
Abstract
Keywords
Introduction
Determining how to prepare and evaluate kidney transplant candidates for optimal outcomes continues to be an outstanding question in kidney transplantation. There are sparse data on the optimal approach or timing of these evaluations and/or education. Clinical guidelines recommend both psychosocial evaluation and kidney transplant-specific education prior to listing. 1 A potential limitation with this approach is that patients may be on the waitlist for kidney transplantation for years or even decades 2 during which patients’ psychosocial and medical presentations could significantly change.
Adherence to medication and lifestyle self-management factors are associated with medical outcomes including acute rejection, posttransplant infections, poorer graft survival, increased medical costs, and mortality.3,4 Despite this, as many as one-quarter to one-third of kidney transplant recipients are insufficiently adherent with immunosuppressant medications 5 and similar proportions of dietary nonadherence have been reported. 6 Systematic reviews indicate improvements in adherence with intervention but recommend multicomponent interventions. 7 We hypothesized that enhanced pretransplant education and multidisciplinary evaluations shortly prior to transplant would improve adherence to medications and lifestyle-related recommendations posttransplant. Therefore, our program created a novel clinical protocol that included enhanced pretransplant education and multidisciplinary evaluation, implemented in a cohort of candidates and their primary supports as the patient neared transplantation. We compared the patients who participated in the novel clinical protocol to a cohort of kidney transplant recipients who received standard of care (SOC) on medical indicators of adherence to medications and lifestyle-related recommendations and associated hypothesized outcomes.
Design/Methods
Design
This is a retrospective cohort evaluation on a quality improvement initiative (implemented between November 2016 and March 2018) compared to a cohort of kidney transplant recipients receiving SOC (transplanted between January 2012 and December 2015). Data were collected with full Institutional Review Board approval (IRB#11187).
Methods
The novel clinical protocol, Countdown to Transplant Clinic (CTC), was developed by a multidisciplinary team for kidney candidates nearing transplant. The CTC's purpose was to ensure patients and their support systems were adequately prepared for the next steps in transplantation by (a) providing transplant lifestyle education and (b) identifying and ameliorating risk factors for negative outcomes in listed patients nearing kidney transplantation. The clinic was designed as a 4 hour half-day clinic with 2 elements: enhanced education and evaluations by social work, psychology, and nephrology. The enhanced educational session was taught by our Transplant Living CommunitySM team, 8 followed by a question-and-answer session with a transplant nurse coordinator, focused on preparedness, necessary lifestyle changes, and behavioral strategies for posttransplant adherence. Routine evaluations were performed by social work, psychology, and nephrology to confirm continued medical and psychiatric stability and confirmation of social supports. Patients were notified at the time of scheduling and via appointment letters that at least 2 of their support individuals were required to accompany them for the educational and social work evaluation portions. If a concern or change in eligibility was identified, the clinical team followed standard protocols to address said factor so the patient could continue to meet listing criteria and proceed to kidney transplantation. Additional materials for the intervention are included in Supplemental Tables A and B.
Setting
An outpatient clinic within a large, urban transplant center located in the Midwestern region of the United States. All transplant patients were seen at the main hospital transplant clinic.
Population
All adult patients listed and awaiting kidney transplantation. Patients are eligible for kidney transplantation if they are at least 18 years of age and undergoing renal replacement therapy for end-stage kidney disease or chronic kidney disease with creatinine clearance of ≤20 mL/min. Patients must also complete multidisciplinary evaluation and, based upon selection criteria, be approved for listing. The median wait time for transplant at our center is 44.4 months. Within the last 5 years, at our center, deceased donor kidney transplant recipients were: 68.4% Caucasian, 25.6% Black, 6% other; 55.6% male; primary kidney diseases include diabetes 26.4%, hypertension 25.0%, glomerular diseases 20.2%, polycystic 7.3%, and 21.1% other; with 97.8% 1-year graft survival and 97.3% 1-year patient survival.
