
Abstract
Objective:
To describe early and midterm outcomes of Viabahn stenting for extensive aortoiliac occlusive disease involving the external iliac artery (EIA).
Methods:
In this single-center retrospective study, all consecutive patients in whom a covered self-expanding (SE) Viabahn stent was implanted (W.L. Gore & Associates, Inc, Flagstaff, Arizona) in the EIA for symptomatic Trans-Atlantic Intersociety Consensus (TASC) II C and D lesions between 2012 and 2020 were included. Lesions limited to the iliac artery were treated percutaneously. Iliac lesions extending down to the common femoral artery (CFA) were treated with a hybrid approach. Patency, major adverse limb events (MALEs), target lesion revascularization (TLR), and limb salvage rates were estimated using Kaplan-Meier curves.
Results:
Of 118 limbs, 48 (41%) were treated for claudication, 33 (28%) for rest pain, and 37 (31%) for tissue loss. Lesions were TASC C (n = 43 limbs, 36%) or TASC D (n = 75 limbs, 64%). Chronic total iliac occlusions were identified in 26 limbs (22%). Concomitant CFA lesions were recorded in 97 limbs (82%). All lesions involved the EIA. Technical success was achieved in 100% of cases. Six (5.7%) perioperative major adverse cardiovascular events occurred, including 4 (3.8%) deaths. Eleven (7.6%) early MALEs were recorded. Two-year primary patency, assisted primary patency, and secondary patency were 85%, 88%, and 95%, respectively. After multivariate analysis, small-diameter stents (<8 mm) were associated with lower primary patency rates (hazard ratio [HR] 3.20, 95% confidence interval [CI]: 1.26-8.13, P = .014) and lower freedom from TLR rates (HR 2.61, 95% CI: 1.02-6.66, P = .045). Adjunctive CFA endarterectomy was significantly associated with higher primary patency rates (HR 0.38, 95% CI: 0.15-0.95, P = .038).
Conclusion:
The use of Viabahn SE covered stents for extensive aortoiliac disease involving the EIA provided acceptable postoperative morbidity and high rates of midterm secondary patency, similar to those usually reported with aortobifemoral bypass. Adjunctive CFA endarterectomy was a major determinant of patency and should be considered an essential component of the treatment strategy. Additional long-term data are necessary to evaluate the role of SE covered stents for the treatment of such lesions.
Clinical Impact
The endovascular management of extensive aortoiliac occlusive disease involving the external iliac artery remains challenging. This study represents one of the largest series dedicated to the treatment of TASC II C and D lesions involving the external iliac artery with self-expanding covered stents. The results suggest mid-term secondary patency rates comparable to those commonly reported after aortobifemoral bypass. Notably, concomitant common femoral bifurcation treatment and the use of ≥8-mm diameter stents were associated with improved patency rates, suggesting that aggressive management of common femoral artery lesions and the use of larger-diameter stents may contribute to optimizing long-term outcomes.
Keywords
Introduction
For many years, extensive aortoiliac occlusive disease (AIOD), classified as Trans-Atlantic Intersociety Consensus (TASC) II C and D lesions according to the TASC II guidelines, 1 has been treated by open surgical repair (OR). This strategy provides excellent early and long-term patency rates2-5 but is associated with significant perioperative morbidity and mortality rates.3,5,6 Over the last 2 decades, endovascular techniques have benefited from major technical improvements, leading to an increased use of purely endovascular or hybrid therapies for the treatment of extensive AIOD.7,8 There are reasonable amount of data suggesting that when compared with open repair, endovascular and hybrid repairs (HRs) are associated with lower perioperative morbidity and mortality rates while providing similar long-term outcomes.9-13 Recent guidelines have suggested endovascular and hybrid techniques should be considered as the first-line treatment even for long chronic total occlusions (CTOs) of iliac arteries.14,15 However, there is no consensus on the optimal endovascular therapy. Although a primary stenting is recommended,14-17 the most appropriate type of stent is still debated. Randomized studies suggested that covered stents are associated with better patency rates18,19 as compared with bare metal stents (BMSs). Another randomized study reported reduced restenosis and target lesion revascularization (TLR) rates with self-expandable stents as compared with balloon-expandable stents. 20 However, most studies included mainly patients with lesions of the common iliac artery (CIA). At the external iliac level, due to the arterial mobility and tortuosity, it is common practice to use nitinol self-expanding (SE) stents, but the optimal device is still to be determined. Viabahn covered SE stents (Viabahn, W.L. Gore and Associates, Flagstaff, Arizona) are made of a nitinol scaffold and an ultrathin expanded polytetrafluoroethylene (ePTFE) fabric. They offer excellent flexibility and an acceptable radial force. These mechanical properties make them theoretically suitable for the treatment of long iliac lesions, especially in tortuous external iliac arteries (EIAs). Previous studies showed promising short- and midterm outcomes21-25 of Viabahn stenting for AIOD. The objective of this study is to report the outcomes of Viabahn stents for TASC C and D aortoiliac disease involving the EIA.
Materials and Methods
Study Design and Inclusion
A prospectively maintained database (Saphir Software, Opale, Paris) dedicated to patients undergoing vascular surgery in our unit was used to retrospectively identify patients who underwent iliac stenting using a Viabahn between 2012 and 2020. Informed consent requirements were waived for this retrospective study. Patients treated with the first-generation stents (Hemobahn, W.L. Gore and Associates) were excluded. Patients with TASC A or B lesions, asymptomatic lesions, acute thromboses, or dissections were also excluded. Baseline and procedural data were collected prospectively and analyzed retrospectively. Follow-up data were collected retrospectively. All patients had a preoperative duplex ultrasound and a computed tomography (CT) scan. Follow-up data included physical examination and duplex ultrasound at 30 days, 6 months, 12 months, and yearly thereafter. In case of abnormal finding on duplex ultrasound, a CT scan was performed. All patients received postoperative antiplatelet therapy, usually with a single agent, but in case of concomitant femoropopliteal stenting, a dual therapy could be preferred.
Operative Technique
Lesions extending to the common femoral artery (CFA) were typically treated using a hybrid approach. In a few cases with lesions of the CFA that did not involve the bifurcation, a purely endovascular technique was preferred.
Endovascular Strategy
Under local or general anesthesia, an ipsilateral puncture was preferentially performed to attempt to cross the lesion. In case of stenosis, standard endovascular wires and catheters were used. In case of chronic iliac occlusion, CTO crossing devices such as 0.018 or 0.035 CXI (Cook Medical) devices were used. When retrograde recanalization failed, an anterograde access via a contralateral CFA puncture was rapidly performed. In some cases of long iliac CTOs, brachial or axillary access was necessary. Whenever possible, we tried to stay away from subintimal recanalization. In a few early cases of endoluminal recanalization failure, a subintimal recanalization was performed using a re-entry device (Outback, Cordis) to find the true lumen at the level of CIAs. With growing experience, we abandoned this strategy to prefer recanalization from above. Predilatation using 4 to 6 mm balloons was typically performed before stenting in cases of long iliac CTOs. For lesions of the CIA, covered balloon-expanding (BE) stents were preferred, but a BMS was used in rare cases. In proximal aortoiliac lesions, a kissing stent technique was performed. When the iliac bifurcation was involved, a BMS was used to preserve hypogastric perfusion. In case of occlusion of the hypogastric artery, the Viabahn stent overlapped the covered balloon-expandable stent deployed in the CIA, or the Viabahn stent was used to treat both the EIA and the CIA. Viabahn stents measured 7 to 10 mm in diameter and 50, 100, or 150 mm in length. Stents were usually sized to the vessel diameter, but could be lightly oversized in case of small arteries <7 mm. Postdilatation of the Viabahn stent was performed in all cases, with a same size balloon. In few cases of heavily calcified artery, high-pressure Conquest UHP balloons (Bard Peripheral Vascular Inc, Tempe, Arizona) were used for remodeling. In a few cases of limited extension to the CFA, an angioplasty with or without stenting (T-stenting technique) was performed. In other cases of iliofemoral disease, a hybrid strategy was preferred.
