
Abstract
Background:
The objective of this systematic review was to provide evidence-based data regarding the safety and efficacy of the low-profile endografts (LPEGs) for abdominal aortic aneurysms.
Methods:
A systematic search of all the literature reported until April 2025 was performed according to the PRISMA (preferred reporting items for systematic reviews and meta-analyses) guidelines. The main outcomes were technical success, mortality, limb occlusions, reintervention, type I endoleak and adjunctive procedures.
Results:
A total of 2744 study titles were identified by the initial search strategy, of which 28 studies were considered eligible for inclusion in the present meta-analysis. A total of 1585 patients (88%, men) were identified among the eligible studies. The overall technical success rate was 97.1% (95% confidence interval [CI] 95.4-98.2%; I2=68%) (InCraft=94.5%; Zenith=97.7%; Ovation=98.7%; Minos=94.2%, Altura=98.8%) while the 30-day mortality rate was 0.9% (95% CI 0.6%-1.3%; I2=0%, p=0.95). The 30-day limb occlusion rate was 1.5% (95% CI 1.0-2.4%; I2=39%) (InCraft=1.9%; Zenith=1.5%; Ovation=1.2%; Minos=1.1%, Altura=1.2%) in the early period while during the follow-up, the limb occlusion rate was 4.1% (95% CI 2.9%-5.7%; I2=69%) (InCraft=5.1%; Zenith=6.0%; Ovation=2.3%; Minos=1.7%, Altura=1.8%). The 30-day reintervention rate was 2.7% (95% CI 1.8-4.0%; I2=57%) (Incraft=1.4%; Zenith=3.4%; Ovation=3.1%; Minos=1.7%; Altura=3.9%) while the pooled late reintervention rate was 7.6% (95% CI 5.3-10.8%; I2=89%) (InCraft=8.6%; Zenith=10.6%; Ovation=6.8%; Minos=3.4%, Altura=5.9%). The incidence of 30-day type Ia endoleak was 2.6% (95% CI 1.5-4.6%; I2=84%) (InCraft=5.9%; Zenith=1.2%; Ovation=2.0%; Minos=1.1%, Altura=1.2%) and 1.5% (95% CI 1.0-2.3%; I2=37%) (InCraft=1.0%; Zenith=1.4%; Ovation=1.6%; Minos=1.7%, Altura=1.2%) in the late period. The overall 30-day adjunctive procedures was 12.2% (95% CI 8.8-16.7%; I2=90%)(Incraft=13.6%; Zenith=24.7%; Ovation=3.3%; Minos=15.4%; Altura=3.0%).
Conclusions:
The present findings support the use of LPEGs in patients eligible for endovascular aortic aneurysm repair especially with hostile iliac anatomies. Limb-related complications remain the Achilles heel for certain devices, underscoring the need for strict postoperative surveillance. Further studies are warranted to investigate the underlying causes of these complications and to assess the long-term durability of these devices.
Clinical Impact
This study provides comprehensive data on the use of low-profile endografts (LPEGs) for the repair of abdominal aortic aneurysms (AAA). Despite significant advances in endograft technology, access-related challenges and limb complications remain among the most common adverse events associated with endovascular aneurysm repair (EVAR). The introduction of LPEGs was intended to broaden the applicability of EVAR to patients with complex anatomies, including narrow or tortuous access vessels and short or angulated aneurysm necks. The objective of this systematic review was to evaluate thirteen years of data on the safety and efficacy of LPEGs in AAA repair. Overall, the results support the use of LPEGs in appropriately selected patients, particularly those with hostile iliac anatomies. However, limb-related complications persist as the Achilles’ heel of certain devices, highlighting the importance of vigilant postoperative surveillance. Further research is needed to elucidate the mechanisms behind these complications and to assess the long-term durability of these devices.
Keywords
Introduction
Since the introduction of endovascular aneurysm repair (EVAR), abdominal stent graft technology has steadily evolved to enhance both patient eligibility and long-term durability. Despite these advances, access-related challenges and limb complications remain among the most frequent adverse events associated with EVAR.1,2 To address these challenges, manufacturers have introduced more flexible, lower-profile devices and delivery systems, enabling endovascular repair in patients with narrow access vessels and complex iliac anatomies. 3
Low-profile endografts (LPEGs), featuring enhanced sealing capabilities and delivery systems with an outer diameter of <18F, have further expanded the feasibility of endovascular treatment in patients with hostile anatomy, including narrow or tortuous access vessels, and short, angulated aneurysm necks. Currently available LPEGs include the Zenith LP (Cook Medical Inc, Bloomington, Indiana), the Incraft (Cordis Corporation, Bridgewater, New Jersey), the Ovation iX (Endologix, Irvine, California), Minos stent graft system (Shanghai MicroPort Endovascular MedTech Co, Shanghai, PRC) and the Altura endoprosthesis (Lombard Medical, Ltd, Oxford, UK).4–8 Although, encouraging mid-term results have been reported for these endografts; long-term outcome data remain limited.4–8 Furthermore, it is still unclear whether individual LPEGs provide distinct advantages or disadvantages, which may ultimately influence clinical outcomes.
The aim of the present meta-analysis was to evaluate the safety and efficacy of low-profile endografts in the treatment of abdominal aortic aneurysms (AAA).
Material and Methods
Protocol and Registration
The present meta-analysis was conducted according to the PRISMA (preferred reporting items for systematic reviews and meta-analyses) guidelines. 9 The search was applied to MEDLINE (database provider PubMed; from 1966 to April 2025), EMBASE (database provider Ovid; from 1980 to April 2025), and Google Scholar and Cochrane Central Register of Controlled Trials (April 2025). A snowball process of the reference lists from the eligible studies was following the retrieval of relevant reports from the database searches. The protocol of the present study was registered in the PROSPERO public database prior to the study initiation. For the present study, institutional Review Board approval was not required.
Search Method
We used the following search terms in all possible combinations: (low-profile) AND ([stent grafts] OR (endografts)) AND (abdominal aortic aneurysm)). All English-language scientific studies related to LPE for AAA reported up to April 2025 were potentially eligible. Two authors independently screened the titles and abstracts obtained from the search against the inclusion criteria. Disagreements were resolved through consensus or by discussion, with a third senior reviewer serving as the final arbitrator. Full reports for all studies that seemed to meet the inclusion criteria or where there was any uncertainty were obtained. The same 2 reviewers further analyzed the full-text articles against the study inclusion criteria, resolving any discrepancies by discussion and/or referral to the third reviewer before the data were finally analyzed. Additionally, the reference lists of reviews were searched to identify further studies for inclusion. After identifying the eligible studies, data were extracted independently by 2 authors using a predesigned datasheet and uploaded after confirmation of agreement on the data.
Inclusion and exclusion criteria
Studies were included in the review if they:
Provided data on LPEGs for AAA
Presented at least one of the main endpoints (technical success, 30-day mortality, aorta-related mortality, limb occlusion, reintervention and type I endoleak)
Studies providing follow-up data ≥12 months
Described ≥30 patients (the cutoff point of 30 patients was chosen as the threshold criterion with the reflection that experience from a center with >30 patients treated with these endografts merits consideration) 1
Studies were excluded if they:
Reported data based on old generation endografts
Reported mixed data with other endografts
Case reports; case series; editorial; review articles
Multicenter studies that included vascular centers reporting their experience separately were also excluded to avoid overlap and overestimation of the data.
We also excluded duplicate or metachronous republication from the same surgical groups; in these cases, only the latest article or the article with the largest number of patients was included.
