
Abstract
Introduction:
Contemporary dosing strategies for rabbit anti-thymocyte globulin (rATG) in kidney transplantation aim to reduce cumulative exposure, minimizing long-term adverse events. The use of ideal body weight-based dosing has been trialed, however concern for increased rejection post-transplant exists due to lower doses of rATG. Research Questions: The primary aim of this study was to compare rejection rates between rATG dosing protocols using actual body weight and ideal body weight and secondarily to evaluate cost savings following protocol implementation.
Design:
This was a retrospective study surrounding implementation of an ideal body weight-based dosing protocol for rATG. We compared 75 kidney transplant recipients in whom rATG was dosed based on actual body weight (pre-protocol group) to 64 in whom dosing was based on ideal body weight (post-protocol group), following a nine-month washout.
Results:
The mean cumulative rATG dose in the pre-protocol group was 6.3 mg/kg of actual body weight. When ideal body weight was used in the post-protocol group, the mean dose was 4.5 mg/kg of actual body weight. The rejection rate was 18.7% pre-protocol and 23.4% postprotocol, which did not represent a statistically significant difference (p = 0.491). The actual annual cost savings after protocol implementation exceeded $162,000, approximately $2,500 per patient.
Conclusion:
Results suggest ideal body weight-based dosing of rATG may reduce exposure and cost, without significantly impacting the risk of rejection in kidney transplant recipients. More studies are needed to confirm these findings.
Keywords
Introduction/Background
Rabbit anti-thymocyte globulin (rATG)(Thymoglobulin™, Genzyme Co, Cambridge, MA) remains a cornerstone of solid organ transplant induction regimens due to its ability to deplete T-cells in the peri-transplant period, preventing allograft rejection. 1,2 Unfortunately, this therapy has also been linked to increased risk for infection and malignancy, which translate into higher healthcare costs. 3 –5 One economic analysis tallied up to 5.5% of total inpatient Medicare expenditures being used for cancer care in the first 3 years post-transplant. 6 When compared to the non-depleting immunosuppressant basiliximab, infections and malignancy are more common with rATG, 7 yet non-depleting induction may not be desirable for patients at an increased risk of organ rejection. In light of this, research efforts have focused on effective strategies for adequate immunosuppression while minimizing adverse drug effects.
Several studies have evaluated reducing exposure and containing drug costs by decreasing the overall induction dose of rATG. A dose-sparing approach of 1 mg/kg/day has been compared to 1.5 mg/kg/day and was found to have a similar effect on prevention of organ rejection. 8 Another strategy employed T-cell count monitoring to guide recurrent rATG doses, whereby rATG was given only when counts surpass a certain threshold. 9 The lack of rATG distribution into adipose tissue may allow for leveraging the pharmacokinetic profile by using ideal body weight (IBW)-based dosing, thereby reducing cumulative exposure. This approach may be particularly sensible in the setting of increasing rates of obesity in the transplant population. 10 Two studies have found these strategies to yield favorable outcomes related to rejection and graft function; however they are limited by small sample sizes and lack of specific information about cumulative dose exposure. 10,11
This quality improvement study sought to evaluate post-transplant care process improvement through dose minimization of rATG using an IBW-based dosing protocol in a large cohort of kidney transplant recipients. The primary outcome of interest was allograft rejection. Secondarily, we sought to evaluate the economic impact of this dosing strategy.
Methods
Design
This was a single center, before-and-after quality improvement study of adult kidney transplant patients. The process was conducted in accordance with the Squire 2.0 guidelines, under the supervision of the Kidney and Pancreas Quality Assessment and Performance Improvement Committee, and approved by the Institutional Review Board (IRB) at this institution. 12
Population
The patient population included patients who are adults (≥18 years old), received a living donor or a deceased donor kidney transplant, and qualified for rATG induction immunosuppression. Due to the timing of protocol implementation, patients who received a transplant in the years 2013 and 2015 were specifically assessed. Patients at this institution receive rATG if their donor specific antibodies (DSA) with mean fluorescence intensity (MFI) were ≥ 2000 or if they have a positive flow cross match with any DSA value. Patients receive basiliximab if they have an HLA 2 haplotype matched donor (sibling) or zero mismatch assuming high resolution HLA typing, are high risk for PTLD, high risk for infection, previous non-kidney/pancreas solid organ transplant, malignancy (especially melanoma), or over 65 years old.