Hybrid Strategy
In case of lesions extending to the CFA, a hybrid treatment was our preferred strategy. Our technique has been previously described. 25 Briefly, under general anesthesia, femoral bifurcation exposure was obtained by a longitudinal groin incision. In most cases, CFA puncture was first performed to cross the iliac lesion. Endovascular techniques used to cross the lesion were as previously described. After crossing the lesion, a longitudinal arteriotomy of the CFA was performed, extending above the epigastric and circumflex iliac arteries. If an anterograde access had been required, the guidewire was externalized through the arteriotomy. The CFA endarterectomy was then performed. After treating iliac lesions as described above, the Viabahn stent was deployed so as to land at the level of the iliofemoral junction and preserve the flow in circumflex iliac and epigastric branches. In cases of length issue, the Viabahn was externalized through the arteriotomy and transected at the iliofemoral junction. Hemostasis was insured with finger compression followed by balloon occlusion. The endarterectomized distal EIA and the Viabahn stent were taken by the first stitches of the patch running suture to insure a stable and soft transition zone. Since the nitinol stents are integrated in the PTFE fabric thanks to bonding films, some of the Viabahn stents were cut without destabilizing the scaffold of the remaining segment. When a suture by patch was not possible, an iliofemoral bypass was performed: both the distal EIA and the Viabahn were taken in the proximal terminoterminal anastomosis. Rarely, an eversion technique was performed.
Definitions
According to the Society for Vascular Surgery, 26 technical success is defined as successful technique to re-establish vessel patency with a residual stenosis of <30%. Primary patency is defined as patency obtained without the need for additional or secondary surgical or endovascular procedures. Assisted primary patency refers to the patency of the endovascular intervention achieved with the use of an additional procedure, as long as occlusion of the primary treated site has not occurred. Secondary patency refers to the patency obtained with the use of an additional procedure after occlusion occurs. Target lesion revascularization (TLR) is defined as any surgical or percutaneous revascularization procedure involving the original target lesions. Indications for TLR were symptomatic stenoses or patency-threatening stenoses. Major adverse limb event (MALE) is defined as above-ankle amputation of the index limb or major reintervention (thrombectomy/thrombolysis, bypass revision, or redo bypass grafting). Major adverse cardiovascular event (MACE) is defined as the composite of myocardial infarction (MI), stroke, and death.
Statistical Analysis
Continuous variables were presented as mean ± SD or median (range), categorical variables as count and percent. Demographic and comorbidity data were recorded per patient. Anatomical and clinical data were reported on a per limb basis. Survival rate curves were calculated and plotted using the Kaplan-Meier method. Univariate analyses were conducted to identify factors predictive of the loss of primary patency, using a Cox proportional hazard regression model. The association of each variable with the outcome was estimated with hazard ratios (HRs) and associated confidence intervals (CIs). In subgroup analyses, data were compared using Pearson’s chi-squared test and Fisher’s exact test for categorical variables, and Welch’s 2-sample t test for continuous variables. The comparison of estimates was performed with the log-rank test. The factors assessed as potential predictors included baseline characteristics (gender, smoking status, age, dyslipidemia, diabetes, chronic renal insufficiency, chronic obstructive pulmonary disease [COPD], cardiac insufficiency, coronary artery disease, prior iliac revascularizations, nontreated occlusion of the superficial femoral artery (SFA), TASC C/D, EIA CTO, and total occlusion of iliac arteries) and preoperative characteristics (stent diameter, adjunctive procedures, and CFA endarterectomy). All the variables that achieved P values < .20 in the univariate analysis were examined with Cox regression multivariate analysis to evaluate independent risk factors for the loss of primary patency. A P value < .05 was considered statistically significant. Data were analyzed using R software version 4.2.2.
Results
Preoperative Data
A total of 118 limbs (105 patients) were included between December 2012 and December 2020 (Figure 1). Demographic data are detailed in Table 1. The indication for surgery was claudication in 41% of limbs and chronic limb-threatening ischemia (CLTI) in 59%. Lesions were TASC C in 36% of limbs and TASC D in 64%. CTO of the entire iliac axis was noticed in 26 limbs (22%). Anatomical data are detailed in Table 2.
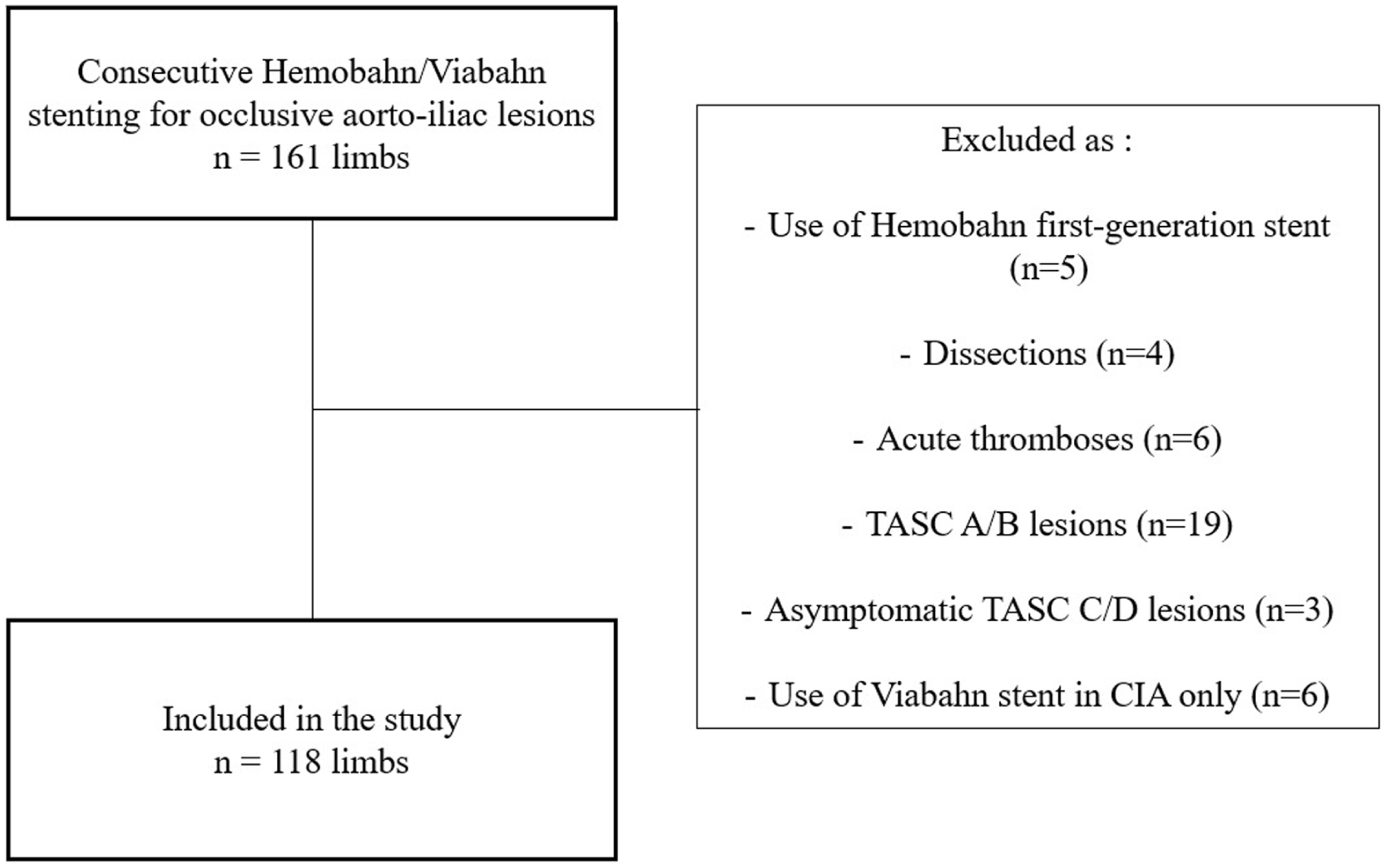
Study flowchart. TASC, Trans-Atlantic Intersociety Consensus; CIA, common iliac artery.
