
Abstract
Perinatal illicit substance use is a nursing and public health issue. Current screening policies have significant consequences for birthing individuals and their families. Racial disparities exist in spite of targeted and universal screening policies and practices. Thus, new theoretical approaches are needed to investigate perinatal illicit substance use screening in hospital settings. The purpose of this analysis is to evaluate the social construction of target populations theory in the context of perinatal illicit substance use screening. Using the theoretical insights of this theory to interrogate the approaches taken by policy makers to address perinatal illicit substance use and screening provides the contextual framework needed to understand why specific policy tools were selected when designing public policy to address these issues. The analysis and evaluation of this theory was conducted using the theory description and critical reflection model.
The preoccupation with controlling the reproductive choices of Black birthing individuals is etched in the very fabric of the United States (Roberts, 1999). There have been multiple attempts to deter such individuals from exercising reproductive autonomy (Roberts, 1999), which is defined as “having the power to decide about and control matters associated with contraceptive use, pregnancy, and childbearing” (Upadhyay et al., 2014, p. 20). The hypervigilance surrounding the reproductive decision making and criminalization of Black birthing individuals has and continues to thrive under the guise of legislation, policies, protocols, and socially constructed norms related to mothering and motherhood (Kim et al., 2020).
Perinatal illicit substance screening has been yet another mechanism challenging the reproductive autonomy of Black birthing individuals. Specifically, fear of the potential consequences of screening (e.g., prosecution, child removal, stigmatization, and coercive treatment) can influence these individuals’ reproductive health decisions. Their decision-making capacity and their power to control matters related to contraceptive use, pregnancy, and childbearing are diminished (Gregory, 2010; Stone, 2015).
On its surface, perinatal illicit substance screening may appear to be a protective mechanism. Screenings have been promoted to safeguard the health of babies and to guide care during the intrapartum and postpartum periods (Murphy-Oikonen et al., 2010). However, these policies and protocols have typically been based on unvalidated tools, implemented arbitrarily, using flawed designs targeted at a specific subset of the population (Miller et al., 2014; Ondersma et al., 2000). Apart from detecting substance use, these tools can also result in trauma and contribute to health disparities and inequities: the exact opposite of healthcare workers’ intentions.
This paper explores how the social construction of target populations can be used to describe policy and protocol approaches to perinatal illicit substance screening. Specifically, these theories provide a framework for understanding the motivation behind policy design based on the social construction of target groups based on societal norms. Examining perinatal illicit substance screening in terms of the social construction of target populations, this paper describes how stereotypes have been used to shape policies that then result in discrimination and health disparities. Understanding how policies may be Biased and/or result in discrimination and health disparities is critical to healthcare professionals, particularly nurses as they are typically charged with implementing such policies.
To understand the driving forces behind the various approaches to perinatal illicit substance use and screening, this analysis begins with an account of the social construction of motherhood and the racialization and criminalization of perinatal substance use. This discussion is followed by a brief review of theoretical insights relevant to understanding how perinatal illicit substance use has been constructed and screening practices implemented.
Social Construction of Motherhood
Motherhood is frequently seen as a rite of passage or status. While it may shape the identity of some birthing and parenting individuals, this status remains unattainable for many (Roberts, 1997). A ‘good mother’ is typically understood to be submissive and dependent, to bear healthy and productive children, to act selflessly and put the needs of her children before her own, to be in a cisgender marriage, not to use licit or illicit substances, not to work outside of the home, and to be dedicated to caring for her family (Wood, 2013). The social construction of motherhood in the United States has largely been based on white, middle-class birthing individuals, and those who fail to meet such standards are shunned and considered bad mothers (Fouquier, 2011).
Conversely, a ‘bad mother’ is often depicted as cold, aggressive, overconfident, unattractive, working outside the home, putting their personal needs before those of their children, and incapable of raising productive citizens (Wood, 2013). Specific to perinatal illicit substance use, individuals who use substances while pregnant have been labeled as bad parents and stereotyped as disrespectful, untrustworthy, selfish, disinterested in prenatal care, incompetent, deviant, and focused solely on getting their next fix (Benoit et al., 2015; Miller, 2001). Their drug use is seen as breaking the “moral code” of motherhood and as compromising the health of the fetus (Benoit et al., 2015). In addition, birthing individuals of color are rarely portrayed positively in mainstream media, instead being associated with perinatal illicit substance use, indirectly reinforcing the notion that Black, Indigenous, and people of color (BIPOC) are not good mothers (Johnston & Swanson, 2003).