Sampling Strategy
An internal transplant database was used to identify all patients who received a kidney transplant in 2013 and 2015 who received rATG for their induction immunosuppression. Patients were reviewed via retrospective chart review and excluded if they had received a combined transplant or if they did not exclusively use rATG for induction. After exclusions were applied, a complete enumeration approach was used to include all other patients meeting inclusion criteria during the study timeframes.
Protocol Implementation
Patients transplanted between January 1 and December 31, 2013 were part of the pre-protocol implementation group and received rATG 1.5 mg/kg based on actual body weight (ABW) for 4 doses (6mg/kg ABW total) beginning on the day of transplant, in accordance with the standard institutional practice at that time. In February 2014, a new protocol dosing rATG at 1.5 mg/kg of IBW for 4 doses was approved by the Kidney and Pancreas Quality Committee, striving to standardize rATG dosing, minimize cost associated with rATG therapy, and reduce risk of medication-related adverse effects. Education was provided to the kidney transplant prescribers and pharmacists, and the protocol was implemented in March 2014.
After a nine-month washout period, patients who received kidney transplantations with rATG induction between January 1 and December 31, 2015 were evaluated for inclusion in the post-protocol implementation group. Dosing based on ABW was permitted if ABW was less than IBW. To be considered consistent with the protocol, doses needed to be within 5% of the admission IBW-based dose calculated by our investigators. Patients who received one dose of basiliximab initially and were subsequently switched to rATG for induction were included, as the providers would have needed to follow the protocol for rATG doses. Additionally, all patients followed a similar immunosuppression protocol post-kidney transplant, including tacrolimus (goal range 8-10 ng/mL in the first month and 6-8 ng/mL after the first month), mycophenolate mofetil (750-1000 mg twice daily), and steroids (methylprednisolone for 2 days followed by a prednisone taper over several weeks until 5 mg daily is reached). Patients were excluded if they received a kidney transplant in combination with any other organ or were less than 18 years old.
Data Collection
Demographics and type of kidney transplant performed (deceased donor versus living donor) were collected for all patients in the pre- and post-implementation periods. Each dose of rATG was collected and categorized according to the weight-based dosing strategy used for calculation in order to assess protocol adherence post-implementation. All rATG doses received by the patient needed to be calculated correctly in order to be considered adherent.
The primary outcome was to compare rates of rejection in the pre-protocol group and post-protocol group to assess for potential counterbalance of protocol implementation. Patients were assessed for the occurrence of acute cellular or antibody-mediated rejection within 2 years post-transplant or at date of last follow-up, whichever occurred first. Patients that met institutional criteria for rejection include those with IA; IB histologic grade with capillaritis and/or C4d positivity; and all patients with IIA, IIB, or III histologic rejection grade per biopsy report. A rejection episode was also included if a patient was treated based on clinical suspicion of rejection, despite the absence of a biopsy, with any of the following agents: methylprednisolone, rATG, eculizumab, or intravenous immune globulin. Rejection episodes were excluded if patients were only treated with oral prednisone or an increase in maintenance immunosuppression. There was a change in United Network for Organ Sharing (UNOS) allocation methodology mid-study that affected the consideration for rejection risk in kidney transplant patients. To assess if this resulted in an imbalance of rejection risk between groups, the peak calculated percentage of panel reactive antibodies (cPRA) was collected for deceased donor organ recipients in both cohorts.
As a secondary endpoint we sought to assess the cost implications of the IBW-based dosing strategy. Acquisition cost of rATG was calculated based on the number of 25 mg vials necessary for the dose the patient would have received based on their actual body weight and was then compared to the cost of 25 mg vials actually utilized to prepare the doses received based on ideal body weight. Due to a change in rATG vial acquisition cost between 2013 and 2015, the 2015 acquisition cost was used for all calculations in this study to approximate institutional cost-savings. Acknowledging that vial acquisition costs vary between institutions and have likely continued to increase since 2015, the goal of this endpoint was to conservatively approximate cost savings.
