
Abstract
Purpose:
Psychosocial assessment of patients comprises an important element in the selection process of appropriate candidates for left ventricular assist device (LVAD) implantation. We sought to determine the association of the well-validated psychosocial assessment of candidates for transplantation (PACT) scale to clinical outcomes post-LVAD implantation.
Materials and Methods:
The PACT scale was used retrospectively to reconstruct psychosocial profiles of all patients who underwent a continuous-flow LVAD implantation for all indications at our institution between March 2008 and August 2012 (N = 230). Psychosocial elements including social support, psychological health, lifestyle factors, comprehension of the operation, and follow-up were evaluated. The primary outcome was overall survival, and the secondary outcomes were hospital readmission, pump thrombosis, hemolysis, gastrointestinal (GI) bleeding, and LVAD driveline infections.
Results:
The mean age of patients was 55.3 years, with 83% being male; 58% (N = 135) were bridge to transplant and 42% (N = 95) were destination therapy. Up to 1-year post-LVAD implant, there were no statistical differences among the 5 PACT candidate groups in terms of survival (P = .79), hospital readmissions (P = .55), suspected or confirmed pump thrombosis (P = .31), hemolysis (P = .43), GI bleeding (P = .71), or driveline infections (P = .06).
Conclusions:
In this single-center retrospective review, post hoc reconstruction of psychosocial profiles using the PACT scale and independent assessment of postimplant outcomes, including survival and adverse events, did not show any association. However, given the small number of patients in the low score PACT groups as well as limited duration of follow-up, further studies are required to elucidate the association.
Introduction
Poor psychosocial factors derived from formal psychosocial evaluation are known to be related to higher morbidity and mortality in heart transplant recipients. 1 However, the role of psychosocial evaluation in patients receiving continuous-flow left ventricular assist devices (LVADs) has been less well established. There have been studies assessing the psychosocial burden overall following LVAD implantation, but there are very limited data on the influence of preimplant psychosocial status on outcomes postimplant. 2 –6
Previously published guidelines recommend that patients being evaluated for mechanical circulatory support undergo formal psychological and social evaluation. 7,8 Patients with poor psychosocial factors may have limited ability to cope with, operate, and respond to alarms on the device in a timely manner. It is often a challenge for them to integrate the lifestyle changes and understand the importance of adherence with anticoagulant medications, follow-up appointments, as well as the risks of bleeding and thrombosis associated with this electromechanical circulatory support device. Patients with active psychiatric conditions and inability to manage the device do not qualify for mechanical circulatory support. Among those who do qualify, we see a spectrum ranging from low to high yet acceptable risk depending on the rating scale used.
The Psychosocial Assessment of Candidates for Transplantation (PACT) rating scale, first published by Olbrisch et al in 1989, has been in widely used and studied as part of pretransplant psychosocial assessment. 3 It was developed in an attempt to increase the consistency of psychological and social evaluation across raters. The PACT has been consistent for interrater reliability and clinically applied for psychosocial assessment of candidates being screened for organ transplant.
Study Hypothesis
With newer continuous-flow LVADs and an increasing number of patients now being considered for destination therapy, the role of psychosocial factors and clinical outcomes of such patients must be assessed. We tested the hypothesis that preimplant PACT scores are associated with various morbidity and mortality outcomes among patients who undergo LVAD implantation.
Methods
After obtaining the approval of the institutional review board, a descriptive comparative design was used. Data were collected by a retrospective chart review on consecutive patients who underwent a continuous-flow LVAD implant at our institution between March 2008 and August 2012 (N = 230). Inclusion criteria were patients who underwent a continuous-flow LVAD during that time period. Those who underwent a right VAD implantation were excluded from the study.
All patients had undergone screening evaluations by social workers at our institution, but the PACT was not used to assess candidacy. Each candidate was assessed for support network, mental health, treatment adherence, substance abuse history, and comprehension of the illness. After appropriate clearance and psychiatric interventions whenever deemed necessary, these patients underwent a Heartmate 2 implant for the respective indication. An independent rater trained to use the PACT and retrospectively scored patients using the narrative analysis of the collected psychosocial profiles. This was done by extensive chart review of documented psychosocial profiles accounting for multiple evaluations when applicable. This was done in a blinded manner to patient outcomes in an attempt to minimize bias.
