
Abstract
Despite institutional claims that social justice is a core professional nursing value, efforts to fulfill this claim remain uneven. The purpose of this study was to examine the circumstances that shape nursing educators' approaches to social justice. In-depth semi-structured interviews with 28 educators teaching theory courses in baccalaureate nursing programs shed light upon the influences that shape how educators integrate social justice. These include formative experiences, institutional factors, and curricular opportunities. Formative experiences include upbringing, educational background, and preparation to teach. Institutional factors consist of the type of institution, geographic location, and the specter of retention, promotion, and tenure. Finally, curricular opportunities and fit include the positioning of Community Health Nursing, fragmentation and tension between “content and context,” and the “driving force” of the National Council Licensure Examination for Registered Nurses (NCLEX). Findings indicate that the capacity to uphold the value of social justice is shaped by experiences across the lifespan, institutional policies, and practices related to faculty hiring, development, career advancement, as well as curricular vision. This study calls for a concerted effort to enact social justice nursing education.
Introduction
There is no shortage of evidence that preventable and unfair negative health outcomes exist along the lines of socially constructed differences, including race, ethnicity, ability, religion, gender, indigeneity, and immigration status (Agency for Healthcare Research and Quality, 2014; Baciu, Negussie, Geller, Weinstein, & National Academies of Sciences, Engineering, and Medicine, 2017). As nursing education is a pillar of the largest segment of the health care workforce, a critical examination of how nursing programs approach social justice is necessary. The degree to which institutions of nursing education approach health equity shapes the manner in which nurses across all settings and specialties facilitate, perpetuate, resist, or transform health inequities. While the American Association of Colleges of Nursing (AACN) identifies social justice as a core nursing value and the pursuit of health equity is an overarching goal of Healthy People 2020 (United States Department of Health and Human Services, Office of Disease Prevention and Health Promotion, 2010) and Healthy People 2030 (United States Department of Health and Human Services, Office of Disease Prevention and Health Promotion, 2019), these remain inconsistently integrated across foundational American Nurses Association documents (Bekemeier & Butterfield, 2005; Valderama-Wallace, 2017). While the Code of Ethics is the most robust with a call to nurses, through professional organizations, to “address unjust systems and social structures,” (American Nurses Association, 2015, p. 36). Generally speaking, however, the Scope and Standards of Practice and Social Policy Statement emphasize nursing autonomy and professionalism, the primacy of individual patient–nurse interactions, and champion interprofessional collaboration (Valderama-Wallace, 2017). The interrogation of existing power dynamics in nursing education is largely absent.
Nursing Education and Social Justice
The AACN (2013) established accreditation standards and core curricular elements based on recommendations from the Institute of Medicine's Future of Nursing Report. The generalist Essentials of Baccalaureate Education for Professional Nursing Practice (AACN, 2008) outlines nine essentials. Here, social justice, human dignity, altruism, and integrity are identified as core values critical to nursing and eliminating health disparities. There are distinct approaches and power dynamics involved with each and they are not aligned. More recently, AACN released the Position Statement on Diversity, Inclusion, and Equity in Academic Nursing, which asserts that necessary actions include a thorough review of admissions processes, leadership to examine conscious and unconscious bias, partnerships with community leaders, and mechanisms to address healthcare inequities (Huerta, 2017). Likewise, the current research priorities of the National League for Nursing and National Institute of Nursing Research call for greater knowledge about effective teaching strategies related to social determinants of health and the “integration of differences based on genomics, sex, ethnicity, age, gender, and other aspects of diversity in educational approaches” (National League for Nursing, 2016, p. 3). Several scholars (Drevdahl, Kneipp, Canales, & Dorcy, 2001; Thurman & Pfitzinger-Lippe, 2017) have called for greater sustained commitment to social justice in nursing, situating this value within the origins of nursing.
The underlying epistemological, ontological, and axiological stances to nursing education are seldom unnamed. The positivist stance embodied within the prevailing contemporary epidemiologic approach of the biomedical model is not unnamed as such in nursing's foundational documents but is the dominant model nonetheless. Discussion of indigenous peoples and indigenous knowledge is rarely addressed by nurse scholars in the United States, with the exception of an examination of indigenous epistemologies and general lack of understanding of “indigenous ways of knowing,” (Boutain, 2008, p. 243). McGibbon, Mulaudzi, Didham, Barton, and Sochan (2014) and Green (2016) communicate the urgent need for the decolonization of the nursing profession that is maintained by White privilege and racism in nursing and manifested in the very fragmentation of curricula into discrete positive units with boundaries and expectations about which topics are important and where concepts belong. Postcolonial nursing scholars' work builds from growing postcolonial feminist literature in nursing, which include myriad lenses through which we examine how colonial history and violence shape present-day phenomena, including the political, intellectual, geographical, cultural, linguistic, psychological, and economic hold of neocolonialism.