Demographic and Clinical Data (105 Patients, 118 Limbs).
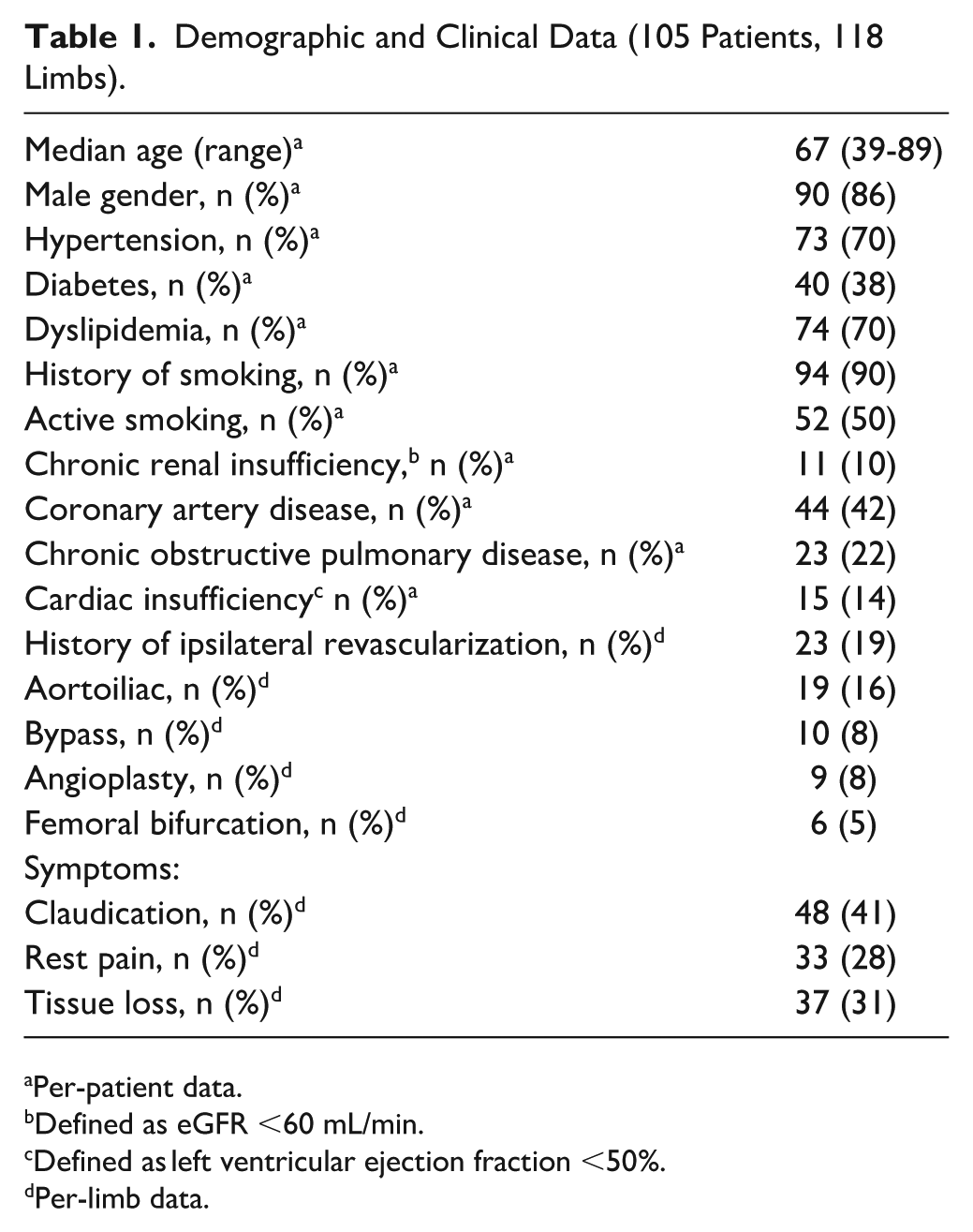
Per-patient data.
Defined as eGFR <60 mL/min.
Defined as left ventricular ejection fraction <50%.
Per-limb data.
Anatomical Characteristics (118 Limbs).
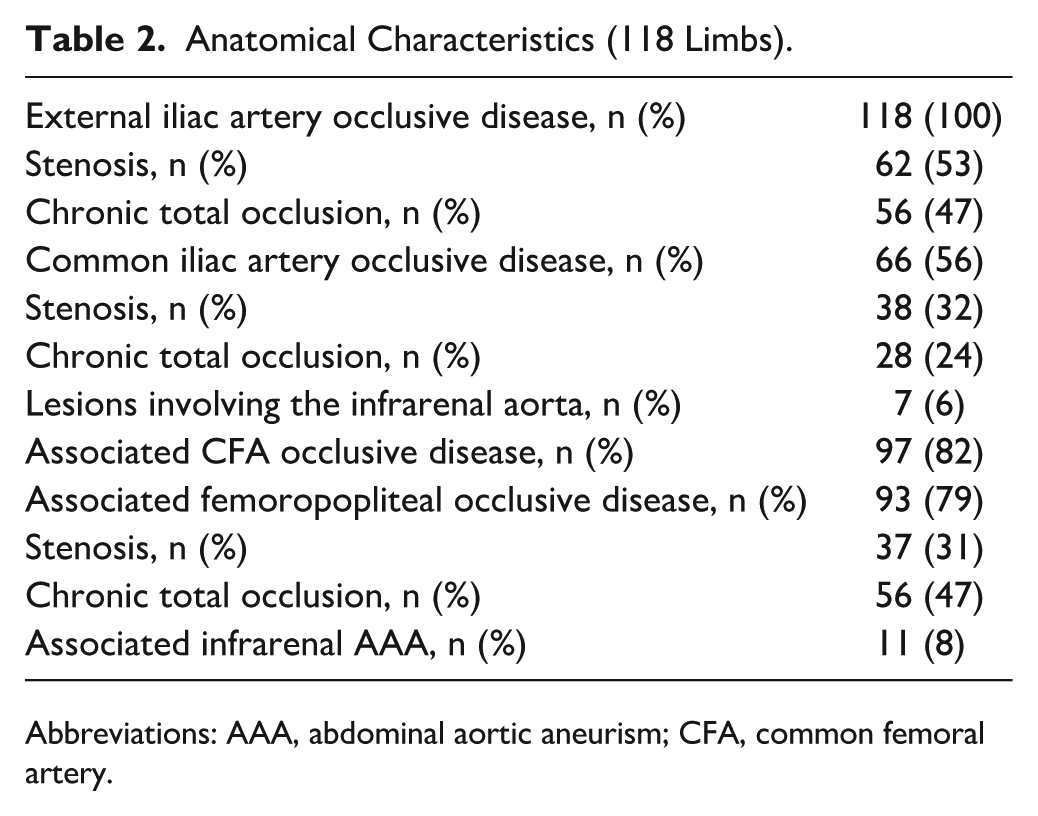
Abbreviations: AAA, abdominal aortic aneurism; CFA, common femoral artery.
