
Abstract
Purpose:
To evaluate the efficacy and periprocedural safety of distal puncture-assisted bidirectional endovascular therapy (EVT) for de novo femoropopliteal chronic total occlusion (FP-CTO).
Methods:
This multicenter retrospective study included 5 institutions and was conducted between 2019 and 2022. Outcomes and complications were analyzed per procedure (94 procedures); major amputation and mortality were assessed per patient based on the index procedure (87 patients). Major complications were defined as the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) classification grade ≥3.
Results:
Wire-crossing success was 98.9%, and technical success was 84.0%. Complications occurred in 23.4% of procedures, including major complications in 8.5% and distal access-site complications in 10.6%, with no major distal access-site complications observed. Distal embolization occurred in 6.4% of procedures and was uniformly graded as CIRSE grade 1. At 1 year, freedom from target lesion revascularization was 82.0%, whereas limb salvage and overall survival were 97.0% and 85.6%, respectively.
Conclusion:
In this selected multicenter cohort, distal puncture-assisted bidirectional EVT achieved a high wire-crossing success rate, with no adjudicated major distal access-site complication identified using the CIRSE classification. However, these safety findings should be interpreted with caution, as failed distal puncture attempts were not captured and the temporal attribution of distal embolization could not be fully established.
Clinical Impact
Distal puncture-assisted bidirectional endovascular therapy may be a useful bailout or planned strategy for complex femoropopliteal chronic total occlusions when conventional antegrade crossing is difficult. This multicenter study provides contemporary procedural outcomes and Cardiovascular and Interventional Radiological Society of Europe-graded complication profiles, allowing clinicians to interpret not only technical success but also the severity and clinical relevance of complications. The findings may help operators discuss procedural risk, select appropriate access strategies, and standardize complication reporting in femoropopliteal CTO interventions. Further studies including attempted but unsuccessful distal puncture cases are needed to define the overall risk-benefit profile of this approach.
Keywords
Introduction
Lower extremity artery disease (LEAD) is a common atherosclerotic condition that can cause functional limitations and, when it progresses to chronic limb-threatening ischemia (CLTI), is associated with a high risk of limb loss and death.1,2 Accordingly, endovascular therapy (EVT) has become a major revascularization option for symptomatic LEAD/CLTI, consistent with recommendations in contemporary clinical guidelines.1,2 Antegrade crossing of femoropopliteal chronic total occlusion (FP-CTO) can be challenging, particularly in long, heavily calcified lesions or those with an ambiguous proximal cap. Antegrade strategies may fail to achieve distal true lumen re-entry in a considerable proportion of cases, even when performed by experienced operators, highlighting the clinical need for alternative crossing techniques. 3 Procedural failure may lead to longer procedure times, higher radiation and contrast exposure, and the potential need for surgical revascularization or, in CLTI, an increased risk of limb loss.
To improve crossing success, bidirectional approaches using retrograde access have been increasingly adopted. The subintimal arterial flossing with antegrade-retrograde intervention (SAFARI) technique introduced the concept of connecting antegrade and retrograde channels to facilitate recanalization when antegrade re-entry is unsuccessful. 4 Subsequently, multiple retrograde access routes—including popliteal, distal femoral, and tibiopedal punctures—have been described as viable alternatives. Contemporary reports and systematic reviews suggest that ipsilateral retrograde approaches can achieve high technical success with acceptable complication rates.5,6
Distal puncture may improve wire-crossing success but is associated with access-site complications, including hemorrhage, pseudoaneurysm formation, arteriovenous fistula, and distal embolization. However, existing reports vary considerably in terms of patient selection, access techniques, and definitions of complications, and a standardized classification system for grading complication severity has not been consistently applied. The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) classification system provides a standardized framework for grading complications, enabling more consistent safety assessment across studies. 7
In this multicenter retrospective study, we evaluated the effectiveness of bidirectional EVT incorporating distal puncture for FP-CTO and assessed periprocedural complications, with the use of severity grading according to the CIRSE classification system.
Materials and Methods
Study Design and Population
We conducted a retrospective, multicenter study at 5 institutions in Hokkaido, Japan. Consecutive cases treated between July 2019 and July 2022 were screened for eligibility. Included cases were those in which EVT was performed for de novo FP-CTO using a bidirectional approach incorporating distal puncture as retrograde access. We excluded cases involving acute or subacute thrombotic occlusions, non-de novo lesions requiring repeat intervention, and those complicated by severe infection. In total, 94 procedures in 87 patients were included, with 7 procedures representing contralateral limb interventions. Procedural outcomes and complications were analyzed on a per-procedure basis (n=94), whereas major amputation and overall survival were assessed per patient using the index procedure, defined as the first-treated limb (n=87).
This study was approved by the institutional ethics committees of all participating centers and conducted in accordance with the Declaration of Helsinki and the Ethical Guidelines for Medical and Health Research Involving Human Subjects issued by the Japanese Ministry of Health, Labor, and Welfare. Given the retrospective design and use of anonymized data without biological specimens, the ethics committees granted a waiver of written informed consent. In lieu of written informed consent, study information including an opt-out option was disclosed on the websites of all participating institutions, allowing patients or their proxies to decline participation.
