
Abstract
Introduction:
Understanding living organ donors’ experience with donation and challenges faced during the process is necessary to guide the development of effective strategies to maximize donor benefit and increase the number of living donors.
Methods:
An anonymous self-administered survey, specifically designed for this population based on key informant interviews, was mailed to 426 individuals who donated a kidney or liver at our institution. Quantitative and qualitative methods including open and axial coding were used to analyze donor responses.
Findings:
Of the 141 survey respondents, 94% would encourage others to become donors; however, nearly half (44%) thought the donation process could be improved and offered numerous suggestions. Five major themes arose: (1) desire for greater convenience in testing and scheduling; (2) involvement of previous donors throughout the process; (3) education and promotion of donation through social media; (4) unanticipated difficulties, specifically pain; and (5) financial concerns.
Discussion:
Donor feedback has been translated into performance improvements at our hospital, many of which are applicable to other institutions. Population-specific survey development helps to identify vital patient concerns and provides valuable feedback to enhance the delivery of care.
Introduction
The demand for transplantation has been increasing due to the mounting disparity between the incidence of end-stage organ failure and the number of available organs. 1 According to the Organ Procurement and Transplantation Network (OPTN), there are 99 381 patients on the waiting list for kidney transplants and 14 679 for liver transplants in the United States. 2 During 2015, 25 005 kidney and liver transplants were performed, and nearly 12 000 candidates were removed from the waiting list due to death or being too sick to transplant. 2 Although decreasing in recent years, living donors present a viable option to supplement the supply of deceased donor organs.
Organ donation from healthy persons appears to challenge the medical tenet of “first do no harm”; however, medical ethicists justify this risk based on positive psychological effects to the donor from providing a direct benefit to the organ recipient or satisfaction derived from the attempt to provide life-saving treatment to the recipient. 3 It is therefore incumbent upon the transplant community to verify that these benefits are achieved, and the donor experience is continually improved. Previous studies have shown that living organ donors have favorable quality of life as well as positive physical and mental health after organ donation. 4,5 Few studies have sought donor’s input on improving the process in addition to assessing their experience, both of which are necessary to develop effective strategies to increase the number of living organ donors.
The primary objective of our study was to assess kidney and liver donors’ experience with donation and identify challenges faced during the process. Our secondary objective was to identify strategies, from donors’ perspective, and to improve the organ donation experience. The information we garner from this survey as to why people donate and how they view their experience will help drive programmatic improvement and inform new strategies to increase living donation rates.
Methods/Approach
Setting, Sampling, and Information Collection
Our Division of Solid Organ Transplantation maintains a list of past living donors for routine medical and psychosocial follow-up. An information letter describing the purpose, risks, and benefits of the study, the survey, and a self-addressed stamped envelope was mailed in July 2013 to all who donated a kidney or liver to our institution between 2000 and 2013. Participants were instructed not to write any identifying information on the survey. A reminder letter was sent to all donors 3 weeks after the initial mailing to encourage return of the survey. The survey was in English, and there was no monetary incentive for completion.
Survey Design
A self-administered survey was specifically designed for this study. Survey items and sections were developed based on a review of the literature as well as individual qualitative interviews with 6 key informants. Key informants included subject area experts, living organ donors, and potential donors. The survey was iteratively revised through 10 rounds of pretesting and being reviewed a total of 31 times: 7 times by subject area experts, including transplants surgeons, coordinators, and social workers; 20 times by the general population; and 4 times by transplant patients. After survey finalization, a pilot test was conducted with organ donors to assess feasibility of survey administration.
The survey was divided into 5 sections. The first section asked donors for basic demographic information, and the second included items about motivation for donation, the preoperative process, and concerns prior to surgery. The third section asked about their perioperative experience, including quality of life, pain, and length of stay. The fourth section included a series of statements related to experience with donation; on a 1- to 5-point Likert-type scale (1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, and 5 = strongly agree); these items showed acceptable internal consistency, with a Cronbach α of .63 (data not shown). The last section asked participants to indicate how helpful they found several resources and individuals during the donation process; participants were given the option to indicate that they did not use or see the particular resource or person. Additionally, open-ended questions regarding specific challenges faced prior to surgery, suggestions for improving the process, and ideas to increase public awareness about living organ donation were included. This study was approved by the University of Rochester’s Research Subjects Review Board and qualified for a waiver of documentation of informed consent.