Intraoperative Data
Intraoperative data are summarized in Table 3. In the vast majority of cases, a single Viabahn stent was implanted. Two Viabahn stents were deployed in 3 (3%) limbs. Technical success was 100%. Complementary CIA stenting was performed in 59 (50%) limbs, 4 of them were performed as bail-out procedure due to dissections (n = 3) or in situ thrombosis (n = 1). Adjunctive procedures were deemed necessary in 66 limbs (56%). One rupture occurred during predilatation, immediately covered by the Viabahn stent.
Intraoperative Data.
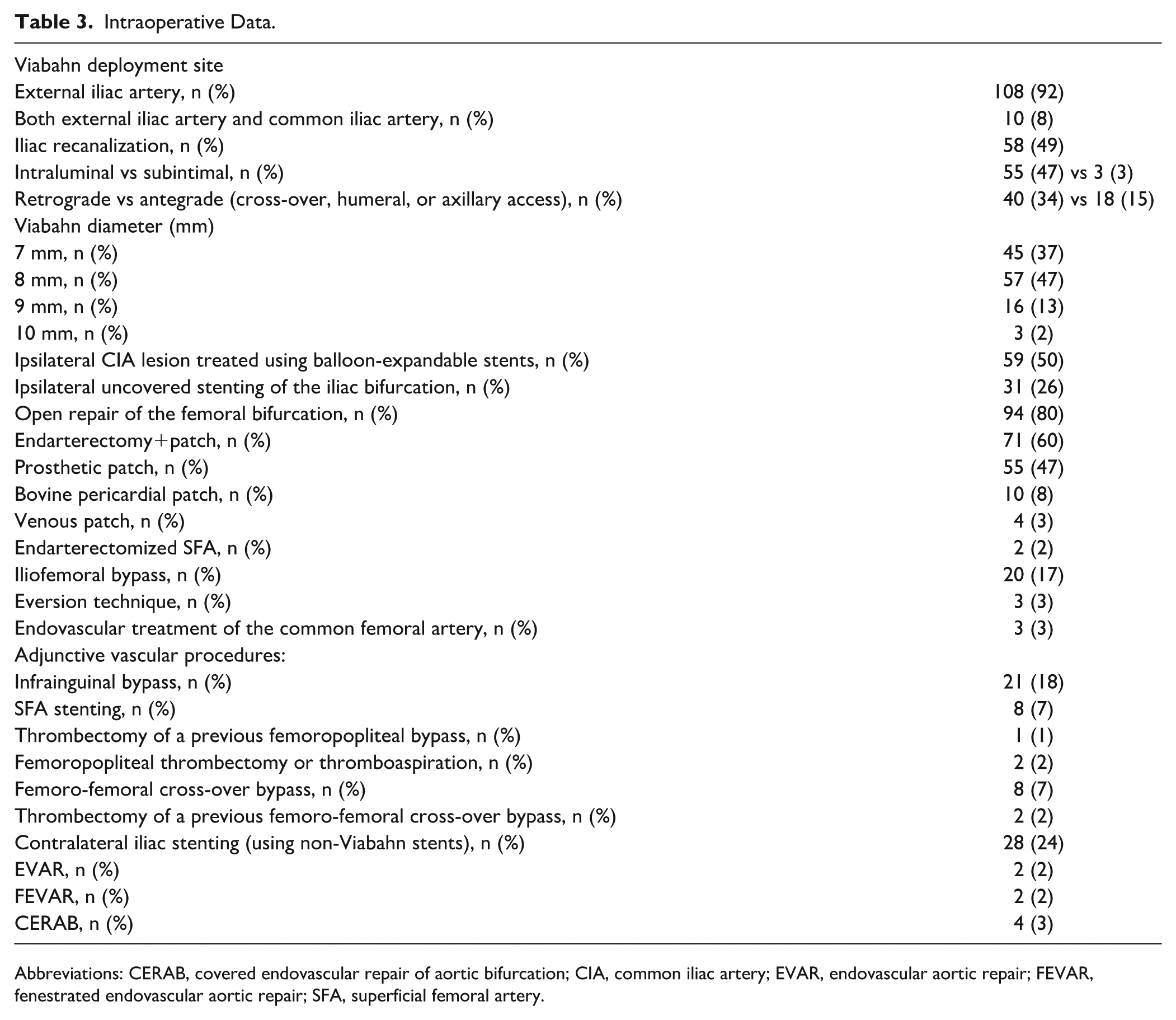
Abbreviations: CERAB, covered endovascular repair of aortic bifurcation; CIA, common iliac artery; EVAR, endovascular aortic repair; FEVAR, fenestrated endovascular aortic repair; SFA, superficial femoral artery.
Early Outcomes
Overall 30-day and in-hospital mortality were 3.8% (4 patients). Deaths occurred in 3 patients (4.8%) with CLTI (1 death after reintervention for groin drainage in an elderly patient, 1 MI, 1 unknown etiology) and in 1 (2.3%) claudicant (1 endocarditis on a bioprosthetic valve). Major adverse cardiovascular events occurred in 6 (5.7%) patients: 1 MI, 1 stroke, and 4 deaths. Five MACEs occurred in patients with CLTI (8.1%), and 1 occurred in a claudicant (4.6%).
Moderate to severe limb-related complications occurred in 15 (12.7%) limbs. They are summarized in Table 4. Major adverse limb events occurred in 9 (7.6%) limbs.
Thirty-Day Limb-Related Complications.