Preimplant PACT Score Risk Groups
The PACT questionnaire is a 10-item rating scale encompassing the aspects of social support, psychological health, lifestyle factors, and understanding of transplant and follow-up. Each factor was subjectively rated on a scale of 1 to 5, and the final rating qualifies candidates from the spectrum of poor to excellent (0-4). This scale has been shown to have high overall interrater reliability (correlation 0.85). 3 In our study, social support (2 items), psychological health (2 items), lifestyle factors (3 items), and comprehension of the operation and follow-up (1 item) were rated. A final rating (1 item) of candidate quality for LVAD therapy was scaled from 0 to 4 (0 = poor with contraindication to surgery, 1 = borderline acceptable under some conditions, 2 = acceptable with some reservations, 3 = good, and 4 = excellent). These 5 final ratings were used to categorize patients into PACT score risk groups.
Outcomes
Once the psychosocial evaluation ratings were complete, and outcomes were independently collected by retrospective chart review. The primary study outcome was overall survival. Mortality was collected within the first year and patients alive 1-year post-LVAD were right censored in the analysis. Various secondary outcomes were collected, including all-cause readmissions, pump thrombosis, hemolysis, gastrointestinal (GI) bleed, and infections. These morbidity outcomes were recorded as present if indicated in the chart between LVAD placement and 1-year postimplant. Pump thrombosis and hemolysis were present if serum lactate dehydrogenase criteria >2000 IU/L was found. Only GI bleeds confirmed by upper endoscopy or colonoscopy were included; occult GI bleeds were not included in our study. Infections, specifically device driveline infections, were recorded. The number of patients having received a heart transplant by the time this retrospective study was conducted were also documented.
Statistical Analyses
Baseline demographics are summarized with appropriate descriptive statistics, either mean (standard deviation) or percentage. Survival within 1 year postimplant was compared among the PACT score risk groups (poor, borderline, acceptable, good, and excellent) using Kaplan-Meier curves and tested with a log-rank test. The distributions of PACT score risk groups were compared among outcome groups with Fisher exact tests. A composite outcome was created for patients experiencing any event (primary or secondary outcome). The distributions of PACT score risk groups were compared to the composite outcome groups with a Fisher exact test with P values ≤.05 considered statistically significant. All statistical analyses were conducted with SAS v9.3 software (SAS Institute, Cary, North Carolina).
