
Abstract
Purpose:
Through a paradigmatic case and a systematic literature review, we present various endovascular strategies for treating pelvic paravesical arteriovenous vascular malformations (AVMs), with a focus on the efficacy of accessing the shunt point through direct puncture of the venous collector.
Case Report:
A 42-year-old male with nonspecific pelvic pain underwent a computed tomography (CT) scan, which revealed bilateral pelvic AVMs characterized by a network of arteriolar afferents originating from the internal iliac arteries and the inferior mesenteric artery, draining into 2 interconnected giant venous sacs in the bilateral paravesical space. The malformation was classified as type II according to the Cho classification. Following an unsuccessful attempt at transarterial embolization, we devised a plan for bilateral transvenous embolization in 2 separate sessions. Venous access was achieved through percutaneous transperineal ultrasound-guided puncture of the dominant outflow venous sac. A microcatheter was then placed directly into the shunt point, where sclerosant and embolic agents were specifically delivered. Follow-up imaging showed complete obliteration of both pelvic AVMs.
Conclusions:
Effective hemostasis of pelvic paravesical AVMs can be achieved by targeting the shunt point from the aneurysmal dominant outflow vein, potentially through direct percutaneous puncture.
Clinical Impact
This study aims to demonstrate the effectiveness of a transvenous approach in cases of embolization of pelvic paravesical arteriovenous vascular malformations (AVMs). The key to successful treatment lies in occluding the shunt point within the aneurysmal dominant outflow vein’s wall, which can be reached transvenously and potentially through direct percutaneous puncture. Although arterial occlusion can be performed additionally, it should not be performed alone due to its higher risk of AVM persistence/recurrence.
Keywords
Introduction
Pelvic arteriovenous malformations (AVMs) are rare,1,2 especially in men, and their presenting symptoms vary from subtle pelvic discomfort and constipation to dramatic scenarios, such as massive pelvic hemorrhage, which can be fatal. Pelvic AVMs present unique anatomical features characterized by dysplastic arteries from the internal iliac artery (IIA) forming shunt points with enlarged venous sacs draining into the internal iliac vein and should be classified as an independent entity within Cho type II category. Their embryological origin is uncertain but may involve incomplete involution or enlargement of primitive venous structures due to early arterial shunt development.3,4
Recognizing the correct anatomy of this type of AVM is crucial to understand the most appropriate endovascular treatment strategy and provide predictive information regarding clinical outcomes. Endovascular treatment often serves as the primary choice, if not the sole curative therapy, as surgical ligation poses a high risk of bleeding, damage to surrounding organs, incomplete obliteration, and potential cosmetic/functional impairments. 5
Case Report
A 42-year-old male suffered from chronic nonspecific pelvic pain that significantly impacted his quality of life. The patient had no notable medical history, underlying diseases, relevant family history, or previous pelvic or abdominal surgical interventions. Physical examination revealed nonspecific findings, with only slight discomfort upon deep palpation in the hypogastrium. Routine laboratory investigations yielded unremarkable results.
During a routine abdominal ultrasound examination, a large, heterogeneous formation with hypoechoic characteristics and arterial flow on Doppler ultrasonography (DUS) evaluation was identified. Subsequent computed tomography angiography (CTA) revealed a massive bilateral AVM within the paravesical spaces. This AVM was composed of multiple arteriolar afferents originating from both the bilateral IIA and the inferior mesenteric artery (IMA). These arterioles drained into 2 interconnected giant venous sacs located in the bilateral paravesical space, ultimately connecting to the left internal iliac vein (IIV).
In 2017, the patient underwent an initial attempt at transarterial embolization, which proved ineffective. A type I Amplatzer Vascular Plug (Abbott, Chicago, Illinois) was placed at the origin of the right pudendal artery during this procedure. Despite the embolization, the patient did not experience clinical improvement, and subsequent CT follow-up revealed no overall reduction in the AVM. On the contrary, an increase in the number of arteriolar afferents arising from the IMA was observed.
The patient was transferred to our center and upon reevaluation of diagnostic examinations (CTA scan, pelvic magnetic resonance imaging [MRI], and diagnostic angiography, illustrated in Figures 1 and 2) a decision was made to pursue transvenous treatment for both malformations in 2 separate sessions. Both treatment sessions were conducted under spinal anesthesia to ensure optimal stillness of the lower limbs and minimize peri-procedural and post-procedural pain. Mild sedation was administered to alleviate patient discomfort.