Analysis
Descriptive statistics were calculated to characterize responses for all survey items. Due to low frequencies for some response categories and to facilitate interpretation, the 5 Likert categories used to assess experience were collapsed into 3: (1) “disagree,” defined as a 1 (strongly disagree) or 2 (disagree) on the Likert-type scale, (2) “neutral,” defined as a 3 (neutral) on the Likert-type scale, and (3) “agree,” defined as a 4 (agree) or 5 (strongly agree) on the Likert-type scale. Similarly, the responses to helpfulness of resources and individuals were collapsed into helpful (2 and 3) and not helpful (1). Statistical analyses were performed using SAS 9.3 (SAS Institute, Inc, Cary, North Carolina).
Responses to open-ended questions were analyzed using qualitative methods. Two members of the study team engaged in open, then axial coding of responses. During open coding, initial codes were developed that defined, labeled, and promoted inclusivity of data. After establishing a broad framework for data analysis, axial coding, a structured process to associate self-reported constructs, led to developing more specific major and minor themes. Discrepancies were resolved through a consensus discussion.
Results
Sociodemographic Characteristics
Surveys were mailed to 426 donors (42% liver donors; 58% kidney donors), and 141 surveys were returned (33.1% response rate); 78% of the study sample were kidney donors and 22% were liver donors. Mean age of the study sample, at the time of survey completion, was 51 (standard deviation 9) years (Table 1). The donors were predominantly female (69.5%), white (96.5%), not Hispanic (94.3%), and married (71.6%). Donors in our sample were highly educated, with 29.1% of donors having completed a master’s or doctoral degree. The most frequent donor–recipient relationship was siblings (23.4%). Respondents donated a mean of 5 ± 3.9 years prior to survey administration.
Donor Characteristics.a
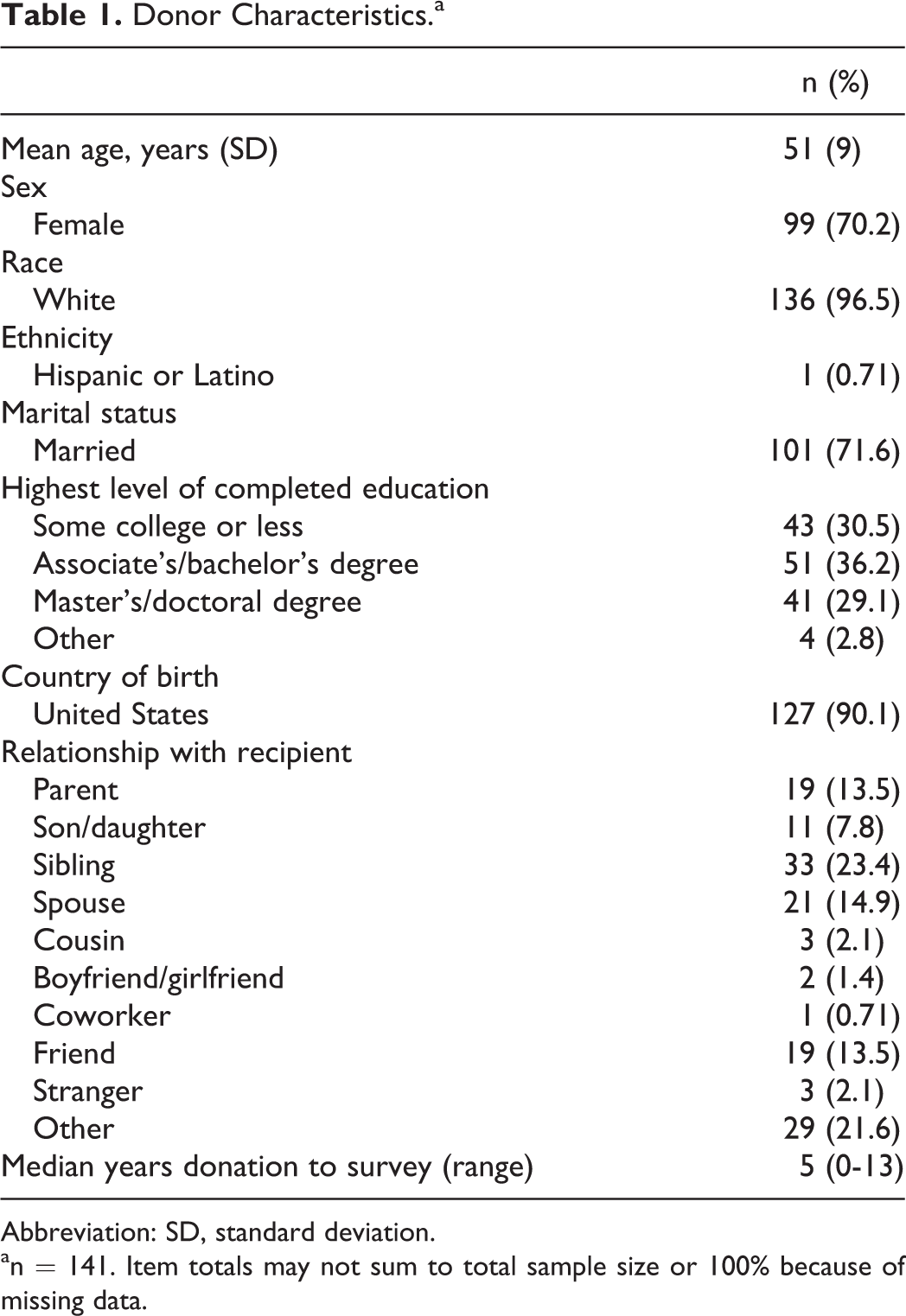
Abbreviation: SD, standard deviation.
an = 141. Item totals may not sum to total sample size or 100% because of missing data.
Predonation Process
Most donors (42.6%) reported that the predonation process took more than 6 months and 48.6% reported 4 to 5 visits prior to surgery (Table 2). Three-quarters (75.7%) of donors reported that they preferred to go to the clinic or hospital as frequently as they did. Almost all donors (89.4%) did not feel obligated to donate, while 27.7% endorsed that they were discouraged to donate. Donors discussed their decision with family (90.8%), friends (62.4%), and coworkers (41.1%). Notable concerns prior to surgery include health/survival of recipient (61.7%), surgical complications (38.3%), pain (29.8%), time off work (28.4%), and inability to donate to their recipient (28.4%).