Sampling
Candidates were identified for the CTC based upon offers of kidney transplantation. Once a listed patient receives an offer for a deceased donor kidney, whether or not they proceed on to receive the offered kidney, their name was added to an internal tracking system as they were expected to receive subsequent offers and be transplanted within the next few months. As soon as a candidate was added to this list, a nurse coordinator contacted the patient to schedule the patient and their supports for the CTC.
The control cohort was all patients who underwent kidney transplantation between January 1, 2012, and December 31, 2015, evaluated consistent with SOC guidelines. This included routine nephrology and social work evaluation at the time of evaluation for listing and yearly reevaluation with nephrology for continued listing.
Data Collection
Data collected across both groups included patient-reported demographics extracted from social work evaluations (ie, age at transplant, zip code, gender, marital status, race, and educational attainment), primary kidney disease, dialysis history, cardiac disease history, transplant date, and outcomes. Additional data for the CTC cohort included the date of CTC and changes in listing status. Outcomes explored included posttransplant laboratory values, hospitalizations within 30-days or 31 to 90 days posttransplant, biopsy-confirmed rejection within 1-year posttransplant, and mortality within 1-year posttransplant. Laboratory values included coefficient of variation (CV%) of all tacrolimus values 3 to 12 months posttransplant, and 30- and 90-day white blood cell (WBC) counts, potassium, and blood glucose (serum). Details regarding measurement, reasoning behind inclusion, and other additional information regarding exploratory outcomes are outlined in Supplemental Table C.
Data Analyses
Descriptive statistics are reported as mean (SD) or as median (interquartile range) for continuous variables based on distribution and as percentages for categorical variables. The means/medians of continuous variables were compared using either Student's t-tests or Wilcoxon's rank-sum tests, depending on data distribution. Categorical variables were analyzed using Fisher's exact or chi-square tests. For any missing values, either predictors or outcomes, we used the multiple imputation method by chained equations. Ten imputed data sets were created and used for these analyses. To account for confounding due to CTC selection bias, we used a propensity score modeling approach to estimate the inverse probability of treatment weight (IPTW). The IPTW was then adjusted in the subsequent analysis of the CTC impact on different outcomes.
Univariate and multivariate propensity score-weighted linear or logistic regression models were used to evaluate the association between CTC, SOC, and outcomes. Variables significant at P < 0.10 in the univariate analysis with the specific outcome were included in multivariate models. Estimates of predictors were reported as B(SE) for continuous outcomes (CV%, WBC, potassium, and glucose) and OR (95% CI) for binary outcomes (30 or 31-90 days posttransplant rehospitalization, biopsy-proven rejection, or mortality). Any P < .05 was statistically significant.
Procedure
A retrospective chart review was performed both manually (by authors RP, SB, SD, and KG) and via Structured Query Language extractions from the electronic medical records, then cross-referenced for accuracy.
Results
Between November 2016 and March 2018, 113 patients participated in the CTC and, as of November 2019, 75 (66.3%) received kidney transplants. The median time between CTC and transplant was 6.51 months (range 5 days to 24.54 months). Of the 38 who participated in the CTC but were not transplanted by November 2019, 12 (10.6%) were still listed, 15 (13.3%) placed on hold/delisted due to medical contraindications, 4 (3.5%) relocated/requested transfer to another center, 2 (1.8%) delisted due to loss of insurance, 2 (1.8%) expired, and 2 (1.8%) delisted due to newly emerged, intervention-resistant psychosocial contraindications. Baseline characteristics are reported in Table 1. Except for primary kidney disease, there were no significant baseline differences between groups.
Baseline and Posttransplant Patient Characteristics.