Results
All patients who underwent LVAD during study period were included (N = 230). Patient characteristics are presented in Table 1. The majority of patients were bridge to transplant (n = 135), with a sizable number being destination therapy (n = 95). Most patients were rated as acceptable, good, or excellent candidates according to their PACT scores risk groups. Six patients were considered poor or borderline candidates, all had relatively emergent LVAD implants.
Baseline Demographics of Study Participants.
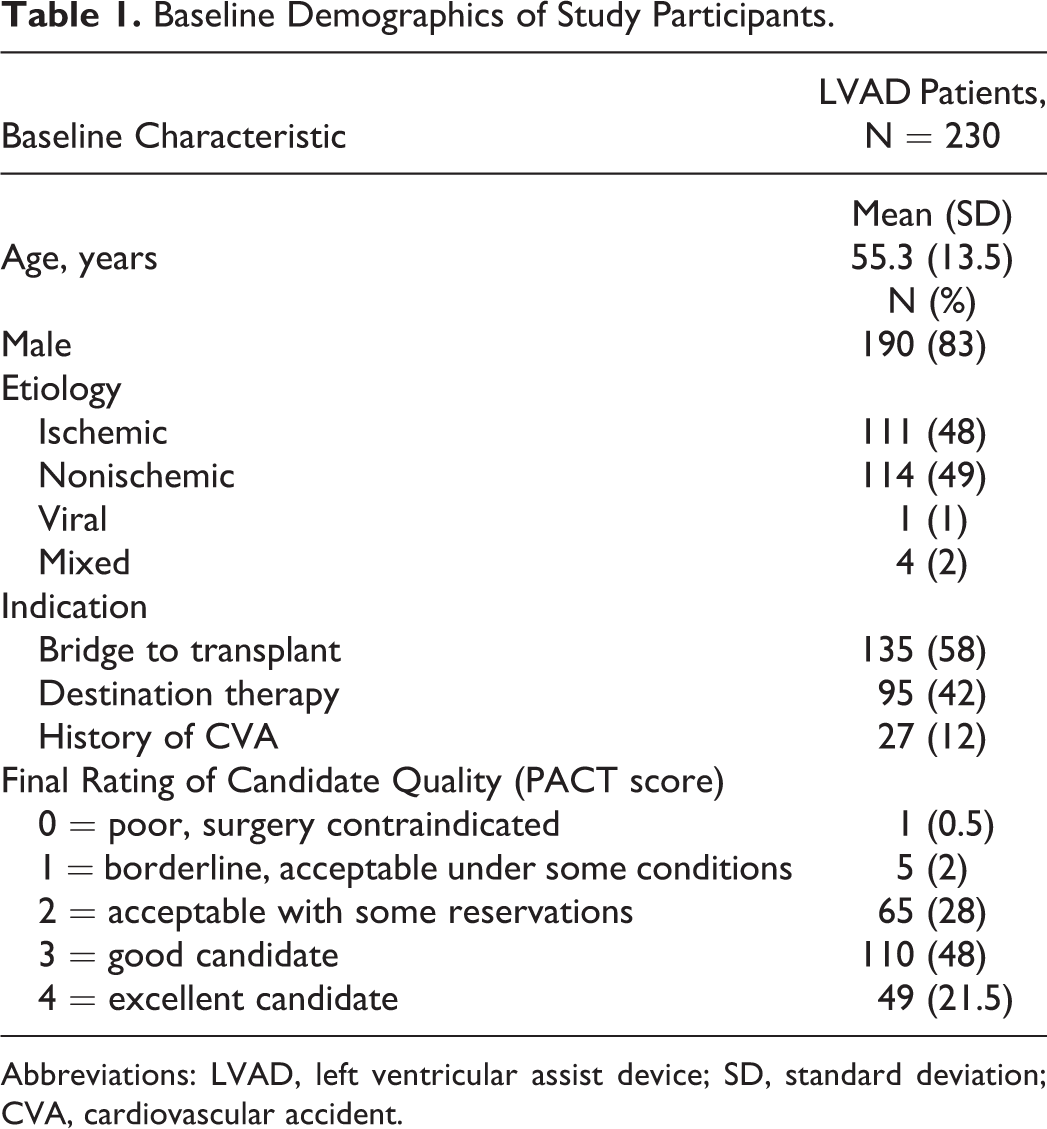
Abbreviations: LVAD, left ventricular assist device; SD, standard deviation; CVA, cardiovascular accident.
Survival According to Preimplant PACT Score Risk Groups
The data failed to indicate a survival difference among the PACT score risk groups (Figure 1; P = .79). Visually, the lowest PACT score risk groups appear to have the best survival; however, only 6 patients comprised PACT score risk groups 0 and 1 combined and therefore should not be used for inferential purposes. When the analysis was repeated including only the 224 patients from PACT score risk groups 2, 3, and 4, there remained no indication of a survival difference among the PACT score risk groups (P = .98).

Overall survival by final PACT score risk groups. PACT indicates psychosocial assessment of candidates for transplantation.
Morbidity According to Retrospectively Collected Preimplant PACT Score Risk Groups
The distributions of PACT score risk groups were compared among groups classified according to the presence or absence of secondary outcomes (Figure 2; Table 2). Up to 1-year post-LVAD implant, there were no statistical differences among the 5 PACT score risk groups for the secondary outcomes. The largest differences were observed among the groups that did or did not experience driveline infection and any infection, although this difference was statistically non significant. Similarly, no difference was observed when comparing the PACT score risk groups with the composite outcome (P = .71). The proportion of patients experiencing at least 1 event was 100% (n = 1), 100% (n = 5), 88% (n = 57), 87% (n = 96), and 82% (n = 40) for the PACT score risk groups 0, 1, 2, 3, and 4, respectively.
