
Abstract
Introduction:
Heparin-induced thrombocytopenia (HIT) is characterized by thrombocytopenia and potential for thromboembolism. Lung transplant recipients are at risk of developing HIT due to heparin exposure peritransplant. We describe the incidence and impact of HIT in lung transplant recipient index hospital length of stay and survival.
Design:
A retrospective cohort was obtained from electronic medical records which were queried for all recipients treated with bivalirudin (institutional treatment of choice for HIT) between January 1, 2005, and February 16, 2017 (N = 1171). Patients who developed HIT >30 days after transplant or after their index transplant admission were excluded. A diagnostic algorithm was used retrospectively to determine clinical HIT with an intermediate or high pretest clinical suspicion (“4T” score ≥4) and either (1) positive anti-heparin–platelet-factor 4 (HPF4) assay and a positive functional platelet assay or (2) a positive HPF4 assay only, in patients who did not undergo cardiopulmonary bypass.
Results:
Among all lung transplant recipients, 2.1% were found to develop HIT in the peritransplant period (N = 25, mean = 88%) with a mean lung allocation score of 50.8 and an incidence of venous thromboembolism of 72%, most upper extremity in location. When matched with historical controls, patients with HIT had a longer overall index hospital length of stay of 43 days (P = .008). There was no difference in short- or long-term survival posttransplant.
Conclusion:
Vigilance for the development of HIT in lung transplant recipients is necessary to prevent further morbidity from thromboembolic events. In our cohort, HIT increased hospital length of stay but did not appear to affect recipient survival.
Keywords
Introduction
Heparin derivatives are commonly used in hospitalized patients for therapeutic and prophylactic anticoagulation. Lung transplant recipients may be exposed to heparin due to its use in organ procurement, cardiopulmonary bypass (CPB), and for postoperative venous thromboembolism (VTE) prophylaxis and arrhythmias. Due to a high risk for VTE postoperatively, 1 prophylactic anticoagulation is initiated with unfractionated heparin (UFH) or low-molecular-weight heparins. However, the use of heparin-containing anticoagulants is associated with a risk of bleeding, hyperkalemia, and heparin-induced thrombocytopenia (HIT).
Venous thromboembolism following solid organ transplant occurs in up to 29% of lung, 2% to 14% of renal, and 3% to 5% of liver recipients, respectively. 1 Lung transplant recipients are at increased risk of VTE due to the presence of central venous catheters, hypercoagulability, 2 and decreased immediate postoperative mobility. The discovery of thrombosis should also prompt consideration for HIT, as this may be the initial clinical finding in 25% of patients. 3
Heparin-induced thrombocytopenia is an immune-mediated response to heparin exposure. In some patients, the heparin molecule may form a complex with platelet-factor 4 released by activated platelets. These heparin–platelet-factor 4 (HPF4) complexes can be recognized by immunoglobulin G (IgG) class antibodies, forming immune complexes. 4 The HPF4–IgG immune complexes can bind to specific receptors in the platelet membranes and/or endothelial cells, leading to platelet activation, aggregation, release of procoagulant microparticles, endothelial activation, and thrombin generation. This immune reaction is manifested clinically by thrombocytopenia and a paradoxical prothrombotic state that can result in arterial thromboembolic event and/or VTE, increasing morbidity and mortality. 5
The available literature describing HIT in lung transplant patients is limited, comprising several case reports and a single case series. Our study attempts to describe the largest known cohort of lung transplant recipients who developed HIT peritransplant, compared to a matched cohort, and explored how this diagnosis impacts recipient survival.
Materials and Methods
Design, Setting, and Population
A retrospective cohort study was undertaken of 1171 lung transplant recipients at a quaternary referral hospital, transplanted between January 1, 2005, and February 16, 2017, approved by the institutional review board (IRB; #17-398). The requirement for informed consent was waived by the IRB, since the data obtained were limited and deidentified. Patients who received a retransplant (N = 21) or multi-organ transplant were excluded (N = 7) as their clinical course was considered to be unique. From this list, all patients treated with the direct thrombin inhibitor bivalirudin were derived (N = 51). This ensured that all patients who underwent treatment for the suspected or confirmed HIT were captured, since bivalirudin is the treatment of choice at our institution.
Chart review was used to determine whether the diagnosis of HIT was confirmed unequivocally by a diagnostic HIT algorithm (Figure 1) including clinical and laboratory data. Four criteria are used for evaluation of the pretest probability of HIT; platelet count fall, timing of platelet count fall, thrombosis, and other possible causes for thrombocytopenia, known as the 4T HIT score. For patients with thrombocytopenia who had an intermediate or high pretest clinical suspicion based on the4T HIT clinical risk score ≥4, the diagnosis of HIT was confirmed by either of the following criteria: a positive anti-HPF4 antibody assay and a positive functional platelet assay (serotonin release assay/heparin-induced platelet aggregation assay [SRA/HIPA]) or, for patients who did not undergo CPB, a positive anti-HPF4 antibody assay.