Procedure and Access Strategy
Distal puncture was performed in all procedures included in this study. The timing of distal puncture, whether employed as the primary crossing strategy or as a salvage approach following failed antegrade crossing, was left to the discretion of the treating operator. Distal puncture sites were categorized as the distal superficial femoral artery, the popliteal artery, or an infrapopliteal artery, including the tibioperoneal trunk and the crural vessels, namely the anterior tibial, posterior tibial, and peroneal arteries. The use of ultrasound guidance, choice of puncture device, intraprocedural heparin dose, and method of distal access-site hemostasis were not predefined and were determined by each operator according to lesion characteristics and institutional practice. Hemostasis at the distal puncture site, including balloon-assisted hemostasis and thrombin use, was recorded and is summarized in Table 2. Because this retrospective registry included only procedures in which distal puncture was successfully established and incorporated into a bidirectional approach, failed distal puncture attempts were not captured and could not be analyzed. Accordingly, the proportion of FP-CTO procedures in which distal access was attempted or required to achieve crossing could not be determined from this registry. The timing of first recognition of distal embolization relative to guidewire crossing, device manipulation, lesion preparation, stent implantation, or distal hemostatic maneuvers was not prospectively or systematically recorded in this retrospective registry. In practice, distal embolization was typically identified on completion angiography. As this was a retrospective multicenter registry, distal puncture technique and procedural strategy were not standardized across centers and were only partially recoverable from the source records.
Definitions
Chronic kidney disease (CKD) was defined as an estimated glomerular filtration rate <60 mL/min/1.73 m2 8 or maintenance dialysis. Distal puncture was defined as percutaneous retrograde arterial access distal to the target CTO lesion. Wire-crossing success was defined as successful passage of a guidewire, with or without a microcatheter, through the CTO with confirmed entry into the distal true lumen, as assessed by angiography, with or without intravascular ultrasound (IVUS). Technical success was defined as a final residual stenosis of ≤30%, as visually estimated on completion angiography. Complications were categorized into 4 types. Distal access-site complications were those attributable to the distal puncture site. Primary access-site complications were those attributable to the primary access site. Target lesion- and device-related complications were non-access-site complications attributable to the treated segment or devices, including distal embolization, acute occlusion or thrombosis, and device-related events. Systemic complications were periprocedural adverse events not attributable to the distal access site, the primary access site, or the target lesion or device. Complication severity was graded using the CIRSE classification 7 ; major complications were defined as CIRSE grade ≥3 and minor complications as CIRSE grades 1 to 2.
Outcome Measures
The primary efficacy endpoint was wire-crossing success, and the secondary efficacy endpoint was technical success.
The safety endpoints were periprocedural complications. In analyses at the event level, each distinct complication was counted as a separate event. In analyses at the procedure level, each procedure was classified according to the occurrence of any complication and, separately, any major complication. Procedures involving more than one complication event were consolidated into a single row in the procedure-level complication table.
Time-to-event outcomes at 1 year included target lesion revascularization (TLR), major amputation, and all-cause mortality. Time to TLR was calculated from the date of the corresponding procedure, whereas time to major amputation and all-cause mortality were calculated from the date of the index EVT. Patients were censored at the last available follow-up date; those lost to follow-up were censored at the date of last contact.
Statistical Analysis
Categorical variables were presented as counts and percentages, and continuous variables as mean±standard deviation or median (interquartile range), as appropriate. Proportions were reported with exact 95% confidence intervals (CIs). Procedural outcomes and periprocedural complications were analyzed on a per-procedure basis (n=94). For time-to-event analyses at 1 year, TLR was evaluated on a per-procedure basis among procedures with successful guidewire crossing (n=93), whereas major amputation and all-cause mortality were evaluated on a per-patient basis (n=87).
All statistical analyses were performed using EZR version 1.61 (Jichi Medical University, Tochigi, Japan), a graphical user interface for R version 4.2.2 (The R Foundation for Statistical Computing, Vienna, Austria). EZR is a modified version of R Commander designed for biostatistics. 9
Results
Baseline characteristics at enrollment are summarized in Table 1. The mean age was 74.6±9.0 years, and 46 patients (52.9%) were male. Common comorbidities included hypertension (86.2%), diabetes mellitus (47.1%), dyslipidemia (65.5%), and CKD (62.1%); 15 patients (17.2%) were receiving maintenance hemodialysis. Chronic limb-threatening ischemia was present in 34 patients (39.1%). The mean left ventricular ejection fraction was 60.2%±12.2%.
Baseline Characteristics of 87 Patients.