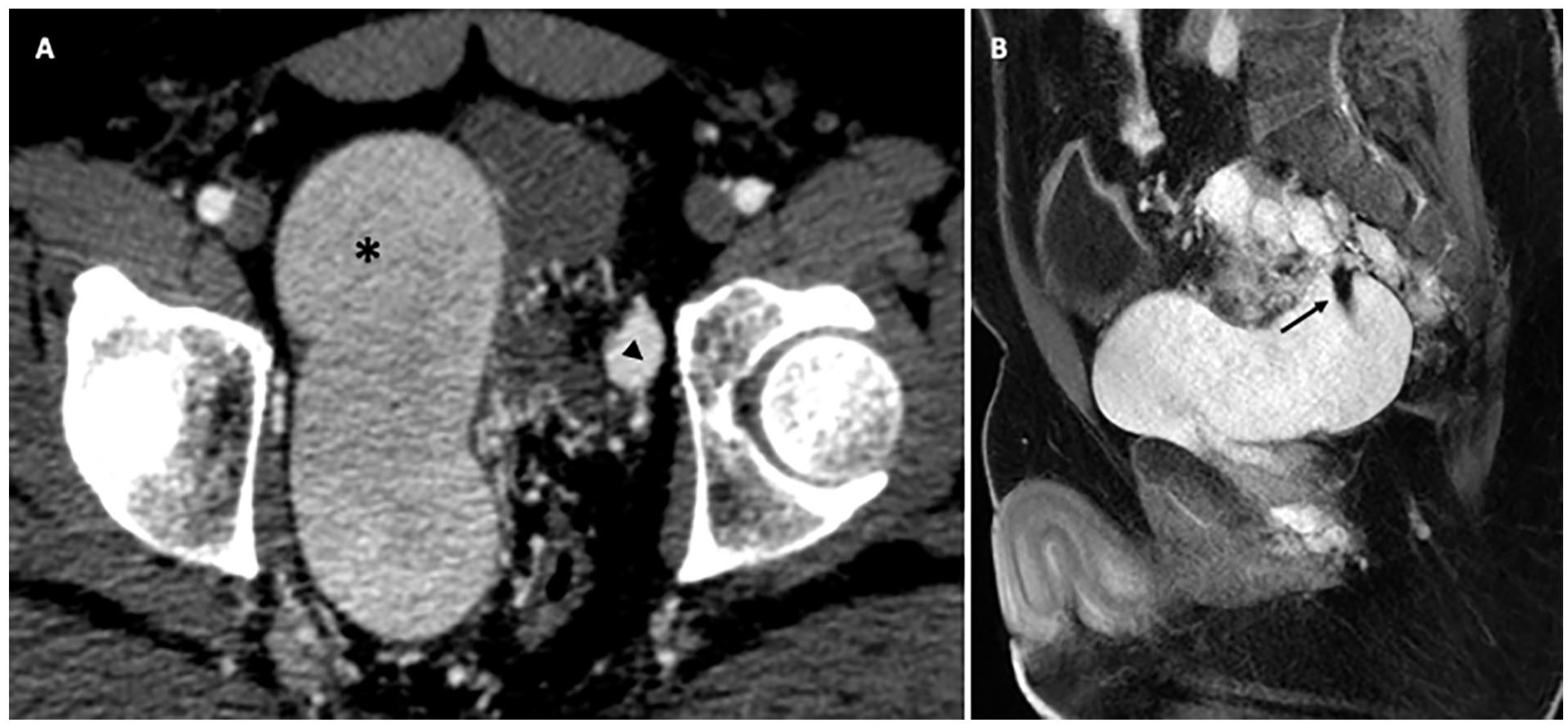
(A) Contrast-enhanced computed tomography in the arterial phase shows the left (star) and the right (arrowhead) giant venous collector; (B) magnetic resonance T1-weighted 3D fat-sat post-contrast in sagittal view reveals the main venous collector (the right one) with a signal void due to the arterial inflow through the shunt point (arrow).
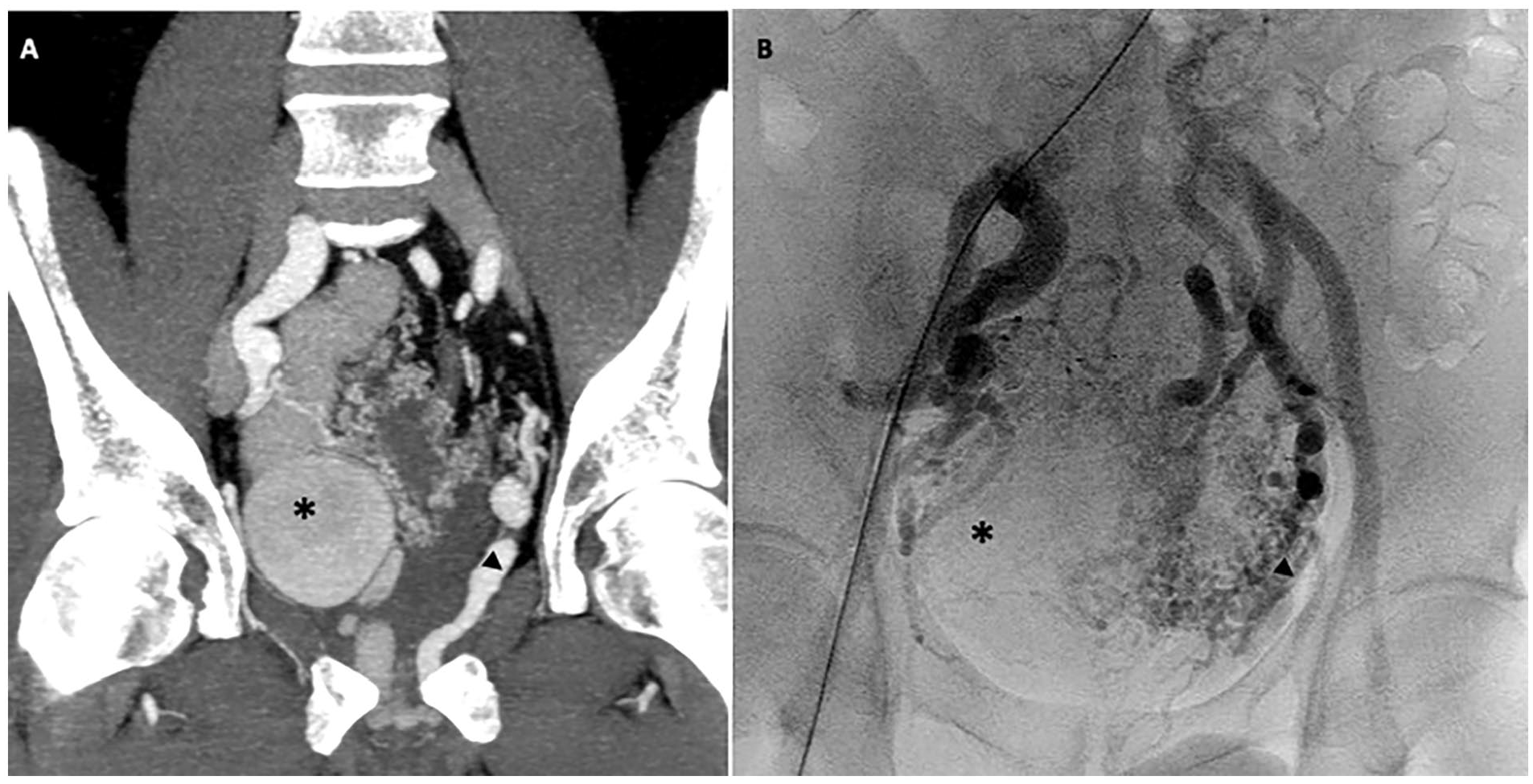
(A) Contrast-enhanced computed tomography in the arterial phase showing the 2 ectatic venous collectors with the corresponding angiographic imaging (B), where is best seen the pathological dense network of convolute arteriolar vessels arising from bilateral iliac arteries and inferior mesenteric artery, converging into the right (star) and the left (arrowhead) drainage outflow veins.
The left side was treated first, and the technique employed was similar in both sessions but mirrored. Two vascular accesses were established: 1 venous and 1 arterial.
The venous access was achieved through percutaneous transperineal ultrasound-guided puncture of the venous sac with the patient in a “fetal position.” A sterile field, from the lower back to mid-tight comprising the perineal zone, was prepared; the surgical bay was covered with a sterile drape. This access was used to advance a 4F sheath and a microcatheter (Progreat 2.7F, Terumo, Japan) for treatment. The arterial access (from the contralateral common femoral artery) was obtained with the patient in a supine position and used for homolateral iliac arterial axis angiography and subsequent selective homolateral IIA angiography. To perform this access, the