Preoperative and Postoperative Processa
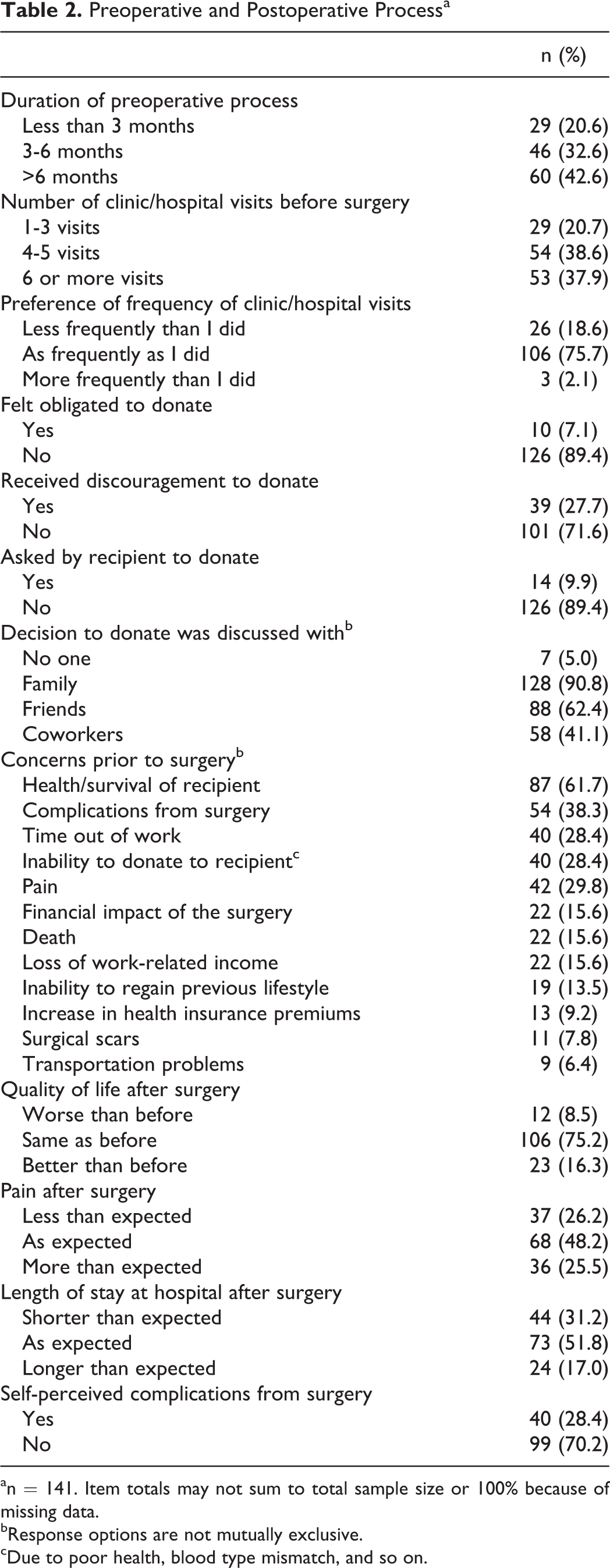
an = 141. Item totals may not sum to total sample size or 100% because of missing data.
bResponse options are not mutually exclusive.
cDue to poor health, blood type mismatch, and so on.
Experience With Donation
Overall, donors appear to have a positive donation experience. The vast majority of donors felt well after their donation (94.3%), and 87.9% agreed that the decision to donate was easy for them. Almost all (97.9%) disagreed that they were pressured by others to donate, 84.4% agreed that they would donate again, and only 2.1% regretted their decision to donate. Furthermore, 94.3% of donors agreed that they would encourage others to become donors.
Helpfulness of Resources and Individuals
Donors reported on their perceived helpfulness of resources and individuals throughout the donation process. Overall, informational brochures were reported to be helpful by 70.2% of donors. Nearly half (46.1%) of the donors reported that they did not communicate with other donors; however, of those who did, 48.9% found communication with other donors to be helpful. Internet searches/websites were deemed moderately helpful (65.2%). The majority (78.0%) of donors did not use social media as a resource during their donation process. Discussion with health-care providers was reported to be helpful by 75.9% of donors. When questioned about specific providers, transplant surgeons, coordinators, and social workers were reported to be most helpful by 92.9%, 92.2%, and 79.4% of donors, respectively.
Postdonation Experience
Quality of life after was reported to be the same as prior to surgery in 75.2% of donors and 16.3% reported it to be better than before (Table 2). Almost half (48.2%) of donors reported that their pain level after surgery was as expected, and 25.5% reported it to be more than expected. Most donors (70.2%) did not report any self-perceived complications from surgery and length of stay was as expected in 51.8%.
Open-Ended Questions
A summary of the themes from qualitative analysis is presented in Table 3 and subsequently.
Themes, Selected Subthemes, and Example Quotes From Open-Ended Survey Items.