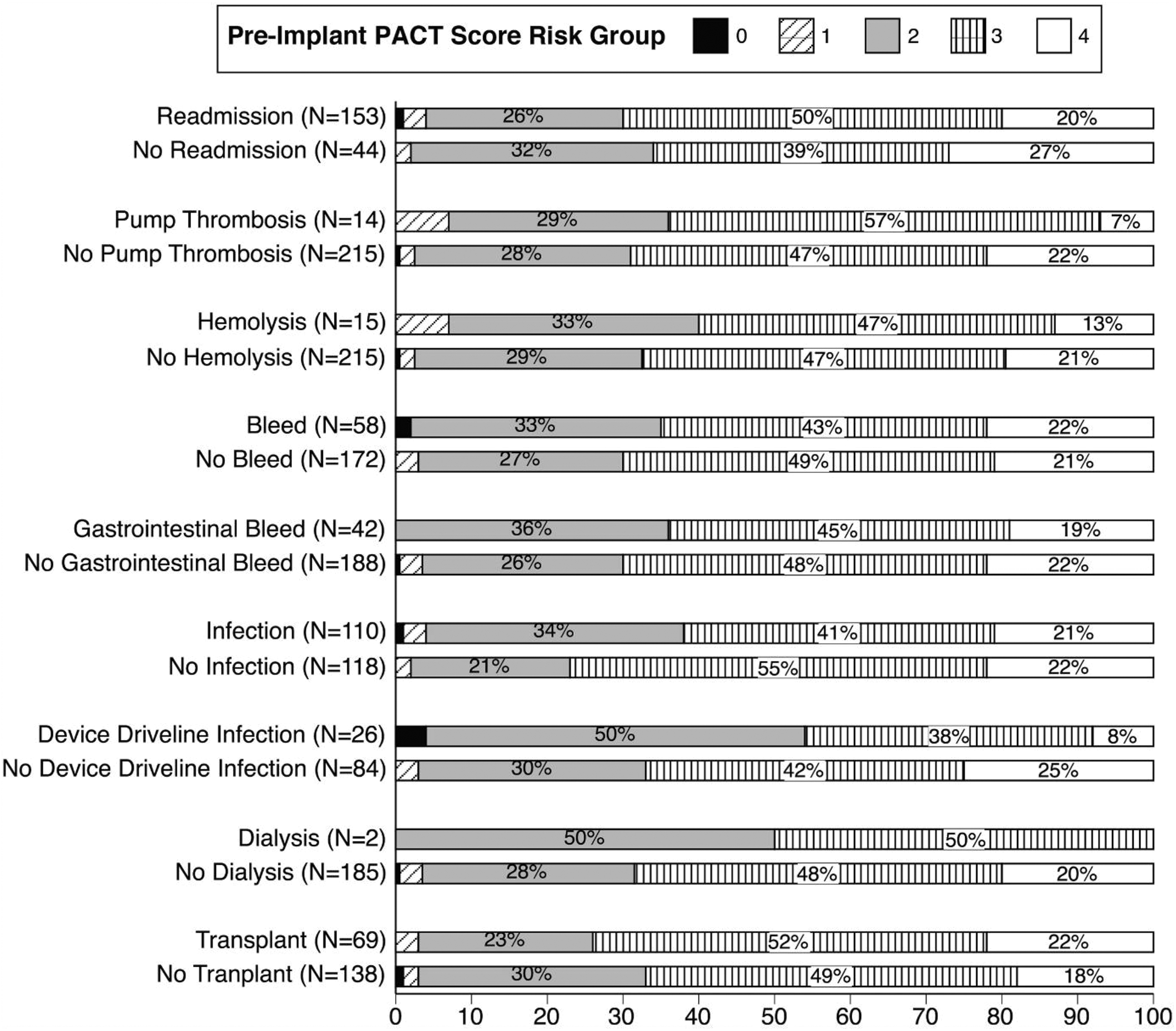
Morbidity outcomes by PACT score risk groups. PACT indicates psychosocial assessment of candidates for transplantation.
Morbidity Outcomes in Risk Groups by Final PACT Score Risk Groups.