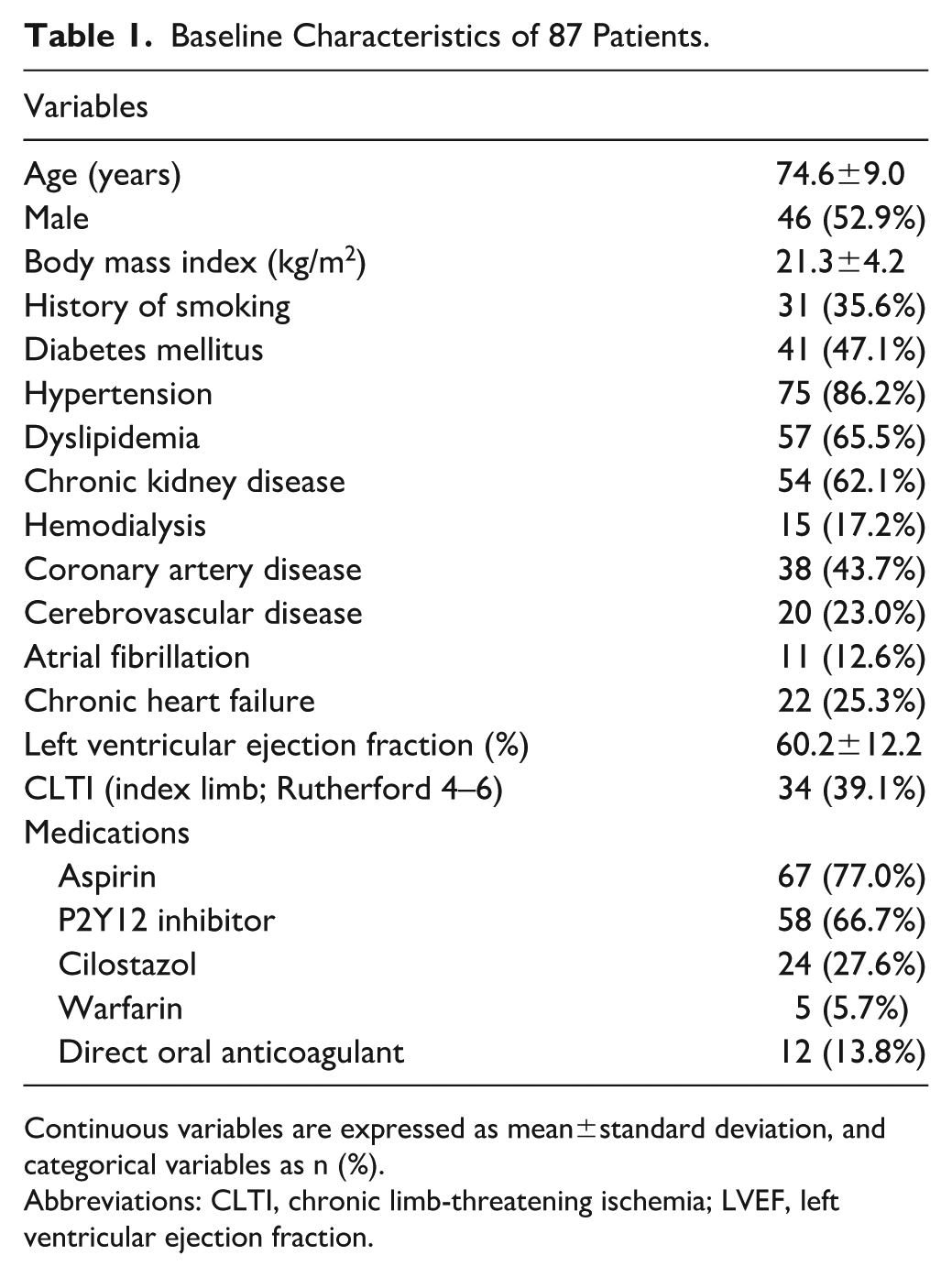
Continuous variables are expressed as mean±standard deviation, and categorical variables as n (%).
Abbreviations: CLTI, chronic limb-threatening ischemia; LVEF, left ventricular ejection fraction.
Lesion characteristics are summarized in Table 2. Distal access was obtained via the distal superficial femoral artery in 57 procedures (60.6%), the popliteal artery in 28 (29.8%), and an infrapopliteal artery in 9 (9.6%). According to the Trans-Atlantic Inter-Society Consensus II (TASC II) classification, 10 lesions were classified as B in 4 procedures (4.3%), C in 34 (36.2%), and D in 56 (59.6%). The Global Limb Anatomic Staging System (GLASS) stage distribution was stage 1 in 1 (1.1%), stage 2 in 11 (11.7%), stage 3 in 27 (28.7%), and stage 4 in 55 (58.5%). The median CTO length was 200 mm (interquartile range [IQR], 120–220), and the median procedure time was 153 minutes (IQR, 115–185).
Lesion/Procedural Characteristics of 94 Procedures.