Data Analysis
Descriptive statistics were used to characterize sample demographics as well as the primary and secondary endpoints. The chi-squared test was used to compare rates of rejection between groups. We report the difference in risk and associated 95% confidence interval (CI) for an episode of rejection between pre- and post-protocol groups. An alpha level of 0.05 was set as the threshold for statistical significance.
Results
Study Sample
A total of 172 patients were screened for inclusion, of which 139 were included, 75 in the pre-protocol implementation group and 64 in the post-protocol implementation group. The most common reason for exclusion was receipt of a combined organ transplant (Figure 1). Patients were predominantly Caucasian and underwent living donor transplantation. Mean age was similar between groups; however the mean cPRA in deceased donor transplant was lower in the pre-protocol group compared to the post-protocol group (64% vs 74%). This was expected based on the change in UNOS allocation methodology that occurred during the study timeframe. There were no patients that had a reported cPRA of zero. Additional baseline characteristics are reported in Table 1. The median (SD) duration of follow-up for this study was 719 (58) days in the pre-protocol group and 702 (91) days in the post-protocol group, or 1.96 and 1.92 years respectively.
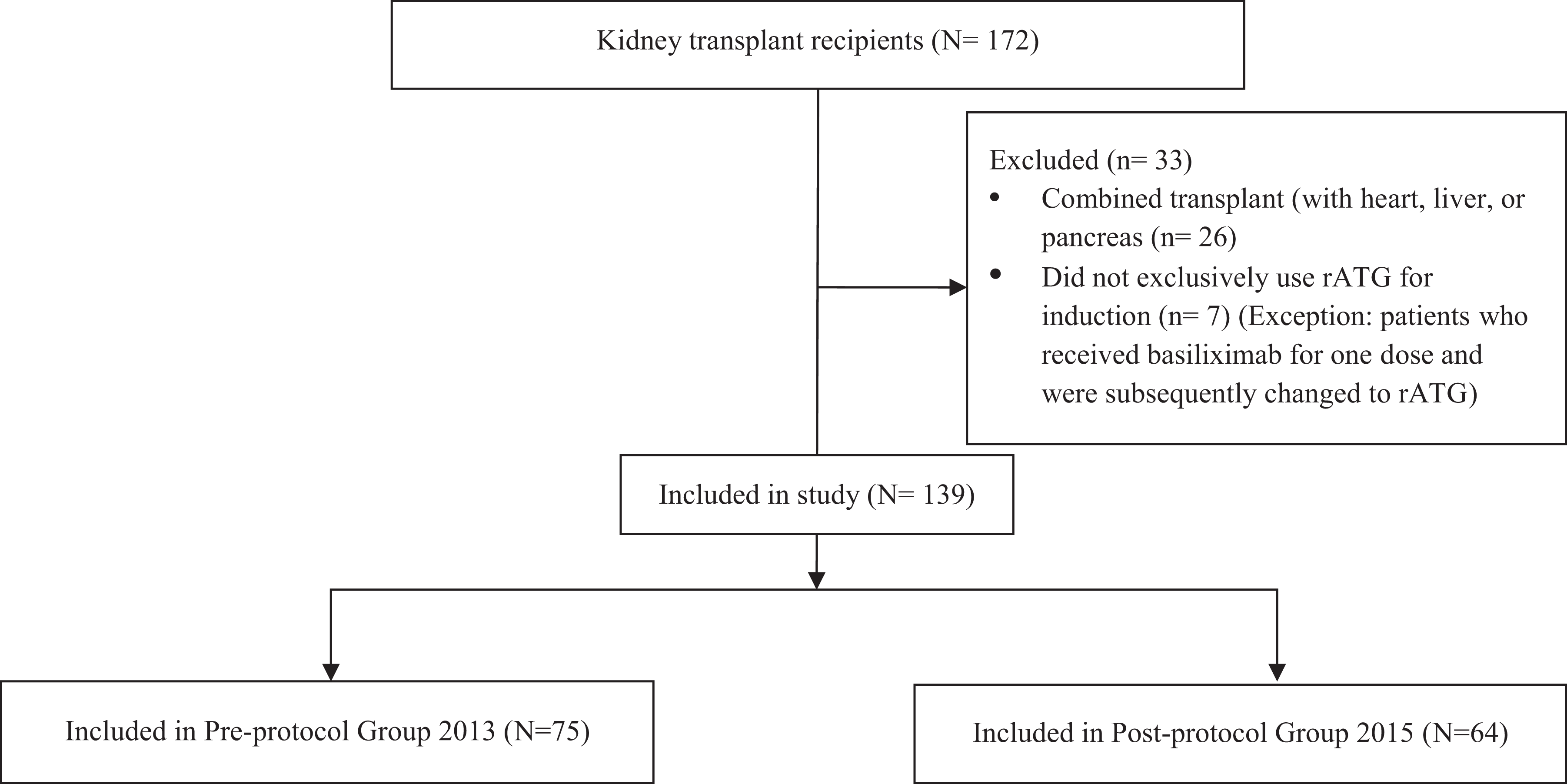
Participant flowchart.