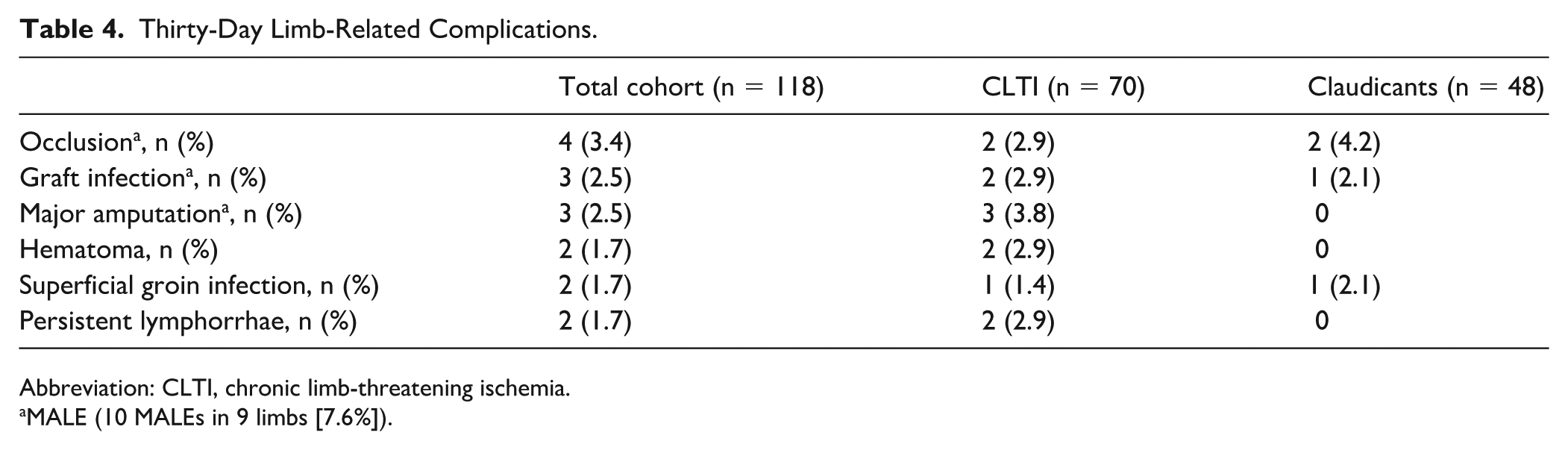
Abbreviation: CLTI, chronic limb-threatening ischemia.
MALE (10 MALEs in 9 limbs [7.6%]).
The median length of stay was 8 days (range 1-42). Length of stay was longer in patients with CLTI: 9 days (interquartile range [IQR] 7-15) versus 6 days (IQR 5-8) in claudicants (P = .015).
Follow-up
Median follow-up was 28.6 months (range 0-93). Kaplan-Meier estimates of overall survival were 87% (95% CI: 80-94) at 1 year, 81% (95% CI: 74-89) at 2 years, and 71% (95% CI: 62-82) at 3 years. Kaplan-Meier estimates of freedom from MALE were 83% (95% CI: 76-91), 80% (95% CI: 72-88), and 73% (95% CI: 64-83) at 1, 2, and 3 years, respectively.
When compared with the preoperative period, the median Rutherford stage was significantly lower at the end of the follow-up (0 [0-2] vs 4 [3-5], P < .001). Kaplan-Meier estimates of freedom from major amputation were 95% (95% CI: 91-99) at 1 year, 93% (95% CI: 88-98) at 2 years, and 90% (95% CI: 84-97) at 3 years (Figure 2A).
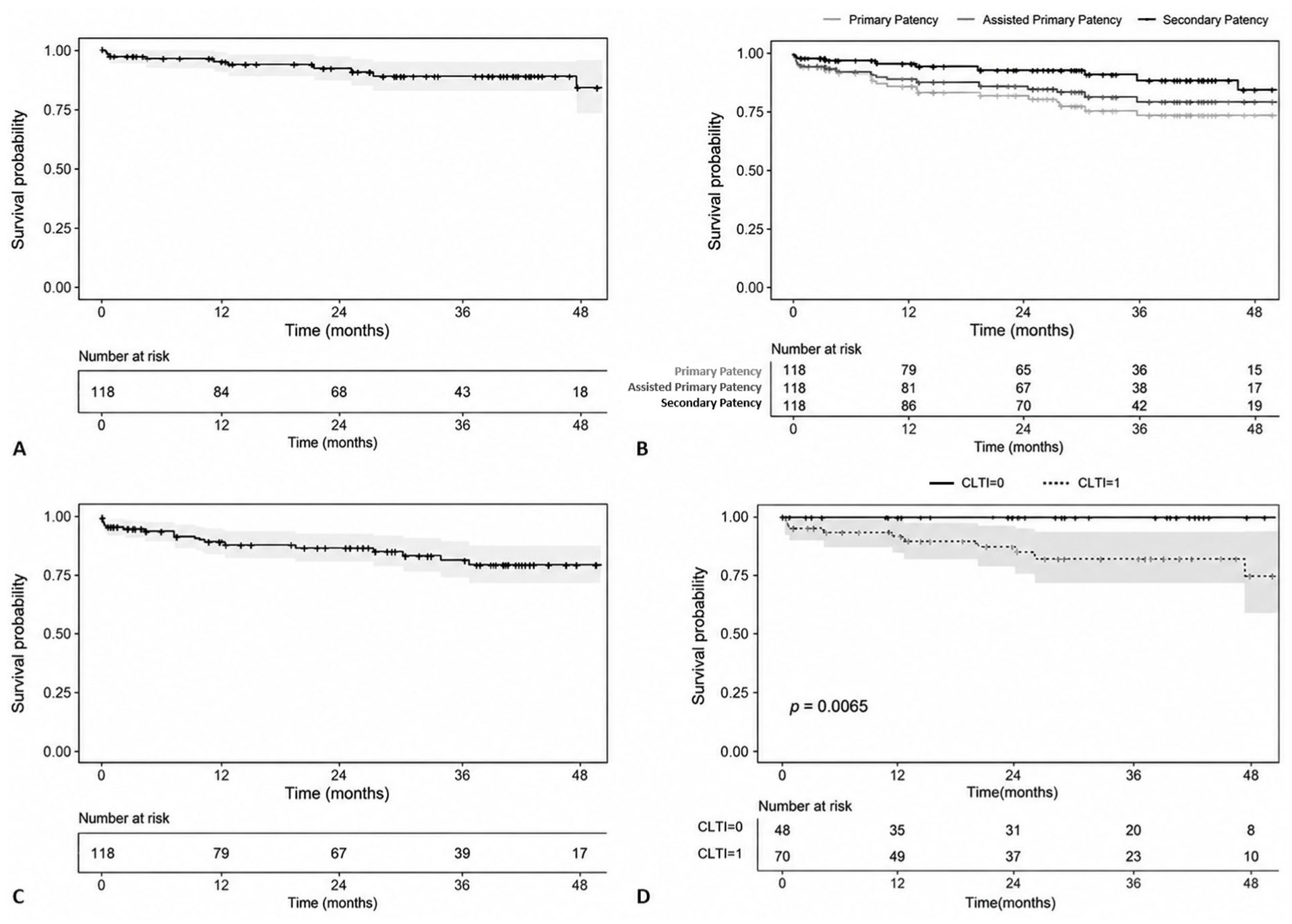
Kaplan-Meier curves with number of patients at risk for: (A) Freedom from major amputation. (B) Primary patency, assisted primary patency, and secondary patency. (C) Target lesion revascularization. (D) Freedom from major amputation in patients with chronic limb-threatening ischemia versus claudicants. CLTI, chronic limb-threatening ischemia; TLR, target lesion revascularization.
Kaplan-Meier estimates of primary patency were 89% (95% CI: 84-96), 85% (95% CI: 78-92), and 78% (95% CI: 69-88) at 1, 2, and 3 years, respectively (Figure 2B). Kaplan-Meier estimates of assisted primary patency were 91% (95% CI: 86-97), 88% (95% CI: 81-95), and 82% (95% CI: 74-91) at 1, 2, and 3 years, respectively (Figure 2B). Kaplan-Meier estimates of secondary patency were, respectively, 97% (95% CI: 94-100), 95% (95% CI: 90-99), and 91% (95% CI: 84-98) at 1, 2, and 3 years (Figure 2B).
