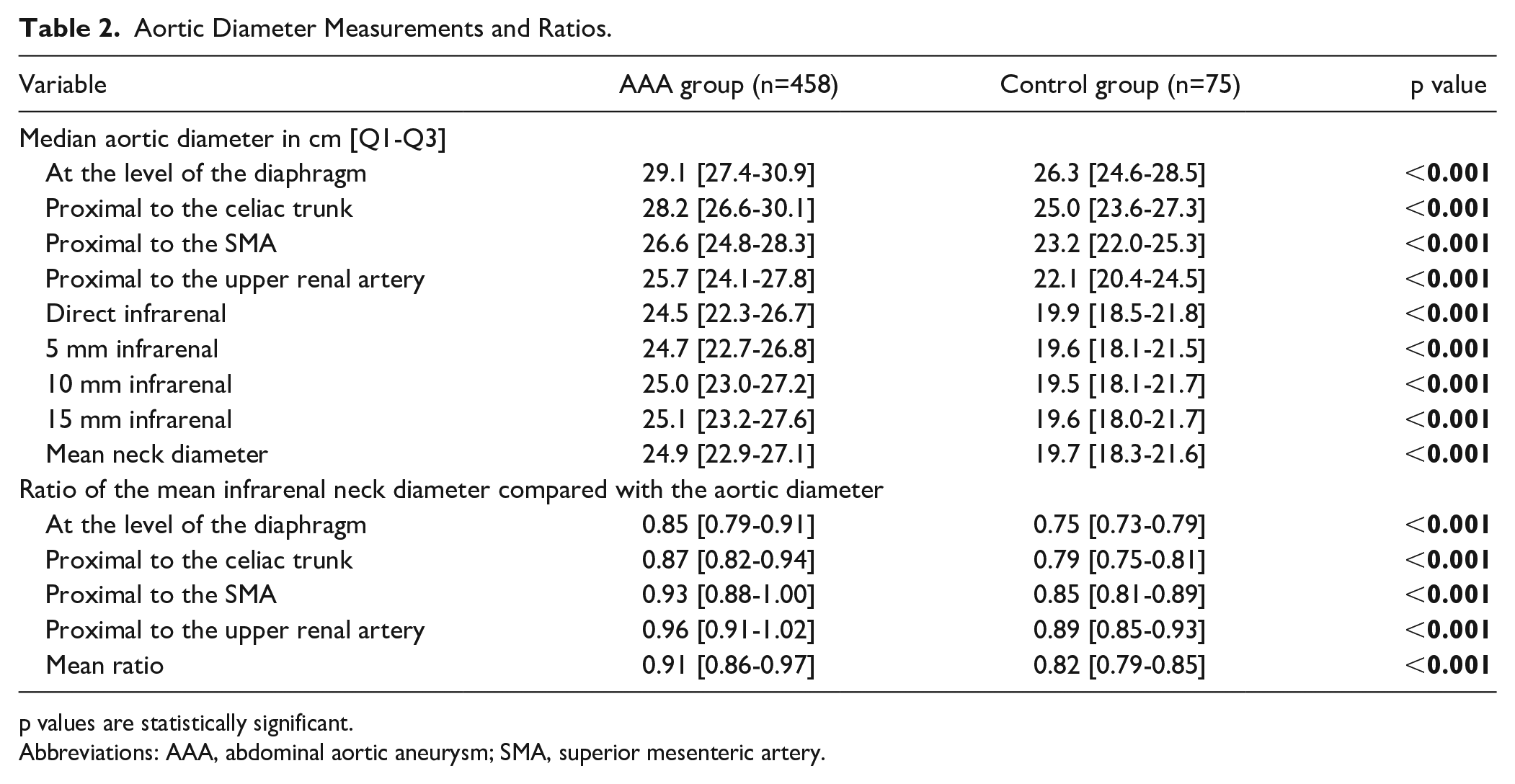
p values are statistically significant.
Abbreviations: AAA, abdominal aortic aneurysm; SMA, superior mesenteric artery.