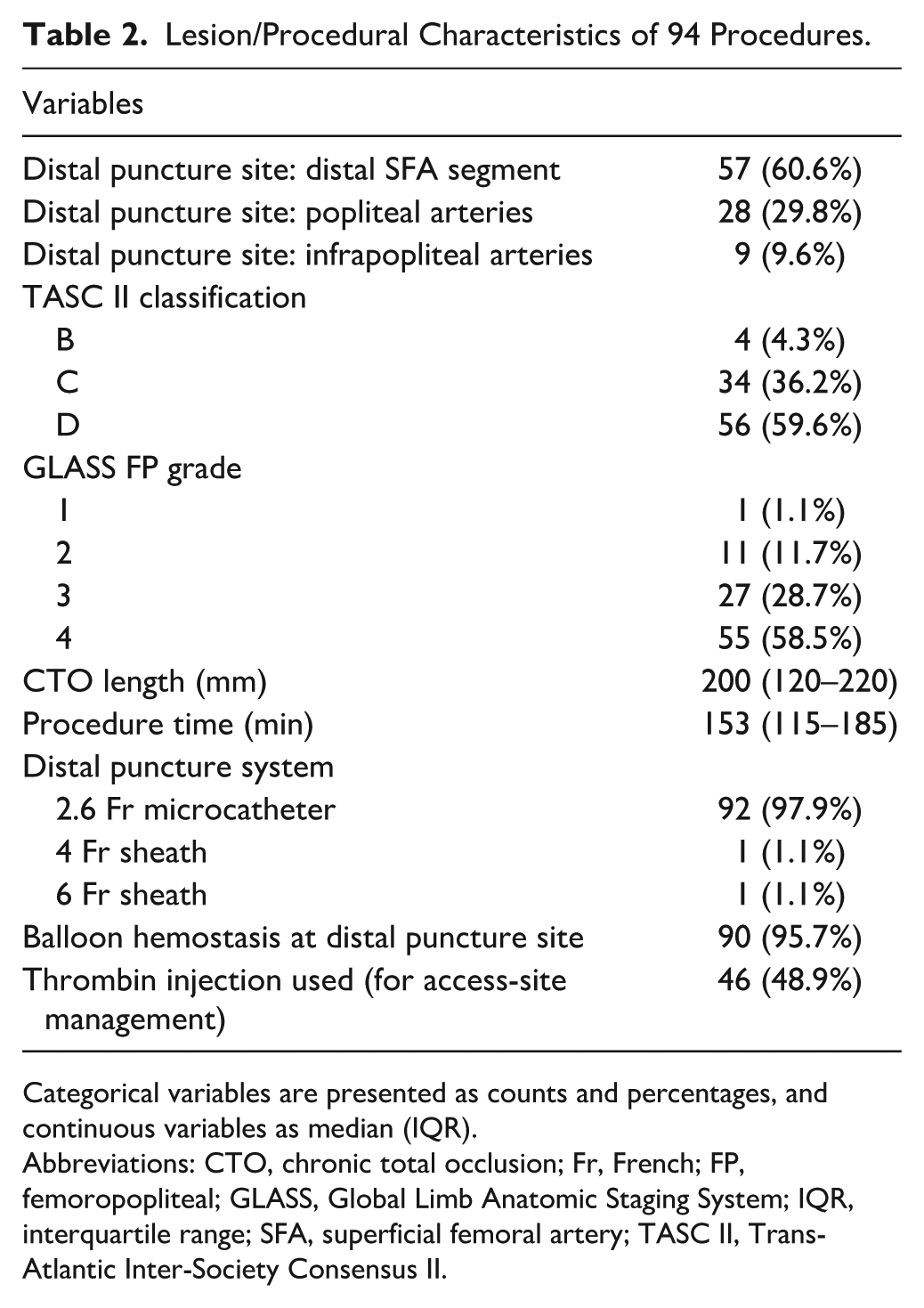
Categorical variables are presented as counts and percentages, and continuous variables as median (IQR).
Abbreviations: CTO, chronic total occlusion; Fr, French; FP, femoropopliteal; GLASS, Global Limb Anatomic Staging System; IQR, interquartile range; SFA, superficial femoral artery; TASC II, Trans-Atlantic Inter-Society Consensus II.
Procedural Outcomes
Wire-crossing success was achieved in 93 procedures (98.9%; 95% CI, 94.2–99.8). Technical success was achieved in 79 procedures (84.0%; 95% CI, 75.3–90.1), corresponding to 79 of 93 wire-crossing successes (84.9%). Among the 93 procedures with successful wire crossing, 14 did not meet the technical success criterion due to residual stenosis exceeding 30% on completion angiography. Of these, 13 involved TASC II C/D lesions, 12 involved GLASS FP grade 3/4 lesions, and 12 were treated without scaffolding (Table 3).
Procedural Characteristics of 14 Procedures With Successful Wire Crossing but Without Technical Success.