Data Extraction Process
A data extraction form was designed to collect all the variables from the eligible studies. The following data were extracted: first author’s name, country (where the study was undertaken), study year, study design (prospective, retrospective), recruitment period, total number of patients, mean age, number of male patients and number of patients treated outside for instruction of use (IFU) device. The baseline data, cardiovascular risk factors (ie, chronic obstructive pulmonary disease, history of cerebrovascular disease, coronary disease, chronic renal failure), were also extracted. Moreover, data were collected regarding surgical urgency (ie, elective, emergent, urgent); type of LPEGs, procedure details (operation time, fluoroscopy time, contrast use); and type I endoleaks (early [<30 days], late [>30 days]).
Statistical Analyses
End points: definition, data synthesis and treatment effect
The numbers of patients with the outcomes of interest were extracted from each of the eligible studies and were reported as the proportion of patients with the corresponding outcome among all patients in every study.
The main outcomes analyzed were technical success; mortality (<30 days and during follow-up); limb occlusion; reinterventions (<30 days and during follow-up); type I endoleak and adjunctive procedures.
Technical success was defined as successful delivery and deployment of the LPEGs in the planned location without any unintentional coverage of the visceral or iliac vessels and absence of type I and III endoleak within the first 24 hours.4,5,7,10–22 A major adverse event was defined as any harmful and/or unintended postoperative outcome that led the patient to prolonged hospitalization or death. Such events were myocardial infarction, stroke, renal failure, gastrointestinal ischemia, and access bleeding.
Adjunctive procedures after endovascular aortic aneurysm repair (EVAR) are secondary intraoperative or postoperative endovascular or surgical interventions performed in addition to the primary EVAR, with the aim of optimizing technical success, sealing, fixation, or restoring/maintaining adequate perfusion of target vessels. These include maneuvers such as balloon angioplasty, placement of additional stent-graft cuffs or extensions, coil or plug embolization, limb thrombectomy, or open surgical conversion when necessary. 23
Study quality assessment, heterogeneity and publication bias
The assessment of methodologic quality of each study was assessed by 2 authors using the Newcastle-Ottawa scale (NOS). 24 The NOS was developed to assess the quality of the studies using the star system (maximum of 9 stars), in which a study was judged using 3 broad perspectives: (1) selection of the study groups; (2) comparability of the groups; and (3) ascertainment of the outcome of interest. We used a formal statistical test for heterogeneity (I2 test). Overall study risk of bias was deemed as high, some concerns, or low according to the NOS score and plots created using the risk-of-bias visualizations (ROBINS-I) tool (Supplemental Figure 1). 25 Studies were deemed to be at high risk of bias overall if any domain (selection criteria, comparability, or outcome) received a high risk of bias rating. In addition, the risk of bias was assessed by visual inspection of funnel plots and using the Egger regression test. The Comprehensive Meta-analysis statistical software, version V4 (Englewood, New Jersey), was used for analysis.
Results
Study Selection
A total of 2744 study titles were identified by the initial search strategy. The review of the titles and abstracts revealed that 2605 studies were irrelevant at the first screening stage. An additional 139 reports were evaluated further. Of the eligible studies 116 were excluded for one or more of the following reasons: studies providing mixed data with other endografts (n=2); studies that did not provide data on the main outcomes (n=10); studies reported on old generation endografts (n=17); studies with sample size of ≤30 patients (n=8); studies without or with ≤12 months follow-up (n=3); case reports or series (n=21); commentary or technical notes or review (n=21); irrelevant (n=18); studies with duplicate data and/or patients (n=10).
Finally, after applying these exclusions, 28 studies4–8,10–22,26–35 with a total of 4057 patients, were identified as potentially eligible for inclusion in the systematic review and meta-analysis after the addition of 5 studies15,20,33–35 resulting from the snowball process (Figure 1). Two studies8–32 from the same center were included in the present meta-analysis because they provided data from different patient recruitment periods. All the eligible studies included in the present meta-analysis are presented in Table 1.
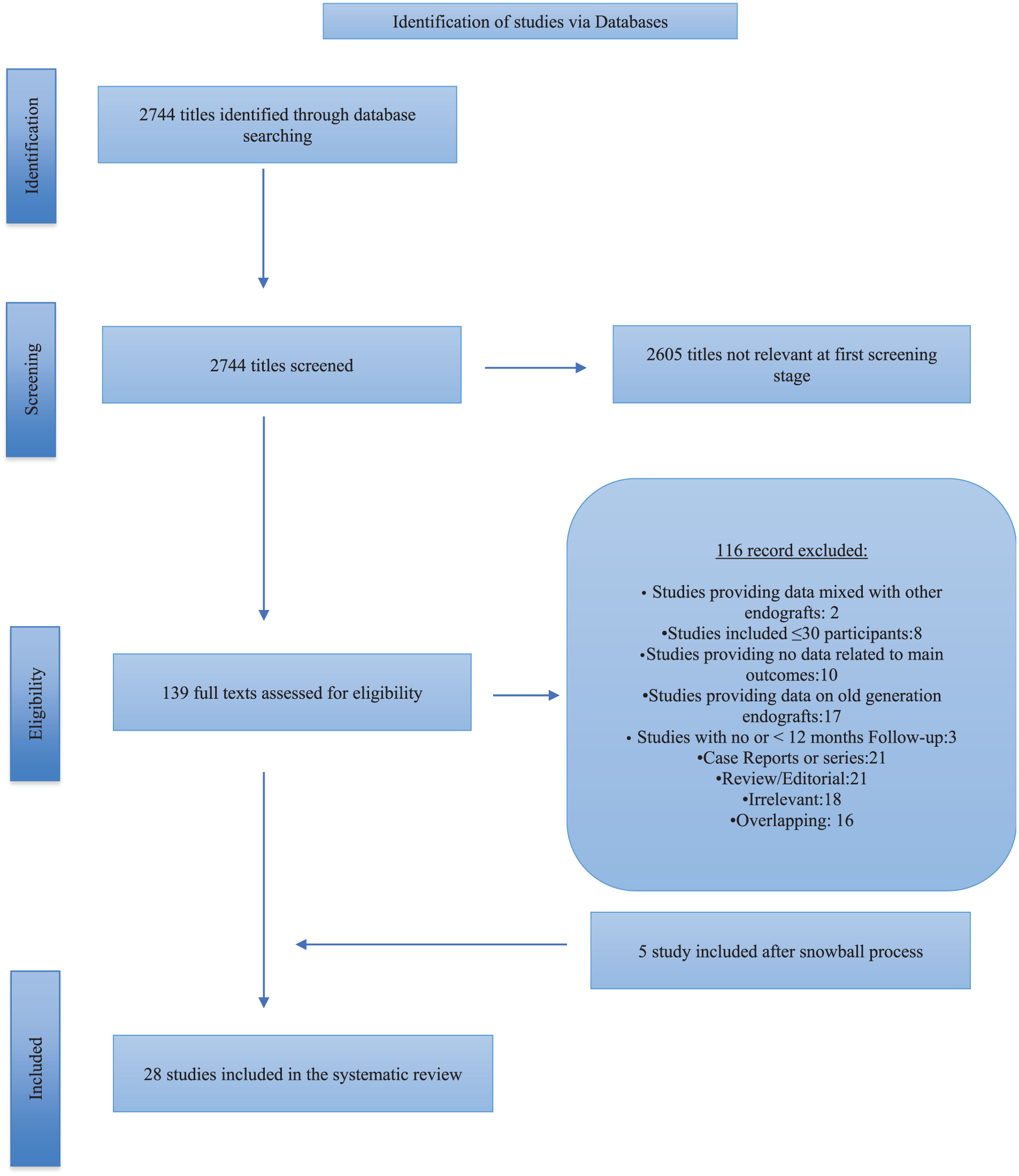
Study flow chart (“Preferred reporting items for systematic reviews and meta-analysis” diagram).
