
Abstract
Liver transplantation offers a life-saving option for those with liver cirrhosis, but it is associated with significant healthcare costs with some reports estimating the average cost of hospitalization as high as $878,400. 1 Acute on chronic liver failure (ACLF) describes a syndrome characterized by rapid deterioration in liver function associated with extrahepatic organ failures and high mortality without transplantation. Transplantation is recognized to confer a survival benefit in ACLF. The European Association for the Study of the Liver-Chronic Liver Failure (EASL-CLIF) criteria grades ACLF by 3 levels of increasing severity. Higher levels are associated with a complicated posttransplant course and increased healthcare utilization. 2 Due to limited resources, transplant centers face pressure to allocate resources in a manner that is both economical and ethical, an effort complicated by payment models that disincentivize offering transplantation to those who incur higher costs. To date, little research has been done investigating the economic impact in the ACLF population.
We performed a single center, retrospective cost of illness analysis describing a cohort of patients 18 years or older who underwent deceased donor liver transplant from January 2017 to June 2019 for ACLF, defined by the EASL-CLIF criteria. Exclusion criteria included living donor recipients, multiorgan transplants, and re-transplants.
Patient information including demographics, clinical characteristics, 30/90-day readmissions, liver transplantation outcomes, direct costs (including fixed and variable expenses), and length of stay (LOS) are summarized in
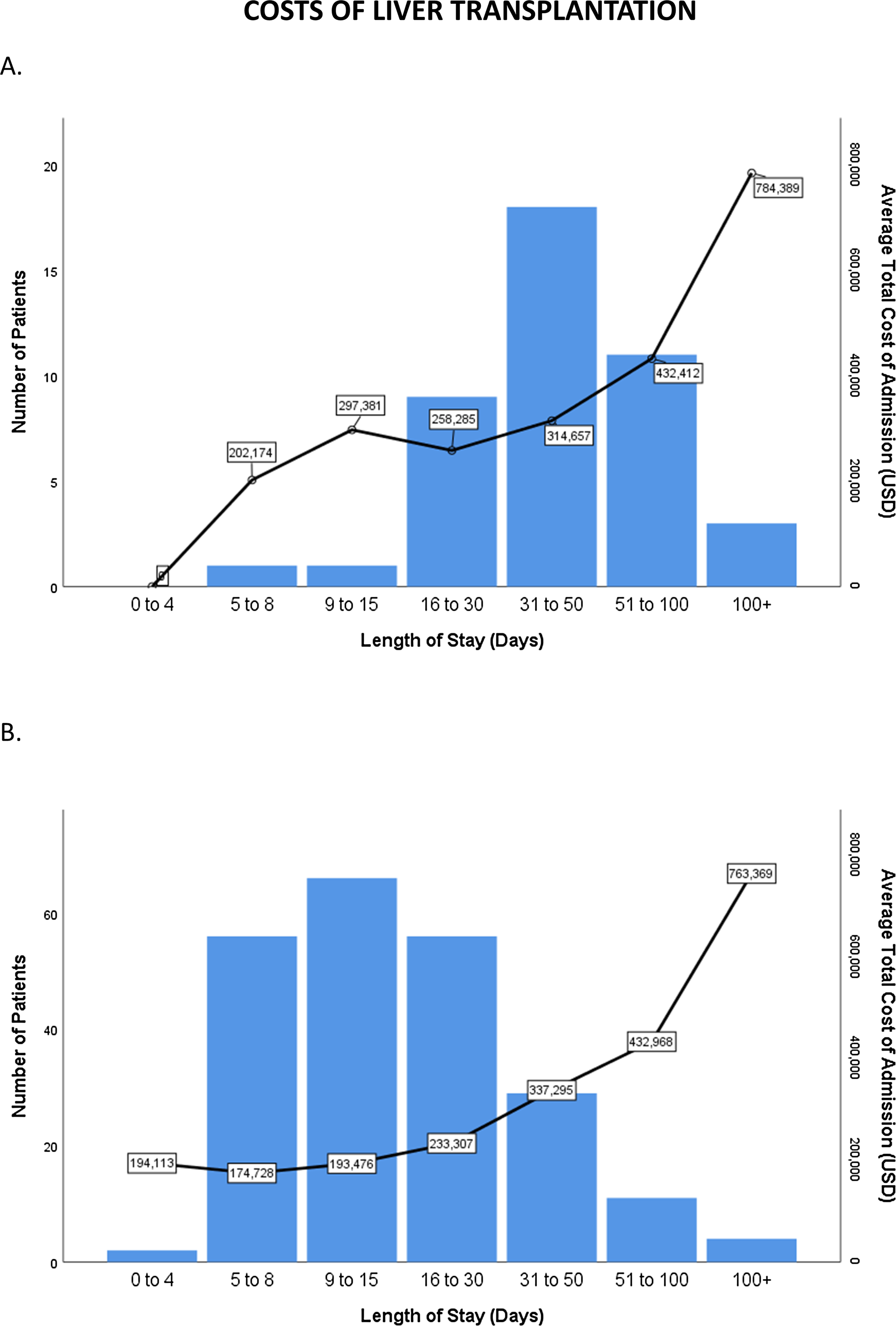
Costs of liver transplantation. (A) Cirrhosis with acute on chronic liver failure. (B) Cirrhosis without acute on chronic liver failure.