The perpetuation of the good mother/bad mother dichotomy, based on the experiences of white, middle-class women, puts low-income and BIPOC birthing individuals at a disadvantage and makes it extremely difficult, if not impossible, for these individuals or groups to achieve the social identity of a good mother (Fouquier, 2011).
Deserving Motherhood
Society at large does not value or promote motherhood equally among birthing individuals. White birthing individuals have been encouraged to procreate, while Black birthing individuals have been systematically denied, discouraged, and even demonized for procreation, with the exception of forced procreation during slavery (Roberts, 1997, 1999; Springer, 2010). The simultaneous promotion of motherhood for some and its suppression for others raises the question, why should some people deserve motherhood while others do not? Some would argue that every birthing individual has the fundamental right to decide whether or not they want to parent, as a core element of reproductive justice. Melding reproductive rights with social justice discourse, the theory of reproductive justice shifts the conversation from “choice” to human rights (Ross & Solinger, 2017). The decision whether or not to have a child, the ability to parent in a safe and healthy environment, sexual autonomy, and gender freedom are all fundamental principles of reproductive justice (Ross & Solinger, 2017). However, given the history and political climate of the United States, BIPOC birthing individuals have not been provided with reproductive justice. Instead, they have endured the racialization and criminalization of motherhood and perinatal substance use.
The Racialization and Criminalization of Perinatal Substance Use
The criminalization of perinatal illicit substance use garnered national attention in the 1970s and 80s as part of the war on drugs, in which illicit substance use was designated “public enemy number one” (Lassiter, 2015, p. 135). Although individuals of reproductive age have historically used both licit and illicit substances, crack cocaine took center stage in this moral panic, aided by mainstream media outlets (e.g., television, newspaper, and radio; Springer, 2010). With the help of popular media outlets, perinatal illicit substance use was not only criminalized, but also racialized.
During this period, images of the typical crack cocaine users flooded mainstream media alongside details of the drug's devastating effects on children (Springer, 2010). Media were able to create a narrative about crack cocaine that led people to associate a specific location (urban communities) and identity (overwhelmingly Black individuals) as representing the epidemic. Media portrayals of substance use among BIPOC individuals reinforced the image of substance use as an experience tied to poor, ethnic communities and the interpretation of such individuals as deviant, criminal, and deserving of punishment (Springer, 2010). The racialized depiction of crack cocaine led to the overestimation of its use among BIPOC people, helping shape popular opinion and guiding hospital policy development (Springer, 2010; Toscano, 2005).
Conversely, media often associate low-income white women with tobacco and alcohol use, while upper-class white women are rarely depicted as substance users (Springer, 2010). That said, the methamphetamine and opioid epidemics were often associated with low income and middle-class white women respectively (Netherland & Hansen, 2016; Springer, 2010). Substance use within white communities typically was and continues to be portrayed in the media as surprising, atypical, and deserving of compassionate care (Netherland & Hansen, 2016). This portrayal aligns with the historical lack of acknowledgement of substance use among white people and reinforces the notion that white individuals who use substances are victims deserving of empathy rather than punishment (Netherland & Hansen, 2016).
Pregnant and postpartum BIPOC individuals have been the focus of many controversial cases surrounding efforts to criminalize perinatal illicit substance use. This can be seen in fetal protection laws, child abuse statutes, the misapplication of existing laws outside of their intended scope, biased protocols, discriminatory and discretionary screening practices, and patient–provider privacy breaches. Such practices have resulted in the prosecution and conviction of pregnant and birthing individuals, who may be accused of delivering substances to their fetus, child neglect, or even of murder after a stillbirth (Paltrow & Flavin, 2013). The criminalization of perinatal illicit substance use reinforces widely held beliefs about the behavior of pregnant and birthing individuals; serves as population control, by deterring procreation out of fear of prosecution; supports politicians’ political aspirations, by demonstrating a willingness to prosecute deviants; and distracts from the structural issues that contribute to poor birth outcomes, such as poverty and access to healthcare (Goodwin, 2017; Ocen, 2017; Schneider & Ingram, 1993).