Baseline Study Characteristics of Included Studies.
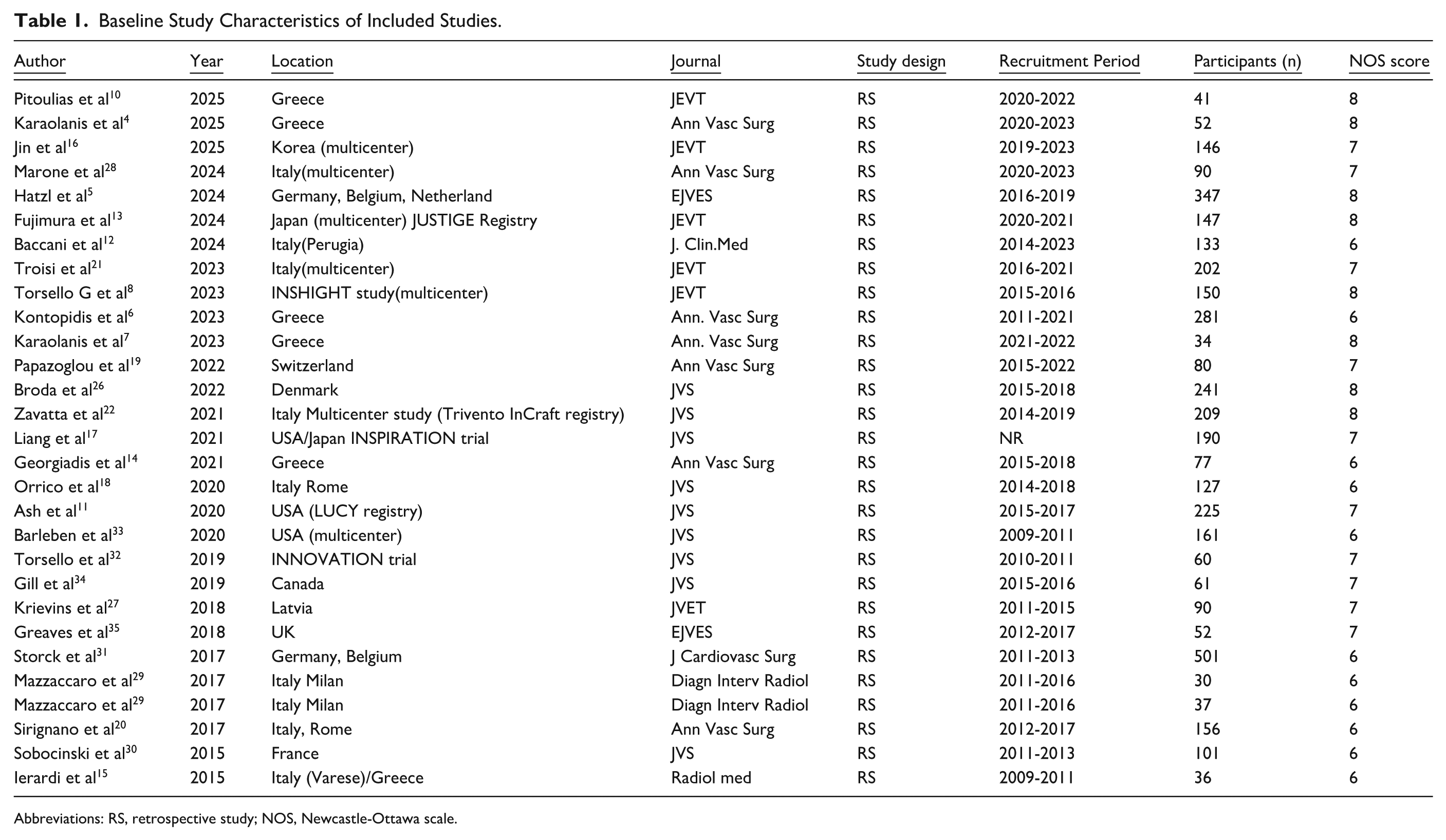
Abbreviations: RS, retrospective study; NOS, Newcastle-Ottawa scale.
Study Characteristics
All the eligible studies in the current meta-analysis are presented in Table 1. The included studies up to 2025 while the patients’ recruitment period was from 2009 to 2025. Of the 4057 (mean age 74 [70-78] years) patients included, 88% were men. Of them, 73% had hypertension; 47% dyslipidemia; 35% had coronary artery disease; 22% chronic obstructive pulmonary disease; 19% diabetes; 15% chronic kidney disease; 8% history of cerebrovascular diseases; 1% had prior aortic procedure whereas 49% were active smokers. Sixty-one percent of the patients were categorized as American Society of Anesthesiologists (ASA) classification ≥3.
Eleven studies8,12,14,16–19,22,29,32,34 (n=1270 patients) used the Incraft device, 8 studies6,11,15,20,29,31,33,34 (n=1442 patients) the Ovation platform, 5 studies5,13,22,26,30 (n=1038) the Zenith LP device, 3 studies4,10,28 (n=183 patients) reported outcomes on Minos stent-graft system and 2 studies7,27 (n=124 patients) on the Altura endoprosthesis.
Of the procedures, 97% had been elective, 2% had been emergent and 1% had been urgent. The mean operative time was 100 minutes (ranged from 85 to 119 minutes) (reported in 18 studies),4,5,8,11–14,18–22,26–31,34,35 the mean fluoroscopy time was 20 minutes (ranged from 17 to 23 minutes (reported in 13 studies),4,5,7,10,12,14,18,20,21,27,29,34,35 the contrast medium was 107 ml (ranged from 63 to 135 mL [reported in 10 studies]).4,5,7,12,21,34,35 The mean length of stay was 3 days (ranged from 1 to 4 days) reported in 13 studies,4,7,10,11,14,18,20,21,26,27,29,31,34 while the mean follow-up was 26 months (ranged from 12 to 31 months) reported in all included studies.4–8,10–22,26–35 Table 2 summarizes all the available studies between the different LPEGs.
Anatomical and Perioperative Characteristics of the LPEGs.