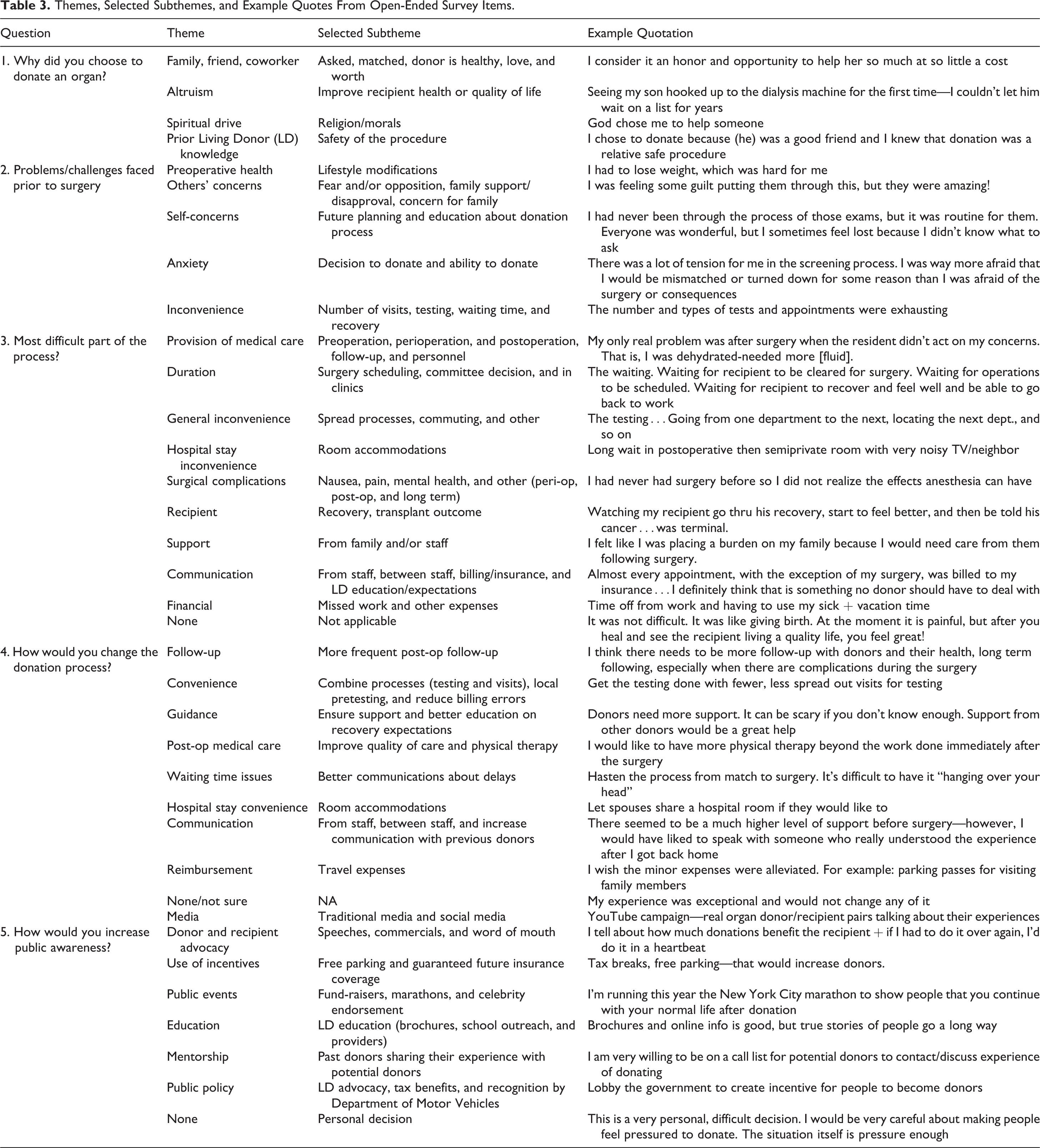
Donation reasons
Relationship with the recipient, altruism or desire to improve the health and quality of life of the recipient, spiritual drive, and prior knowledge of the benefits and safety of living donation were all cited as reasons respondents chose to donate an organ.