patient was rolled from fetal to supine position, maintaining the sterile drape beneath him. Intravenous devices (sheath and microcatheter) were secured in a sterile wrap and placed between the patient’s legs during the adjustments. In the supine position, the inguinal area was sterilized again, and a surgical drape was placed, covering the patient from head to toe. Two windows were opened: one for the arterial puncture above the contralateral inguinal area, and the other, medially to the former, to allow the release and manipulation of intravenous devices.
The angiographic series confirmed the correct positioning of the microcatheter in the target venous collector and highlighted the shunt point, ie, the treatment target. The left-sided fistula was obliterated using a “sclero-embolization” technique, involving the release of both metallic coils (13 Concerto Medtronic microcoils, Minneapolis, Minnesota) followed by glue injection (1 mL Glubran 2, Viareggio, IT mixed with Lipiodol—1:2 ratio). On the right side, the sclerosant agent alone (11 mL of Glubran 2, Viareggio, IT mixed with Lipiodol—same ratio) was used. The microcatheter was directly placed in the shunt point, advanced with a microwire into the venous sac, and the sclerosant agent was injected, aiming to prevent the formation of a “casting” in the core of the venous collector to reduce thrombogenic response.
Immediate post-procedure arteriography and 24 hour post-procedure ultrasound examinations in both cases revealed the complete absence of flow signals in the treated AVM, confirming the favorable outcome of both sessions, as shown in Figure 3.