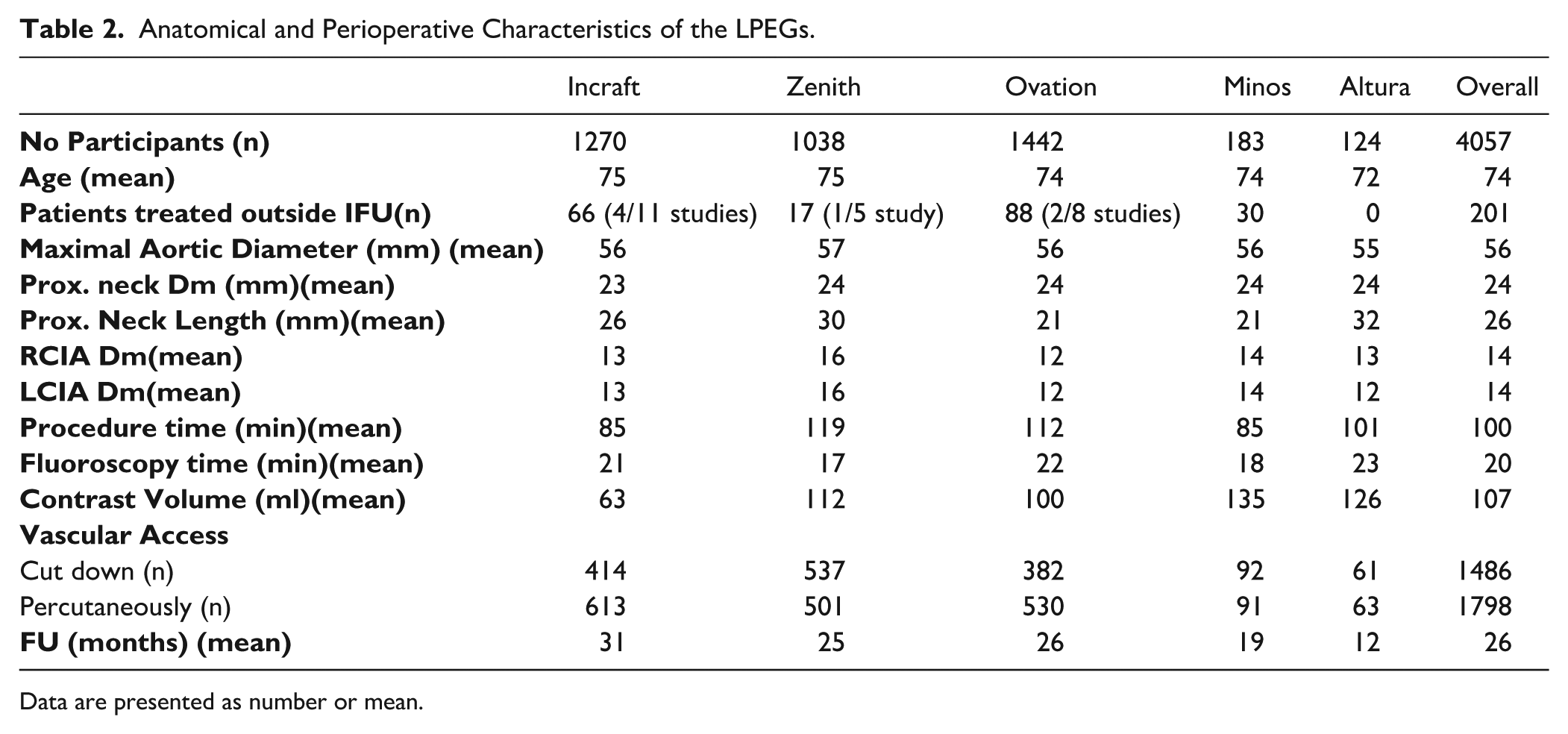
Data are presented as number or mean.
Meta-Analysis
Prevalence of Technical Success
Overall technical success was 97.1% (95% CI 95.4-98.2%; I2=68%, p=0.63;) reported in all the eligible studies (Figure 2).4–8,10–22,26–35 The publication bias was not significant (coefficient, 6.21; standard error [SE], 0.54; p=0.6).
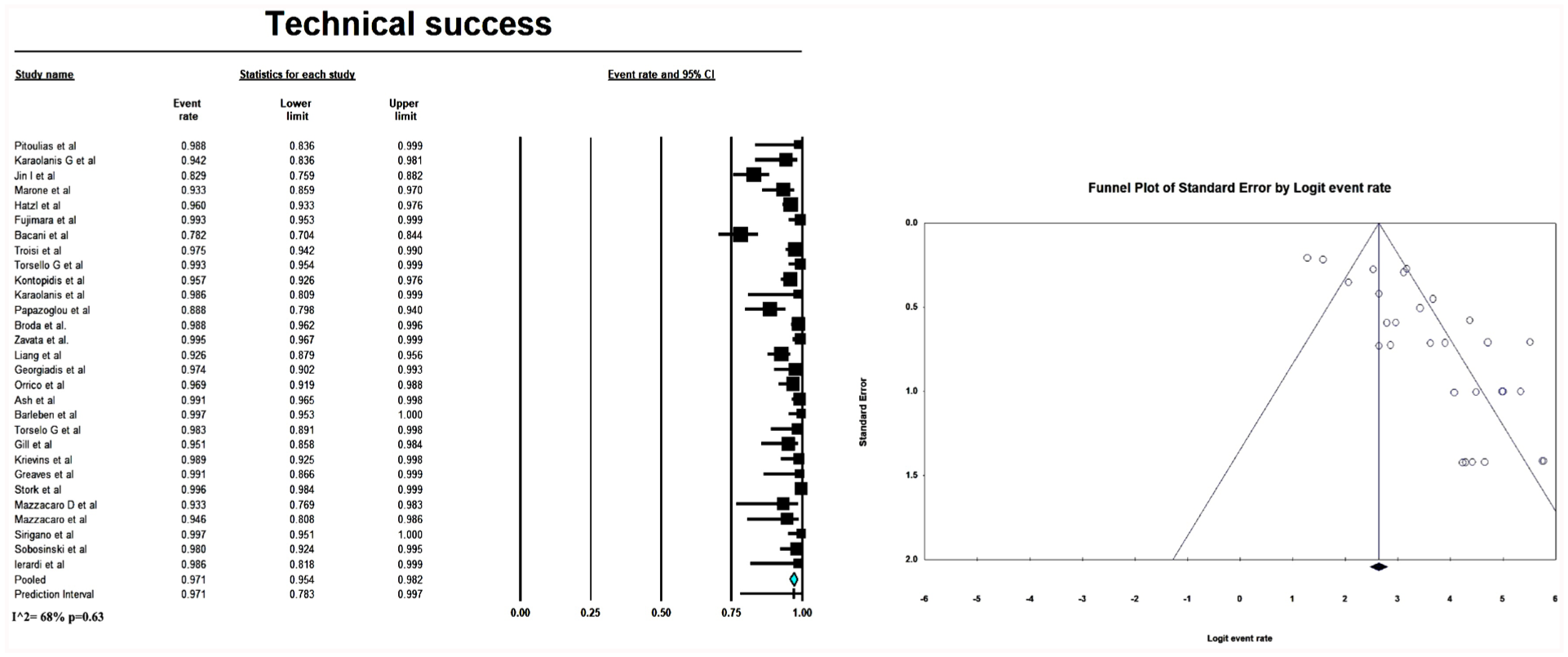
Forest plot presenting the meta-analysis of technical success rate. Event rates in the individual studies presented as squares, with 95% confidence interval (CIs) presented as extending lines. The pooled event rate with its 95% CI is depicted as a diamond. ES, Effect estimate.
The technical success for the Incraft device was 94.5% (95% CI 90.1-97%; I2=83%, p=0.01; 11 studies),8,12,14,16–19,22,29,32,34 for the Zenith was 97.7% (95% CI 95.9-98.7%; I2=36%, p=0.17; 5 studies),5,13,21,26,30 for the Ovation of 98.7% (95% CI 96.6-99.5%, I2=64%, p=0.007; 8 studies),6,11,15,20,29,31,33,35 for the Minos was 94.2% (95% CI 89.4%-96.9%; I2=0%, p=0.48; 3 studies)4,10,28 and for the Altura was 98.8% (95% CI 94.2%-99.8%; I2=0%, p=0.88; 2 studies).7,27
Prevalence of Mortality
The prevalence of 30-day mortality was 0.9% (95% CI 0.6%-1.3%; I2=0%, p=0.95) reported in 26 studies (Figure 3A).4–8,10–17,19–22,26–32,34,35 The publication bias was significant (coefficient, 2.50; standard error [SE], 0.40; p=0.01).