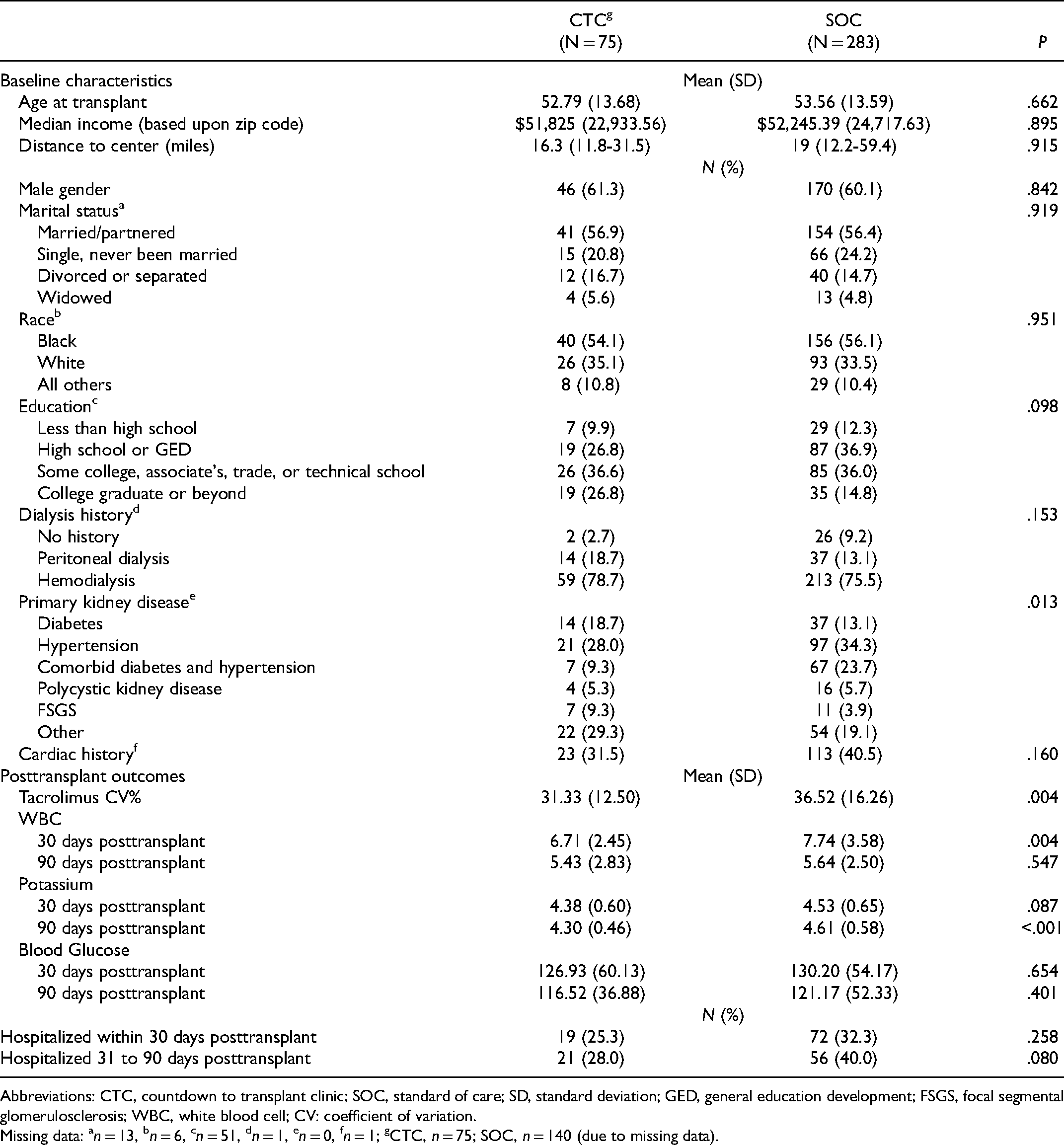
Abbreviations: CTC, countdown to transplant clinic; SOC, standard of care; SD, standard deviation; GED, general education development; FSGS, focal segmental glomerulosclerosis; WBC, white blood cell; CV: coefficient of variation.