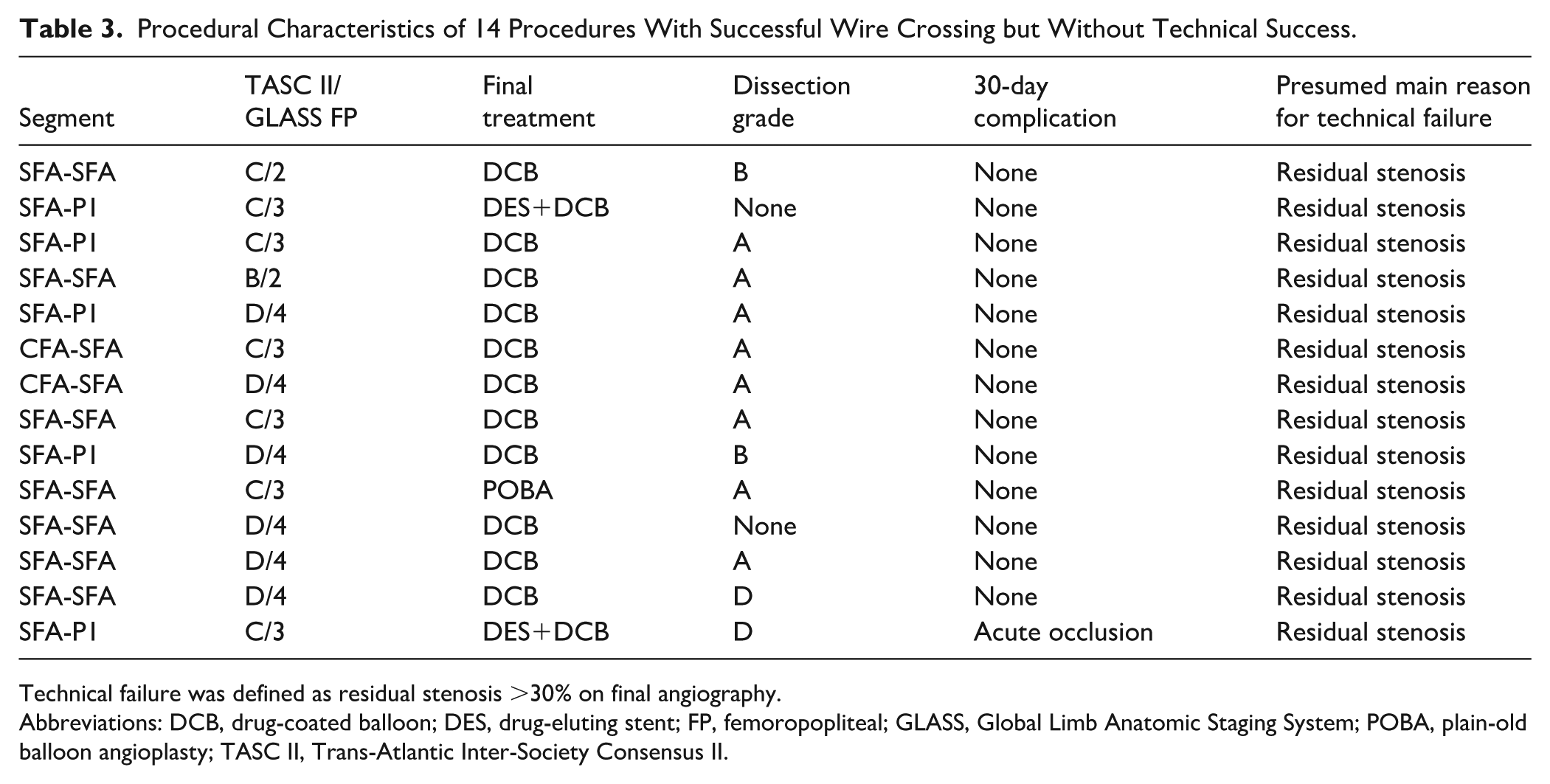
Technical failure was defined as residual stenosis >30% on final angiography.
Abbreviations: DCB, drug-coated balloon; DES, drug-eluting stent; FP, femoropopliteal; GLASS, Global Limb Anatomic Staging System; POBA, plain-old balloon angioplasty; TASC II, Trans-Atlantic Inter-Society Consensus II.
Complications occurred in 22 of 94 procedures (23.4%; 95% CI, 16.0–32.9); a detailed procedure-level list is provided in Table 4. Major complications (CIRSE grade ≥3) occurred in 8 of 94 procedures (8.5%; 95% CI, 4.4–15.9). Distal access-site complications occurred in 10 of 94 procedures (10.6%; 95% CI, 5.2–18.7), all of which were minor (CIRSE grade 1); no major distal access-site complications were observed (0 of 94; 0.0%; 95% CI, 0.0–3.8). Target lesion- and device-related complications occurred in 10 of 94 procedures (10.6%; 95% CI, 5.2–18.7), including distal embolization in 6 procedures (6.4%; 95% CI, 2.4–13.4), all adjudicated as CIRSE grade 1; the remaining 4 were major events (4.3%; 95% CI, 1.2–10.5). Primary access-site complications occurred in 3 of 94 procedures (3.2%; 95% CI, 0.7–9.0), and 1 systemic complication was recorded. As 2 procedures involved more than one complication event, these category counts are not mutually exclusive. The timing of first recognition of distal embolization could not be reliably determined from the retrospective records, as it was documented on final angiography rather than at a predefined procedural step. Thrombin use for distal hemostasis was documented in 93 of 94 procedures; thrombin was used in 46 and not used in 47, with 1 procedure having missing data. All 6 distal embolization events occurred in thrombin-treated procedures (6/46; 13.0%) and none in procedures without documented thrombin use (0/47).
Procedure-Level List of Periprocedural Complications (n=22 Procedures).