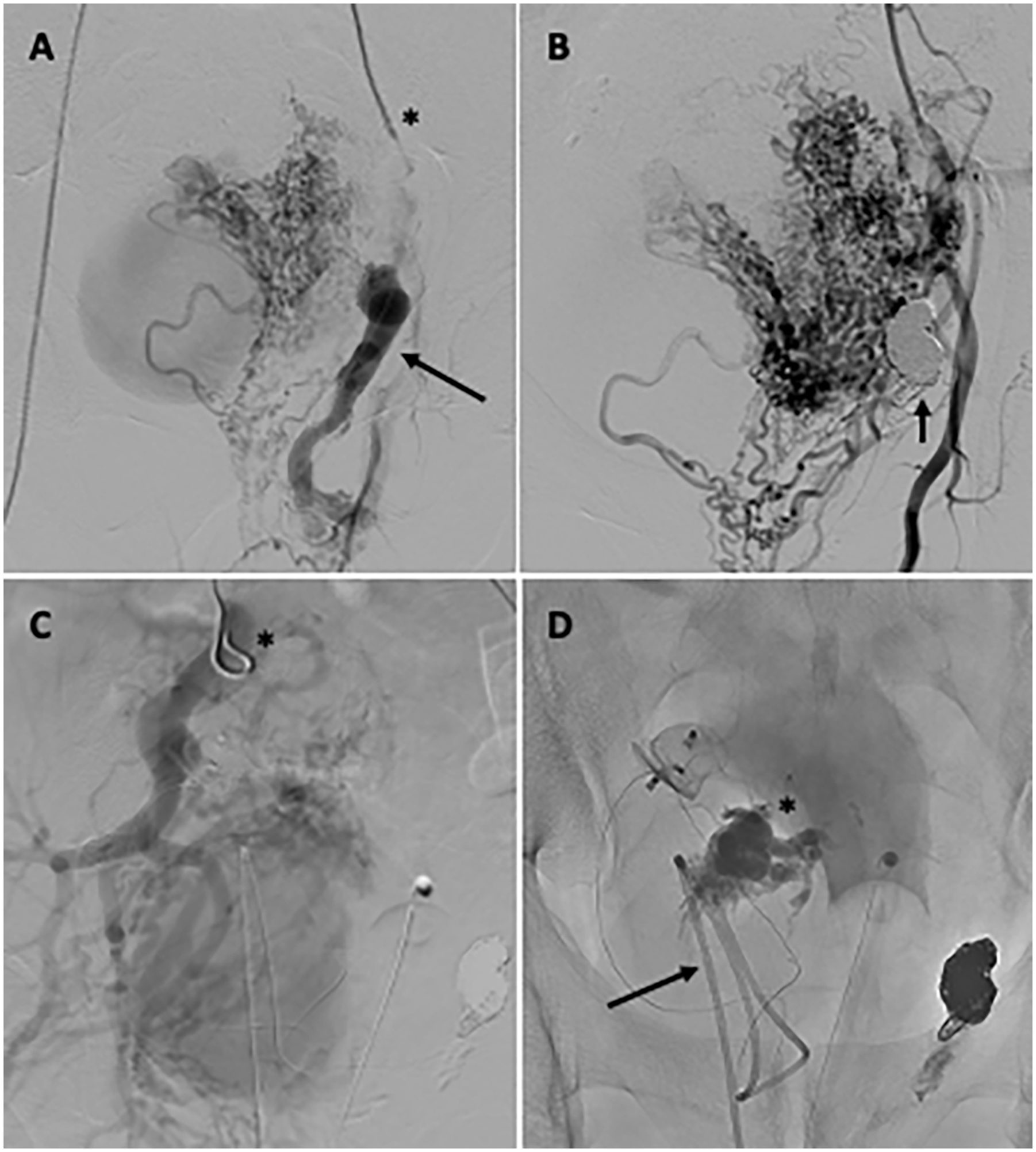
(A) Pre-procedural left IIA arteriography performed through a coaxial system made of 45 cm long 5F sheath + 5F diagnostic catheter (star), highlights the left venous collector in which is placed, through the percutaneous transperineal access, a 0.016 in microwire (arrow). Post-procedural left IIA arteriography (B) shows a cast of coils and glue (arrow) preventing the filling of the left venous collector, proving the success of the embolic therapy. Pre-procedural right IIA arteriography (C) made through 5F diagnostic catheter (star) shows contrast filling of the right venous sac, which was obliterated, as shown in the non-subtracted post-procedural fluorography (D), with Glubran 2 polymerized within the shunt point (star) using a coaxial system composed of a 5F percutaneous transperineal sheath, hydrophilic diagnostic catheter, and microcatheter (arrow).
Upon discharge, the day after each procedure, the patient experienced no side effects. Clinical general examination was not significant, he did not complain of any abdominal/pelvic symptoms. Short-term therapy consisting of heparin, low-dose steroid, and paracetamol, if needed, was prescribed. After the latter procedure, the patient was also advised to wear an abdominal elastic band to prevent excessive blood stasis/thrombosis in the larger right venous sac. In addition, 1 month after the final session, an enhanced CT scan was performed, confirming the absence of contrast media inside the 2 venous collectors, proving the successful shunt occlusion (Figure 4).