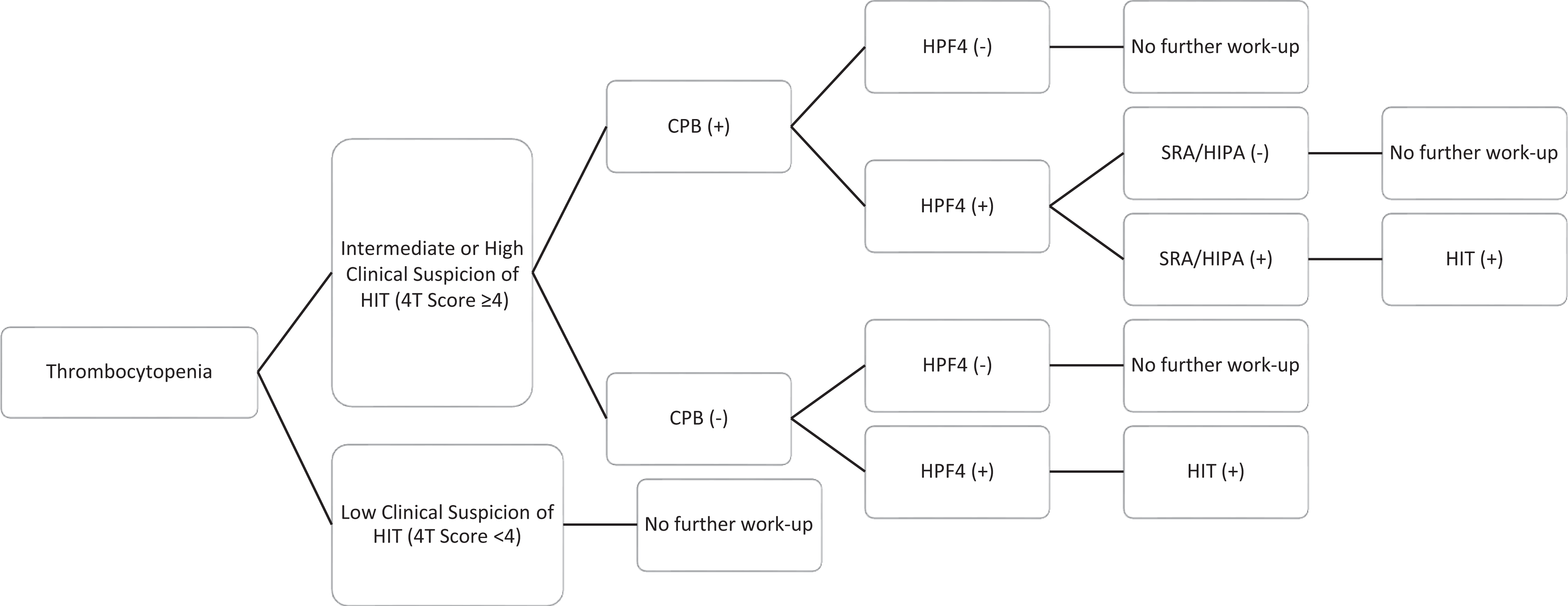
Diagnostic algorithm for clinical heparin-induced thrombocytopenia. CPB indicates cardiopulmonary bypass; HIT, heparin-induced thrombocytopenia; HIPA, heparin-induced platelet aggregation assay; HPF4, anti-heparin-PF4 IgG assay; IgG, immunoglobulin G; SRA, serotonin release assay; SRA and HIPA are both functional platelet assays; 4T score, clinical risk score for heparin-induced thrombocytopenia.
The anti-HPF4 antibody test is sensitive, however, less specific than the functional HIT assays. 6 False-positive anti-HPF4 results can occur in up to 50% of patients who undergo CPB; however, the incidence of HIT remains much lower at approximately 1% to 3%. 3,7 Therefore, patients should undergo a functional assay to improve the specificity of testing regardless of the pretest probability. 3 Our diagnostic algorithm was determined retrospectively but is consistent with diagnostic recommendations. Patients who developed HIT within 30 days of transplant or during their index admission for transplantation were included in the study.
A control group of patients were chosen from the original cohort, matched to the HIT group patients in a 2:1 ratio with statistical propensity score matching of age, race, gender, indication for transplant, lung allocation score (LAS) at the time of transplant, and whether they received a single or double lung transplant. Matching these factors between cases and controls were felt to control for confounding factors including the underlying disease process and severity.