Comparison of Demographics, Outcomes, and Costs in Acute on Chronic Liver Failure Versus Non-Acute on Chronic Liver Failure Transplants.
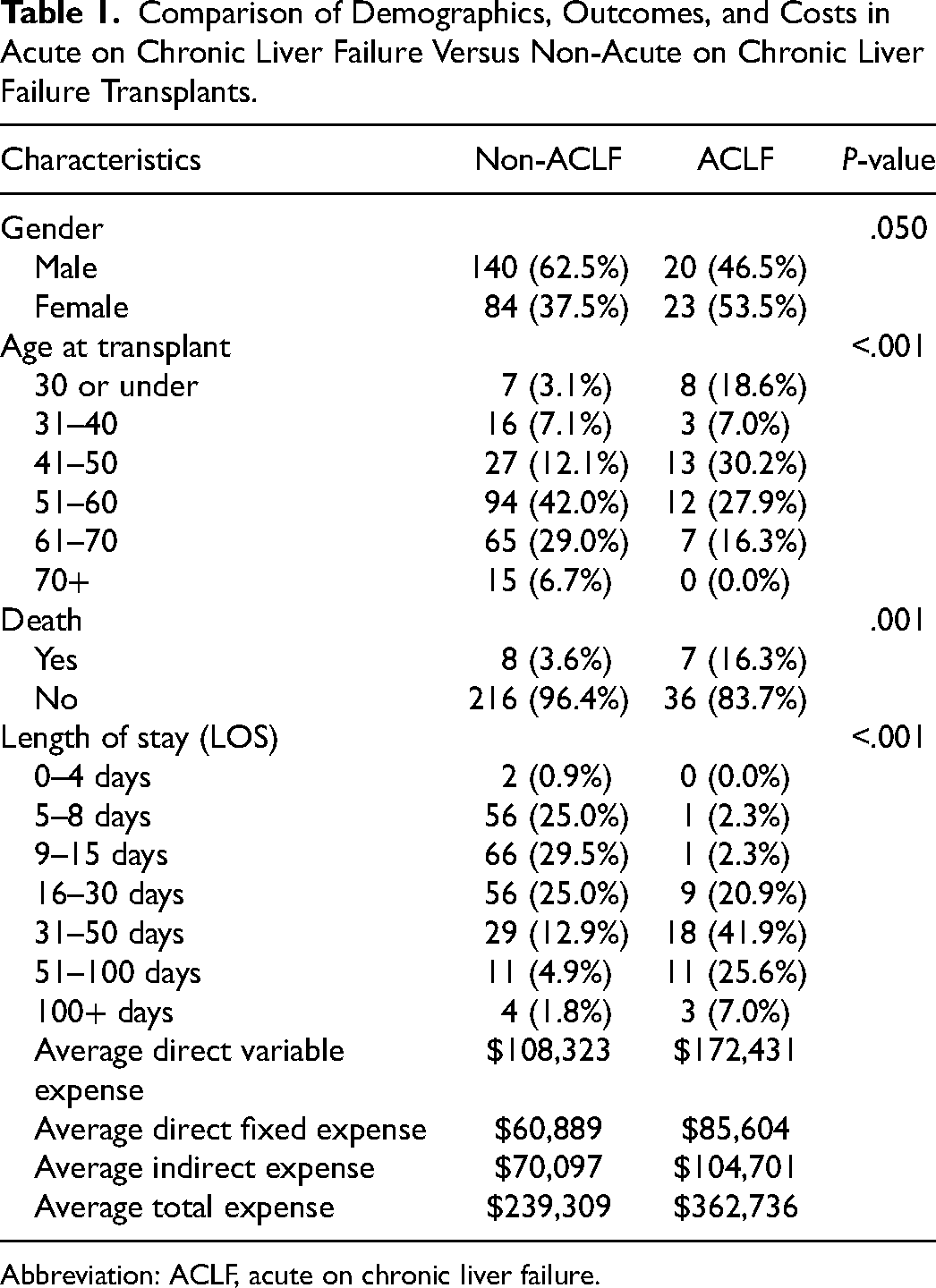
Abbreviation: ACLF, acute on chronic liver failure.
Our exploratory pilot described transplant-care expenditures in patients with ACLF, increasingly recognized as an acceptable indication for liver transplantation. The location of our transplant center in Maryland, USA, which utilizes a reimbursement model charging payers fixed rates for services, 3 provides a preview of “payment bundling” initiatives being considered for wider implementation. It is important to note that such payment models may affect the willingness of transplant centers to provide liver transplantation to the sickest cohort who are in the direst need of transplantation but also incur the highest costs. Value-based payments linking costs to outcomes are an emerging trend and predicting transplant costs a priori would lead to a transparent, informed and negotiated discussion between transplant centers and payers. We hope that future studies providing in-depth analyses of both transplant expenditures and outcomes in ACLF will result in cost-conscious, equitable and inclusive policies.