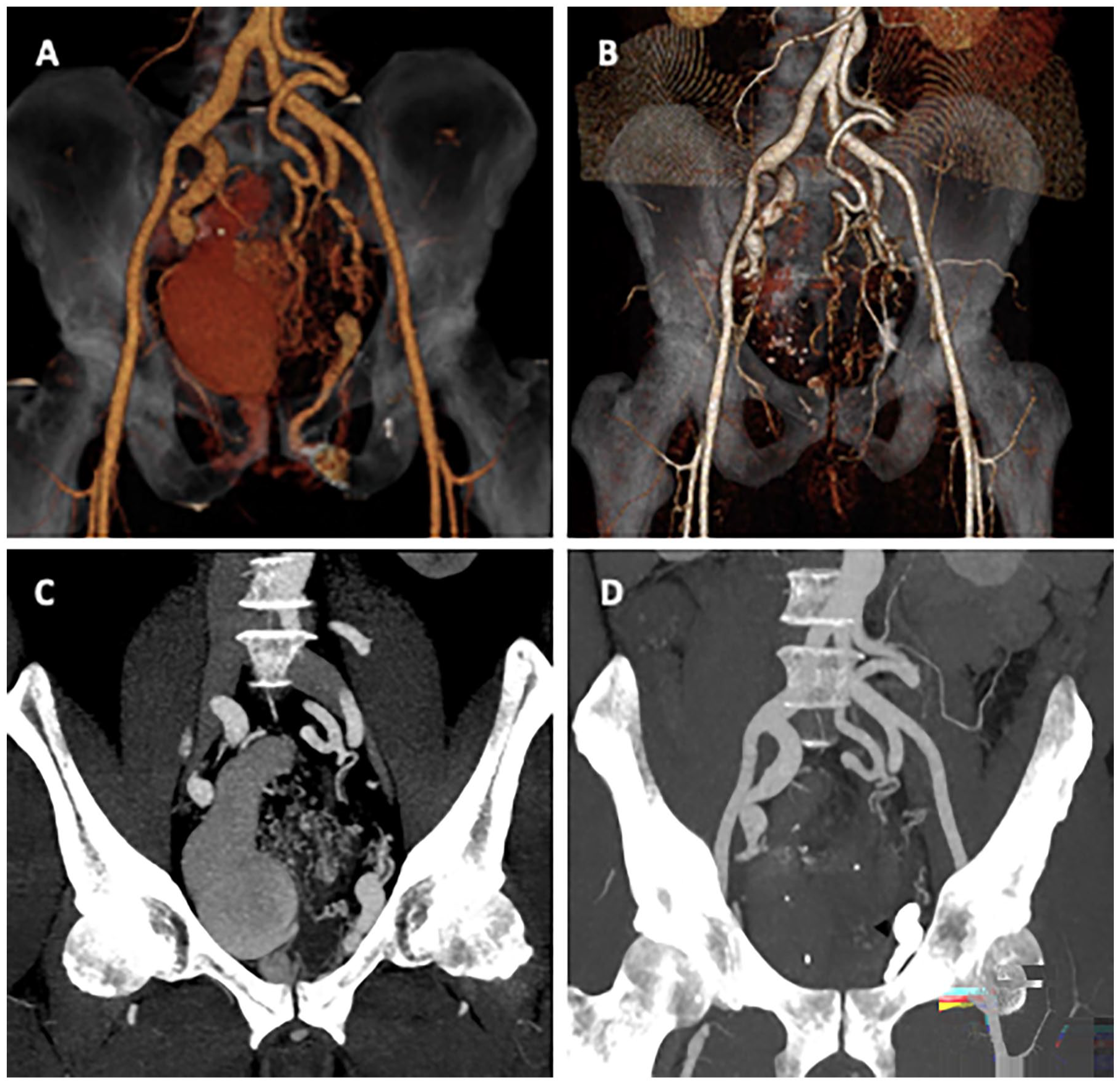
Pre-procedural (A; C) and post-procedural (B; D) computed tomography volume rendering and multiple intensity projection reconstruction show the success of the endovascular embolic treatment; a dense cast of coils is appreciable in the left side of the pelvis in last picture (arrow).
Literature Review
A systematic literature review was conducted according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 6 The medical literature of the last 23 years (from 2000 to November 2023) on the endovascular treatment of pelvic AVMs was reviewed, screening Excerpta Medica dataBASE (EMBASE), Medical Literature Analysis and Retrieval System Online (PubMed/MEDLINE), Cochrane Central Register of Controlled Trials (CENTRAL), ClinicalTrials.gov, and Google Scholar.
Searching strategy involved both MeSH terms and free-text strings. Studies were excluded if abstract only, not in English, animal cases, cadaver/autopsy series, or reporting other vascular pathologies or AVMs in other body locations (brain, spine, uterus, renal, rectum, etc) or other types of treatments (ie, surgical treatment or stereotactic radiotherapy). Retrieval and identification of records were performed by 2 authors (F.M. and M.V.) independently. A third author (A.D.) solved discrepancies. From 241 records screened, 22 met the inclusion criteria of at least 1 pelvic AVM, of non-iatrogenic nature, undergone endovascular treatment. Selected articles were then evaluated to collect data regarding patient’s sex and age, side of the AVM, arteries and veins involved in the inflow and outflow of the malformation, endovascular treatment technique (transarterial and/or transvenous and embolization agent used), and number of sessions. Since data reported in some articles covered both pelvic AVMs and AVMs in other locations, only those that specified data for pelvic cases were included. Studies included were summarized in Table 1.