Demographic Characteristics of Sample by Assigned Group.a
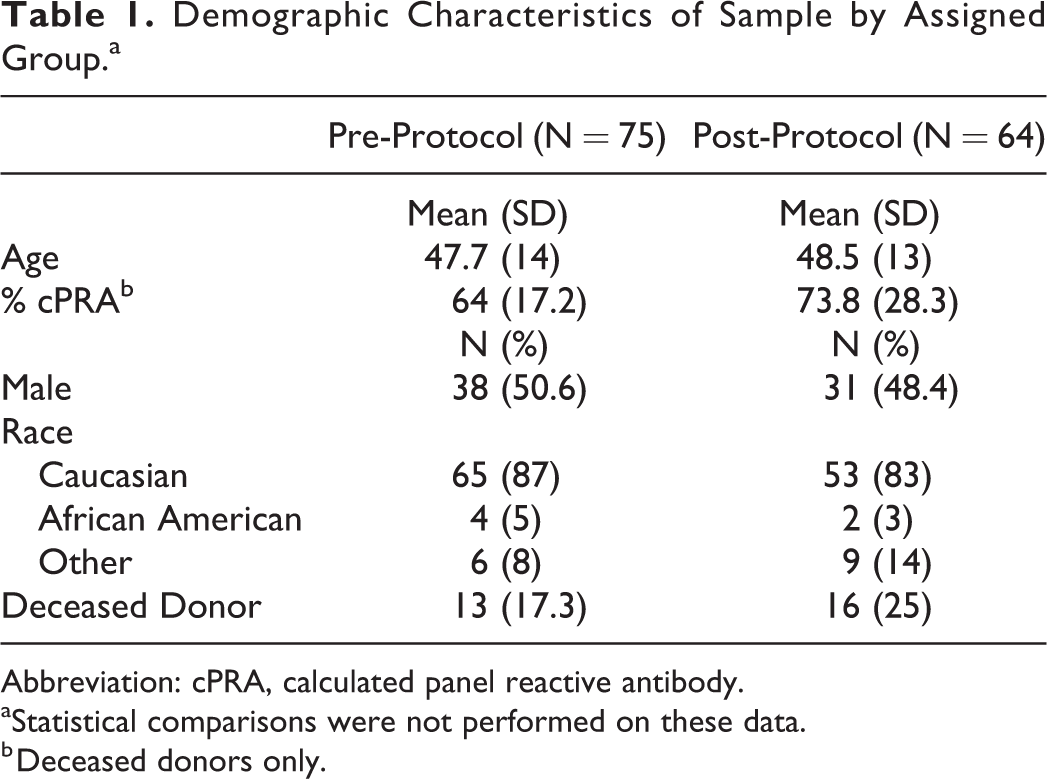
Abbreviation: cPRA, calculated panel reactive antibody.
aStatistical comparisons were not performed on these data.
b Deceased donors only.