Problems/challenges faced prior to surgery
Lifestyle modifications (eg, weight loss and smoking cessation), concerns of and about others including family or friends’ disapproval of the donation decision, stresses related to future planning and predonation education, anxiety over committee decision and ability to donate, and inconveniences encountered in the testing and scheduling process were identified as the major challenges donors faced in the predonation period.
Most difficult part of the process
Varied themes were recognized as the most difficult issues donors confronted including inconveniences (inpatient accommodations, testing, and scheduling delays), surgical complications, communication with and between health-care professionals, provision of medical care throughout the process—inclusive of long-term follow-up, lack of familial or health-care team support, financial effects of donation, and recipient outcome. Some identified no difficulties in the process.
Ideas to change the process
Greater convenience, more frequent follow-up, better communication, assistance with and guidance on recovery expectations, as well as reimbursement for donation-related expenses were all suggested by donors as ways to improve the process.
Strategies to increase awareness
Major themes included the use of media (social and traditional), hosting or partaking in public events, granting incentives, as well as changes to policy. Many donors stated they were willing to be involved in the effort, whereas a few donors believed the decision to donate was a personal one, and awareness of living donation should not be increased.
Discussion
We surveyed a sample of our institution’s liver and kidney donors from the past decade to identify donor-suggested strategies to improve the organ donation process and to increase public awareness about living organ donation. Donor follow-up has been an increasing concern of the transplant community as demonstrated through recently adopted OPTN policy calling for meaningful and complete follow-up information to be submitted to the United Network for Organ Sharing. 6
Consistent with previous studies, 4 –7 most donors reported that they would donate again, and the vast majority were able to regain or improve upon their predonation quality of life. Almost all donors in our study would encourage others to become organ donors; yet, nearly half (44.0%) of our sample agreed that the organ donation process could be improved. Suggestions for process improvement were evaluated in discrete and open-ended questioning.
A theme that emerged from qualitative analysis was that the preoperative process is too lengthy. When assessed quantitatively, 42.6% of donors reported that the preoperative process took greater than 6 months; interestingly, 75.7% of donors also reported that they would have preferred to visit the clinic and hospital as frequently as they did. The preoperative process at our institution is intentionally comprehensive to ensure that donors are making an informed decision and that they are medically and psychologically cleared to donate. Nevertheless, this is a valid concern voiced by donors, and we have begun reexamining processes in order to expedite the time from evaluation to donation without compromising patient safety. As a result, this metric is tracked and regularly reported on our living donor quality assurance and performance improvement dashboard.
Donors voiced frustration with the numerous office and laboratory visits that were spread out across several days or weeks as well as occurring at different locations around the hospital. Previously, donors were scheduled to undergo 1 evaluation test at a time, moving to the next if they met criteria. This process has been condensed throughout the years, although all donors included in the study were required to travel to our center for at least 2 days of appointments. The donor-suggested intervention of scheduling several appointments in 1 day, such that they can complete several office visits in a single trip, is a quality project in progress. Additionally, to help facilitate the evaluation, our Independent Living Donor Advocate now works as an appointment navigator, guiding donors to testing locations around the hospital.
Donors endorsed various apprehensions prior to surgery including the recipient’s health, impact on caregiving responsibilities, complications, time out of work, and pain. These concerns echoed those previously reported. 8 –10 Although donors faced preoperative trepidations, only 3.5% of respondents believed they did not receive adequate information before deciding to donate; still, there may be room for additional counseling as elicited in the open-ended answers. Consistent with the study by Agerskov et al, 11 health-care professionals, including transplant surgeons, coordinators, and social workers, were reported to be very helpful during the donation process; these individuals should therefore ensure that they are easily accessible to address donor’s questions and alleviate concerns. An additional resource that our sample found to be exceedingly valuable, although not universally accessed, was previous donors. In response, our program is working to increase the presence and engagement of former donors in the preoperative education process. Using previous donors as public ambassadors and advocates for living donation was also frequently suggested as a potentially effective strategy to increase organ donation.