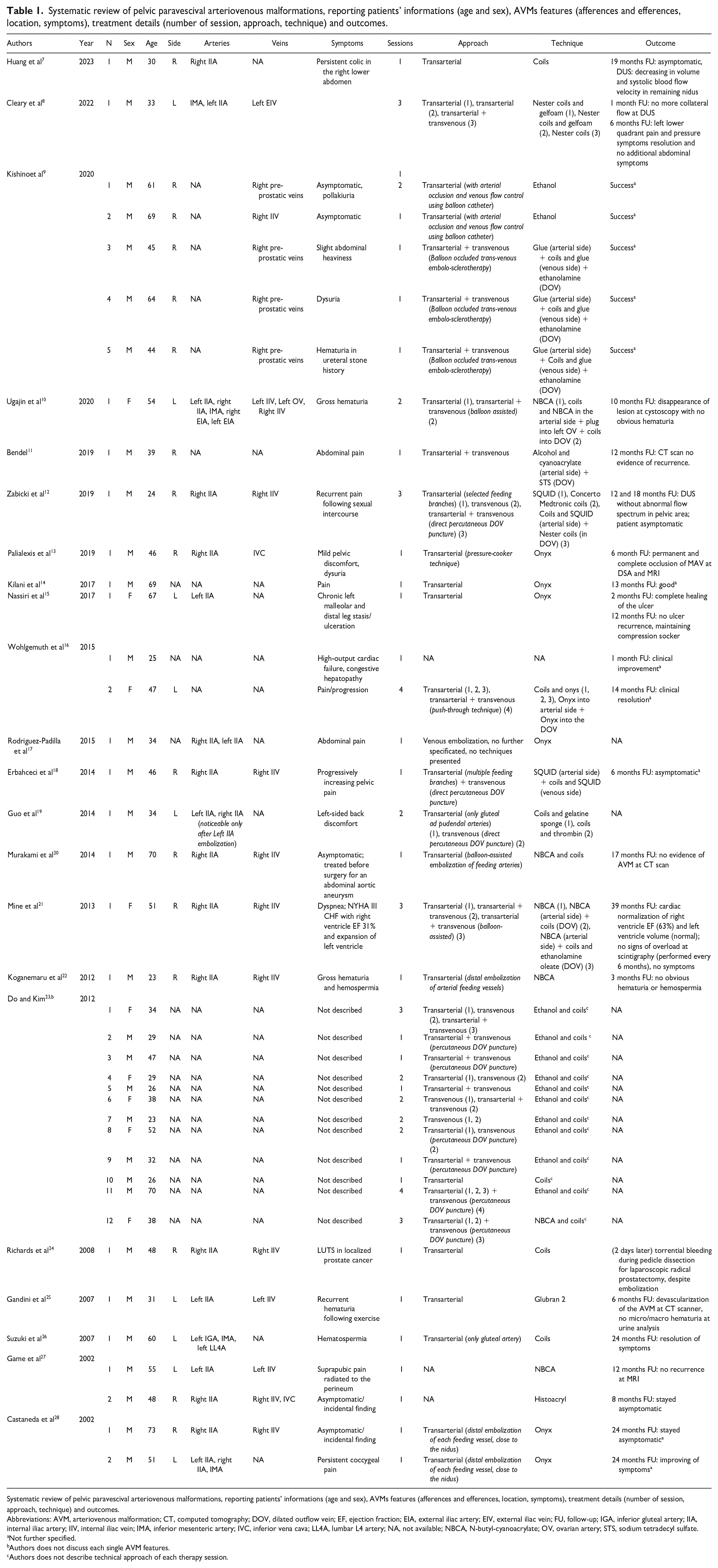
Systematic review of pelvic paravescival arteriovenous malformations, reporting patients’ informations (age and sex), AVMs features (afferences and efferences, location, symptoms), treatment details (number of session, approach, technique) and outcomes.
Systematic review of pelvic paravescival arteriovenous malformations, reporting patients’ informations (age and sex), AVMs features (afferences and efferences, location, symptoms), treatment details (number of session, approach, technique) and outcomes.
Abbreviations: AVM, arteriovenous malformation; CT, computed tomography; DOV, dilated outflow vein; EF, ejection fraction; EIA, external iliac artery; EIV, external iliac vein; FU, follow-up; IGA, inferior gluteal artery; IIA, internal iliac artery; IIV, internal iliac vein; IMA, inferior mesenteric artery; IVC, inferior vena cava; LL4A, lumbar L4 artery; NA, not available; NBCA, N-butyl-cyanoacrylate; OV, ovarian artery; STS, sodium tetradecyl sulfate.
Not further specified.
Authors does not discuss each single AVM features.
Authors does not describe technical approach of each therapy session.
Iconographic literature review of pelvic paravesical AVMs with dilated outflow vein which underwent endovascular therapy is shown in Figure 5.