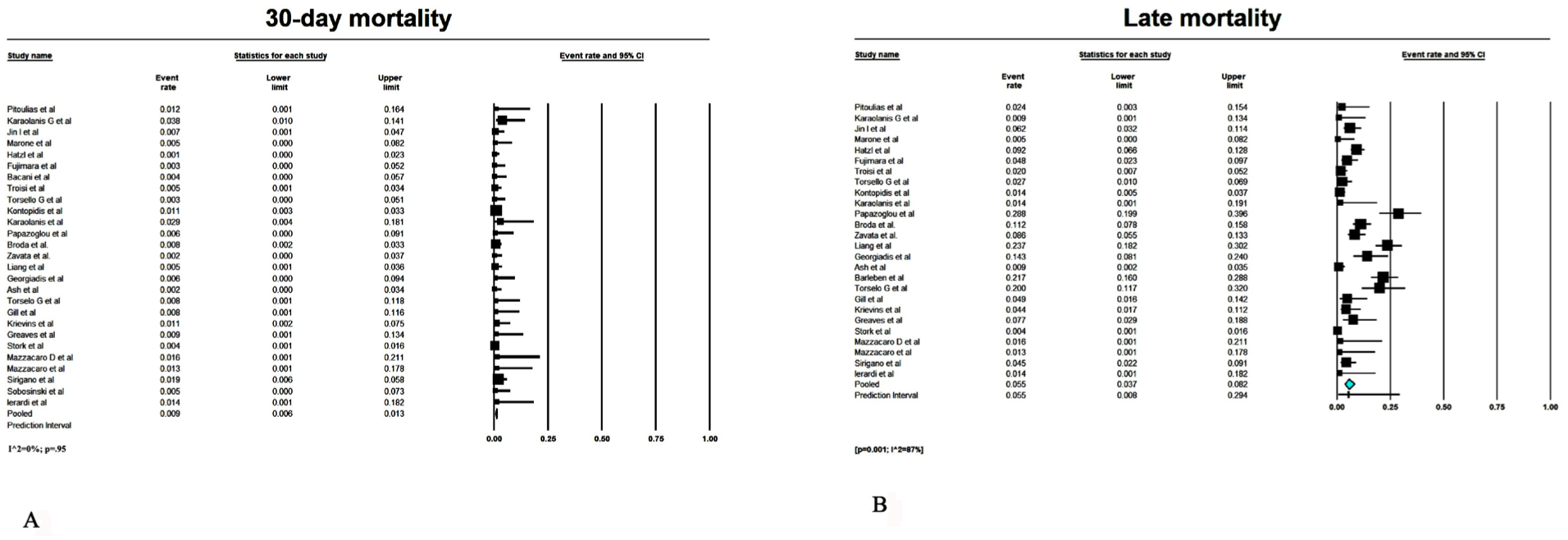
Forest plot presenting the meta-analysis of 30-day and late mortality rate. Event rates in the individual studies presented as squares, with 95% confidence interval (CIs) presented as extending lines. The pooled event rate with its 95% CI is depicted as a diamond. ES, Effect estimate.
The 30-day mortality rate for the Incraft device was 0.6% (95% CI 0.3%-1.3%; I2=0%, p=0.99; 10 studies)8,12,14,16,17,19,22,29,32,34 for the Zenith was 0.5% (95% CI 0.2-1.3%; I2=0%, p=0.85; 5 studies),5,13,22,26,30 for the Ovation of 1.0% (95% CI 0.5-1.8%, I2=0%, p=0.63; 7 studies),6,11,15,20,31,33,35 for the Minos was 2.3% (95% CI 0.7%-6.8%; I2=0%, p=0.40; 3 studies)4,10,28 and for the Altura was 1.8% (95% CI 0.5%-6.9%; I2=0%, p=0.49; 2 studies).7,27
The overall late mortality rate was 5.5% (95% CI 3.7%-8.2%; I2=87%, p=0.001) reported in 25 studies (Figure 3B).4–8,10,11,13–17,19–22,26–29,31–35 The publication bias was significant (coefficient, 5.0; standard error [SE], 0.71; p=0.003).
The incidence for late mortality was 10.9% (95% CI 6.3%-18%; I2=86%, p=0.17; 9 studies)8,14,16,17,19,22,29,32,34 for the Incraft device, 6.5% (95% CI 3.7%-11.3%; I2=78%, p=0.003; 4 studies)5,13,22,26 for the Zenith platform, 2.7% (95% CI 1.2%-8.6%; I2=91%, p=0.11; 8 studies)6,11,15,20,29,31,33,35 for the Ovation platform, 1.3% (95% CI 0.6%-5.1%; I2=0%, p=0.66; 3 studies)4,10,28 for the Minos endograft and for the Altura device was 3.9% (95% CI 1.6%-9.5%; I2=91%, p=0.44; 2 studies).7,27
Prevalence of Limb Occlusion
The overall incidence of 30-day limb occlusion was 1.5% (95% CI 1.0-2.4%; I2=39%, p=0.04) reported in 18 studies (Figure 4A).4,5,7,11–14,18–22,26–28,31,32,35 The publication bias was significant (coefficient, 3.47; standard error [SE], 0.50; p=0.003).
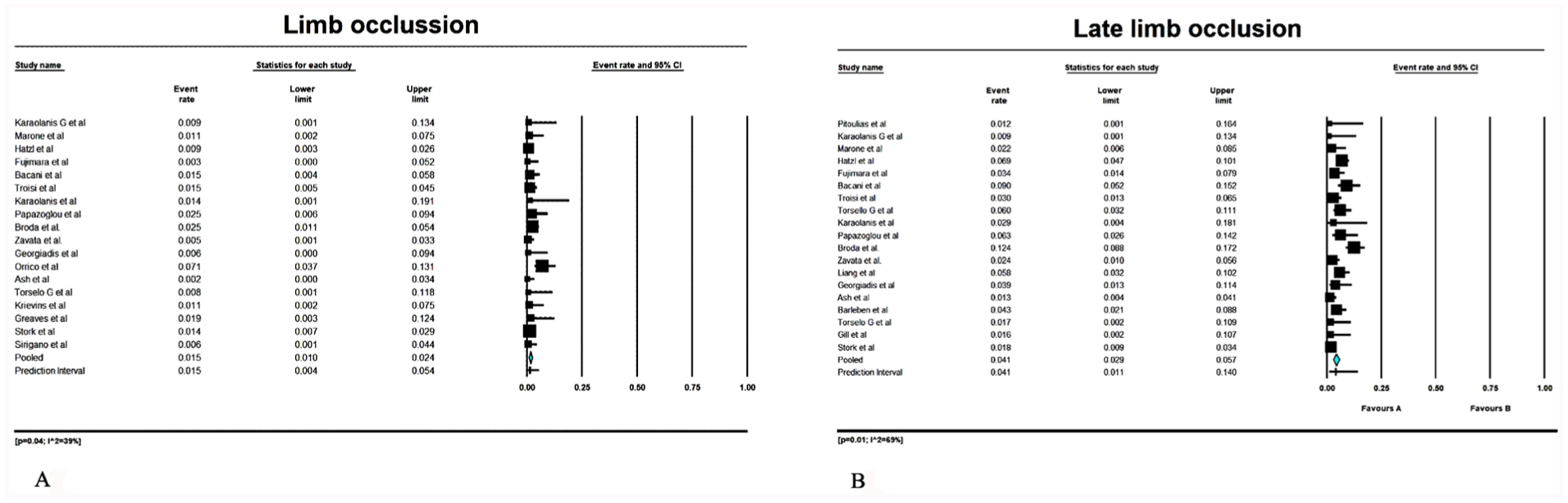
Forest plot presenting the meta-analysis of 30 day and late limb occlusion rate. Event rates in the individual studies presented as squares, with 95% confidence interval (CIs) presented as extending lines. The pooled event rate with its 95% CI is depicted as a diamond. ES, Effect estimate.