Paltrow and Flavin (2013) conducted a landmark study that reviewed over 400 fetal protection prosecution cases, in which criminal or civil actions were taken against women using illicit substances during pregnancy between 1973 and 2005. They found that Black women represented more than half of the cases, and that low-income women, regardless of race, represented over 70% of cases reviewed. Incarceration, civil commitment, and mandated participation in drug treatment programs were among the punishments levied against these individuals.
This criminalization of both pregnancy and one's behavior sets a dangerous precedent, in that it allows for the behaviors, decisions, and actions of pregnant and birthing individuals to be subject to investigation and prosecution if they do not align with societal norms without consideration of larger institutional biases and sociocultural influences (Goodwin, 2017; Toscano, 2005). It also drastically reduces the options available to such individuals, pregnant or otherwise, as detection or disclosure can have significant consequences (Goodwin, 2017; Ocen, 2017; Paltrow & Flavin, 2013).
Methods
When determining how best to conceptualize perinatal illicit substance screening protocols, we considered intersectionality, critical race theory, reproductive justice, moral panic theory, and the social construction of target populations as theoretical approaches. While all of these perspectives deepen the understanding of this phenomenon, the social construction of target populations was chosen because of its structured approach to categorizing target populations, its ability to describe motivational factors influencing policy design, and its predictive nature concerning the allocation of benefits or sanctions. Chinn & Kramer; (2018) model of theory description and critical reflection was used to analyze and critique theories of social construction of target populations.
The Social Construction of Target Populations
The social construction of target populations theory was originally developed in the 1980s by Schneider and Ingram to help explain how different factors or characteristics influence agenda setting, design, selection, implementation, and evaluation of public policy (Ingram et al., 2007; Schneider & Ingram, 1993). Unlike existing policy theories available at the time, the theory of the social construction of target populations emphasizes the significance of social constructions and the allocation of beneficial and punitive policies, the enduring effects of policies even when ineffective, and how changes in social constructions or institutions occur over time. Simply put, this perspective draws attention to the conditions under which policies are designed, who those policies affect, and how policy choices impact the target group (Ingram et al., 2007).
Schneider and Ingram (1993) distinguished four target populations or groups: advantaged, contenders, dependents, and deviants. Depending on individual group membership, policy and policy tools will be beneficial or burdensome, the individual will be viewed as deserving or undeserving, and the individual will have a high or low ability to mobilize politically (Table 1). Placement within these groups is based on socially constructed norms. The notion that target populations are formed and reinforced based on social constructs and interactions within the political arena builds on Berger and Luckmann's social construction of reality, as they were among the first sociologists to develop this line of theory (Berger & Luckmann, 1967).
Social Construction of Target Populations: Target Populations’ Descriptions.

Adapted from Schneider, A., and Ingram, H. (1993).
Policy Tools
Policy tools are the features embedded in the policy that are used to motivate or coerce the target population to comply with a specific law, guideline, or desired behavior (Schneider & Ingram, 1990, 1993). Policy tools can shape and reinforce messages about what behavior is desirable, which citizens are deserving or undeserving, who is subject to punishment, and what role the government should play to enforce these policies (Schneider & Ingram, 1993). Policy tools have been categorized as authoritative, incentivized, capacity, symbolic and hortatory, and learning (Table 2; Schneider and Ingram, 1990). Each policy tool puts forth a set of behavioral assumptions regarding what is needed to gain compliance from the target population (Table 2).
Social Construction of Target Populations: Behavioral Assumptions of Policy Tools.