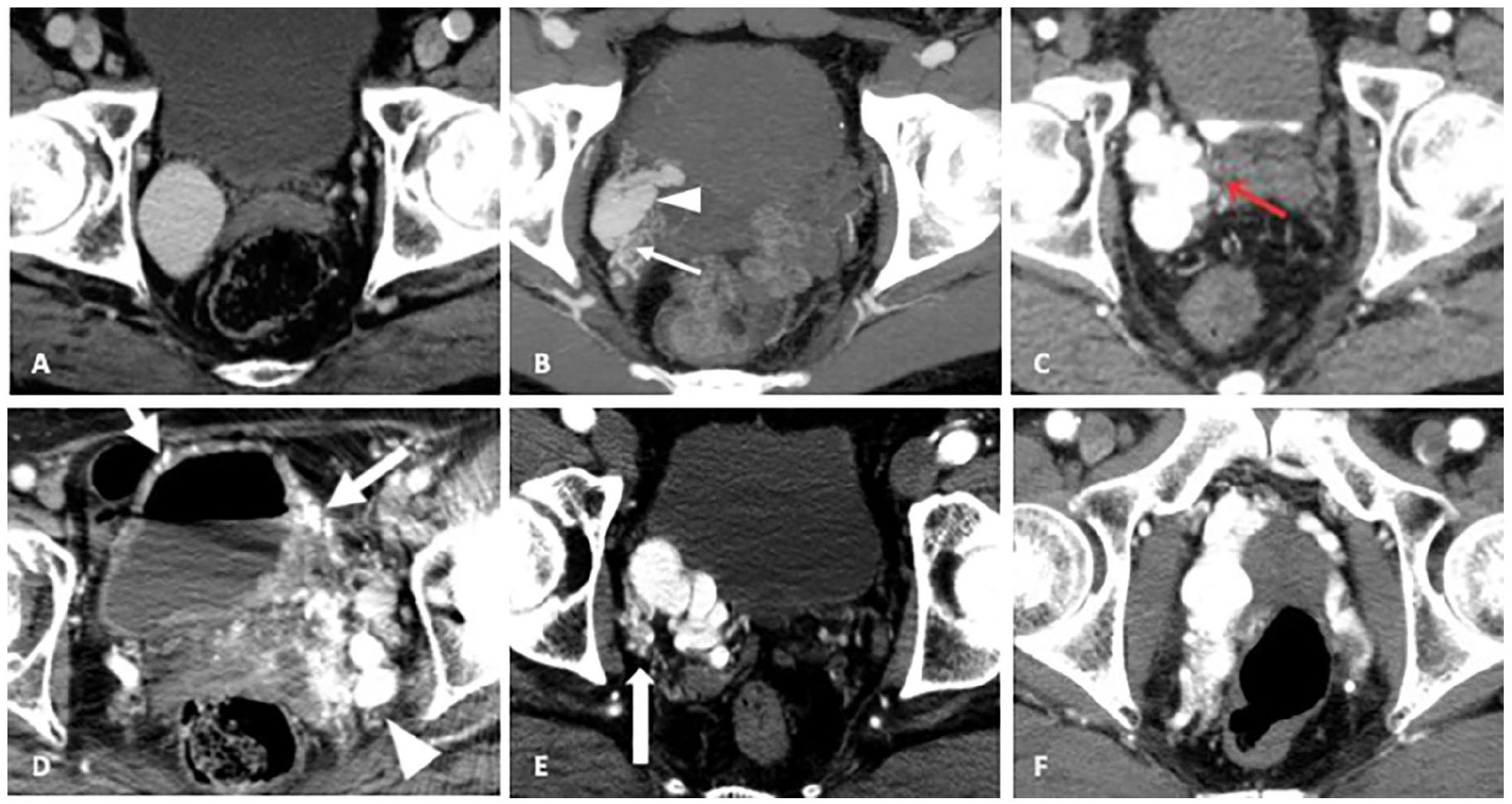
Contrast-enhanced computed tomography in the arterial phase showing, in the axial reconstruction, some of the reviewed cases of pelvic paravesical type II according to Cho et al. The AVM, focusing upon the dilated outflow vein (arrows and arrowheads). Kishino et al 9 (A), Koganemaru et al 22 (B), Gandini et al 25 (C), Ugajin et al 10 (D), Murakami et al 20 (E), Suzuki et al 26 (F).
To summarize, procedures can be subdivided into 2 groups: those performed through a transarterial approach (patients who underwent primarily a transarterial-alone embolization or “TA”) and those performed through a combined approach (patients who underwent primarily a combined transarterial + transvenous approach or “C”). Results are categorized into “incomplete outcome” (patients who required another intervention or evidence of AVM persistence at follow-up imaging) and “success” (complete resolution of symptoms, either with or without imaging evidence of AVM resolution).
A total of 41 patients were treated; 17 patients were excluded from the analysis due to the absence of follow-up data or endovascular technique information. In the “TA group” (19 patients), success was recorded for 11 patients (57.9%). However, 6 patients (31.6%) required at least 1 more treatment session: 4 underwent a combined or transvenous-alone approach and 2 underwent another transarterial-alone approach; both required a third session once again. Success was achieved in 100% of cases after adopting a combined or transvenous-alone approach. The remaining 2 patients (10.5%) achieved an incomplete outcome without further interventions.
In the “C group” (5 patients), success was achieved for all patients (100%) at the first combined approach session. No further interventions were needed.
Discussion
Pelvic AVMs are rare and treatment strategies are often complex. 8
Due to their recurrent morpho-structural features (numerous dysplastic arteries arising from IIA, communicating via shunt point with an enlarged venous sac, and draining finally into the internal iliac vein), pelvic AVMs must be considered as an independent entity falling within the “type II” category according to Cho et al’s 4 AVM classification (which is, type IIIa or IIIb sec. Yakes et al 3 ). It is challenging to assume their embryological development: they could originate from incomplete involution—or enlargement—of embryological/primitive venous structures, caused by early arterial shunt development, similar to what occurs in Vein of Galen Aneurysmal Malformation (VGAM), with which they share structural and morphological features. As speculated by Kishino et al, 9 paravesical AVMs could derive from the enlargement of anastomotic veins between the IIV and the pre-prostatic plexus, widening due to arteriovenous shunt generation and partial occlusion of the IIV drainage route. Alternatively, as discussed by Mallios et al, 29 they could represent persisting primitive vascular channels fed by multiple arteriolar shunts.