Theoretical Framework and Conceptual Relationships
The theoretical approach for this study was informed by social constructionism and critical social theory. This theoretical approach assumes that our understanding of reality emerges from human interaction, rather than being grounded in biology or genetics, which is an assumption of essentialism (Ore, 2008). When difference is infused with pervasive hierarchy, exploring dynamics of domination and subordination can aid in the understanding of how power shapes the stratification of labor, assumed behavioral norms, focus on survival, and understanding of self. The purpose of critical social theory, particularly in education, is the critique of “oppressive social arrangements” (Leonardo, 2004, p. 11) and use of transcendent language and theoretical exposition to create knowledge that is emancipatory. An essential aspect of this process is facing social inequality and putting forth critical questions to examine such problems with nuance and complexity.
Approaches that focus on diversity generally emphasize sociocultural differences and commonalities among various groups based on ethnic, gender, racial, class, or other categories upheld in the United States (Adams & Zuñiga, 2016). Efforts that focus on diversity and inclusion can do so without including issues of inequality or justice. Social justice approaches, on the other hand, focus on the ways in which social group differences interact with systems of power and oppression to maintain stratification of various social groups. The theory, goal, and process of social justice require genuine belief and valuing of diversity in order to dismantle the systems that advantage or disadvantage members of social groups (Bell & Adams, 2016). As the foundational documents of nursing strongly emphasize the professionalism of nurses, it is important to note that this claim to power and status indicates a tension with social justice. Shirley and Padgett (2006) describe how the discourse of professionalism serves as an occupation's claim to status and an evolving means of organizing relationships around collective interest and the public good.
Nurse educators are uniquely positioned to facilitate the nursing education of future nurses and assume leadership positions in programs, schools, and professional organizations that oversee nursing education. There is a dearth of information about the mechanisms and factors influencing the integration of social justice in nursing education. The purpose of this study was to better understand the circumstances that shape educators' approaches to social justice in nonpracticum courses in Baccalaureate nursing programs. Such an examination of faculty perspectives can reveal the landscape of current and needed policies, practices, and research.
Methods
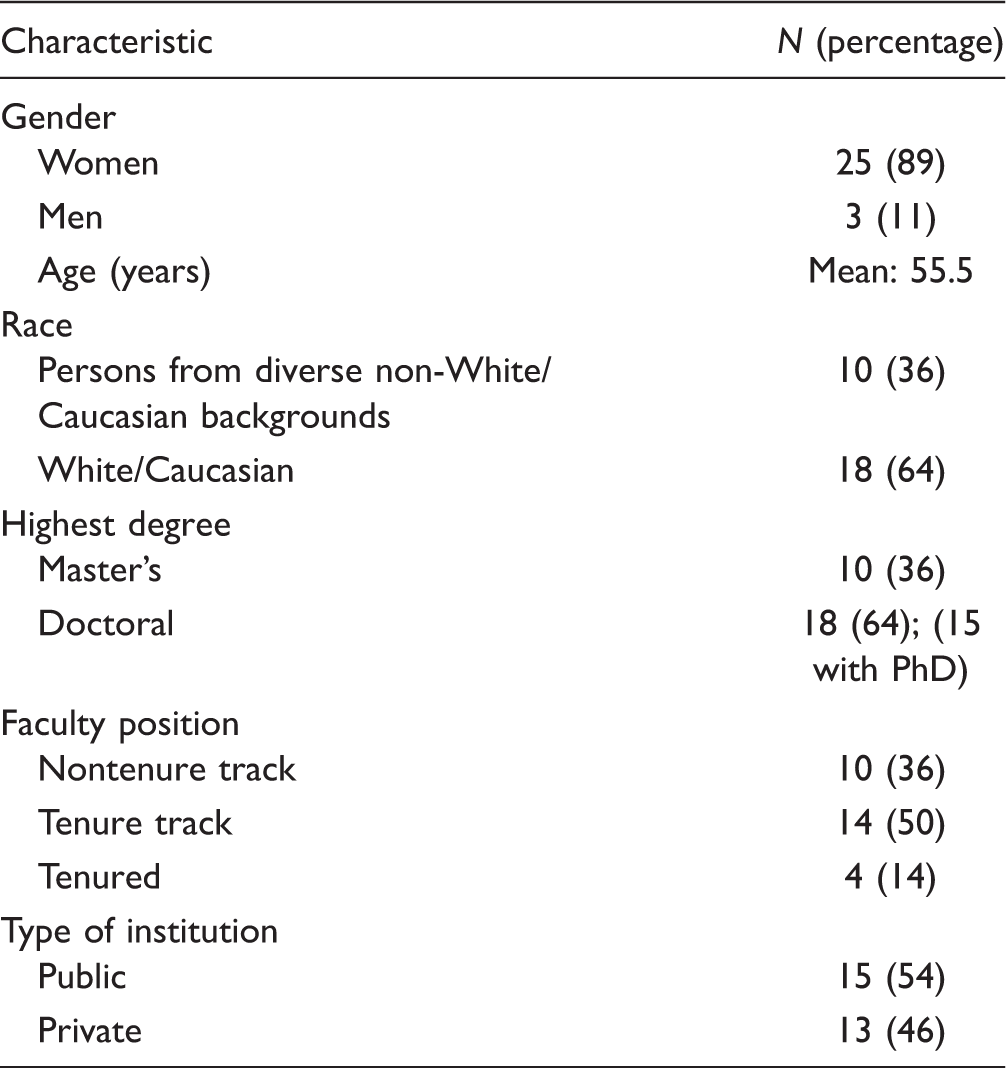
Participants' Characteristics.