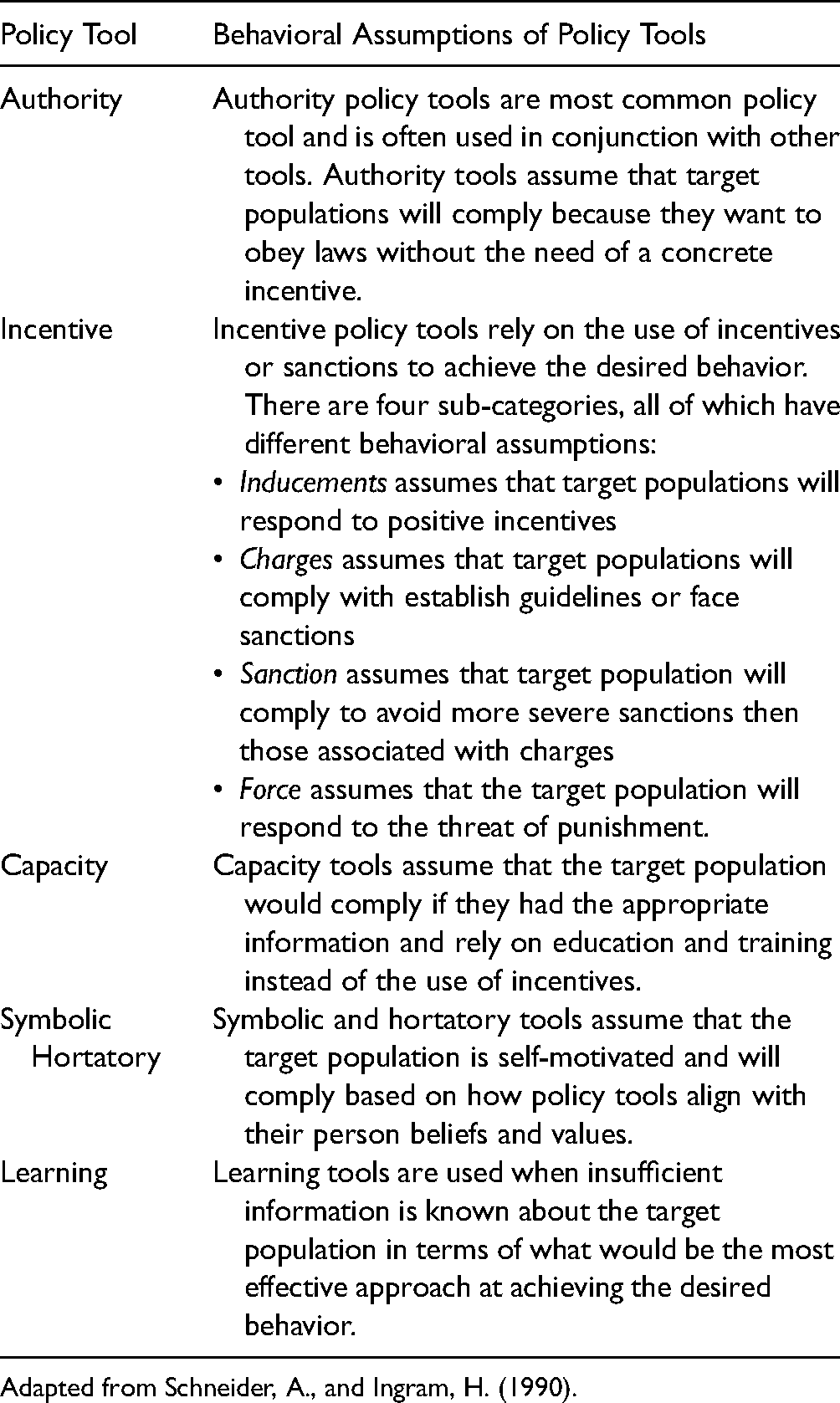
Adapted from Schneider, A., and Ingram, H. (1990).
Fundamental Elements of the Social Construction of Target Populations
Schneider and Sidney (2009) proposed nine fundamental elements of public policy: (1) defining the problem and goals, (2) allocating benefits and burdens, (3) identifying target populations, (4) establishing rules, (5) selecting tools, (6) implementing strategy, (7) social constructions, (8) justifying policy (explicit or implicit), and (9) assumptions (explicit or implicit). Policy design begins with identifying the issue to be addressed and establishing policy goals and the desired outcome(s). In defining the issue, policy makers identify a target population and select policy tools to solicit the desired outcome based on how the target population is socially constructed. Policy makers justify the selected policy approach and the allocation of benefits (e.g., social programs) or burdens (e.g., incarceration) based on the socially constructed target population. Establishing rules and implementation strategy overlap, in that policy makers focus on who gets what resources and when, in addition to evaluating the policy. These policy tools can be used to design policies at the federal, state, local, and institutional (e.g., healthcare systems). Lastly, Ingram and colleagues (2007) described six propositions that demonstrate the interrelationship between theory concepts and overall purpose (Table 3).