Data Collection
For both control and HIT groups, in addition to matching variables, patient data were extracted including the use of extracorporeal membrane oxygen (ECMO) or CPB, hospital and intensive care unit (ICU) length of stay (LOS), readmissions within 30 days, and survival days until censorship, defined as the time of data extraction. The type and duration of anticoagulation peritransplant were investigated in HIT patients, with laboratory data including HIT diagnostic laboratory testing, and complete blood counts. Duration and type of anticoagulation used were also recorded from medical administration records in the electronic chart. Diagnostic testing for HIT included both antigenic and functional HIT assays. Results of the antigenic enzyme-linked immunosorbent assay (ELISA) detecting IgG-specific antibodies against HPF4 complexes in patient serum (anti-PF4-Heparin IgG assay; GTI Diagnostics, Waukesga, Wisconsin) were recorded with positive assays reported with an optical density >0.4. Functional HIT assay results, including the 14C-SRA and the HIPA, results were also recorded. Upper extremity and lower extremity duplex and ventilation-perfusion scan or computerized tomography of the chest with contrast studies (completed if clinically indicated) from all patients after their diagnosis of HIT were reviewed for the presence of thromboembolism. Any episodes of bleeding documented were recorded and separated into major 8 and nonmajor bleeding, with the number of transfusions received recorded.
For each patient, a 4T HIT score 9 and Lillo-Le Louët score 10 for prediction of HIT in the setting of CPB (if applicable) were obtained from chart documentation from Vascular Medicine consultation or retrospectively calculated. The 4T score was used to determine the pretest clinical suspicion of HIT. Scores were divided into low (≤3), intermediate (4-5), and high (≥6) pretest clinical suspicion, corresponding to an estimated HIT risk of <5%, 8% to 28%, and 21% to 100%, respectively. 9,11 The Lillo-Le Louët score accommodates for thrombocytopenia attributable to CPB, which generally resolves during the first 4 postoperative days. 10 Scores are separated into low (<2) and high (≥2) probability of HIT, with negative and positive predictive values of 97% and 62%, respectively. 10
The primary end point was patient survival following lung transplant until study censorship. Secondary end points included thromboembolic events, hospital and ICU LOS, 30-day readmission rates, as well as 30-day, 90-day, 180-day, and 1-year survival.
Data Analysis
Statistical analysis was completed by biostatisticians; all tests were 2 tailed, with a statistical significance level of 0.05 using SAS 9.3 software (SAS Institute, Cary, North Carolina). Propensity scores were used to match the control group to the HIT group in a 2:1 ratio. Cohort patients were assigned scores and matched to HIT patients based on a radius model of propensity score differences for selected variables: age, race, gender, indication for transplant, LAS at the time of transplant, and receipt of a single or double lung transplant. 12 Descriptive statistics of the control and HIT group characteristics were calculated including mean, median, frequency, standard deviation, and confidence intervals (CIs).
The Kruskal-Wallis was used to determine whether ICU LOS, hospital LOS, and readmission frequency were significantly different between the HIT and control group. The χ2 testing was used to evaluate categorical variables including 30-day readmissions between the HIT and control group. Both the log-rank test and Cox proportional hazard model were applied to test whether patient survival days (30-day, 60-day, 6-month, 1 year, and overall) were different between the HIT and control groups.
Results
Fifty-one patients were treated with bivalirudin in the selected cohort; however, 23 patients were excluded because they did not fulfill criteria of the diagnostic HIT algorithm, and 3 patients were excluded due to a late diagnosis, defined as more than 30 days after transplant. (Figure 2). Patients with HIT (N = 25) were aged 26 to 70 years (mean [M] = 58.5, 95% CI: 54.3-62.7), and most were male (n = 22, 88%). Over half of the patients underwent double lung transplant (n = 13, 52%) with the most common indication for transplant being restrictive lung disease, specifically idiopathic pulmonary fibrosis (N = 14, 56%), followed by chronic obstructive pulmonary disease (N = 7, 28%) and other indications (N = 4, 16%) including sarcoidosis and lymphangioleiomyomatosis. Among recipients with HIT, median LAS was 42.6 (mean = 50.8, 95% CI: 41.6-60.0), and scores ranged from 31 to 90. Prior to May 2005, the LAS was not used, therefore, 2 patients did not have this score. Cardiopulmonary bypass was used in 12 transplant recipients with HIT (48%), and ECMO was used for 1 recipient with HIT (4%) intraoperatively. The matched control group demonstrated similarities in terms of age, gender, and the presence of bilateral lung recipients, in addition to the use of extracorporeal life support (CPB and ECMO; Table 1).