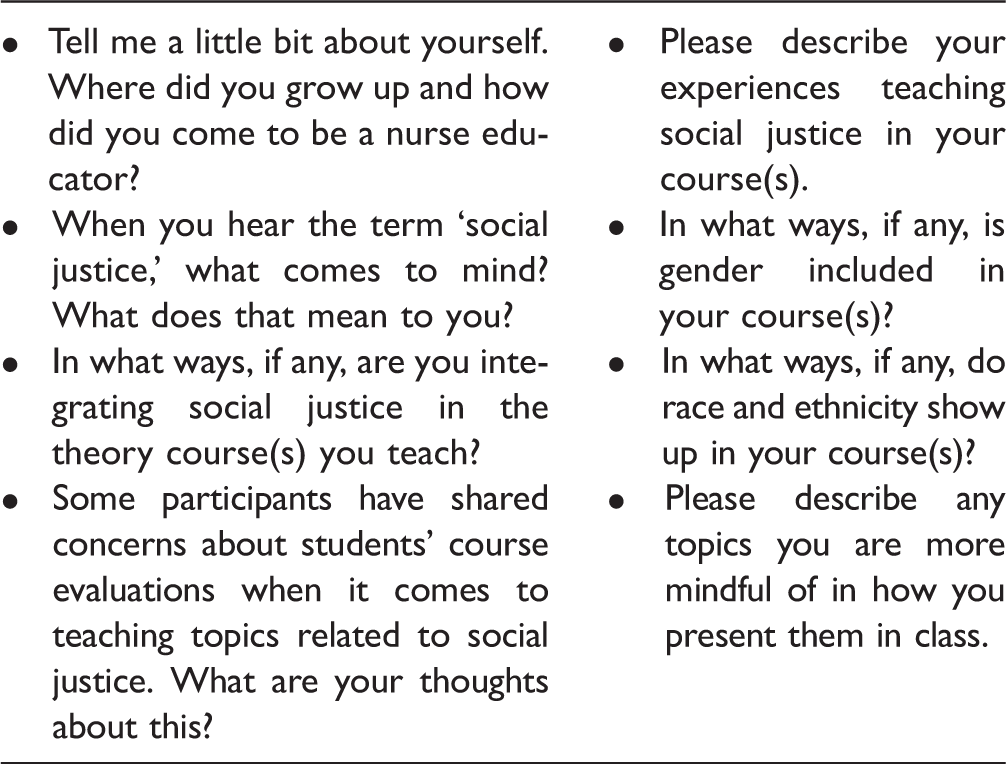
Selection of Interview Guide Questions.
My efforts to examine and explain the data collected from the 28 interviews followed the iterative process described by Charmaz (2014). A constant comparative method allowed for the examination of new data in relation to existing data. Interpretation of responses required that I bracket my views about social justice and my teaching philosophy and pedagogy. While my positionality informed initial thoughts and reactions to participants' responses, my awareness of them allowed me to prioritize the purpose of my study.
Results
The mean age of the participants was 55.5 years and the vast majority of participants identified as women (89%). Faculty of color comprised 36% of the sample and most participants have a doctoral degree (64%). Participants held various positions including nontenure track (36%), tenure track (50%), and tenured (14%). Finally, slightly more than half (54%) were teaching at a public institution at the time of our interview.
Influences that shape how nurse educators teach social justice in their theory courses fit within three broad conceptual categories: (a) formative experiences such as childhood, education, and preparation to teach; (b) the institutional context in relation to nursing leadership, geography, and institutional factors; and (c) curricular opportunities such as the positioning of Community Health Nursing, separation of content and context, and the NCLEX.
Formative Experiences
Upbringing and othering
Several participants who described intentional integration of social justice attributed this, at least in part, to their youth and upbringing. Those conceptualizing social justice as taking action and righting wrongs spoke of parents who were involved in the civil rights movement, brought them to marches, and discussed civil rights leaders at home. A number referred to books they read as adolescents such as The Jungle (Sinclair, 1985) and Bury My Heart at Wounded Knee (Brown, 1970). Participants also spoke of socioeconomic, racial, and ethnic dimensions of the communities in which they grew up. They also described experiences as immigrants or refugees or as the children of immigrants or refugees. Experiences of othering were salient influences. Most who conceptualized social justice as action described how they have faced racism, xenophobia, sexism, classism, homophobia, and other forms of oppression throughout their lives, including the institutionalized discrimination they navigate as faculty.