Kaplan-Meier estimates of freedom from TLR were 90% (95% CI: 85-96), 87% (95% CI: 80-94), and 79% (95% CI: 70-89) at 1, 2, and 3 years, respectively (Figure 2C).
Subgroup Analyses
Details on subgroup analyses are provided in Table 5. In the group of patients with CLTI (n = 70), Kaplan-Meier estimates of freedom from major amputation were, respectively, at 1, 2, and 3 years of 92% (95% CI: 86-99), 88% (95% CI: 80-97), and 83% (95% CI: 73-94) (Figure 2D). Patency and TLR rates were not significantly different between patients with CLTI as compared with claudicants.
Estimates of Midterm Outcomes With 95% Confidence Bounds in Subgroups.
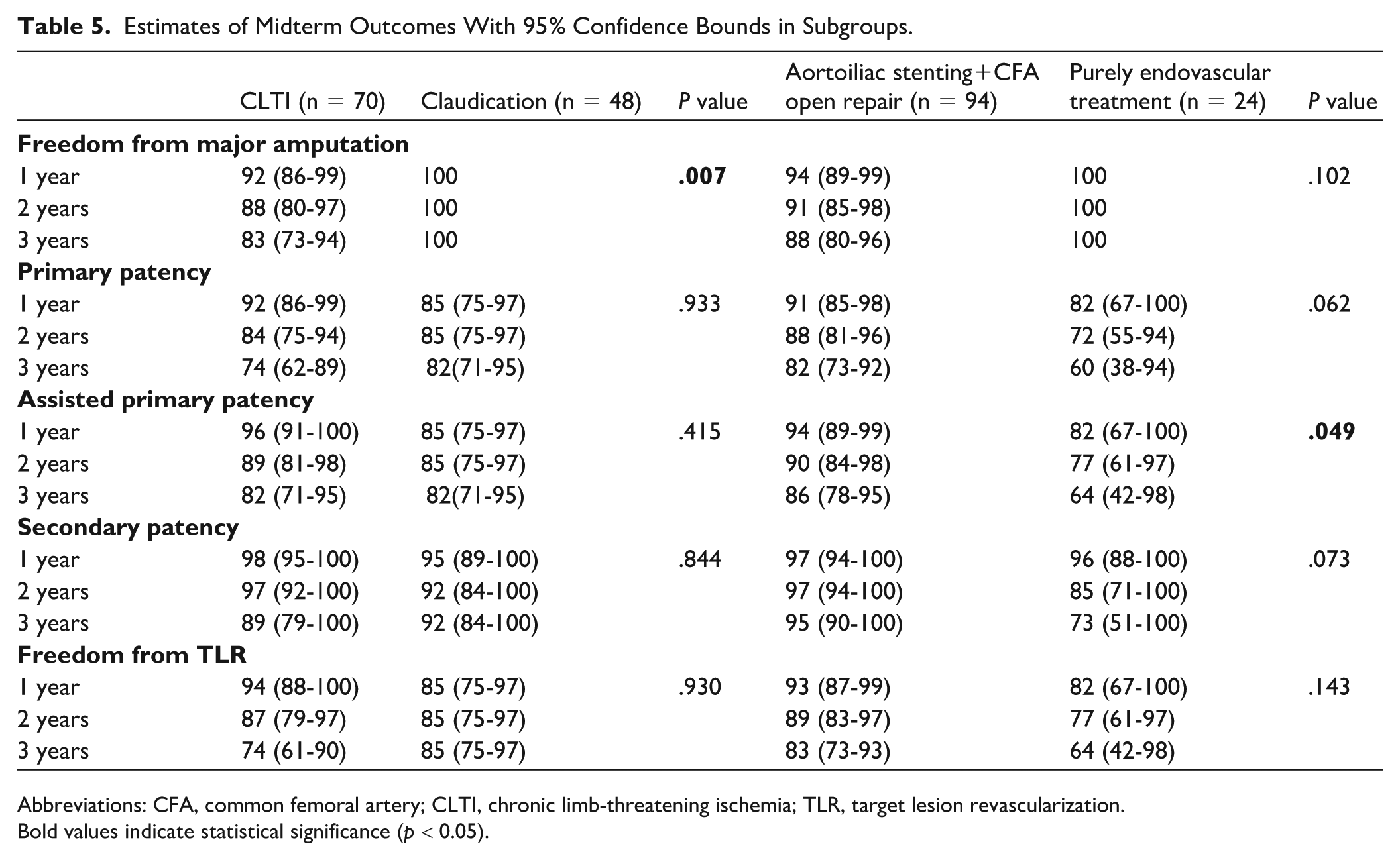
Abbreviations: CFA, common femoral artery; CLTI, chronic limb-threatening ischemia; TLR, target lesion revascularization.
Bold values indicate statistical significance (p < 0.05).
In the group with HR (n = 94), assisted primary patency rates were significantly higher than in the group receiving purely endovascular treatment (P = .049). There was a non-significant trend toward better primary patency rates, secondary patency rates, and freedom from TLR in the hybrid group as compared with the endovascular group. Complete iliac CTO was significantly more frequent in the case of purely endovascular revascularization (50% vs 15%, P < .001) (Table 6).
Comparison of Clinical Data and Anatomical Data in.