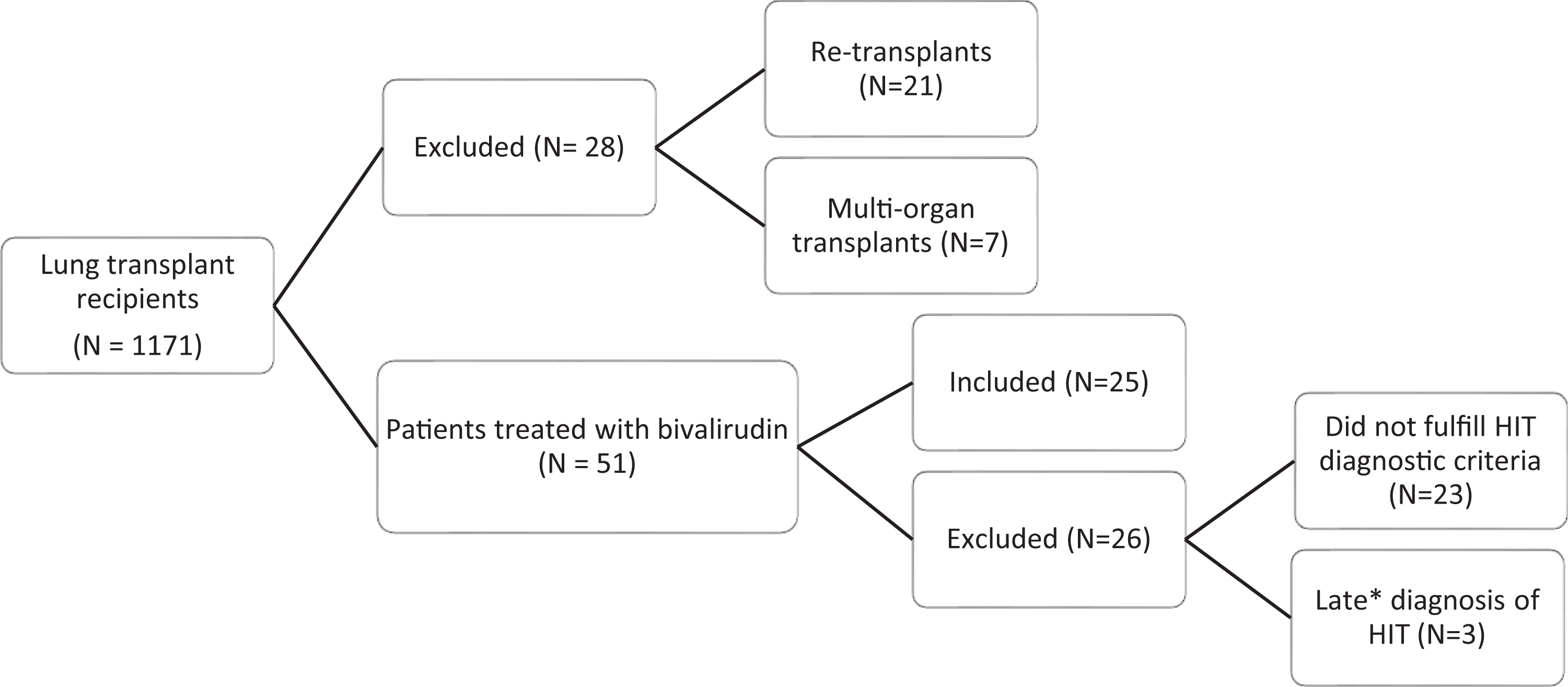
Heparin-induced thrombocytopenia (HIT) patient selection algorithm.* >30 days after transplant.
Characteristics of Total Population, Heparin-Induced Thrombocytopenia Group, and Matched Controls.