Although the embryogenesis remains uncertain, it is important to recognize their unique anatomical features to adopt the most suitable endovascular treatment strategy. It is known, in fact, that surgical ligation of proximal arteries in type II (Cho et al 4 ) AVMs is contraindicated, as this invariably leads to the recruitment of new feeding vessels and obliteration of the best arteries useful for endovascular treatment, resulting in AVM persistence or recurrence.16,29
As highlighted by our systematic literature review, there is no consensus on the embolization technique (transarterial and/or transvenous) nor on the type of embolizing agent to use.
Similar to surgical ligation of proximal arteries, endovascular treatment should not be limited to transcatheter arterial embolization, as it could lead to the same outcome: Huang et al 7 and Nassiri et al 15 both reported 2 cases in which occlusion of feeding arteries led only to a reduction in AVM flow—not to complete obliteration. For the same reason, this approach often requires multiple embolization sessions to achieve a satisfactory outcome: Cleary et al 8 needed 3 different sessions with different arterial targets to eliminate intra-venous sac flow—same as Game et al, 27 who instead needed 5 sessions.
This “plasticity” in arterial vessels recruitment was immediately evident at Murakami et al, 20 who described how, after embolizing the main left-sided AVM arterial afferences, new smaller feeding arteries from the right side—unenhanced at the preoperative angiographic study—became prominent at the post-procedure arteriographic series, reestablishing the venous sac perfusion. Guo et al 19 reported an analog case, which instead required 2 different embolization sessions.
Arterial embolization alone was ineffective also for Richards et al, 24 who experimented torrential bleeding during laparoscopic prostatectomy despite an apparently successful prophylactic transarterial embolization of a known pelvic AVM.
The key to a successful pelvic AVM treatment is the occlusion of the shunt point, which lies within the wall of the aneurysmal vein; this can be performed through an anterograde transvenous approach or through direct percutaneous puncture of the dominant outflow vein (DOV)—as different authors (Zabicki et al, 12 Do et al, 23 and Erbahceci et al 18 ) successfully performed.
Arterial occlusion can be in addition operated when DOV obliteration seems to be incomplete; Koganemaru et al 22 had to embolize the right superior vesical artery after the regular transvenous approach to stop the DOV—which was great in dimension—filling. Alternatively, as reported by Cleary et al 8 and Erbahceci et al, 18 selective arterial branch occlusion could be helpful in advance, to slow high arterial flow through the shunt point, favoring the positioning/polymerization of embolic or sclerosant agents.
In the systematic review we conducted, AVMs treated with a combined first-line approach (transarterial + transvenous) had a success rate of 100% (defined as complete resolution of symptoms, with or without imaging evidence of AVM resolution). No further interventions were needed. In patients undergoing primarily transarterial embolization, at least 1 additional treatment was necessary in 31.6% of cases; success was achieved in all cases by adopting a subsequent combined or exclusively transvenous approach. Similarly, in our study, transarterial embolization alone was not effective. From our review of the literature, it appears that the transvenous approach, whether alone or combined, allows for clinical success in almost all cases. These results supported our choice to use a transvenous approach.
There is still no consensus about the embolic agents to adopt for the DOV occlusion: they could be solid embolizers (coils, plugs, microparticles) or liquid ones (adhesives such as NBCA and Glubran or non-adhesives, such as Onyx, SQUID, Glefoam, etc); some authors injected in addition thrombine 19 to favor clotting. Embolotherapy could be associated with sclerotherapy (ethanol, STS, polidocanol, etc): the combined technique exploits the embolic-induced blood stasis to reach an optimal control of sclerosant spread during its injection, maximizes its local effect prolonging its dwell-time with endothelium, and reduces the risk of non-target polymer migration; for the same reasons, Mine et al, 21 Ugajin et al, 10 and Kishino et al 9 temporarily occluded the unique draining vein with a balloon catheter before transvenous sclerotherapy.
Similarly, Wohlgemuth et al 16 adopted the so-called “push-through” technique, also known as pressure-cooker,28,30 which consists of retrograde filling (using a microcatheter with a 5 cm long detachable tip) of the nidus after building a solid plug in the dominant venous outflow; he chose to use Amplatzer Vascular Plug.
Conclusions
The endovascular treatment of pelvic AVMs with a DOV remains challenging; the effective hemostasis for this type of vascular malformation can be achieved by targeting the shunt point from the venous draining sac, accessed through transvenous means or direct percutaneous puncture. In select cases, arterial hemostasis may prove beneficial as well. The choice of embolic agent should take into consideration its availability, the operator’s expertise, the shunt point conformation, and its anatomical localization. In alignment with the studies we reviewed, we underscore the necessity for further investigation to comprehensively understand the pathophysiology of AVMs and the long-term outcomes associated with various endovascular approaches.
Footnotes
Author’s Note
This material was not presented at any conference.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Consent for publication was obtained for every individual person’s data included in the study.