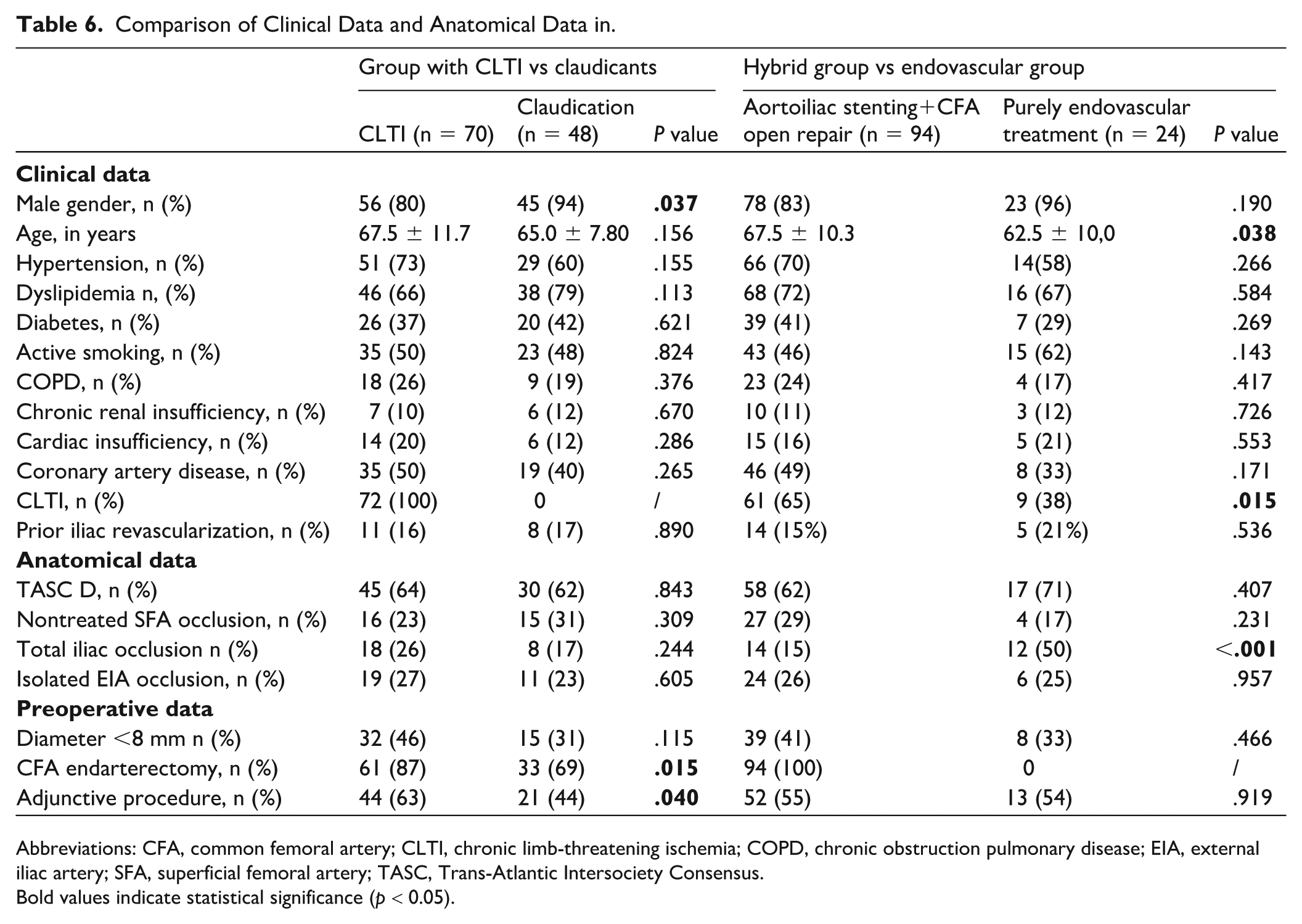
Abbreviations: CFA, common femoral artery; CLTI, chronic limb-threatening ischemia; COPD, chronic obstruction pulmonary disease; EIA, external iliac artery; SFA, superficial femoral artery; TASC, Trans-Atlantic Intersociety Consensus.
Bold values indicate statistical significance (p < 0.05).
Prognostic Factors of Loss of Primary Patency and of Need for Target Lesion Revascularization (Overall Survival Analyses)
All variables with a P value < .20 after univariate analysis were included in the multivariate Cox regression to identify independent predictive factors of loss of primary patency and need for TLR (Table 7). After multivariate analysis, the use of a stent <8 mm was significantly associated with lower primary patency rates (hazard ratio [HR] 3.20, 95% CI: 1.26-8.13, P = .014) and higher TLR rates (HR 2.61, 95% CI: 1.02-6.66, P = .045). Adjunctive CFA endarterectomy was significantly associated with improved primary patency rates (HR 0.38, 95% CI: 0.15-0.95, P = .038).
Univariate and Multivariate Cox Proportional Ratio for Primary Patency and Freedom from TLR.
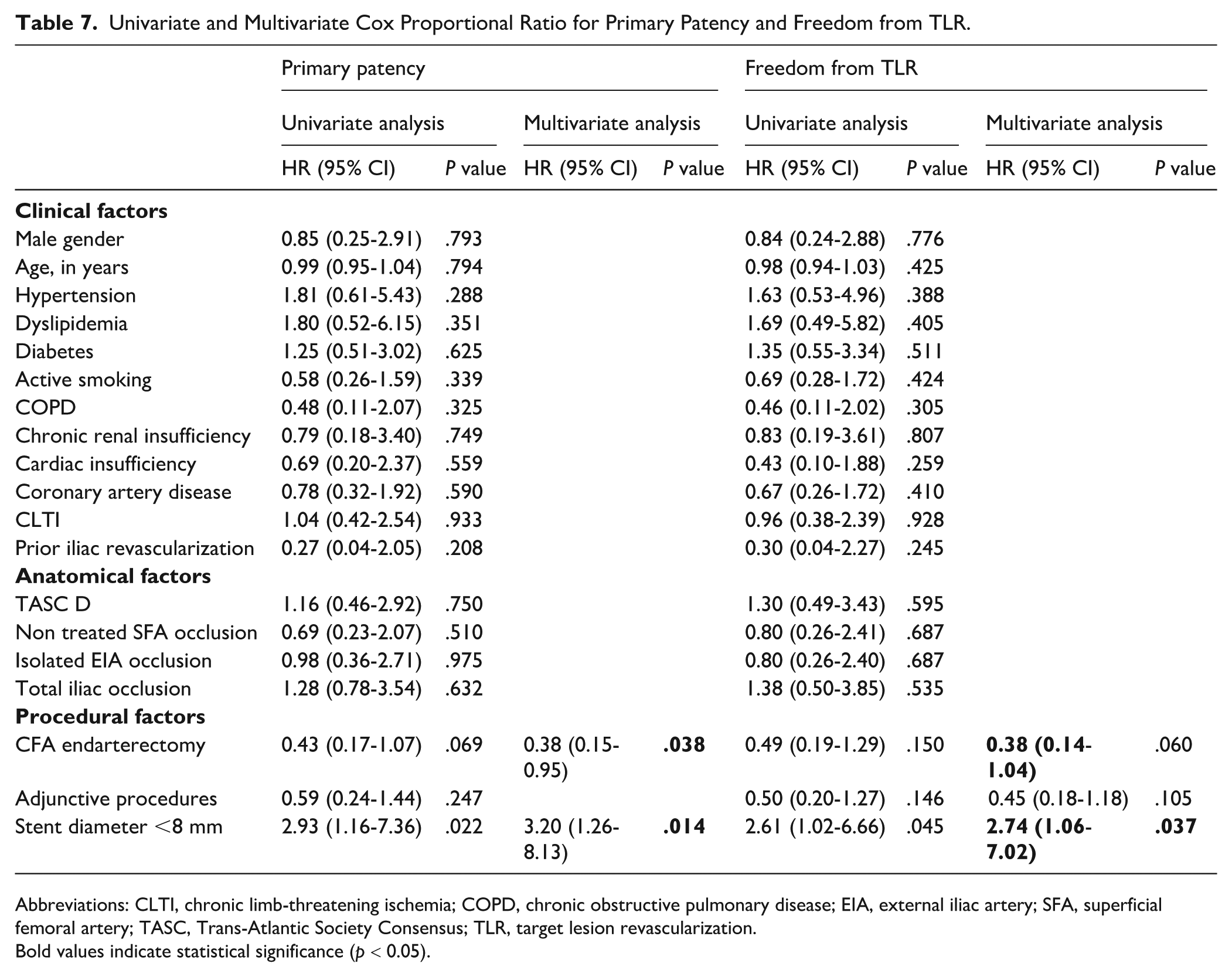
Abbreviations: CLTI, chronic limb-threatening ischemia; COPD, chronic obstructive pulmonary disease; EIA, external iliac artery; SFA, superficial femoral artery; TASC, Trans-Atlantic Society Consensus; TLR, target lesion revascularization.
Bold values indicate statistical significance (p < 0.05).