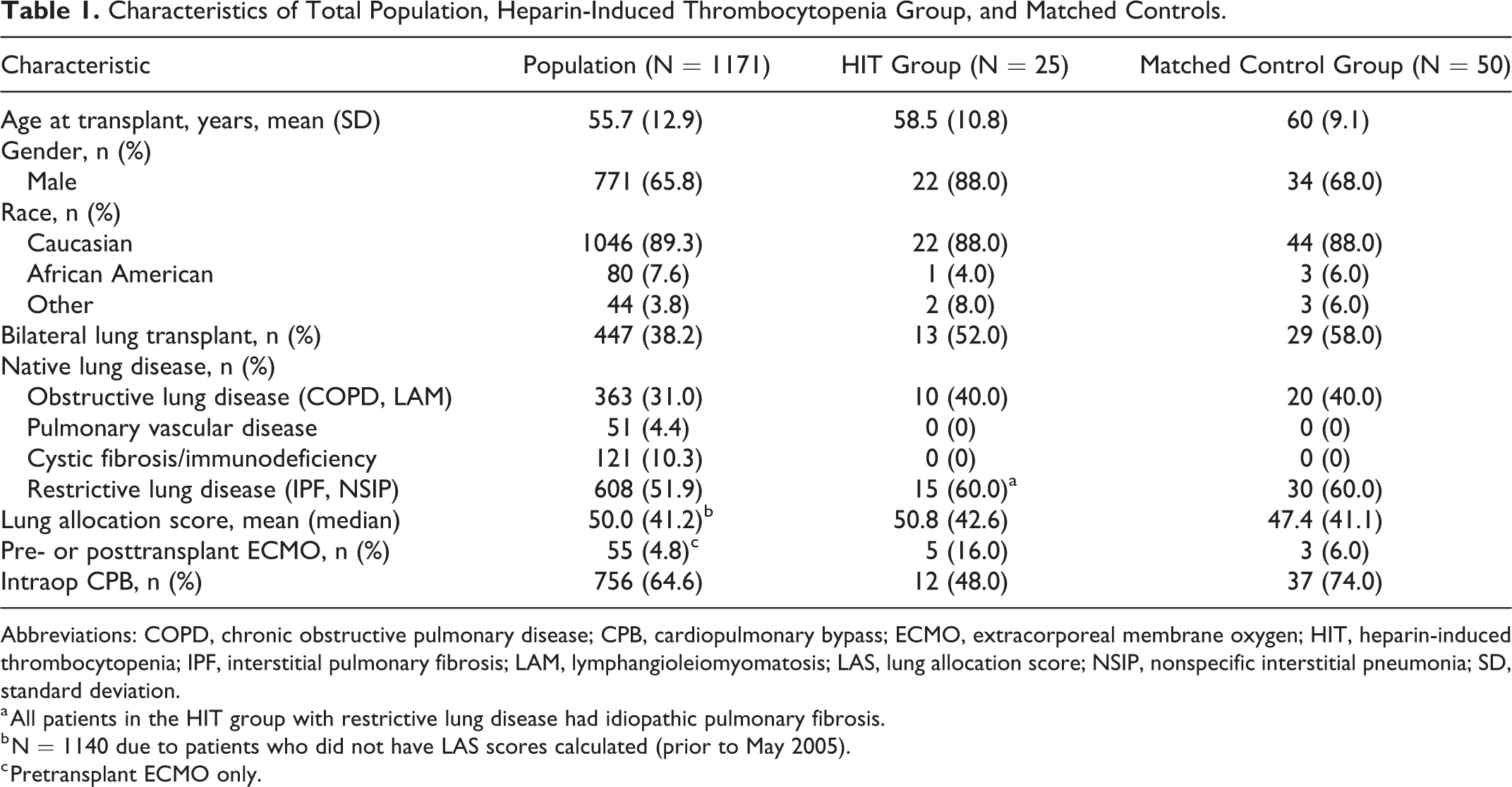
Abbreviations: COPD, chronic obstructive pulmonary disease; CPB, cardiopulmonary bypass; ECMO, extracorporeal membrane oxygen; HIT, heparin-induced thrombocytopenia; IPF, interstitial pulmonary fibrosis; LAM, lymphangioleiomyomatosis; LAS, lung allocation score; NSIP, nonspecific interstitial pneumonia; SD, standard deviation.
a All patients in the HIT group with restrictive lung disease had idiopathic pulmonary fibrosis.
b N = 1140 due to patients who did not have LAS scores calculated (prior to May 2005).
c Pretransplant ECMO only.
In total, 12 (48%) patients received intraoperative UFH during implantation, CPB or ECMO, and 1 patient received bivalirudin intraoperatively because of a pretransplant diagnosis of HIT. After transplant, 15 (60%) patients received only subcutaneous UFH (5000 U administered twice daily), 7 (28%) patients received both subcutaneous and intravenous (IV) UFH, and 3 (12%) received an UFH infusion alone (IV infusions were used for atrial fibrillation, VTE, and ECMO). Patients received a mean of 13.4 (95% CI: 10.9-15.9) days of UFH therapy prior to being diagnosed with HIT, with 84% being exposed to heparin for 9 or more days prior to diagnosis.
Most patients with confirmed HIT had an intermediate pretest clinical suspicion based on 4T score (68%, n = 17), but 8 (32%) patients had a high pretest suspicion. For 1 patient, the Lillo-Le Louët score was not calculated due to unclear duration of CPB. All other recipients who underwent CPB had Lillo-Le Louët scores indicating a high pretest suspicion of HIT.
All patients with confirmed HIT had a positive anti-HPF4 antibody test (N = 25) with a mean optic density of 1.74 (95% CI: 1.45-2.03). Functional assays were completed in all but 1 patient. Twenty-one patients had a positive SRA, 3 patients had a negative SRA but a positive HIPA. One patient who did not undergo CPB had a negative HIPA and no SRA testing.