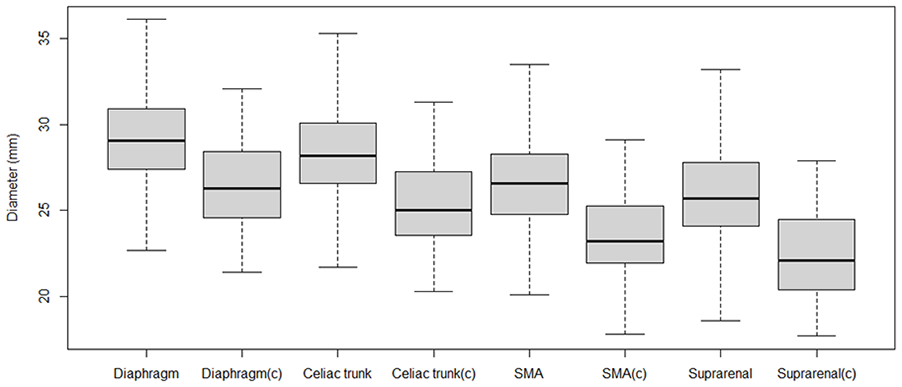
Box and whisker plots of diameters of all suprarenal measurements. SMA, superior mesenteric artery; (c), control group.
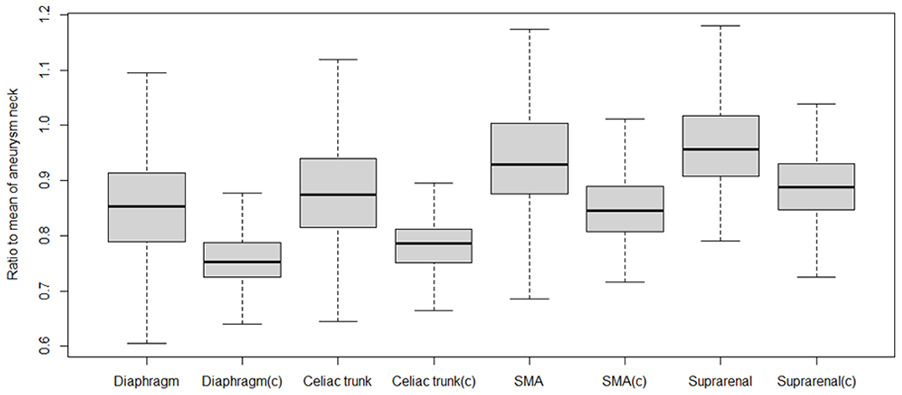
Box and whisker plots of all ratios. SMA, superior mesenteric artery; (c), control group.
In both the AAA group and control group, significant correlations were found between the mean infrarenal neck diameter and gender, length, weight, and BSA. No such correlation was observed for age. (Table 3) However, in both groups, all ratios between the mean infrarenal neck diameter and the 4 suprarenal aortic diameters were not correlated with age, sex, height, weight, or BSA, except for the ratio between the mean infrarenal neck diameter and the aortic diameter measurement proximal to the upper renal artery, which was correlated to weight and BSA in the control group (Table 3).
Correlations in Aneurysm and Control Group.
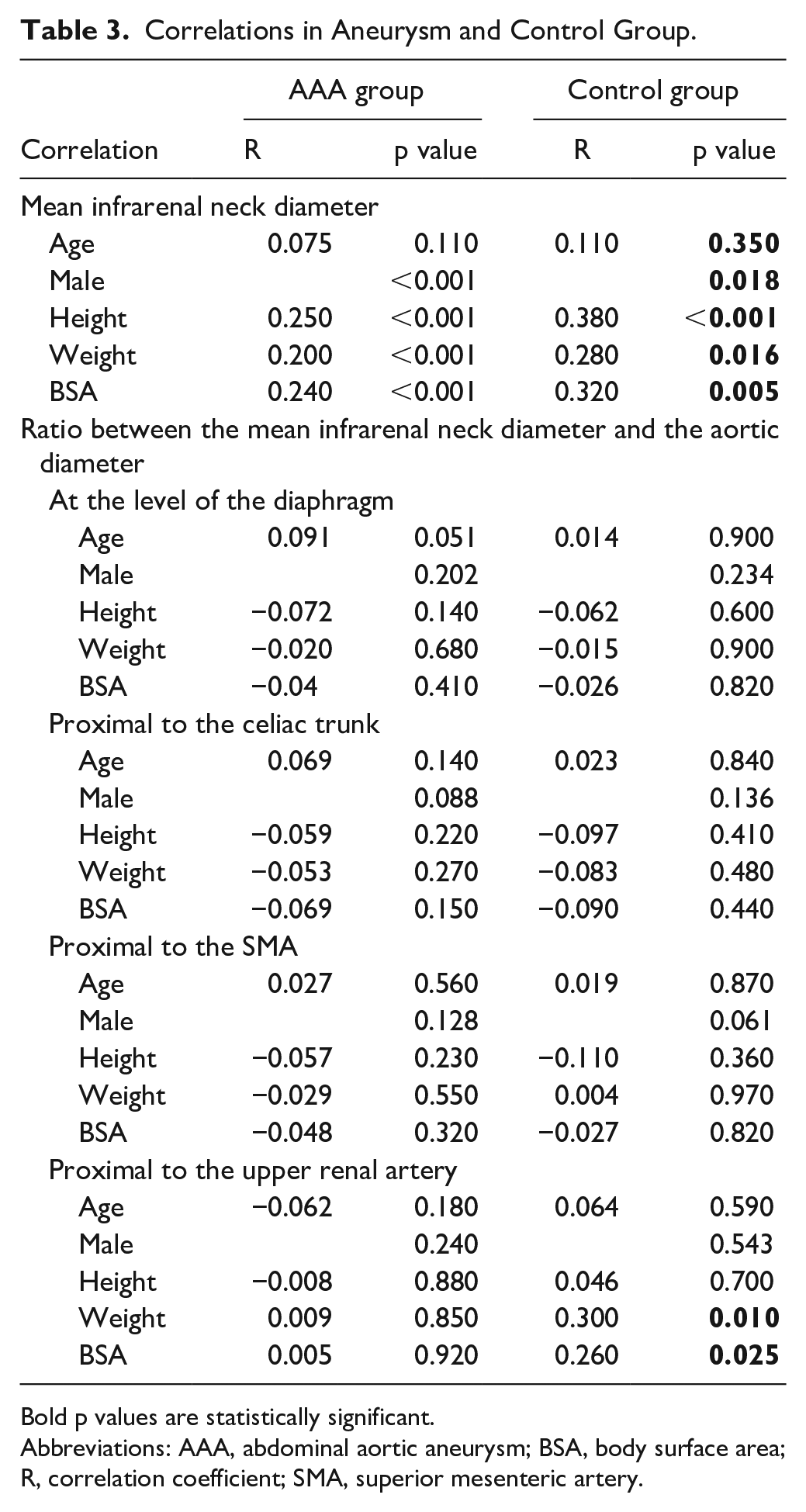
Bold p values are statistically significant.
Abbreviations: AAA, abdominal aortic aneurysm; BSA, body surface area; R, correlation coefficient; SMA, superior mesenteric artery.
Discussion
Patients treated for an infrarenal aneurysm had significantly increased suprarenal and infrarenal aortic diameters compared with nonaneurysmal patients. As expected, the aortic diameter was largest at the diaphragm and narrowed toward the renal arteries. In AAA patients, the mean suprarenal aortic diameter was only around 10% larger compared with the control group, while the mean infrarenal aortic diameter was around 25% larger. This finding was also illustrated by decreased ratios between the mean infrarenal neck diameter and the suprarenal aortic in the AAA group. This indicates that the aortic neck in most AAA patients was more dilated than the suprarenal aorta. The difference in the suprarenal aortic diameter between both groups cannot be clearly attributed to a single factor because abdominal aneurysm is a complex condition caused by a combination of genetic and environmental factors. 12 The variance in diabetes and renal insufficiency incidence between the AAA group and the control group may have had impact on this observed difference because aortic aneurysm formation and expansion is negatively associated with diabetes and is positively associated with renal insufficiency.13,14
Because there are no aortic side branches distal to the renal arteries up to the inferior mesenteric artery, the aortic diameter will likely remain stable in the segment. However, the infrarenal aortic diameters of patients in the AAA group increased toward the distal aorta, whereas the infrarenal aortic diameters were stable in the control group. In patients with an AAA, the infrarenal aortic diameter may increase toward the distal aorta because the aneurysm does not always have a clear starting point. Moreover, this may also be an indication that the infrarenal aortic neck is already diseased.