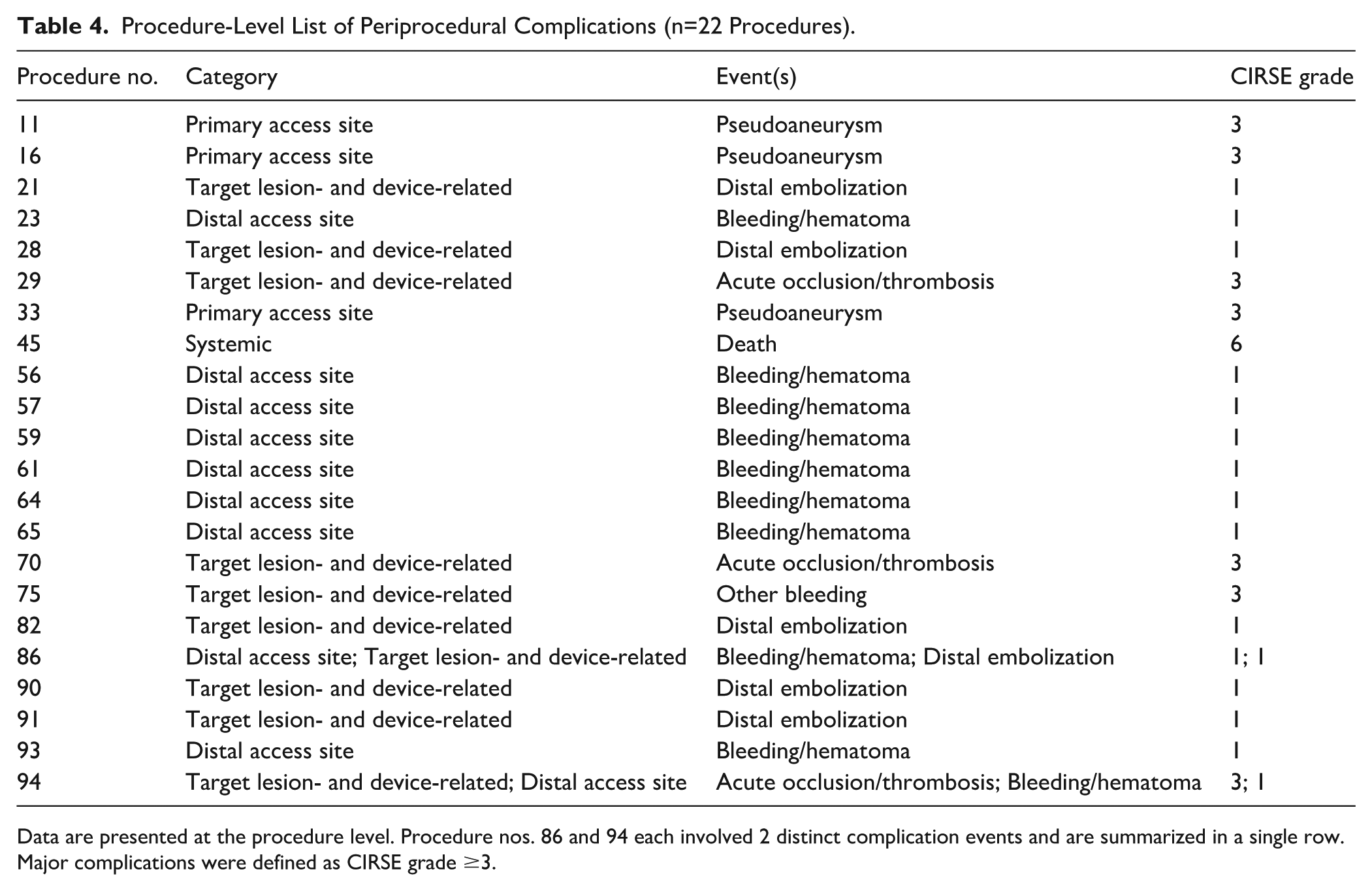
Data are presented at the procedure level. Procedure nos. 86 and 94 each involved 2 distinct complication events and are summarized in a single row. Major complications were defined as CIRSE grade ≥3.
Figure 1 shows the Kaplan-Meier curves for the 1-year time-to-event outcomes. Among surviving patients, the median patient-level follow-up was 321 days (IQR, 87–673). Target lesion revascularization at 1 year was evaluated on a per-procedure basis among the 93 procedures with successful guidewire crossing. The 1-year freedom from TLR was 82.0% (95% CI, 68.4–90.2). Major amputation was evaluated on a per-patient basis (n=87), with 2 events, and the 1-year limb-salvage rate was 97.0% (95% CI, 88.6–99.3). All-cause mortality was evaluated on a per-patient basis (n=87), with 8 deaths, and the 1-year overall survival rate was 85.6% (95% CI, 72.7–92.6).