Discussion
In this retrospective single-center cohort study, Viabahn stents for the treatment of TASC II C/D iliac lesions extending to the EIAs provided an excellent rate of technical success and encouraging midterm results. Technical success was achieved in all procedures, even in the presence of CTOs. Although postoperative complications mainly occurred in fragile patients with CLTI, the MACE (5.7%) and MALE (7.6%) rates were substantial in the current series. They remain consistent with the previously reported postoperative complication rates of 3% to 15% after endovascular repair or HR8-10,27 of TASC II C/D lesions and compare favorably with rates previously reported after aortobifemoral bypass.3,5,6,10,11,28 In our series, the median length of stay was relatively long (8 days) compared with previous reports.7,10,25,29-31 This finding is explained by the high proportion of patients with CLTI (59%), some of them with tissue loss requiring wound care in our unit. Also, it was our practice to discharge patients at least 5 days after HR of iliofemoral lesions. This length of stay was reduced significantly after the COVID-19 crisis and the shortage of nurses in our unit.
Hybrid repair and endovascular repair of complex aortoiliac occlusive lesions have been associated with improved short-term outcomes compared with aortobifemoral bypass. Whether this benefit persists during follow-up is still unclear, as no randomized study comparing long-term mortality, limb salvage, and quality of life has yet been published. Some comparative data suggested similar 1- and 2-year primary patency rates, although long-term primary patency appeared to be higher after open surgery.2-5,10,27,31 However, at the cost of usually minor endovascular reinterventions, it has been suggested that secondary patency rates after endovascular repair or HRs are similar to those of open surgery.7,8,13,32,33 Our results tend to support this finding with a 95% secondary patency rate at 2 years, consistent with the 90% to 100% rates commonly reported after aortobifemoral bypass.4,8,10,27 In the current series, HR seemed to be associated with better outcomes than purely endovascular repair, with higher assisted primary patency and a trend toward higher primary patency, secondary patency, and freedom from TLR. Importantly, management of CFA disease had a major impact on midterm patency: after multivariate analysis, adjunctive CFA endarterectomy was significantly associated with improved primary patency rates (HR 0.38 95% CI: 0.15-0.95, P = .038). This finding should be interpreted in light of the higher prevalence of CTOs among limbs treated with a purely endovascular approach. Overall, these results suggest that the favorable outcomes observed in this series may not be attributed solely to the performance of the Viabahn device, but rather to a broader hybrid strategy combining EIA stenting with optimal treatment of the femoral bifurcation. This underscores the importance of systematic assessment and aggressive management of CFA disease in patients with extensive aortoiliac occlusive lesions. Previous series reported similar results with patency rates competing with those reported by open repair.12,24,25,28,30,34 Recently, Starodubtsev et al 35 , in a randomized prospective trial comparing HR with OR for TASC II C and D lesions, showed comparable primary patency rates in the 2 groups (93% vs 93% at 1 year and 91% [HR] vs 89% [OR] at 3 years, P = .38). In our early practice of treatment of complex iliac lesions using Viabahn stents, we may have underestimated occlusive lesions of the CFA, which remained untreated. It has now become our current practice to treat aggressively lesions of the CFA. This strategy is in line with the recent guidelines, which suggest that any CFA lesions >50% in patients with CLTI should undergo surgical treatment.36,37 In this series, CFA lesions were preferably treated by open repair. In our practice, endovascular treatment was limited to fragile or obese patients. Although endovascular repair of the CFA has been associated with encouraging short- and midterm results,38,39 dedicated stents devices are still lacking.
Our study focused on the use of Viabahn stents to treat extensive EIA lesions, which have been associated in extensive iliac disease involving the EIA. Few studies have focused on specific patency rates after endovascular treatment of EIA lesions.29,40-43 and lower patency rates than those reported after isolated CIA treatment have been observed.41,43 Timaran et al 43 reported a 5-year primary patency rate of 23% after EIA stenting versus 72% after CIA stenting. However, these studies included first-generation BMS, both SE and BE. The choice of stent at the EIA level is particularly difficult. Due to the mobility of the EIAs and their tendency to tortuosity, the use of SE nitinol stents is often preferred at this level. The ICE randomized controlled trial found significantly lower 1-year restenosis rates for SE stents than for BE stents (6.1% vs 14.9%, P = .006), with this difference appearing to be greater in the EIA. 20 Self-expanding stents have a high conformability and flexibility that make them suitable in tortuous iliac arteries. Covered stents have also been suggested to offer better early and long-term outcomes at the iliac level,18,19,44 reducing the risk of peripheral embolism and intrastent restenosis caused by myo-intimal hyperplasia. The COBEST (Covered Versus Balloon-Expandable Stent Trial) trial confirmed these findings, with higher primary and secondary patency rates for covered stents in TASC II C and D lesions.18,44 In contrast, recently, the DISCOVER trial (Dutch Iliac Stent trial: COVERed balloon-expandable vs uncovered balloon-expandable stents in the CIA) did not find any significant difference between SE and BE stents regarding binary restenosis, freedom from occlusion, and TLR at 2 years. 45 Several meta-analyses and retrospective studies corroborated these mixed results.19,46-49 These findings must be interpreted with particular caution, given the inclusion of various anatomic lesions, strategies, and devices. Nevertheless, these studies converge on the superiority of covered stents in severe lesions (TASC II C and D).
Viabahn covered nitinol SE stents should be a good option in the management of long EIA occlusive disease. Bracale et al 22 reported excellent patency rates in 61 limbs with TASC II C and D AIOD though anatomical site information was not available. Psacharopulo et al 21 compared open repair with Viabahn stenting in a prospective study of 41 patients with TASC D lesions, finding no significant difference in primary patency at 2 years, but a shorter length of stay after Viabahn stenting. Lesions involved EIA in 50% of cases. Recently, Squizzato et al 40 in a multicenter retrospective study about 93 patients receiving primary endovascular treatment of EIA occlusive disease with Viabahn stents reported excellent primary and secondary patency rates (respectively, 89.8% and 91% at 42 months). In the present series, secondary patency rates seemed comparable (91% after 36 months), but primary patency rates were lower (78% after 36 months vs 90% after 42 months). Squizzato et al included all TASC categories and excluded lesions involving the CIA, which may explain their better primary patency rates.
The use of a stent diameter <8 mm was significantly associated with the loss of primary patency and higher TLR rates. These results are in line with previous studies32,40,50 and imply an adverse effect of small-diameter arteries on primary patency. In contrast to BMS, Viabahn stents could easily be oversized in these cases without any risk of rupture.
Our study has some limitations: first, it is intrinsically limited by its single-center retrospective design. Then, the limited number of events may have limited the statistical analysis. No control group was used to compare our results with OR or other endovascular devices. In addition, we could not identify patients for whom a Viabahn stenting was scheduled but not implemented due to a failed recanalization, potentially overestimating technical success in these extensive lesions. Finally, the high proportion of hybrid procedures limits the interpretation of our results regarding the isolated performance of Viabahn stents, as outcomes are strongly influenced by concomitant treatment of CFA disease.
Conclusion
To our knowledge, this study is the largest to evaluate Viabahn stent-graft implantation for extensive AIOD involving the EIA. This strategy was associated with acceptable postoperative morbidity and high midterm secondary patency, comparable to rates commonly reported after aortobifemoral bypass. Our results suggest that using larger-diameter stents and aggressively treating CFA disease may improve patency rates, to be closer to those reported by aortobifemoral bypasses. However, additional long-term data are necessary to evaluate the role of SE covered stents for these complex lesions.
Footnotes
Ethical Considerations
For this type of retrospective study, formal consent is not required.
Consent for Publication
Consent for publication was not required for this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.