The platelet nadir for patients with HIT following transplant was a mean of 51.4 × 103/μL, 95% CI: 39.5-63.3, and platelet recovery was seen within a mean duration of 10.5 days (95% CI: 3.4-17.6) for all. Platelet recovery was defined as a substantial and steady recovery of platelet count from its nadir to at least 100 × 103/μL. Two patients with HIT never had a complete platelet recovery, and both later passed away due to multi-organ failure within their index transplant admission. For 2 transplant recipients, data for platelet recovery were not available; due to 1 developing HIT at another institution and the other with a platelet nadir of >100 × 103/μL.
Three (12%) patients suffered episodes of major bleeding; 1 patient had postsurgical bleeding immediately following his lung transplant and 2 others bled due to a gastrointestinal source. Of note, the postsurgical bleeding was in a patient who had bivalirudin treatment prior to transplant. One patient experienced nonmajor bleeding. Patients did, however, require transfusions during their hospital stay after initiation of bivalirudin for HIT treatment, requiring a mean of 1.8 U of packed red blood cells (95% CI: 0.2-3.5). There were no deaths due to major bleeding.
The incidence of thrombosis associated with a diagnosis of HIT was 72%. Fifteen (60%) patients had acute deep vein thrombosis (DVT), 2 (8%) patients had acute pulmonary embolism (PE), and 1 (4%) patient had objectively confirmed acute DVT and PE. Most patients were found to have upper extremity DVT (n = 10, 40%), compared to lower extremity DVT (n = 4, 16%), and synchronous upper and lower extremities DVT (n = 1, 4%). All cases were VTE with no arterial thromboembolic events and no HIT thrombosis-related deaths.
Transplant patients with HIT were found to have a significantly longer overall hospital LOS (P = .011) in comparison to control patients. The control group was found to have a mean hospital stay of 32 days (95% CI: 21.0-43.2) as compared to 43 days (95% CI: 29.0-57.8) in the HIT group. There was no difference in ICU LOS (P = .22), with patients staying in the ICU for a mean of 16 days (95% CI: 6.8-24.4) and 14 days (95% CI: 6.0-21.4), in the HIT and control groups, respectively (Table 2). Transplant recipients in the matched control group were readmitted more frequently within 30 days after discharge (P = .0007); 62% of patients were readmitted in the control group (N = 31), as compared to 20% (N = 5) in the HIT group.
Length of Stay, Readmission Rate, and Overall Survival Between Groups.

Abbreviations: ICU, intensive care unit; LOS, length of stay; SD, standard deviation.
Median survival for the HIT cohort was 721 days (1.97 years) until study censorship, with a range between 25 and 2830 days following transplant (M = 1051.12, 95% CI: 690.3-1412.0). One HIT patient died within the first 30 days due to multi-organ failure secondary to sepsis. Chronic allograft rejection was the most common cause of death (n = 3, 12%); with 2 patients passing away with bronchiolitis obliterans syndrome grade III and 1 with restrictive allograft syndrome. 13 There were no thrombosis-related deaths due to HIT.