Most White participants, several of whom moved to the West Coast from the Midwest, described living in homogenous neighborhoods with few speaking of being othered in relation to economic status and gender. Othering among White participants was primarily about experiencing racialization and, to a lesser degree, experiences of being members of working class families. Such experiences have led participants to consider naming White privilege in their courses in addition to highlighting marginalization by socioeconomic status. Many also spoke of gendered family and societal expectations of occupations available to them but not to the extent of racial segregation. Several spoke of the options of becoming a nurse, teacher, or nun but falling in love with nursing. Interestingly, few said that gender showed up in their courses and how they teach, despite the occupation being very gendered. Most non-White participants spoke of their migration to the United States, their current locations on the west coast, or that of their parents. Their responses captured dimensions of navigating experiences of othering. One participant who migrated to the United States said: My mom's a single mom. Even though she spoke English and had an education, she wasn't licensed here. She took minimum paid jobs. I was aware of being different. She stood up there looking at the board and she reads patients' names, “Lawanda, Lashanda,” you know, “Laqueesha … ” She handpicked them and said, “What happened to giving kids normal names,” right? For someone who's grown up with a foreign name, and told to change my name countless times like I'm highly sensitive. I was so stunned.
A Latina participant expressed concerns about the need for greater awareness about pathways to nursing among high school career counselors based on her own career trajectory: I didn't really have any guidance so I took a medical assisting course that was expensive, not knowing I could go straight into nursing. It took me seven years to get into the ADN program then I got my BSN. Years later I got a Masters and about ten years after that I started the PhD program. There's a lot of us like that. The guidance we didn't have.
Many White participants, on the other hand, communicated conditions of housing segregation and insulation from non-White and nonmiddle-class lived experiences. One stated, “I grew up in a predominantly White affluent private school environment, from, you know, all the way until I was 18.” Another participant described having grown up in a homogenous area: “Where I grew up, it was primarily um probably the majority of people were White and I think the other minorities were East Indian or Chinese.” Yet another spoke in a reflective manner: My mom was an immigrant, she always felt like an outsider, but you know she was still White. We were the only kids with free lunches, you know, and they tried to put us all in special education. So I definitely feel like I have a taste of that.
The few exceptions to isolation and segregation experienced by participants who identified as White were attributed to parental political stance or growing up in a multiracial family. One woman said: I grew up in a predominantly African-American community. We were one of two or three White families in the neighborhood. I was pretty much the only White kid in the class and that was on purpose. My parents were really into integration and social justice kinds of things so they purposely moved us into that neighborhood to sort of walk the walk. I'm very White. You know I look that way to people and I have heard White people say things to me that used to completely blow me away. It took me a long time to kind of get my bearings around that. I have confronted that in nursing and I've seen it in nursing, I've seen it in practitioners with their assumptions about populations they're caring for.
Educational background
Participants' educational backgrounds also influenced their approaches. Slightly more White faculty (76%) than diverse faculty of color (70%) studied nursing exclusively. Seven participants (25%) reported studying a nonnursing discipline in addition to nursing and those who studied social sciences or humanities were more likely to emphasize social context, situate nursing's theoretical approaches as one among others, and identify the influence of classroom power dynamics on learning. Those who studied nursing exclusively were more likely to emphasize building empathy, increasing awareness of differences and focusing on content. One participant who teaches various BSN courses stated: I think psych departments do a much better job—when we talked about it in Peds, we talked about, ‘Here are the stages and then you become independent and then you move out of your parents’ house’ and I was thinking, wow, that's so culturally based because everyone doesn't [emphasis added] move out of their parents’ house and sometimes your spouse moves into your parents’ house, right? I think we do a shit job of reminding ourselves to include the Humanities in nursing. I think that it is so important to get our students to remember that there is outside the hospital, outside of nursing, that there is outside the box. [emphasis added] Sometimes the only [emphasis added] way you do that is through being exposed to things like gender theory, art, and culture different from your own. We lack and undervalue [emphasis added] it in nursing, because we say there's not time for it, it's not on the NCLEX.
Preparation to teach
Nearly all participants spoke of their “sink or swim” circumstances when assuming faculty roles. Those who completed a doctoral degree in education communicated their desire to learn how to become educators. Those with a master's degree in Nursing Education also expressed comfort with developing learning objectives, teaching methods, and assessment. A line of demarcation based on the constructs of race and ethnicity emerged. White participants who did not pursue graduate degrees in programs focused on education largely spoke of learning on the job and doing their best while diverse participants of color spoke of support, belonging, and mentorship from colleagues in other departments or at other institutions as well as ethnic-specific or “minority”-specific professional organizations for underrepresented nurses. Topics discussed among trusted colleagues included pedagogy, navigating department politics, and tenure. Another participant, despite having experience teaching test preparation, reflected and stated that, “Nobody thought to stop and say, ‘Wait a minute, is this really something this person can handle?’ If I hadn't had the training, I would’ve crashed and burned.”
Participants spoke of inheriting syllabi and PowerPoints and the norm of teaching immediately without coteaching or some form of preceptorship with a reduced course load. Few received a doctoral degree in education and several spoke of nursing education courses being largely limited to master's programs, although the course content and takeaways from these were described as forgettable. Findings highlight invisible labor of diverse faculty of color as well as those with teaching experience and familiarity with assessment, evaluation, and curriculum development. One participant who described how she “loves curriculum” stated: You listen to a lot of nurse educators. They hate curriculum and they just want to teach. They just know what they know, their own specialty areas and just like, “Leave me alone.” I wonder sometimes if that's a function of not really having been formally prepared to be educators. I spend a fair amount of time educating not only the general faculty but even curriculum committee members on curriculum and what it means.