Outcomes
The mean rATG dose received was 1.5 mg/kg of ABW in the pre-protocol group and 1.5 mg/kg of IBW in the post-protocol group (equivalent to 1.3 mg/kg of ABW). Mean cumulative rATG dose received in the pre- and post-protocol groups was 6.3 mg/kg and 4.5 mg/kg of ABW, respectively. Adherence to the new protocol was 77% (49/64 patients) (Table 2). Sixteen patients in the pre-protocol group received more than the standard 4 doses of rATG and 15 patients in the post-protocol group received fewer than the standard 4 doses. Giving non-standard rATG doses was at the discretion of the transplant surgeons based on a variety of clinical factors, but overall the pre-protocol group received more rATG than the post-protocol group, as expected based on the new IBW-based protocol. The actual amount of rATG that was administered was reflected in the mean single and mean cumulative rATG doses reported above.
Protocol Adherence.
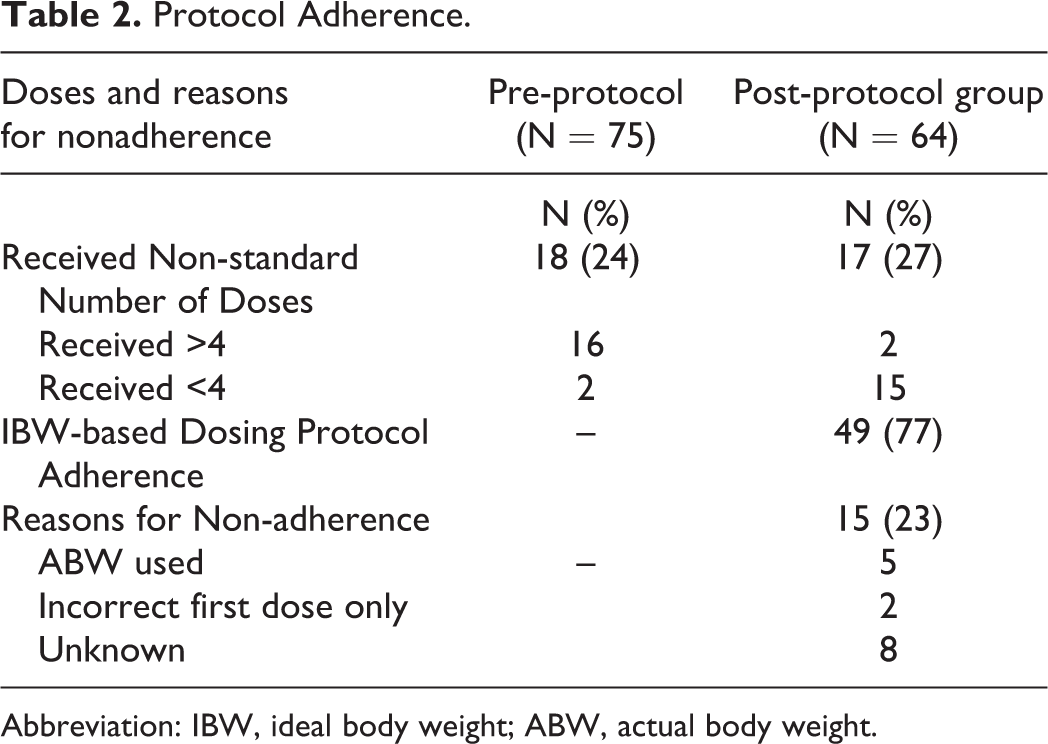
Abbreviation: IBW, ideal body weight; ABW, actual body weight.
Rejection occurred in 18.7% (n = 14) of patients in the pre-protocol group and 23.4% (n = 15) of patients in the post-protocol group within the first 2 years after transplant. The difference in risk was 4.7% (95% CI -8.9%, 18.3%, P = 0.49). Acute cellular rejection accounted for the majority of cases. The proportion of deceased donor transplants, ie non-directed donation affected by allocation guidelines, who experienced rejection was similar in both groups (29% vs 27%). Among those deceased donor transplants experiencing rejection, the mean cPRA was 61% in the pre-protocol group (n = 4) compared to 91.5% in the post-protocol group (n=4) (Table 3). When including only the 49 patients in the post-protocol group in whom the IBW-based dosing protocol was used for all doses, rejection occurred in 22.4% (n = 11). Compared to the pre-protocol rejection rate of 18.7%, the difference in risk was 3.7% (95% CI -11.0%, 18.3%, P = 0.6).