The Incraft device reported a rate of limb occlusion of 1.9% (95% CI 0.7-5.1%; I2=61%, p=0.02; 6 studies),12,14,18,19,22,32 the Zenith device of 1.5% (95% CI 0.8-2.8%; I2=16%, p=0.31; 4 studies)5,13,22,26 the Ovation platform of 1.2% (95% CI 0.6-2.3%; I2=0%, p=0.52; 4 studies)11,20,31,35 the Minos endograft a limb occlusion of 1.1% (95% CI 0.2-5.0%; I2=0%, p=0.92; 2 studies)4,28 and for the Altura endograft of 1.2% (95% CI 0.2-5.8%; I2=0%, p=0.88; 2 studies)7,27
The overall late prevalence of limb occlusion was 4.1% (95% CI 2.9-5.7%; I2=69%, p=0.01) reported in 19 studies (Figure 4B).4,5,7,8,10–14,17,19,21,22,26–29,31–34 The publication bias was significant (coefficient, 4.0; standard error [SE], 0.64; p=0.008).
The prevalence of late limb occlusion for the Incraft device was 5.1% (95% CI 0.6-5.2%; I2=32%, p=0.17; 8 studies),8,12,14,17,19,23,32,34 for the Zenith device was 6.0% (95% CI 0.6-5.2%; I2=82%, p=0.001; 4 studies),5,13,22,26 for the Ovation was 2.3% (95% CI 1.2-4.6%; I2=54%, p=0.011; 3 studies),11,31,33 for the Minos was 1.7% (95% CI 0.6-5.2%; I2=0%, p=0.82; 3 studies),4,10,28 and for the Altura endograft was 1.8% (95% CI 0.5-6.9%; I2=0%, p=0.048; 2 studies).7,27
Prevalence of Reintervention
The overall incidence of 30-day reintervention rate was 2.7% (95% CI 1.8-4.0%; I2=57%, p=0.01) reported in 21 studies (Figure 5A).4–7,10–16,18–22,26–28,32,35 The publication bias was significant (coefficient, 4.49; standard error [SE], 0.48; p=0.0025).
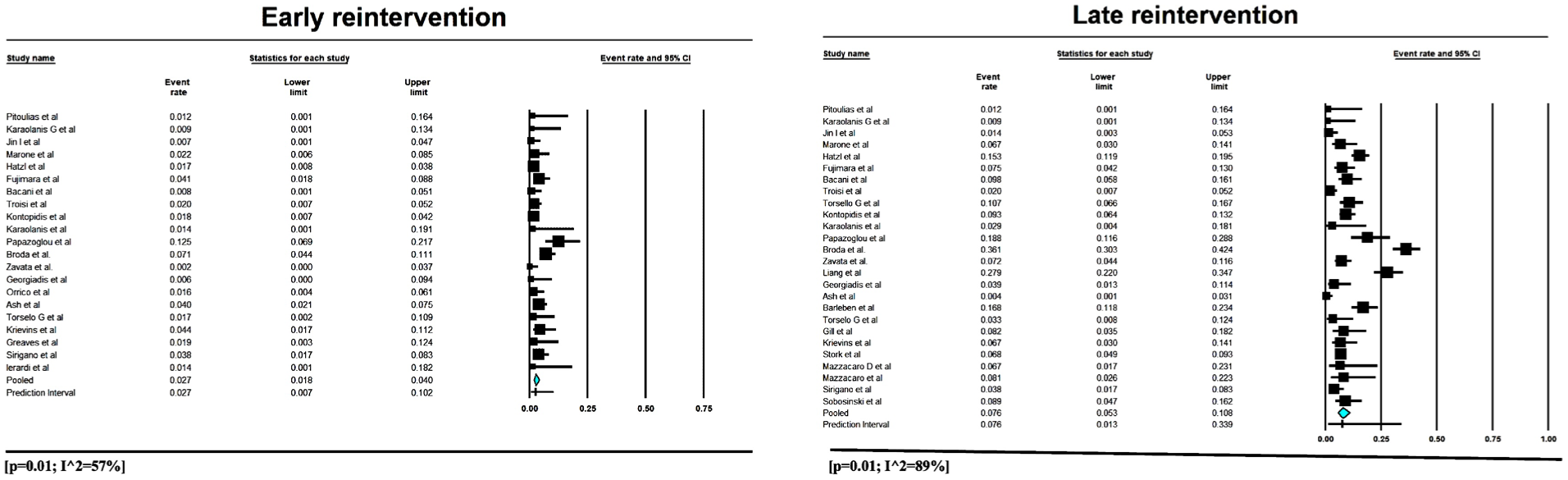
Forest plot presenting the meta-analysis of early and late reintervention rate. Event rates in the individual studies presented as squares, with 95% confidence interval (CIs) presented as extending lines. The pooled event rate with its 95% CI is depicted as a diamond. ES, Effect estimate.
The reintervention rate for the Incraft device was 1.4% (95% CI 0.4-5.3%; I2=78%, p=0.01; 7 studies),12,14,16,18,19,22,32 for the Zenith device was 3.4% (95% CI 1.6-6.9%; I2=75%, p=0.07; 4 studies)5,13,21,26 for the Ovation platform was 3.1% (95% CI 2.0-4.7%; I2=0%, p=0.54; 5 studies)6,11,15,21,35 for the Minos endograft was 1.7% (95% CI 0.6-5.2%; I2=0%, p=0.82; 3 studies)4,10,28 and for the Alura endograft was 3.9% (95% CI 1.6-5.9%; I2=0%, p=0.44; 2 studies)7,27
The overall late reintervention rate was 7.6% (95% CI 5.3-10.8%; I2=89%, p=0.01) reported in 25 studies (Figure 5B).4–8,10–14,16,17,19–22,26–34 The publication bias was not significant (coefficient, 4.7; standard error [SE], 0.64; p=0.0087).
The prevalence of late reintervention rate for the Incraft device was 8.6% (95% CI 5.0-14.4%; I2=86%, p=0.01; 10 studies),8,12,14,16,17,19,22,29,32,34 for the Zenith device was 10.6% (95% CI 4.5-23.2%; I2=95%, p=0.001; 5 studies),5,13,21,26,30 for the Ovation was 6.8% (95% CI 3.9-11.8%; I2=82%, p=0.001; 6 studies),6,11,20,29,31,33 for the Minos was 3.4% (95% CI 0.9-9.2%; I2=34%, p=0.22; 3 studies),4,10,28 and for the Altura endograft was 5.9% (95% CI 2.8-11.9%; I2=0%, p=0.043; 2 studies).7,27
Prevalence of Type Ia Endoleak
The incidence of early type Ia endoleak was 2.6% (95% CI 1.5-4.6%; I2=84%, p=0.01) reported in 24 studies (Supplemental Figure 2A).4–8,10–16,18–22,26,30–32,34,35 The publication bias was significant (coefficient, 5.9; standard error [SE], 0.62; p=0.001).