For the primary outcome of the study, the impact of HIT diagnosis on patient overall survival posttransplant up to the time of study censorship, we found there was no significant difference between the control and HIT groups (P = .415; Table 2 and Figure 3). In addition, no difference was found between HIT and control groups in 30-, 90-, 180-, 365-day posttransplant recipient survival.
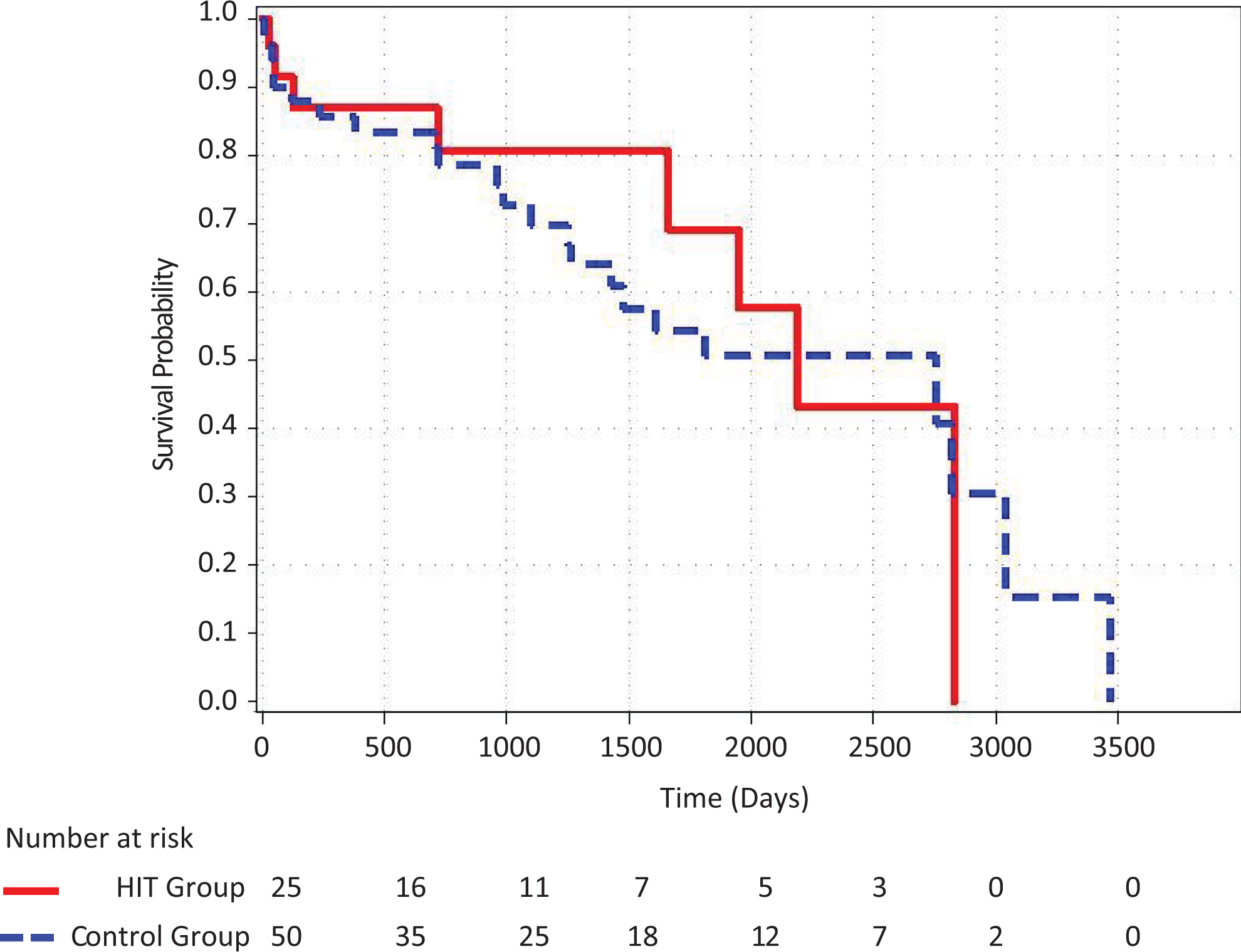
Cox model of overall survival in HIT and control groups. HIT indicates heparin-induced thrombocytopenia.
Discussion
This is the first large observational study describes 25 cases of confirmed HIT over a 12-year period at a single transplant center; 2.1% of all lung transplant recipients. The limited literature available indicates a slightly lower incidence of 0.9% based on a smaller single case series. 14 This difference may be dependent on several factors, including the frequency of use of ECMO or CPB, duration, type and dose of anticoagulation (based on specific institutional practice), and severity of illness.
Arterial thromboembolic event and VTE are common in HIT, with retrospective and prospective cohorts reporting an incidence of objectively confirmed thromboembolic events in 20% to 34% of patients within 30 days of HIT diagnosis. 3,15 –17 Without treatment, the rate of thrombosis was estimated at 5% per day without alternative anticoagulation with a direct thrombin inhibitor. 18 In our study, we found an incidence of VTE of 72%, higher compared to other reports, but no patients had arterial thromboembolism. Upper extremity VTE were present in 60% of patients, likely due to the presence of central venous catheters during the peritransplant and early postoperative period. This is consistent with previous reports of HIT in which most upper extremity DVT events were related to the concomitant presence of central venous catheters. 19
This study supports the concept that HIT has an impact on hospital LOS in the lung transplant population. The increased LOS should not be attributed to pretransplant disease severity, as HIT patients were matched to the control cohort based on LAS. This phenomenon has been observed post-cardiac surgery, where a diagnosis of HIT was found to increase LOS by 6 to 7 days and increase hospital costs by more than US$20 000 per patient.
Chronic allograft dysfunction was the most common cause of death for recipients with HIT, similar to lung transplant recipients overall who survive more than 1 year. 20 Despite the fact that patients who develop HIT have a very high 30-day incidence of arterial thromboembolic event and VTE as well as thrombosis-related death, 17,21 we did not observe any significant difference in terms of mortality between lung transplant recipients who developed HIT and those who did not. We believe that early recognition and prompt management was of paramount importance to mitigate the risk of extensive and/or life-threatening thromboembolic events. Additionally, our investigation had a limited sample size, not adequately powered to detect a difference in survival. Future studies involving multiple centers may allow for an adequate number of cases.
The matched control population had an increased 30-day readmission as compared to the HIT group. We believe that since patients with HIT remained in the hospital longer, they may have had any possible readmission issues addressed during this time and/or were admitted to rehabilitation at the time of discharge with close monitoring and follow-up, preventing readmissions.