Most donors (78.0%) reported that they did not use social media during their donation process, but a notable proportion suggested using social media to increase awareness of living organ donation in their open-ended responses. Because our study sample included patients who donated an organ at our institution within the past decade, it is plausible that many did not use social media because its popularity has only begun to rise in the past few years. To date, most studies have focused on improving the public’s knowledge of deceased organ donation and increasing registration rates via interactive online platforms. 12 The use of social media to recruit living donors has also begun to be documented in the literature. 13 Therefore, the use of social media may be a promising platform to increase awareness and donation rates.
A quarter of donors (26% kidney and 23% liver) reported that their pain after surgery was more than anticipated and one of the most difficult aspects of the donation process. Laparoscopic kidney donation became routine at our institution in 2005, and while it is likely that this reduced the overall pain experienced by our donors, our survey assessed donor expectations. Greater than expected postoperative pain was reported by participants, suggesting education and pain management as areas for improvement. Donors who have had no previous surgeries or have a low pain threshold may benefit from epidural analgesia to mitigate postdonation discomfort; consequently, we routinely consent all of our donors for epidural analgesia in case they are converted to open nephrectomy.
Financial themes were raised throughout the survey including donor’s concerns prior to surgery (financial impact, loss of work-related income, and increase in health insurance premiums), ideas for improvement (reimbursement), and ways to raise awareness (incentives). Out-of-pocket donor costs have been estimated to average US$2231 to US$6141 in inflation-adjusted US Dollars and primarily result from travel/lodging expenses and missed work. 14 –16 Additionally, racial and ethnic minorities, a chronically underrepresented donor group, have identified financial pressures as a major barrier to their willingness to donate. 15,17 International guidelines support comprehensive recompense of donor’s documented expenses, although unlike a portion of our surveyed donors and recent national polls, these guidelines do not favor financially incentivizing living donation. 18 –21
Compared to the national donor population, our study sample comprised more females, had a greater proportion of non-Hispanic white individuals, greater proportion of married donors, and higher level of educational attainment. A recent analysis of kidney donors by Schold et al reported that women are more compliant with postdonation follow-up as are those who are older, married, and more educated which could translate to a higher survey response rate 22 ; white race and older age have also been found to be correlated with closer follow-up in the liver donor population. 23 Still, despite a higher prevalence of end-stage renal disease, minorities are persistently underrepresented as donors and living donor recipients—as are lower income individuals. A recent consensus conference 24 suggested areas for intervention to address the multifactorial roots of this disparity; among these are removing financial disincentives (discussed earlier) and increasing collaborative research on ways to break down the barriers to transplant or donation. Surveys on prior living donors, such as ours and of others, can help to achieve this second aim by elucidating culturally specific concerns and ideas for improvement in the donation process which could translate into interventions to increase access for minority donors. Due to low response and follow-up rates seen in the target demographic, a concerted effort to seek input from underrepresented groups would be warranted.
There are several limitations of this study. First, we were unable to compare characteristics of donors who did not return the survey to respondents, due to the anonymous nature of the surveys. This presents a potential sampling bias, as the experience of nonresponders may be different. Second, changes to the donation process over the study period, including those highlighted earlier, may have affected responses. Major concerns were ubiquitous and did not seem to be related to time of donation. Going forward, we plan to administer comprehensive surveys earlier to generate more timely feedback. Our center’s results may not be generalizable to other institutions due to (1) differences in practice, (2) nonnationally representative sample, and (3) the response rate of 33%, although this is comparable to the response rate of other nonincentivized mailed national health-care satisfaction surveys.
This study addresses the vital concerns of donors and provides valuable feedback to both enhance living donor processes and to help increase organ donation rates. While translated into specific performance improvements at our institution, many of the suggestions are applicable to other centers or even national campaigns. Future research should assess whether implementing donor suggested strategies will translate into a more positive donor experience and ultimately increases in the number of living organ donors.
Footnotes
Acknowledgment
The authors would like to thank the living donors who made this study possible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.