Missing data: an = 13, bn = 6, cn = 51, dn = 1, en = 0, fn = 1; gCTC, n = 75; SOC, n = 140 (due to missing data).
As reported in Tables 2 and 3, participation in the CTC was statistically associated with lower CV%, 30-day WBC count (but not 90-day WBC), 90-day potassium levels (30-day potassium trended towards significance), and 30- and 90-day hospitalization rates, even when other factors were entered into models that could impact outcomes (eg, income and age). No comparisons were made across cohorts on biopsy-confirmed rejection or mortality, as there were not enough in the CTC cohort (1 and 5, respectively) for statistically meaningful comparisons. Tables 2 and 3 display the variables retained for inclusion in the models. For CV% of serum tacrolimus, receiving SOC (vs CTC) and significant cardiac history was associated with a higher CV%. For WBC counts, SOC (vs CTC), younger age at transplant, and being single/never married (compared to partnered/married) were associated with higher 30-days posttransplant WBC counts. Being identified as Black (compared to White) and polycystic kidney disease (compared to diabetes) predicted higher 90-day WBC counts, but the cohort was no longer significant. None of the predictors were significant in the model for potassium at 30-days posttransplant (data not shown). However, SOC (vs CTC) and being divorced/separated (vs married/partnered) predicted higher 90-day posttransplant potassium levels. Condition (CTC vs SOC) was not significant in either model examining posttransplant serum glucose.
Multivariate Linear Regression Model Estimates.
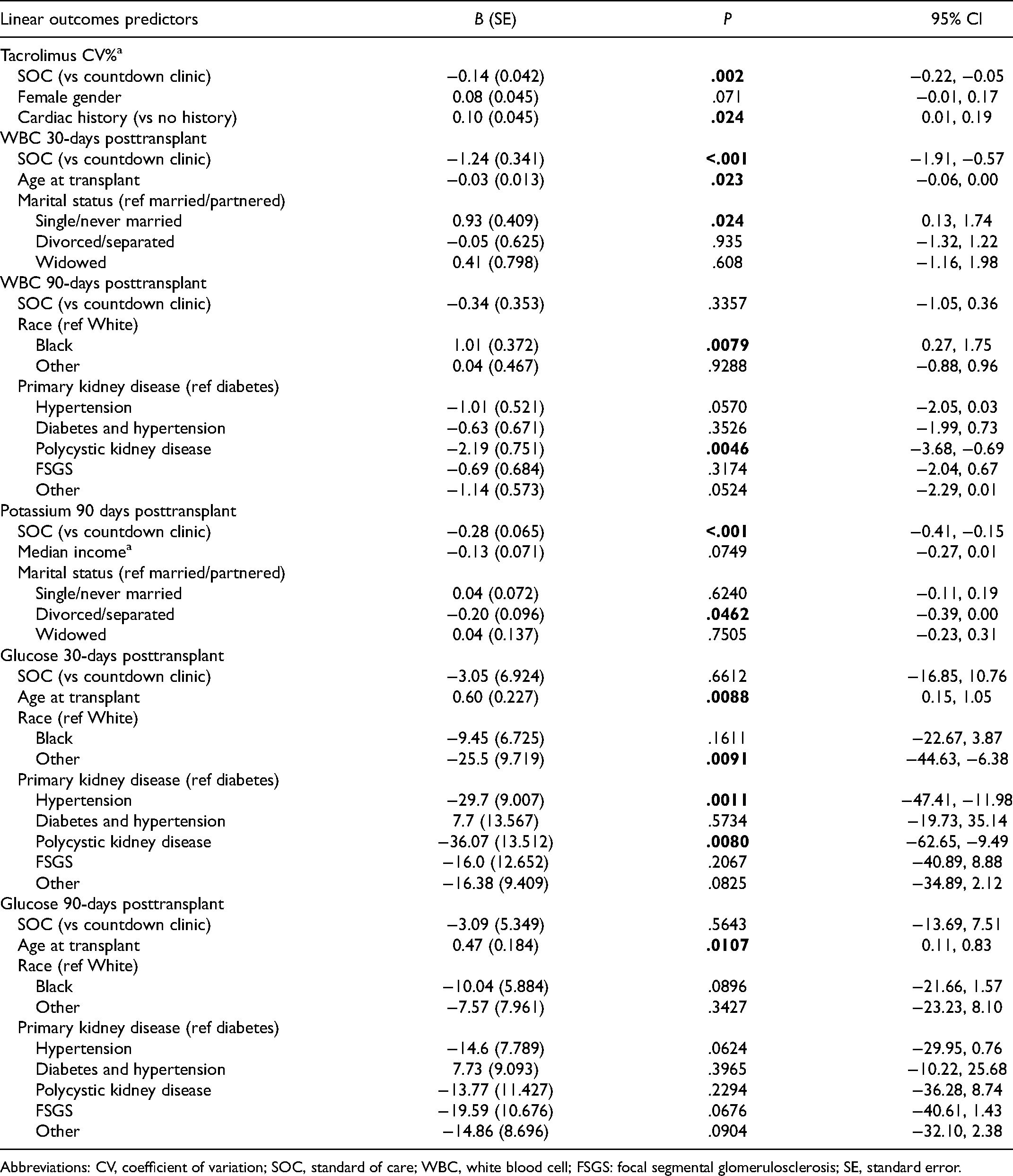
Abbreviations: CV, coefficient of variation; SOC, standard of care; WBC, white blood cell; FSGS: focal segmental glomerulosclerosis; SE, standard error.
Multivariate Logistic Regression Model Estimates for 30- and 90-day Hospitalization.
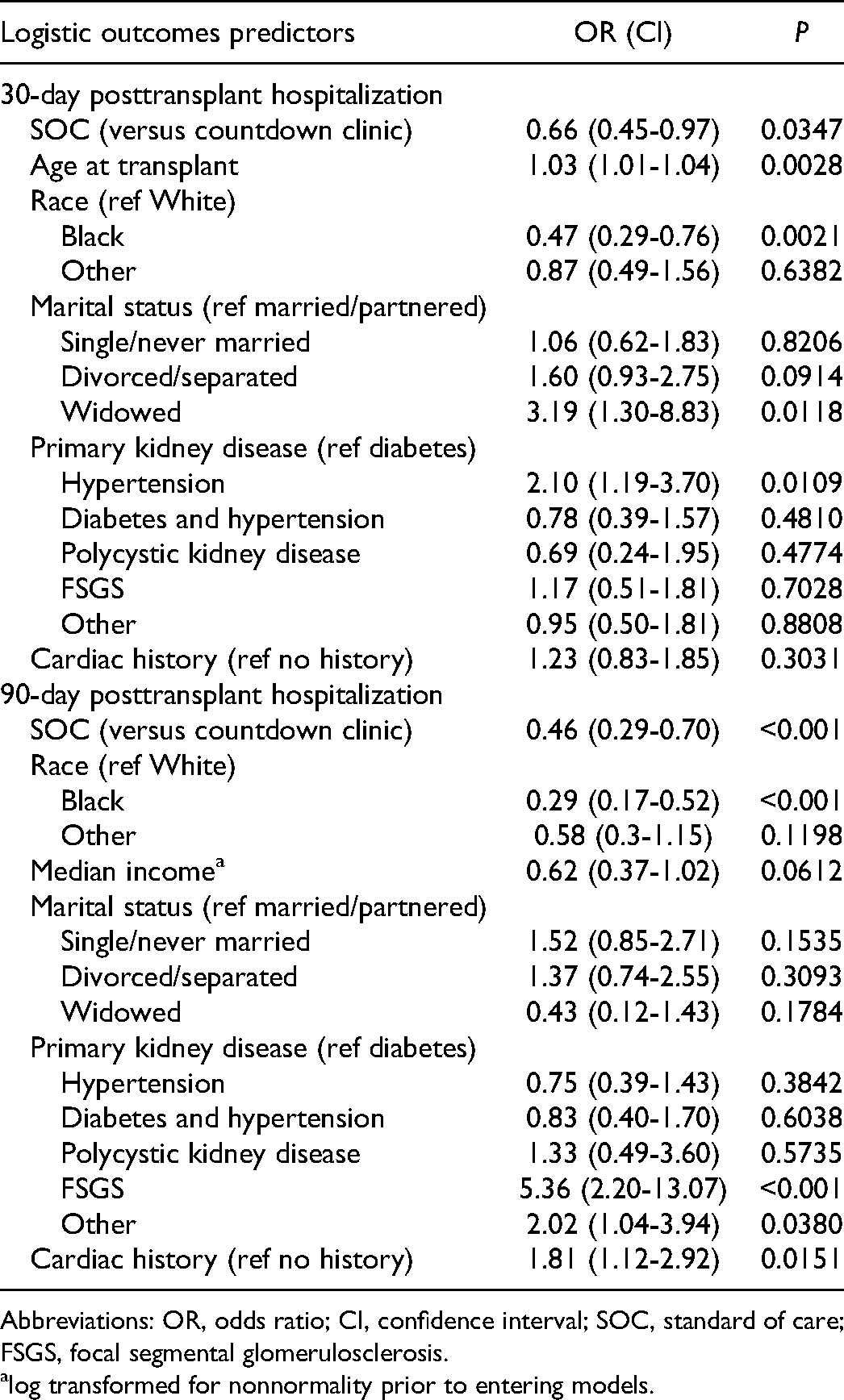
Abbreviations: OR, odds ratio; CI, confidence interval; SOC, standard of care; FSGS, focal segmental glomerulosclerosis.
log transformed for nonnormality prior to entering models.
For 30-day posttransplant rehospitalizations, SOC (vs CTC), older age at transplant, white race (vs Black), widowed (vs married/partnered), and hypertension (vs diabetes) predicted a greater likelihood of rehospitalization within 30 days of transplantation. Similarly, SOC (vs CTC), white race (vs Black), primary kidney disease of focal segmental glomerulosclerosis (FSTS) or other (vs diabetes), and a significant cardiac history predicted rehospitalization within 31 to 90 days posttransplant.
Discussion
An ongoing question in organ transplantation is how to best prepare candidates for transplantation to optimize patient outcomes. Participation in a pretransplant, multidisciplinary education, and evaluation clinic aimed at identifying and ameliorating risks for negative outcomes may improve behaviors related to medication and lifestyle adherence. Specifically, participation in the CTC was associated with lower CV% in serum tacrolimus 3- to 12-months postkidney transplantation, lower serum potassium 90-days posttransplant, and lower rehospitalization rates within 3-months posttransplant. While we cannot pinpoint which aspects of the intervention were the most impactful, this provides preliminary support for implementing larger, controlled trials of interventions in the period preceding kidney transplantation.
Although the model examining day 30 potassium levels was not significant, participation in the CTC and not being divorced/separated versus married/partnered were related to lower 90-day potassium levels. However, posttransplant medications may act as a confounding variable on potassium levels, and thus whether education and resources regarding dietary recommendation increase adherence to dietary recommendations warrant further exploration.