Characteristics of Patients Experiencing Rejection.a
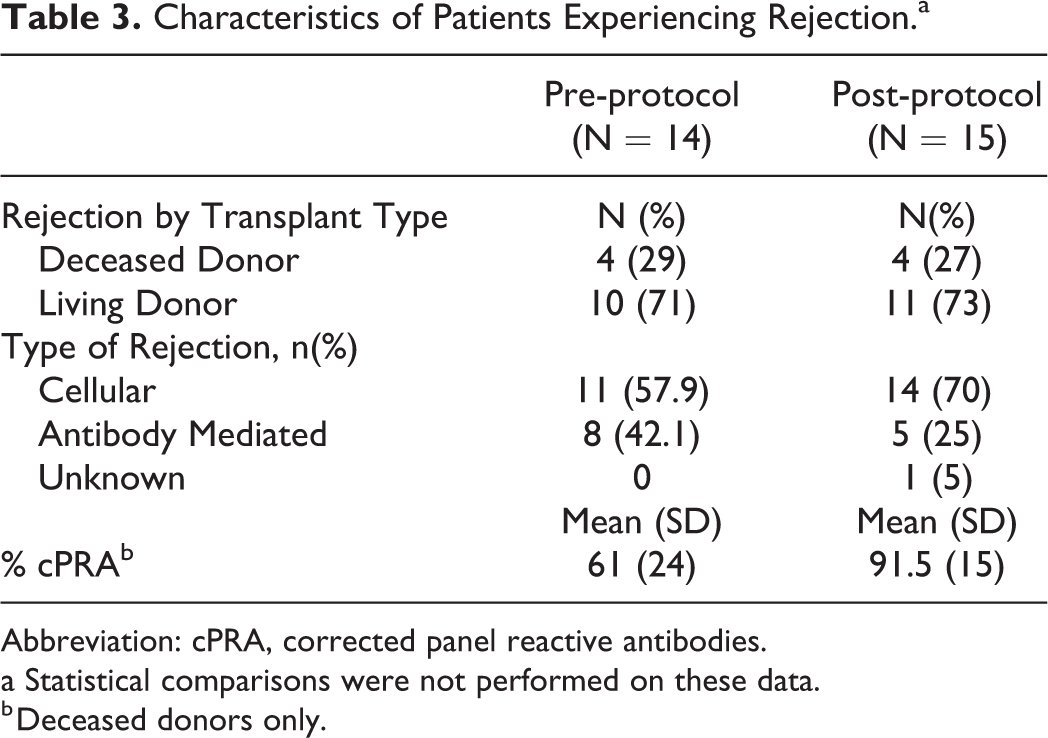
Abbreviation: cPRA, corrected panel reactive antibodies.
a Statistical comparisons were not performed on these data.
b Deceased donors only.
Cost-savings calculations performed with 2015 ATG vial acquisition cost demonstrated a cost-savings of more than $162 000 for the institution, or approximately $2500 per patient when the IBW-protocol was used. Projected annual cost if ABW had been used post-protocol was $680 372 whereas the actual cost incurred with the IBW protocol was $517 395. This led to a cost savings of $162 977, or $2546 per patient.
Discussion
This quality improvement study analyzed the impact of implementing an IBW-based dosing strategy for rATG in kidney transplant recipients. Decreasing total rATG exposure did not produce a statistically significant increase in transplant rejection rates following protocol implementation. Additionally, this strategy resulted in an estimated cost savings of approximately $2500 per patient for the institution.