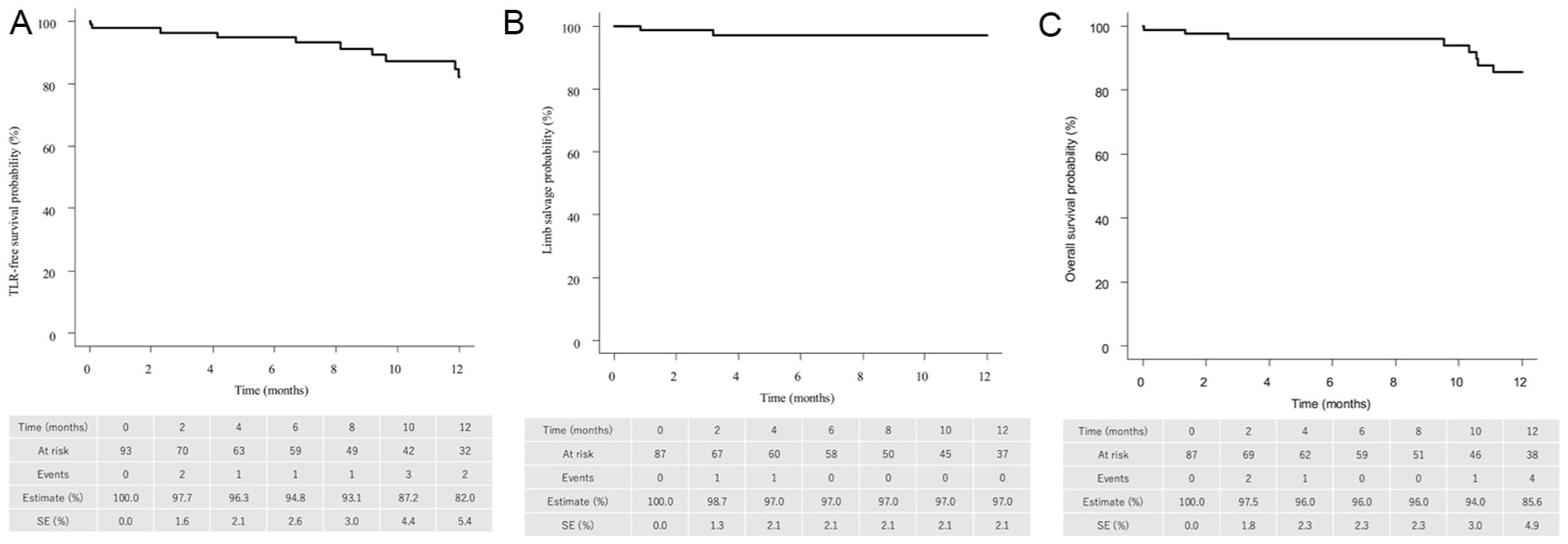
One-year Kaplan-Meier estimates of clinical outcomes after bidirectional EVT incorporating distal puncture for FP-CTO. (A) Freedom from TLR. (B) Limb salvage. (C) Overall survival.
Discussion
In this multicenter retrospective DIPLOMA study of bidirectional EVT with distal puncture for FP-CTO, 2 main findings deserve emphasis. First, wire-crossing success was achieved in 93 of 94 procedures (98.9%), despite the high lesion complexity. Second, although any periprocedural complication occurred in 22 procedures (23.4%) and major complications (CIRSE grade ≥3) occurred in 8 of 94 procedures (8.5%), distal access-site complications occurred in 10.6% and were uniformly graded as CIRSE grade 1, with no adjudicated major distal access-site complication identified. A detailed procedure-level complication list further showed that the major events were primarily non–distal-access complications. One-year clinical outcomes also provide useful context, with freedom from TLR of 82.0%, limb salvage of 97.0%, and overall survival of 85.6%.
Lesion crossing remains the pivotal step in FP-CTO intervention, particularly in long, calcified occlusions or lesions with an ambiguous proximal cap. The SAFARI technique established the concept of connecting antegrade and retrograde channels to achieve recanalization when antegrade re-entry fails. 4 Subsequently, retrograde approaches have been adopted increasingly, and systematic reviews have shown good technical success with relatively low complication rates, supporting the role of retrograde access as a bailout strategy and, in selected cases, as a primary access strategy.5,6 In this context, the high wire-crossing success rate observed in the DIPLOMA study suggests that distal puncture may serve as a useful adjunctive or bailout option in anatomically complex FP-CTO lesions. Compared with the high wire-crossing success rate, technical failure in this cohort was more often attributable to an inability to achieve an adequate final lumen following successful crossing. All 14 technical failures were attributable to residual stenosis >30% following successful crossing. Most occurred in anatomically complex lesions, with 13 of 14 involving TASC II C/D lesions and 12 of 14 treated without scaffolding. These findings suggest that lesion complexity, rather than failure of the distal puncture-assisted crossing strategy itself, contributed to the discrepancy between wire-crossing success and technical success.
A key contribution of the present study is the standardized assessment of access-site safety using the CIRSE classification system. 7 Beyond reporting overall event rates, this study provides a procedure-level description of complications, clarifying that major events were predominantly non–distal-access complications. Previous reports on distal access have varied widely in how complications were defined and graded, such that event rates alone may not accurately reflect their true clinical impact. By linking complications to the required treatment and their sequelae, the CIRSE classification enables more meaningful comparisons across cohorts and techniques. 7 From this perspective, distal access-site events in the DIPLOMA study were not rare; however, all adjudicated distal access-site complications were minor. These findings should nonetheless be interpreted within the context of the retrospective adjudication framework. The timing of first recognition of distal embolization was not systematically recorded, and embolic events were generally identified on completion angiography. In the present cohort, all 6 distal embolization events occurred in procedures in which thrombin was used for distal hemostasis. However, as the timing of first recognition of embolization was not systematically recorded and embolic events were generally identified on completion angiography, these findings reflect an association rather than evidence of causality. Therefore, although distal embolization was categorized as a target lesion- and device-related complication in this study, a contributory role of distal hemostatic maneuvers, including thrombin injection or balloon-assisted hemostasis, cannot be entirely excluded. These findings are consistent with the broader evidence indicating that retrograde access can be performed with acceptable safety in experienced hands. A systematic review and meta-analysis in patients with critical limb ischemia reported high technical success and low rates of serious access-related complications associated with retrograde arterial access. 6 Similarly, a cohort study evaluating tibiopedal and distal femoral retrograde access reported rare access-related complications and favorable technical outcomes. 11 In popliteal-based strategies, anterolateral retrograde puncture of the distal popliteal artery or tibioperoneal trunk has been described as a useful and safe bailout technique for FP-CTO after failed antegrade attempts, 12 and dedicated series have also shown favorable success and safety profiles for a retrograde popliteal approach. 13 In the DIPLOMA study, distal access was obtained predominantly via the distal superficial femoral artery or popliteal artery (90.4%), with infrapopliteal access used in 9.6%; therefore, these safety findings may not be directly generalizable to cohorts with a higher proportion of infrapopliteal access.