Participation in the CTC did not significantly impact blood glucose at 30- or 90-days posttransplant. Even when patients are adherent to endocrinological recommendations, glycemic control posttransplant is complicated and can be impacted by steroids and calcineurin inhibitors. Alternatively, hospital readmissions are an important health care quality measure. A previously published literature suggests high rates of rehospitalized postkidney transplantation. 9 For hospitalizations within 30-days and 31 to 60-days posttransplant, participation in the CTC may have lowered this risk. As other authors have noted, factors impacting hospital readmissions in chronic kidney disease and kidney transplant are not adequately understood but multicomponent interventions, such as this one, have the potential to reduce hospital readmissions. 9
There are several limitations. First, this was not a randomized controlled trial (RCT); although sophisticated modeling approaches (ie, IPTW) were applied to closer approximate effect sizes across groups in observational studies. To infer effects more accurately, fully powered RCTs are needed along with multimethod assessments including medication event monitoring. Furthermore, the multicomponent nature of the intervention makes it unclear what components were the most impactful. Novel methodologies may permit comparisons across and between individual components of multicomponent interventions that should be considered when applicable. Lastly, the direct, objective measurement will be important in the future examination as outcomes collected were largely proxies, albeit with empirical relationships to behaviors. Future research is needed with prospective, RCTs, with representative and concurrent samples of kidney transplant candidates and their supports, across multiple centers, examining and controlling for different components of the intervention.
Conclusions
Participation in a pretransplant, multidisciplinary education, and evaluation may improve posttransplant outcomes. The next steps include pilot testing small, randomized trials to determine the power and feasibility of recruitment. However, prospective, fully powered RCTs using factorial designs are recommended to parse out the unique effects of education from individual evaluations.
Supplemental Material
sj-docx-1-pit-10.1177_15269248211064888 - Supplemental material for Prerenal Transplant Education and Evaluation Positively Impacts Outcomes
Supplemental material, sj-docx-1-pit-10.1177_15269248211064888 for Prerenal Transplant Education and Evaluation Positively Impacts Outcomes by Michelle T. Jesse, Erin Clifton and Dean Y. Kim, Dayna Nicholson, Rujuta Patil, Shweta Bhavsar, Soham Desai, Kendyll Gartrelle, Anne Eshelman, Elizabeth Fleagle, Brian Ahmedani, Noelle E. Carlozzi, Amy Tang, Anita Patel in Progress in Transplantation
Supplemental Material
sj-docx-2-pit-10.1177_15269248211064888 - Supplemental material for Prerenal Transplant Education and Evaluation Positively Impacts Outcomes
Supplemental material, sj-docx-2-pit-10.1177_15269248211064888 for Prerenal Transplant Education and Evaluation Positively Impacts Outcomes by Michelle T. Jesse, Erin Clifton and Dean Y. Kim, Dayna Nicholson, Rujuta Patil, Shweta Bhavsar, Soham Desai, Kendyll Gartrelle, Anne Eshelman, Elizabeth Fleagle, Brian Ahmedani, Noelle E. Carlozzi, Amy Tang, Anita Patel in Progress in Transplantation
Supplemental Material
sj-docx-3-pit-10.1177_15269248211064888 - Supplemental material for Prerenal Transplant Education and Evaluation Positively Impacts Outcomes
Supplemental material, sj-docx-3-pit-10.1177_15269248211064888 for Prerenal Transplant Education and Evaluation Positively Impacts Outcomes by Michelle T. Jesse, Erin Clifton and Dean Y. Kim, Dayna Nicholson, Rujuta Patil, Shweta Bhavsar, Soham Desai, Kendyll Gartrelle, Anne Eshelman, Elizabeth Fleagle, Brian Ahmedani, Noelle E. Carlozzi, Amy Tang, Anita Patel in Progress in Transplantation
Footnotes
Author Contributions
MTJ participated in the research concept and design, the performance of the research, data analysis, and interpretation, and writing of the paper. EC, DYK, DN, AE, and AP participated in research concept and design, the performance of the research, and critically reviewed the article. RP, SB, SD, KG, and EF participated in the performance of the research, data analyses, and writing of the article. BA, NC, and AT participated in the data analysis and interpretation and critically reviewed the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.