The prevalence of endoleak type Ia after use of Incraft device was 5.9% (95% CI 3.1-11%; I2=84%, p=0.08; 9 studies),8,12,14,16,18,19,22,32,34 for the Zenith was 1.2% (95% CI 0.6-2.3%; I2=0%, p=0.44; 5 studies)5,13,22,26,30 for the Ovation was 2.0% (95% CI 1.0-4.3%; I2=58%, p=0.02; 7 studies),6,11,15,20,29,31,35 for the Minos was 1.1% (95% CI 0.7-7.1%; I2=0%, p=0.90; 3 studies)4,10,28 and for the Altura was 1.2% (95% CI 0.2-5.8%; I2=0%, p=0.88; 2 studies)7,27
The incidence of overall late type Ia endoleak was 1.5% (95% CI 1.0-2.3%; I2=37%, p=0.036) reported in 23 studies (Supplemental Figure 2B).4–8,10,11,13–17,19,20,22,26–29,31–34 The publication bias was significant (coefficient, 4.3; standard error [SE], 0.40; p=0.003).
The prevalence of late endoleak type Ia after use of Incraft device was 1.0% (95% CI 0.4-2.7%; I2=44%, p=0.08; 8 studies),8,14,16,17,19,22,32,34 for the Zenith was 1.4% (95% CI 0.3-6.8%; I2=79%, p=0.007; 3 studies)5,13,26 for the Ovation was 1.6% (95% CI 0.9-3.0%; I2=34%, p=0.16; 7 studies),6,11,15,20,29,31,33 for the Minos was 1.7% (95% CI 0.6-5.2%; I2=0%, p=0.82; 3 studies)4,10,28 and for the Altura was 1.2% (95% CI 0.2-5.8%; I2=0%, p=0.88; 2 studies).7,27
Prevalence of Type Ib Endoleak
The incidence of early type Ib endoleak was 1.1% (95% CI 0.8-1.6%; I2=0%, p=0.72) reported in 24 studies (Supplemental Figure 3A).4–8,10–16,18–22,26,27,29–32,35 The publication bias was significant (coefficient, 2.6; standard error [SE], 0.49; p=0.015).
The prevalence of endoleak type Ib after use of Incraft device was 1.4% (95% CI 0.8-2.4%; I2=0%, p=0.96; 9 studies),8,12,14,16,18,19,22,29,32 for the Zenith was 0.8% (95% CI 0.4-1.7%; I2=0%, p=0.48; 5 studies)5,13,22,26,30 for the Ovation was 0.8% (95% CI 0.2-2.5%; I2=50%, p=0.05; 7 studies),6,11,15,20,29,31,35 for the Minos was 1.1% (95% CI 0.1-7.1%; I2=0%, p=0.90; 2 studies)4,10 and for the Altura was 1.2% (95% CI 0.2-5.8%; I2=0%, p=0.88; 2 studies)7,27
The incidence of overall late type Ib endoleak was 1.6% (95% CI 1.0-2.4%; I2=33%, p=0.72) reported in 21 studies (Supplemental Figure 3B).4–8,10,13–17,19,20,22,26,28,29,30–34 The publication bias was significant (coefficient, 4.9; standard error [SE], 0.34; p=0.015).
The prevalence of late endoleak type Ib after use of Incraft device was 1.2% (95% CI 0.6-2.4%; I2=0%, p=0.65; 9 studies),8,12,14,16,18,19,22,29,32 for the Zenith was 2.1% (95% CI 0.9-5.0%; I2=59%, p=0.058; 4 studies),5,13,26,30 for the Ovation was 1.1% (95% CI 0.3-3.7%; I2=68%, p=0.014; 5 studies),6,15,20,31,33 and for the Minos was 1.3% (95% CI 0.1-4.2%; I2=0%, p=0.99; 3 studies).4,10,28
Prevalence of Adjunctive procedures
The overall adjunctive procedures was 12.2% (95% CI 8.8-16.7%; I2=90%, p=0.57) reported in 24 studies (Supplemental Figure 4).4,5,7,8,10–14,16,18–22,26–32,34,35 The publication bias was significant (coefficient, 5.27; standard error [SE], 0.85; p=0.02).
The prevalence of adjunctive procedures for Incraft device was 13.6% (95% CI 8.3-21.5%; I2=89%, p=0.001; 10 studies),8,12,14,16,18,19,22,29,32,34 for the Zenith platform was 24.7% (95% CI 17.3-34%; I2=89%, p=0.83; 5 studies),5,13,21,26,30 for the Ovation was 3.3% (95% CI 1.2-8.8%; I2=81%, p=0.05; 5 studies),11,20,29,31,35 for the Minos endograft was 15.4% (95% CI 3.6-47.1%; I2=98%, p=0.01; 3 studies),4,10,28 and for the Altura endograft was 3.0% (95% CI 1.0-8.1%; I2=0%, p=0.57; 2 studies).7,27
Discussion
In this systematic review we pooled the available data on low-profile endografts for endovascular repair of abdominal aortic aneurysms (AAA). Overall, LPEGs demonstrated acceptable outcomes in terms of technical success, and mortality; however, a relatively high rate of adjunctive procedures was observed, primarily related to limb occlusion and type I endoleak.
The overall technical success rate across all 5 LPEGs was remarkably high (97.1%). This finding is consistent with expectations, reflecting both the growing experience with endovascular aortic aneurysm repair since its introduction in 1993 and the technological advances achieved by low-profile endografts. 1 By reducing the diameter of delivery systems, these devices, enable improved navigation through tortuous or heavily calcified arteries, thereby minimizing the need for surgical access and reducing intraoperative complications.4–8 Such innovations have enhanced deployment precision and control, contributing to consistently high technical success rates reported in the literature.4–8
The predominance of elective procedures (97% of cases) among the included studies likely contributed to the favorable outcomes. Elective settings allow for comprehensive preoperative planning and optimal patient selection, both of which are critical for procedural success. In addition, the availability of appropriate logistics and experienced staff also plays a pivotal role, as limitations in these factors may compromise procedural quality and result to suboptimal outcomes. 5
A key finding of this meta-analysis and a notable limitation of certain low-profile endografts (LPEGs) is the relatively high rate of limb graft occlusion (LGO) and reintervention. The pooled incidence of LGO was 4.1% during the follow-up, with the Zenith and Incraft devices demonstrating higher rates of 6.0% and 5.1%, respectively. Recently, the Enzen trial, which compared the Zenith and Endurant II device, reported an overall rate of LGO of 5.8%, Zenith (9%), Endurant (3.4%), p=0.002. 36 Similarly, European cohort studies outcomes of the Zenith Alpha AAA reported unexpectedly high mid-term LGO rates ranging from 10.7% to 15.0% in European cohorts.26,37 The underlying etiology remains uncertain. In response to early reports, the manufacturer issued a field safety notice highlighting 4 potential contributors: (1) deployment of a flared limb into a small ipsilateral gate, (2) gate misalignment, (3) excessive overlap of iliac limbs above the bifurcation, and (4) narrow aortic bifurcation anatomy. Nevertheless, subsequent analyses by Hatzl et al 5 and Bogdanovic et al 37 did not confirm a consistent association between these factors and occluded limbs. Additional contributors, such as gate diameter, graft fabric properties, delivery system compression, and stent design may also influence outcomes and should be considered in the design of future device generations. 38
Although the InCraft platform has not been extensively discussed with respect to limb graft occlusion (LGO), this complication has been reported in 2 multicenter studies.8,17 The INSIGHT study, documented an LGO incidence of 3.4%, while the INSPIRATION study reported at 5.7%.8,17 Similarly, Baccani et al 12 reported 13 reinterventions, 9 of which were attributed to endograft component occlusion. The mechanisms driving these adverse events remain uncertain, though one possible explanation is the thromboembolic materials dislocated from the suprarenal component of the fractured stent. Supporting this concern, the INSPIRATION study, 17 identified stent fractures in 20 patients over a 5-year follow-up period, underscoring the need for further investigation. Zavatta et al 22 reported a limb occlusion rate of 2.4% and, through subgroup analysis, identified that the concomitant presence of 2 or more hostile iliac features (iliac tortuosity index >1.5, iliac artery calcification >50%, Aortic bifurcation ≤16 mm and external iliac artery ≤6 mm) adversely affected iliac limb patency, and increased the reintervention rates.