Dosing strategies for rATG have varied over the years, recently aiming to reduce overall exposure during induction immunosuppression. 13 While the initial trials that established the safety and efficacy of rATG studied total doses of 10.5 mg/kg or higher, more modern studies have used cumulative doses of 5.9 to 6.53 mg/kg given over 4 to 7 days. 11,14 A study by Hardinger et al. used a cumulative rATG dose of 6mg/kg and showed a 95% 2-year rejection free survival despite using a lower dose than was previously thought necessary. 15 This dose-limiting concept was further investigated by Wong et al., who evaluated 1.5 mg/kg/day (4.5 mg/kg cumulative dose) compared to 1 mg/kg/day of rATG (3 mg/kg cumulative dose). Though T-cell suppression was sustained longer during the 6 months following transplant in the 1.5 mg/kg/dose group, regimens were similar with respect to their ability to prevent organ rejection. 8
After implementing a protocol to further limit rATG exposure based on drug pharmacokinetics and prior reported experiences with IBW-based dosing, we sought to assess the potential counterbalance of increased rates of rejection. Though a slightly higher percentage of patients experienced rejection in the post-protocol group, no statistically significant difference in rejection rate was seen. It is notable that low rejection rates and a limited sample size made it difficult to determine the true clinical relevance of this finding. The higher cPRA found in the post-protocol group of deceased donor patients may have contributed to the rejection trend by patients being at a higher risk of rejection at baseline; however this number was based on 4 patients per group, and the majority of rejections were T-cell, not antibody, related. Our results are consistent with other studies using lower cumulative doses of rATG, which also found similar rates of rejection and graft survival compared to the higher historical rATG dosing. 16 –18
One such study retrospectively compared cumulative doses of rATG >7.5mg/kg ABW to <7.5 mg/kg ABW, using the latter as a surrogate for IBW based dosing in a 5-day regimen of rATG. Unfortunately, patients were not actually dosed based on IBW and exact cumulative dose exposure was not reported. 10 Another publication compared rATG >7.5 mg/kg IBW to <7.5 mg/kg IBW, finding no difference in biopsy-proven rejection rates or graft survival. This investigation was limited by its small sample size and failure to report total dose received, limiting comparability to contemporary dosing strategies. 11 These results, in addition to the results from our quality improvement study, demonstrate that reducing the rATG dose to 1.5mg/kg/dose based on IBW may not impact rejection rates. Overall, the small number of patients in these trials does not allow for definitive conclusions, but suggests the need for larger, prospective studies to confirm these results.
The actual annual cost savings of over $162 000 at our institution, or $2500 per patient demonstrated by this study is becoming increasingly important in a time of decreasing insurance reimbursement rates. Cost savings without negatively impacting clinical outcomes are vital to maintaining transplant program solvency. Actual cost savings accrued using this dosing strategy will be dependent on individual institutional pricing and the patient population. Reducing overall exposure to thymoglobulin could also lead to further cost-savings by avoiding complications such as infection or malignancy. Further exploration of the association between reduced thymoglobulin exposure and risk for these clinical outcomes, along with any corresponding cost savings, is a topic for future research.
Strengths and Limitations
This represents the largest known study evaluating an IBW-based dosing strategy for rATG. Our practice was highly protocolized, allowing for precise and consistent treatment among patients, reducing inter-patient, practice-based variability. The transplant program has established regimented follow-up procedures providing patients with close monitoring for post-transplant complications and medication adjustments, resulting in improved follow-up and recognition of allograft rejection. Though larger than previously published reports on the subject, this quality improvement study was still limited by a small sample size and low incidence of rejection, making definitive conclusions difficult. In an effort to optimize our capture of true rejection episodes, we chose to include those which were also treated based on clinical suspicion, despite the absence of a biopsy. While this increased the sensitivity of our definition, it may have resulted in a higher rate of false positives among rejection episodes. Information on the maintenance immunosuppression regimens and adherence was not collected. Corrected panel reactive antibodies were collected for deceased donors in both groups, but donor specific antibodies (DSA) and positive crossmatch data were not collected. As rATG mainly affects T-cell mediated rejection via T-cell depletion, it has less of an impact on antibody mediated rejection. Additionally, since our institution uses a protocol to determine which patients receive rATG, similarly sensitized patients were represented in each group and DSA information was not vital to interpretation of the results. Lastly, despite a high degree of protocol adherence utilizing IBW-based dosing, adherence rates less than 100% may have provided more conservative results of our findings.
Conclusion
This quality improvement study demonstrated that patients receiving rATG 1.5mg/kg/dose based on IBW did not experience a significantly higher percentage of rejection episodes following kidney transplant. Decreasing overall exposure to rATG may reduce adverse effects while producing cost savings. Based on the lack of robust, prospective trials using this dosing strategy, further studies are needed to confirm the clinical significance of the results presented here in a larger population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.