Access-site safety should be considered separately from non–access-site complications arising from complex FP-CTO interventions. In the DIPLOMA study, major complications occurred in 8.5% of procedures, and no adjudicated major distal access-site complication was identified. Rather, the major events were classified primarily as target lesion- and device-related complications. At the same time, all distal embolization events occurred in thrombin-treated procedures; however, as the timing of first recognition of embolization was not systematically documented, a causal contribution of distal hemostatic maneuvers to some embolic or thrombotic events cannot be fully excluded.
This distinction is clinically important because it suggests that procedural risk in bidirectional FP-CTO EVT is not determined solely by the retrograde puncture itself. In addition to careful puncture-site management, embolic risk reduction, device selection, and overall procedural planning warrant equal attention.
Contemporary real-world series also support the feasibility of retrograde access14,15 and selected transpedal strategies. 16 At the same time, cross-study comparisons should be made cautiously because patient selection, puncture level, lesion complexity, and complication definitions vary across reports. In the present cohort, distal access was applied to anatomically complex FP-CTO lesions, as characterized by the TASC II and GLASS classifications, and the 1-year freedom from TLR rate of 82.0% provides clinically relevant context for interpreting the procedural results.
This study has several limitations. Because of the retrospective design, the favorable outcomes observed with distal puncture should not be interpreted as evidence of a causal relationship. Furthermore, the absence of a comparator group precludes direct comparison with antegrade-only strategies. In addition, the modest sample size limits the precision of event-specific estimates and the generalizability of these findings. The timing of distal puncture, whether employed as a primary strategy or as a salvage approach, was left to the operator’s discretion, which may have introduced selection bias and limited generalizability across centers with different levels of expertise. The relatively small proportion of infrapopliteal access limits detailed conclusions regarding safety according to puncture level. Complications were identified from site-reported clinical records without central adjudication; therefore, ascertainment may have varied across centers, and minor events may have been underreported. In addition, the timing of first recognition of distal embolization relative to guidewire crossing, lesion treatment, and distal hemostatic maneuvers was not systematically documented; therefore, the causal contribution of thrombin injection or balloon-assisted hemostasis to some embolic or thrombotic events could not be determined. Finally, heterogeneous follow-up duration and the use of outcome-specific analysis units limit comparability with studies employing uniform patient-level endpoints. In addition, because the registry included only procedures in which distal puncture was successfully established, failed puncture attempts were not captured, and the technical success rate of distal puncture itself could not be assessed. For the same reason, the proportion of all FP-CTO procedures in which distal access was required to achieve crossing could not be determined.
Conclusion
In this selected cohort of anatomically complex FP-CTO lesions, bidirectional EVT incorporating distal puncture was associated with a high wire-crossing success rate. No adjudicated major distal access-site complication was identified using the CIRSE classification; however, these findings should be interpreted with caution given the retrospective design, the exclusion of failed distal puncture attempts, and the limited ability to establish the temporal attribution of distal embolization. Prospective studies with standardized procedural documentation are warranted to better define the indications and safety profile of distal puncture.
Footnotes
Acknowledgements
ChatGPT (OpenAI) was used to assist with improving manuscript readability, grammar, and the preparation of preliminary drafts of figure and table captions. All AI-assisted content was reviewed and edited by the authors, who take full responsibility for the accuracy and integrity of the final manuscript. No AI-generated or unverifiable references were included. The authors would also like to thank Editage (![]() ) for their assistance in editing and reviewing the English language of this manuscript.
) for their assistance in editing and reviewing the English language of this manuscript.
Ethical Considerations
This study was approved by the Joint Ethics Review Committee of the Tokushukai Group (approval no. TGE02061-012). It was conducted in accordance with the Declaration of Helsinki and the Ethical Guidelines for Medical and Health Research Involving Human Subjects issued by the Japanese Ministry of Health, Labour, and Welfare. As the study was retrospective and used anonymized data without human biological materials, the ethics committee granted a waiver of written informed consent.
Consent to Participate
In place of written informed consent, study information, including an opt-out option, was made publicly available on the websites of the participating hospitals. This allowed patients or their proxies to decline participation.
Consent for Publication
Not applicable. This study does not include any individual details, images, or videos that could identify a specific person.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.