The infrarenal and suprarenal diameters in our series were similar to data from other reports.7,15–17 Rogers et al 15 showed that aortic diameters of nonaneurysmal patients were correlated with age, sex, and BSA. In the current series, we also found a significant correlation between sex, height, weight, and BSA in both the AAA and control groups. Age was not significantly correlated in the current series. Zhu et al 17 showed, in a prospective population-based cohort study with nonaneurysmal patients, that age was correlated with mean infrarenal neck diameter, but they only found that the upper percentiles of mean infrarenal neck diameter increased with age. People with larger baseline aortic diameters were more prone to dilation of the infrarenal aorta. Research by Solberg et al 18 underlines that an increased baseline diameter is more prone for dilatation. Because we have not distinguished between these groups, this, and a lack of power, could be the reason we did not find a significant correlation between age and diameters in our series.
When we calculated the ratios between the mean infrarenal neck diameter and the suprarenal diameters serving as an internal control, there was no correlation between any of these ratios and age, sex, height, weight, or BSA in both groups, except for the ratio between the mean infrarenal neck diameter and the aortic diameter measured proximal to the upper renal artery, which was correlated with weight and BSA. This might be a statistical error, but it also seems that some ratios may be more representative than other ratios. In our own experience, the diameter of the aorta proximal to the upper renal artery varies more than other suprarenal measurement points. The data summarized in Table 2 show that the interquartile range of the measurements proximal to the upper renal artery is larger than that at the other points. However, this topic needs further evaluation. In clinical practice, the mean infrarenal neck diameter should be related to the most representative suprarenal aortic diameter.
We were not able to relate aortic diameter with race/ethnicity in this study because these data were not available. However, there are series reporting aortic diameters in non-European healthy people, and they can be compared with our findings. Wang et al 19 measured the inner aortic diameter in 1340 Chinese patients and reported a mean diameter of 16.5 mm in male patients. Jasper et al 20 measured suprarenal diameters in a healthy Indian population at the location of vertebra Th12. They found a mean suprarenal aortic diameter of 19.0 mm. These diameters are smaller than the aortic diameters in the current series, but the inner-to-inner aortic diameter was measured in both series, as we have measured outer-to-outer. Moreover, West European people are generally taller than Asian people, which may contribute to this difference. 21 It would be interesting to see whether a ratio between the mean infrarenal neck diameter and the suprarenal aortic diameter corrects for these differences.
To the best of our knowledge, this is the first study investigating the ratios between the mean infrarenal neck diameter and the suprarenal diameters serving as an internal control. The clinical relevance of this novel concept using an internal control to correct for gender and body size has yet to be assessed and validated in EVAR and AAA patients. In future research, it should be assessed whether the ratio between the mean infrarenal aortic diameter and the suprarenal diameter may be a better predictor for a durable proximal seal in EVAR patients than the absolute infrarenal aortic diameter varying greatly between patients with different gender and body size. Moreover, we have yet to identify the cutoff point above which this ratio is a risk factor for development of a type IA endoleak. This ratio may also correct for comorbidities and a ratio between the AAA diameter and the suprarenal aortic diameter may help to better determine an AAA diameter cutoff for women. We encourage other investigators to validate our newly proposed ratio system in their own patient database.
In this study, it seems quite extensive to assess the ratio between the mean infrarenal aortic diameter and the suprarenal aortic diameter in a single patient. However, with the rapidly increasing field of artificial intelligence, these measurements may be automated in the future. The aneurysm diameter can already be accurately measured using artificial intelligence prior to surgery. 22 Although this technology still needs to be improved, adopting automated software in the future seems like an obvious step. This technology could enhance future clinical studies by analyzing the suprarenal and infrarenal aortic diameters both preoperatively and postoperatively in large cohorts.
This study is at risk for bias because it was conducted retrospectively. Although all aortic measures were conducted without knowledge of the patient’s characteristics, the control group was assembled by hand, which introduces bias. On the other hand, all patient characteristics were known and they were all treated in the same vascular center in a nonurgent setting.
Conclusion
Suprarenal and infrarenal aortic diameters are both significantly increased in AAA patients. The mean infrarenal neck diameter is correlated with sex, height, weight, and BSA. However, when the suprarenal aortic diameter was used as an internal control for the mean infrarenal neck diameter, we were able to correct for these variations in aortic diameters due to sex and body size. The clinical relevance of this ratio in AAA patients has yet to be assessed in future research.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.