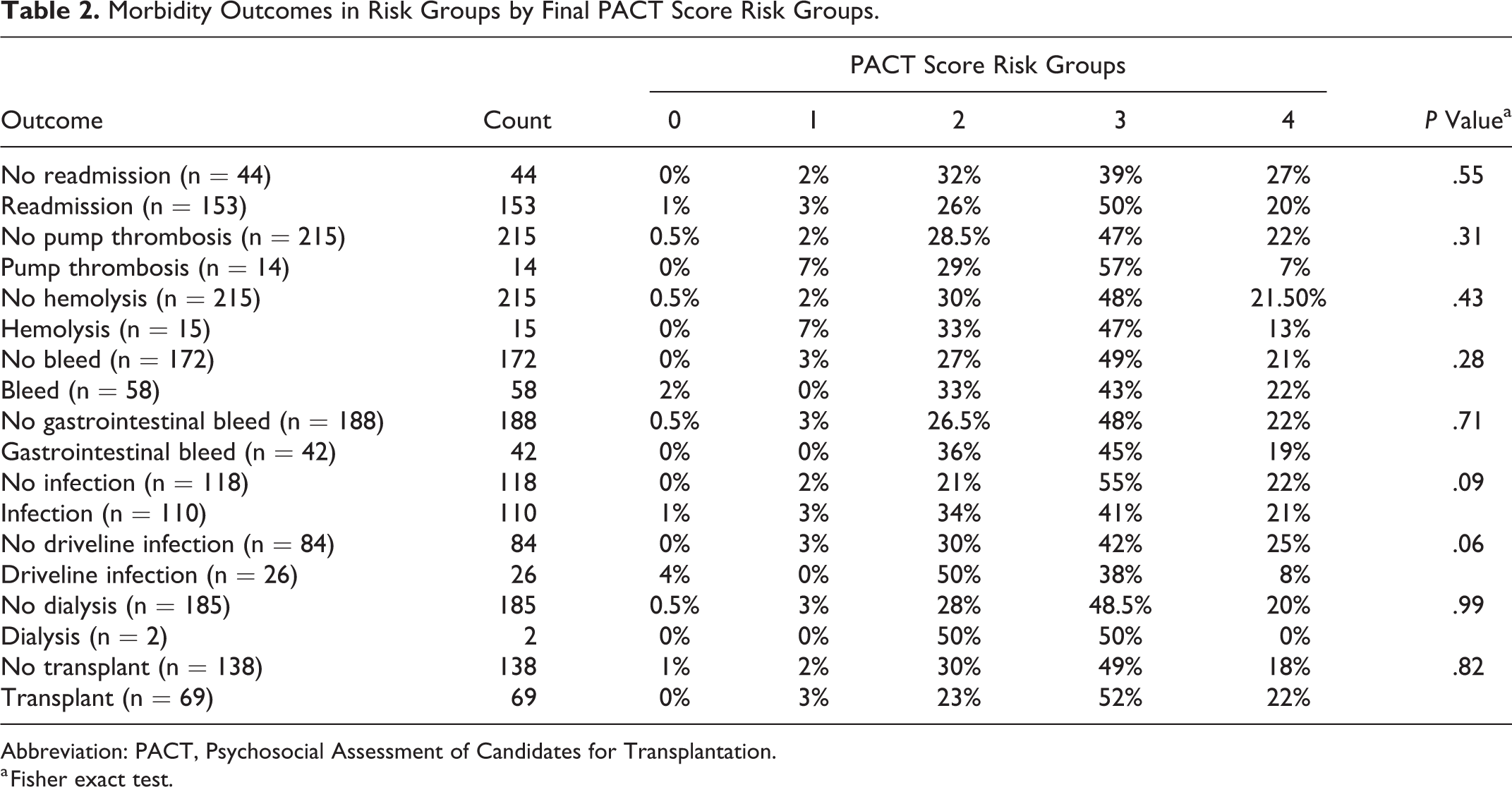
Abbreviation: PACT, Psychosocial Assessment of Candidates for Transplantation.
a Fisher exact test.
Transplant status at the time of study was available for 207 (90%) patients and revealed that 69 (33%) patients received a heart transplant while 138 (67%) patients did not, with no significant difference in the final rating of candidate quality assessment among the groups (P = .82).
Among those who received a heart transplant, 3% (n = 2) had a PACT score risk group of 1, and the rest belonged to PACT score risk groups 2, 3, and 4, respectively, with majority (n = 36, 52%) being group 3 (good candidates). A total of 16% (n = 11) of patients who received a heart transplant were initially classified as destination therapy at the time of VAD placement who underwent subsequent listing to get a heart transplant.
Discussion
In this single-center study comprising of 230 patients who underwent a continuous-flow LVAD implantation with preimplant psychosocial evaluations, retrospectively derived PACT score risk groups showed no differences with postimplant outcomes, including survival. As observed, most of the patients belonged to PACT score risk groups 2 and 3, which were acceptable and good candidates, respectively. Patients in groups 0 and 1, although a small number, who underwent device implant on a relatively emergent basis, did do well. As much as these findings are surprisingly suggestive of lack of direct correlation between low PACT score risk groups and poor outcomes, contrary to what one would expect, we need to examine this more in detail.