Another participant who teaches Med-Surg spoke of pedagogical development: We're so focused on, “Here's the way the body works. Here's the right way to take care of it. Here's the right medicine to get them.” You know—it's much more concrete [emphasis added] what we teach, and so the ability to guide a discussion … We're not so good at that because we don't have that practice. The way we educate our nurses is we say, “Hey, you're a good nurse. Let's put you in a hospital and you can teach students how to be a good nurse,” as opposed to this is college. Let's open up their minds.
Some participants characterized teaching as a “natural” component of nursing. One, in particular, said, “We all get how to do patient teaching. Every nurse is a teacher and it's true.” This conflation of beside nursing with teaching baccalaureate level courses was expressed only by faculty who teach Med-Surg and Pathophysiology. This suggests that policies and intentional practice of nursing education, higher education, and preparation to teach do not merit attention and commitment. Institutional dimensions also emerged among many participants' comments.
Institutional Context
Nursing leadership
Several spoke of gatekeeping, inconsistency and inaction by various nursing organizations, associations, and regulatory bodies. A number situated their efforts as priorities despite perceived silence from nursing leadership. One participant of color teaching at a public university described seeking a doctoral degree in large part because a PhD is “more recognized and not questioned.” This participant voiced frustration about the lack of prioritization of social justice in the manner in which nurse leaders have established priorities. White women are still spinning in their own circle. I don't know how they prioritize what they're willing to take on and what they feel is important. I try to go into those spaces and voice opposition to some of the nonsense then I get discouraged because they just go around and around. We're not making any kind of movement or progress. In this profession, you've got to find your allies and work and let the bigger group of folks do what they do. They've been spinning their wheels for over 35 years, I'm sure they're going to keep spinning. I'm telling you but I wouldn't tell my students this.
White and Asian faculty teaching various courses apart from Community Health Nursing were more likely to describe the role of the Board of Registered Nursing (BRN), AACN, and accrediting bodies as guides to follow. Most non-Asian faculty of color questioned the lack of “walking the walk” among organizations and bodies that oversee and shape nursing. Faculty teaching courses other than Pathophysiology, Pharmacology, and Medical-Surgical were more likely to mention inaction of nursing leadership.
As one participant put it, advancing the nursing profession would mean that social justice would be a “prime priority” with acknowledgement that “there's so much we could do as a profession.” Another participant spoke of the need to integrate social justice into one's nursing identity development. Only two mentioned the ANA's Code of Ethics, including this faculty: The ANA put out some report, “We're so much more diverse than we were.” We're less White, which is good, but they're not really looking at the lens. I mean African American enrollment is down but I don't see ANA thinking that's gonna be a crisis. I'm glad they're paying attention to access to care but to move the needle? We have a lot of work [emphasis added]. We're good about preaching social justice and putting it in our Code of Ethics, but we don't walk that walk. If we did, our ANA leadership would reflect it.
Geographic location and type of institution
The influence of geography and type of institution informed the degree to which participants included different social justice concerns. I routinely asked, “How does gender show up in your course or in the classroom?” Most responded that gender has not really been an issue because most students have been women or that nursing textbooks have improved their inclusion of male and female pronouns when describing nurses. One responded, “The transgender piece has just begun, I think, filtering into our consciousness,” attributing this to the patient population in a rural area.
Student discomfort with topics related to gender identity and sexuality figured prominently in interviews with participants at private institutions, while faculty at public institutions expressed a range in empowerment and support to broach social justice. It is striking that participants communicated students' discomfort with the topic of race and not racism nor poverty. Several spoke of delaying any discussion about race toward the end of the term, if at all. One participant teaching various courses stated, “I think a lot of students don't want to talk about race. They want to talk about other –isms,” which is why she asks students to consider institutionalized sexism in relation to STEM careers before broaching redlining and the crisis in Flint, Michigan “in a way that doesn't feel in their face so they're more receptive to things like institutionalized racism.” In later interviews, I asked participants to comment on previous participants' hesitation to discuss racism. One who teaches Pathophysiology and Med-Surg wondered if perhaps introducing the topic “makes them [students] emotionally uncomfortable but maybe cognitively they [faculty] also face” not being “equipped” to handle the direction or circumstances of the discussion. We see here the relevance of stance and pedagogical preparation. The idea that racism is only invoked by broaching the subject explicitly, as opposed to a central organizing factor in society, indicates investment in colorblindness.
Only two participants brought up transgender health concerns without any prompts and nearly the entire handful who do speak to students about transgender health issues do so in a reactionary manner based on students' clinical experiences. One did not anticipate having to speak with students about addressing transgender patients until a nurse at a site refused to address a patient appropriately: “It never dawned on me.” It is notable that, after this event, this participant spoke to an administrator before inviting a guest speaker to discuss transgender health concerns in class. This indicates that such topics are risky. Another participant stated: At first maybe I wouldn't have brought it up because some students flip out if you talk about um sexual identity. Before I was like, “I'll leave that—if it comes up, I'll talk about it.” There's so many transgender folks on the units so now I have to bring it up.