Heparin-induced thrombocytopenia is a clinicopathologic syndrome, wherein a diagnosis requires both an intermediate or high pretest clinical suspicion assessed by validated clinical risk prediction scores, followed by laboratory confirmation. We retrospectively designed a diagnostic algorithm for HIT considering the different diagnostic performance of available HIT assays. As such, all patients enrolled in our cohort had a positive HPF4 ELISA, and all patients who had undergone CPB (a setting in which the HPF4 antibody assay is less specific) also had a positive functional assay; either the SRA or HIPA. When both the antigenic and the functional assay are positive, the positive predictive value of HIT is 100%. 22,23 Thus, our diagnostic algorithm assured a strict diagnostic criteria for HIT.
Previous HIT studies have shown that UFH is associated with an increased risk of developing HIT compared with low-molecular-weight heparin. 24 In our study, transplant recipients who developed HIT had been exclusively exposed to UFH, with more than a third receiving therapeutic continuous IV UFH treatment posttransplant. This may also help explain the higher incidence of HIT of 2.1% in our study.
Platelet recovery is seen within 7 days in 90% of patients with HIT; however, it can take up to several weeks. 25,26 In a previous investigation of HIT in liver transplant recipients, recovery of platelets (to 100 × 103/μL) within 1 to 2 weeks was observed. 27 Findings were similar in our lung transplant population. It is important to recognize the wide differential of thrombocytopenia after lung transplantation that may be considered if HIT is excluded and causes which may also contribute to a slightly delayed platelet recovery in HIT, including medications and infections.
Treatment of HIT includes the use of a direct thrombin inhibitor to prevent thrombosis, which can place patients at increased risk of bleeding. In addition, these anticoagulants do not have readily available effective reversal agents. Bleeding events have been estimated at approximately 9% for argatroban and 12% for bivalirudin based on a recent meta-analysis. 28 In our study, major bleeding occurred in 3 HIT patients on bivalirudin treatment; this rate of 12% is similar to previous investigations in a combined medical and surgical critical care population. 29
Limitations
Only patients who were treated with bivalirudin were included for this retrospective study. Nevertheless, we are confident that we did not miss any cases of confirmed HIT in lung transplant patients. In support of this (a) patients were not started on anticoagulation with a direct thrombin inhibitor unless they had an intermediate or high pretest clinical suspicion of HIT assessed by the Vascular Medicine service with the use of validated risk prediction scores, (b) bivalirudin is the preferred thrombin inhibitor in our institution, while argatroban is rarely (if ever) used. Bivalirudin use for the treatment of HIT is off-label but has been demonstrated to be a safe and effective treatment for HIT, 28,29 and (c) all cases of suspected HIT are evaluated and followed by the vascular medicine service, who restrict and monitor use of direct thrombin inhibitor.
We designed a very strict diagnostic algorithm for HIT confirmation because neither the 4T HIT nor the Lillo-Le Louët score has been validated specifically in transplant patients who frequently have multifactorial thrombocytopenia and to isolate specifically patients with HIT. We recognize that this approach to our study design may have resulted in the exclusion of some patients with HIT from our analysis; however, we believe that our study sample included patients with unequivocal diagnostic confirmation of HIT.
In addition, a matched retrospective cohort was used to assist in describing the results of our HIT lung transplant recipient sample. Despite optimal statistical efforts and use of a large cohort of over 1000 patients, differences in the use of extracorporeal life support (ECMO and CPB; 80% in the control group as opposed to 64% of the HIT group) and gender are present between the 2 groups, which remains a limitation for drawing significant conclusions.
This cohort study is also a single-center investigation, with institutional practices in terms of surgical and medical care of lung transplant patients. This may make our findings less generalizable.
Future Directions
Best practices in treating lung transplant patients should include an early evaluation of HIT risk factors in the setting of thrombocytopenia, particularly in patients who require CPB/ECMO. The electronic medical record could be used as an adjunct to flag when these risk factors are present with an alert to providers. Heparin product use should be limited; if a patient is ambulating or the indication for which therapeutic treatment is no longer present. In stable patients, alternative prophylactic anticoagulation could be considered including oral direct thrombin inhibitors.
Conclusion
Our retrospective cohort illustrated the impact of HIT in lung transplant recipients, increasing morbidity and duration of hospitalization, with unclear effects on mortality. Limiting CPB and ECMO use in lung transplant recipients may reduce the risk of HIT. Utilization of a diagnostic HIT algorithm, such as the one recommended in this article, along with expert consultation to confirm HIT diagnosis is strongly recommended. When many etiologies of thrombocytopenia are possible following lung transplant, judicious use of direct thrombin inhibitor therapy in recipients is warranted. Our goal is to do no further harm to patients as we aim to safely give our patients a new lease on life.
Footnotes
Acknowledgments
Xiaofeng Zhang, for his assistance with statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.