The PACT shows that the rating form is ultimately subjective with the final rating not being a sum or average of individual factor ratings. There are other scales for psychosocial assessment in assessing transplant candidacy but not as widely used compared to PACT. These include Transplant Evaluation Rating Scale (TERS), Psychosocial Levels System, and the more recently developed Stanford Integrated Psychosocial Assessment for Transplant (SIPAT) scale. The TERS scale was developed after PACT and a study looking at bone marrow transplant recipients compared the 2 scales. 9,10 Both scales were found to have a high interrater reliability; however, TERS was designed to be more objective with 10 items rated on a 3-point scale and the final score being derived mathematically. The PACT, although a subjective rating method, was noted to have high interrater reliability. The SIPAT was only very recently developed and has been shown to be comparable to PACT with having a high interrater reliability as well as providing a more detailed psychosocial assessment profile. 11
The impact of psychosocial profiles on quality of life has been examined following VAD implant in a few studies. The quality of life after implantation of mechanical circulatory support devices has a known association with neuropsychological factors in patient and caregiver burden. 5,12,13 There is limited data regarding impact of preimplant psychosocial profiles on postimplant adverse outcomes in LVAD patients. To date, there is only 1 other study that looked at the predictive value of preimplant psychosocial assessment on postimplant psychosocial success and 30-day readmission rate. This study concluded that although the PACT had a high sensitivity and positive predictive value overall, a substantial number of patients who were classified as high risk did not have poor psychosocial outcomes. Investigators used a modified PACT score that correlated with social success and readmission outcome. 14
Yost et al retrospectively examined the impact of the TERS on postimplant LVAD outcomes in a single-center study. The patients were divided into low-, moderate-, and high-risk groups per the TERS rating scale score prior to LVAD implant. The high-risk group was noted to have significantly shorter mean outpatient days, but there was no significant difference in survival, adverse outcomes, postoperative length of stay, or readmission rate. 15 The association between individual psychosocial factors with all-cause death and readmission has been examined in a cohort of destination therapy LVAD patients with no significant differences noted in deaths. However, illicit drug use and depression had a higher readmission risk. 16 In a systematic review and meta-analysis, depression, functional status, and behavioral functioning were associated with a significantly higher infection and readmissions. 17 Another study was completed in our institution where investigators evaluated the overall frequency of readmissions, associated factors, and the related cost burden after a Heartmate II I LVAD implant. Although management of neuropsychiatric and psychosocial issues was a reason for non–LVAD-associated unplanned readmissions, the impact of preimplant psychosocial assessment on readmissions overall was not examined.
It is interesting to note that even candidates who were not considered good candidates did well for the analyzed outcomes. Although the psychosocial assessment in our study was predominantly used to determine candidacy for LVAD placement, the bridge to transplant group candidates who eventually received a heart transplant did not have a significant difference in their retrospectively collected PACT scores compared to those who did not receive a transplant at 1 year. Among the transplanted patients, the majority did have a PACT score risk group of 2 or higher, although a very small number of patients with a PACT score risk group of 1 did receive a heart transplant.
There are several implications regarding these findings. First, using a simple scoring system applied in a population with advanced heart failure does not necessarily capture all the determinants of postprocedural outcomes as complications can occur independent of psychosocial factors. Second, it is important to recognize that PACT score can be modified to some extent following clinical stabilization with LVAD support, and thus it would be insightful to further examine whether individual components of PACT score (modifiable vs nonmodifiable by LVAD) may differentially influence outcomes.
Study Limitations
Those excluded from LVAD implant due to psychosocial factors were not analyzed. The number of candidates who were deemed poor or borderline by PACT score risk groups (groups 0 and 1, respectively) and underwent an LVAD placement in our study was very limited. Although these 2 groups did well on the outcomes, the small number of candidates limits this conclusion. It would also be beneficial to longitudinally follow outcomes among those candidates who did receive a heart transplant with respect to their PACT score risk groups.
Conclusions
In this single-center retrospective review, post hoc reconstruction of psychosocial profiles using the PACT score and independent assessment of postimplant outcomes, including survival and adverse events, did not show any differences among outcomes measured. Certainly, more studies are needed to help guide decision-making regarding the effect of psychosocial factors on clinical outcomes in patients with mechanical circulatory support. Since the progressive nature of end-stage heart failure can place a psychosocial burden and impact quality of life while learning to cope with the disease, a longitudinal evaluation of a larger population similar to our cohort may provide valuable insight. Thus, it is important to follow clinical outcomes that included quality of life and PACT score risk groups. Also in situations where the LVAD implantation is done more emergently, where a detailed and thorough psychosocial evaluation may not always be possible, it would be important to study the potential impact of mechanical circulatory support on outcomes compared to those patients who do undergo a detailed evaluation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.