“The political”: Navigating career advancement
Teaching social justice poses formidable risks in the classroom with ramifications across one's academic career. Two considered checking in with their department chair or dean prior to bringing in transgender guest speakers to talk about transgender health issues. One dean gave their support “as long as it's about nursing.” Another participant, at their previous institution, faced resistance from leadership when seeking to develop a course about LGBTQ health issues on the grounds that such a topic did not constitute nursing. One said: I think as a person of color, I don't need students to initiate it. I can give my opinion on it and I don't mind saying it. That has not shown up on my evaluations as a bad thing yet—maybe if it did, I wouldn't do it anymore, but I think students appreciate just being real.
Later in the interview, this participant explained the challenge of authenticity while trying to conform to nursing faculty culture because their colleagues are among those deciding their “livelihood.” Despite a student's comment about her being “left leaning,” on a recent course evaluation, one participant teaching Community Health Nursing at a public university stated: I can't say I've had an experience where I've presented something controversial and it's come up on a course evaluation. Would I be worried about that? Yeah, a little - maybe subconsciously. I came to this well into my career. Of course I want tenure but I want [students] to come to an understanding or an appreciation of influences at play. I hate to say it but I think that by us not delving into politics too much, maybe we advocate for nurses to stay apolitical also and that's probably a negative thing. Maybe we perpetuate that a little bit. We tell them or suggest joining a professional organization and speak about their views but I don't know. I'm not sure.
Based on participants' comments, retention, tenure, and promotion are at odds with teaching, service, and scholarship meant to uphold the stated professional value of social justice. This calls into question the mechanisms of higher education that protect the status quo.
Younger faculty and others with pedagogical approaches that veer from their predecessors and colleagues navigate an academic landscape of various obstacles. Pedagogical and collegial support influenced the degree to which they're willing to engage students about so-called controversial topics. Epistemological norms and nursing students' ideas of what nursing is and what nurses do also emerged. One participant who teaches Med-Surg stated: Students are focused on disease processes. You only can slide a little bit of social justice in there. That's not what they're there to learn. You've got to meet them where they are. My risk is only the political climate of the day and how defensive students are going to get. Do I have the resources to deal with whatever it is that I'm going to bring up?
The institutional structure of professional progression through retention, tenure, and promotion figured prominently for nearly all participants in tenure track positions. A participant who teaches multiple courses and described many barriers to integrating social justice within and beyond the classroom recalled an administrator's suggestion that she not submitted her dossier for tenure because she would be unsuccessful. Her interpretation of this discouragement was that her scholarship and service focused on social justice were not seen as rigorous contributions to the institution.
The manner in which topics are brought to or allowed to enter classroom discourse and curriculum indicates agency and conceptualizations of topics deemed suitable for or necessary to nursing. Participants also spoke of curricular factors that shape engagement with social justice.
Curricular Opportunities and Fit
Positioning of CHN
Tenure track faculty were more likely to voice the positioning of CHN while nontenure track faculty more often mentioned that social justice belongs in CHN. One participant who seeks to bring “the whole picture” into the classroom tells students that “community health is political by nature.” She went on to communicate that many nurses are uncomfortable with engaging with political determinants of health as well as topics related to colorblindness. “There's still a good deal of faculty who are like, “Why is this such an issue?” It's painful and difficult for White people to look at who they are.” Med-Surg courses, then, are positioned as apolitical. A few participants spoke of the significance of CHN being at the end of most nursing curricula. One who has taught several courses, including CHN, stated: Everything [emphasis added] belongs in Community Health Nursing, right? That's like the garbage dump. Like everything gets relegated to Community Health or they expect that everything they don't cover is going to be covered in Community Health. As we did the curriculum redesign, questions came up like global health and access to care. The initial response is we put it all into public health [laughs.] Fortunately public health faculty were involved and said, “No, wait a minute! We can't be the only ones.” If you keep connecting dots, they see it rather than coming to the last semester—now Community Health has all the responsibility of the download of everything and students are all like, “I wanna work in the ED. I don't wanna hear about community health.”
CHN faculty spoke of positioning in a number of ways. Most asserted the notion that social justice “is embodied” in CHN, oriented toward social justice because of its “population focus” One such participant described having to “fight” for activities and assignments they hoped to assign to students in their CHN course. Resistance from “Med-Surg faculty” was based on concerns about redundancy and doubts about the relevance of activities examining prejudice, discrimination, and institutionalized bias. They stated that Med-Surg faculty “don't have to fight [for anything].” Another CHN faculty spoke of their frustration: I cringe when non-community health people say, “We just need to educate these people—educate them.” No, you don't have to shove a brochure down their throat. You need to help them see how they have power and control to improve their health. If you leave it [social justice] to Community Health and Leadership to plant and water, it's not gonna happen.”
Content versus context
Tension between content and context was present in many participants' comments. Faculty who teach CHN were more likely to speak of the importance and relevance of culture, empathy, privilege, and the concerns of immigrants to nursing, while White participants who do not teach CHN were more likely to share problematic examples of culture as residing within non-White, nonimmigrant, and non-Christian individuals, which is what Drevdahl (2018) problematizes with the emphasis on cultural competency. Several participants communicated a demarcation between what is necessary—content—and what is considered less so—context. Perspectives about time constraints seemed to exacerbate or serve as rationale for this demarcation. As one participant said: There is so much to cover—I need them to have an understanding of the disease state. By complicating that with cultural influences—that's not how I use my time. There is such a greater emphasis on the disease state rather than the person experiencing the disease state. I think they get very narrow-minded and very kind of blind-folded going through nursing education. When you work in acute care, you're so in control of the environment that people and their social and environmental needs and other aspects other than biophysical get put on the back burner when those are probably the biggest issues in their lives.