These findings have important clinical implications. The higher incidence of limb occlusion observed with certain low-profile endografts highlights the need for meticulous postoperative surveillance, as limb-related complications remain one of the leading causes of secondary interventions after EVAR. 1 In the present analysis the overall late reintervention rate was 7.6%. with the highest rates, observed in the InCraft (8.6%) and Zenith (10.6%), devices, a substantial proportion of which were directly related to LGO. In line with these observations, the 2019, the European Society for Vascular Surgery Guidelines strongly recommended long-term surveillance of such low-profile platforms, to better elucidate the mechanisms underlying LGO in LPEGs. 39
With regard to type I endoleak, the outcomes were generally comparable among the LPEGs with the exception of those reported for the InCraft device.12,16 Baccani et al 12 observed a perioperative type I endoleak rate of 20%, which declined during follow-up, while Jin et al 16 reported a similar incidence of 17%, detected intraoperatively or shortly thereafter. In the present meta-analysis, we confirmed a slightly higher rate of type I endoleak associated with the Incraft device compared with other platforms.
Another noteworthy finding was the relatively high incidence of adjunctive procedures, reported in 12.2% of cases, most frequently in patients treated with the InCraft and Zenith platforms. The increased requirement for adjunctive interventions likely reflects to challenging vascular access, particularly in patients with small iliac artery diameters and/or significant tortuosity. Such anatomical difficulties often necessitate additional maneuvers, making adjunctive procedures essential in many cases. 8 A decade ago, adjunctive stenting was already identified as a frequent necessity, and this trend in contemporary practice. 40 These findings may assist in identifying a subset of patients at higher risk for adjunctive procedures, specifically those with hostile iliac anatomies such as small caliber vessels, marked tortuosity, or heavy calcification, features already known to increase technical complexity. 22
The present study has several limitations, most of which reflect those inherent in the included studies. First, the predominantly retrospective design increases the risk of missing data and reporting bias, as key variables were not consistently reported. Moreover, most studies achieved only moderate scores on quality assessment tools such as the NOS, further limiting the strength of the available evidence. Second, substantial heterogeneity was observed with respect to study design, sample size, follow-up duration, endograft type, and the experience level of the participating aortic centers. Outcomes reported from high-volume, specialized centers may not be generalizable to lower-volume centers with less expertise. Furthermore, several aspects of the treatment process including the indications for EVAR, device selection, and the use of adjunctive procedures were left to physician discretion, introducing the potential for selection bias. Consequently, the pooled estimates should be interpreted with caution, as differences in study design (prospective vs. retrospective), variability in device platforms, and non-uniform follow-up protocols likely reduced the comparability and reliability of the reported outcomes. Third, definitions of technical success and major adverse events were not uniform across studies, raising the possibility of outcome overestimation. Fourth, the results cannot be generalized to the broader EVAR population, as most included cases were elective procedures from high-volume centers; outcomes may therefore not be reproducible in lower-volume institutions or in urgent or emergent settings, where perioperative risk is inherently higher. Finally, the lack of detailed data on the underlying mechanisms of limb complications underscores the need for future randomized controlled trials comparing available low-profile endografts to provide more definitive conclusions.
Conclusion
The present findings support the use of low-profile endografts, which have broadened the eligibility for EVAR, particularly in patients with challenging aortoiliac anatomies. Nonetheless, limb-related complications remain the Achilles heel of certain devices, highlighting the need for rigorous postoperative surveillance. Further studies are required to clarify the underlying mechanisms of these complications and to evaluate the long-term durability of low-profile endografts.
Supplemental Material
sj-jpeg-1-jet-10.1177_15266028251388736 – Supplemental material for Thirteen Years Data of Low-Profile Aortic Endografts for Endovascular Aneurysm Repair: A Systematic Review and Meta-Analysis
Supplemental material, sj-jpeg-1-jet-10.1177_15266028251388736 for Thirteen Years Data of Low-Profile Aortic Endografts for Endovascular Aneurysm Repair: A Systematic Review and Meta-Analysis by Georgios I. Karaolanis, Georgios Fanariotis, Nikolaos Bekas, Demetrios Hadjis and Michail G. Peroulis in Journal of Endovascular Therapy
Supplemental Material
sj-jpg-2-jet-10.1177_15266028251388736 – Supplemental material for Thirteen Years Data of Low-Profile Aortic Endografts for Endovascular Aneurysm Repair: A Systematic Review and Meta-Analysis
Supplemental material, sj-jpg-2-jet-10.1177_15266028251388736 for Thirteen Years Data of Low-Profile Aortic Endografts for Endovascular Aneurysm Repair: A Systematic Review and Meta-Analysis by Georgios I. Karaolanis, Georgios Fanariotis, Nikolaos Bekas, Demetrios Hadjis and Michail G. Peroulis in Journal of Endovascular Therapy
Supplemental Material
sj-jpg-3-jet-10.1177_15266028251388736 – Supplemental material for Thirteen Years Data of Low-Profile Aortic Endografts for Endovascular Aneurysm Repair: A Systematic Review and Meta-Analysis
Supplemental material, sj-jpg-3-jet-10.1177_15266028251388736 for Thirteen Years Data of Low-Profile Aortic Endografts for Endovascular Aneurysm Repair: A Systematic Review and Meta-Analysis by Georgios I. Karaolanis, Georgios Fanariotis, Nikolaos Bekas, Demetrios Hadjis and Michail G. Peroulis in Journal of Endovascular Therapy
Supplemental Material
sj-jpg-4-jet-10.1177_15266028251388736 – Supplemental material for Thirteen Years Data of Low-Profile Aortic Endografts for Endovascular Aneurysm Repair: A Systematic Review and Meta-Analysis
Supplemental material, sj-jpg-4-jet-10.1177_15266028251388736 for Thirteen Years Data of Low-Profile Aortic Endografts for Endovascular Aneurysm Repair: A Systematic Review and Meta-Analysis by Georgios I. Karaolanis, Georgios Fanariotis, Nikolaos Bekas, Demetrios Hadjis and Michail G. Peroulis in Journal of Endovascular Therapy
Footnotes
Authors’ Note
Two authors (N.B and G.F.) independently screened the titles and abstracts obtained from the search against the inclusion criteria. Disagreements were resolved through consensus or by discussion, with a third senior reviewer (G.I.K) serving as the final arbitrator. The same 2 reviewers (N.B and G.F) further analyzed the full-text articles against the study inclusion criteria, resolving any discrepancies by discussion and/or referral to the third reviewer (G.I.K) before the data were finally analyzed. After identifying the eligible studies, data were extracted independently by 2 authors (N.B and G.F.) using a predesigned datasheet and uploaded after confirmation of agreement on the data. The protocol of the present study was registered in the PROSPERO public database prior to the study initiation (CRD42025649391).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.