The NCLEX: “A driving force”
As one faculty member who teaches Pathophysiology and Pharmacology stated, “I think it means that we make choices based on what's going to help the student succeed on the NCLEX.” The NCLEX serves as a gatekeeping mechanism for licensure and for nursing program accreditation, which takes into account passing rates. The NCLEX holds significance for students, faculty, and employers.
A number of participants described their vigilance around ensuring student preparation. One participant outlined the way they teach as “scrambling” to simultaneously teach current practice, slightly outdated practice as it will likely be tested on the NCLEX, and other topics relevant to current events that will not be included on the licensing exam, such as health care policy. Another spoke of the relationship between pass rates and accreditation. They stated, “I think the NCLEX doesn't escape any of the faculty because to maintain accreditation we have to have a certain pass rate so that's always in my conscious somewhere.”
Another participant characterized the relationship between nursing education and accreditation in more stark terms, stating, “I think the NCLEX pass rate really holds us hostage,” connecting this to a limited sense of empowerment among faculty. Tenure track faculty were more likely to comment about the NCLEX. Faculty of color were more likely to highlight unclear language and the absence of various concepts from the exam, while their counterparts were more likely to assert, to varying degrees, the importance of the NCLEX in gatekeeping entrance into the profession and protecting the safety of patients.
As one stated, the NCLEX has “become a driving force, whether conscious or unconscious, for a lot of programs and a lot of educators.” It also appears that students' expectations of nursing education have been reinforced by the NCLEX test plan, which does not include many Community Health Nursing concepts. One stated: “You're working so hard to make sure they can pass the NCLEX and cramming all this content in. If it's not on the NCLEX, nobody cares. I've had students question why they had to take Community Health at all.”
In summary, several influences shape the pedagogical approaches that participants utilize to facilitate learning about social justice issues and they span participants' personal and professional experiences. Their upbringing, family, othering, and education set the stage for lived and theoretical understandings of justice. Institutional factors related to career progression, geography and student expectations also shape participants' approaches. Finally, participants' perceptions of curricular opportunities also emerged as influences.
Discussion
This study indicates the interrelated influences that shape nurse educators' approaches to social justice, spanning both life span and micro, meso, and macro factors. The multiple influences that emerged from participants' explorations of social justice in their careers as nurse educators can be situated within a map across the lifespan from upbringing to career and along the continuum of individual, programmatic, and institutional dimensions. These findings connect existing findings in higher education, nursing, and sociology of education, and build upon them within the context of nursing (Bonilla-Silva, 2003; Leonardo, 2002; Puzan, 2003).
Formative Experiences
The salience of participants' childhood experiences of residential segregation upon their conceptualizations was an unexpected though not surprising finding. The long history and ongoing legacy of racist housing policies, serial displacement, and gentrification on isolation and implicit bias are well documented (Carter, Skiba, Arredondo, & Pollock, 2017; Rothstein, 2017). As an occupation with increasing minimum education requirements, existing and historical economic and housing landscapes of those who become nurses are increasingly relevant. Consistent with the primacy to situate one's questions and findings in relation to their positionality and gaze, the growing field of critical whiteness studies seeks to address global White racial privilege, signaling a shift from research about those who are minoritized and marginalized (Leonardo, 2002). Canales (2010) has examined othering in the nursing literature and found exclusionary othering to be most prominent. Marginalization, internalized oppression, and alienation are among the consequences of exclusionary othering (Canales, 2010). Puzan (2003) describes whiteness as a bedrock of nursing, both in practice and education, asserting that power wielded by nurses is rooted in empiricism and the protected knowledge of a profession manifesting in patient–nurse interactions and language. Such othering is facilitated through historical and ongoing legacies of de facto and de jure segregation, which emerged in participants' stories about their childhood and upbringing.
Housing and education are inextricably linked and inequality across all levels of schooling takes several forms, including racial segregation between lower level and upper level courses (Gettleman, 2005), differential access to scholarships and financial aid (Mathews, 2005), and inequitable guidance counseling based on student ethnicity (Linnehan, Weer, & Stonely, 2011). Consistent isolation creates and perpetuates segregation of lived experiences, career trajectories and goals, and the degree to which any given profession must and can be diversified. Efforts to diversify the nursing workforce, therefore, would be superficial if the deep-seated divisions in daily life and across lifespans are not addressed.
Another significant finding that arose is the need for a pipeline for nurse educators along with social justice education and development of pedagogical and andragogical approaches. Relf (2016) found that despite multiple initiatives to increase diversity by Johnson & Johnson, the Institute of Medicine, and the Robert Wood Johnson Foundation, there remains much work for nursing workforce demographics to match those of the United States. Increased racial diversity and greater concordance between nursing workforce and patient population, however, will not guarantee social justice nursing but is a step toward epistemological diversity and cultural responsiveness. A social justice-oriented approach would emphasize theoretical traditions, teaching approaches, and curricular considerations. The findings also indicate the need for active and supportive mentorship for new faculty as they learn about the mechanics of higher academia and map the landscape of power and change. This is consistent with Hamilton and Haozous's (2016) findings that nursing faculty of color are less likely to remain in a faculty position and that retention is shaped by mentoring, organizational climate, and policies that support workplace parity.
Participants' struggles to step into faculty roles are consistent with existing literature about the systematic devaluation of developing teaching philosophies and pedagogies in research-focused doctoral programs (Anderson, 2000). This is particularly notable as research-oriented doctoral degrees are the preferred terminal degree for tenure track positions. If the development of pedagogy and one's teaching philosophy are not foundational to the training or degree required to become a faculty member and, therefore, chairs and deans of nursing programs, then inadequate preparation to teach is institutionalized.
This discretizing and focus on disease state as separate from the patient is telling. It is consistent with the biomedical model where cultural factors, among others, are viewed as complications rather than a necessary dimension of learning to become a nurse. An “information in isolation” approach creates an understanding of health and nursing that removes the impact of context and upstream factors. How nurse educators frame health concerns shapes the constellation of possibilities for partners in health, opportunities for action, and scope of practice.
Curricular Fit: Fragmentation of Colonialism
The influence of tests on education is not a new phenomenon and several participants' comments invite us to consider the role of the NCLEX in the eyes of faculty and students and the overall infrastructure of nursing education. The significance of the NCLEX is similar to the focus on standardized testing throughout the education system beginning in elementary school. Prospective nursing students might consider a program's more recent graduates' NCLEX pass rate as a marker of its capacity to prepare them to pass the exam, which serves as a gatekeeper to entering the profession.
Medicine, health care, and health sciences have not been immune to socioeconomic stratification that exists across society. Increasing minimum education requirements and various aspects of professionalization serve to perpetuate tracking that occurs as early as elementary school. These disciplines and professions have actually played instrumental roles in the construction and pathologizing of difference. A troubling history includes medical experimentation on enslaved people purchased by physicians to advance treatment methods and train future physicians, scientific racism entrenched in the dehumanization of minoritized peoples, the assigning of sex at birth based on the presence or absence of a penis, and the construction of heterosexuality as the standard (Katz, 2008; Washington, 2006). Nursing scholars in Canada and Australia have blazed a trail in examining the historical and ongoing impact of colonialism on health inequities and access to care among indigenous peoples, although there is limited information about the integration of such knowledge into the training of health care providers (Beavis et al., 2015; Turale & Miller, 2006).
The Institutional Context of Nursing Education
Nearly all participants spoke of maneuvering and vigilance around a constructed line delineating between what is political and what is not. They also described teaching strategies that minimize or avoid crossing a particular threshold, whether based on past experiences in the classroom, colleagues' warnings, or explicit statements from program directors or administrators to not engage in particular topics in the classroom. The “political,” the emotional, and the racial are communicated explicitly and implicitly as dimensions to be weary of and not standard components of nursing education despite the claim that social justice is a core professional value (Boswell & Cannon, 2005; Mahlin, 2010). Hesitation about broaching race, racism, and White privilege, warnings from colleagues of color, and delaying discussion of these topics until the end of the academic term can be understood through the concepts of White fragility and rage (Anderson, 2016) and how they interface with the hierarchy of higher education and the retention, tenure, and promotion process (DiAngelo, 2018; Ford, 2011).
Conclusion
This study contributes to what is known about the landscape of nursing education, indicating that individuals who teach social justice do so in spite of uneven and largely superficial institutional support. These findings call for a reckoning of how various experiences and disciplinary knowledge influence and enhance one's understanding of society, health, and caring. To teach social justice in baccalaureate nursing programs is to risk career advancement and lay bare inadequate teaching preparation by terminal degree programs required for tenure track positions. To advance social justice in nursing requires collective reckoning that faculty who are minoritized bear the inequitable burden of navigating the minefields of power that shape their upbringing, career aspirations, experiences as students, experiences as faculty, and beyond.
Supplemental Material
PPN881726 Supplemental Material - Supplemental material for “Spinning Their Wheels … ”—Influences That Shape How Nurse Educators Teach Social Justice
Supplemental material, PPN881726 Supplemental Material for “Spinning Their Wheels … ”—Influences That Shape How Nurse Educators Teach Social Justice by Claire P. Valderama-Wallace PhD, MPH, RN Ester Carolina Apesoa-Varano PhD in Policy, Politics, & Nursing Practice
Footnotes
Acknowledgments
This work would not be possible without the tireless and often unsung or dismissed efforts by minoritized leaders, visionaries, scholars, activists, and martyrs to name, address, and dismantle unjust social structures and the ideologies that perpetuate inequities. Much gratitude to my dissertation and qualifying exam committees for believing in this work and providing thoughtful guidance. Special thanks to every scholar whose work informed and inspires this scholarship and how I envision my career. I also want to acknowledge the Jonas Nurse Scholars Program. Finally, I thank my partner, children, and parents for their encouragement, patience, and love.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.