Social Construction of Target Populations: Theory Propositions.
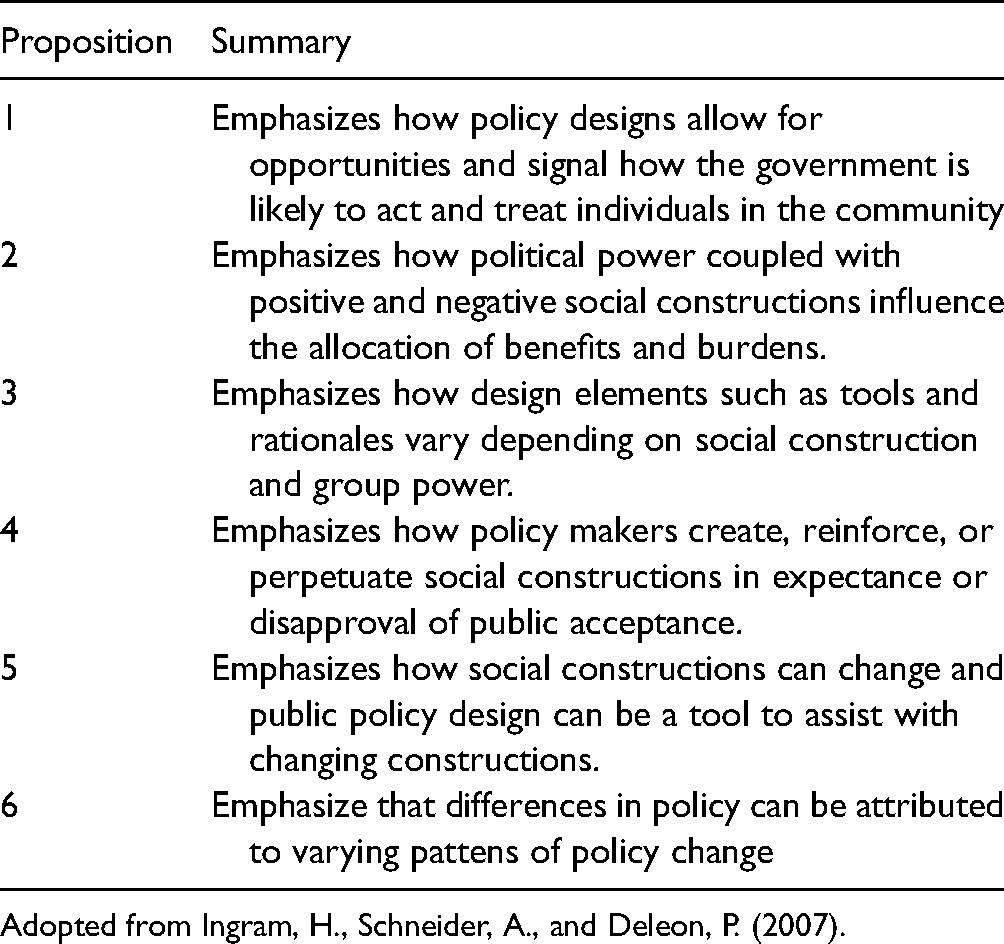
Adopted from Ingram, H., Schneider, A., and Deleon, P. (2007).
Applications of the Social Construction of Target Populations
A broad range of qualitative and quantitative researchers have examined a wide variety of topics from the perspective of social construction of target populations (Fording et al., 2011; Owens & Smith, 2012; Pierce et al., 2014). The variety of methodological approaches taken to examine different policy domains demonstrates the theoretical versatility of the social construction of target populations perspective.
Deploying the Social Construction of Target Populations
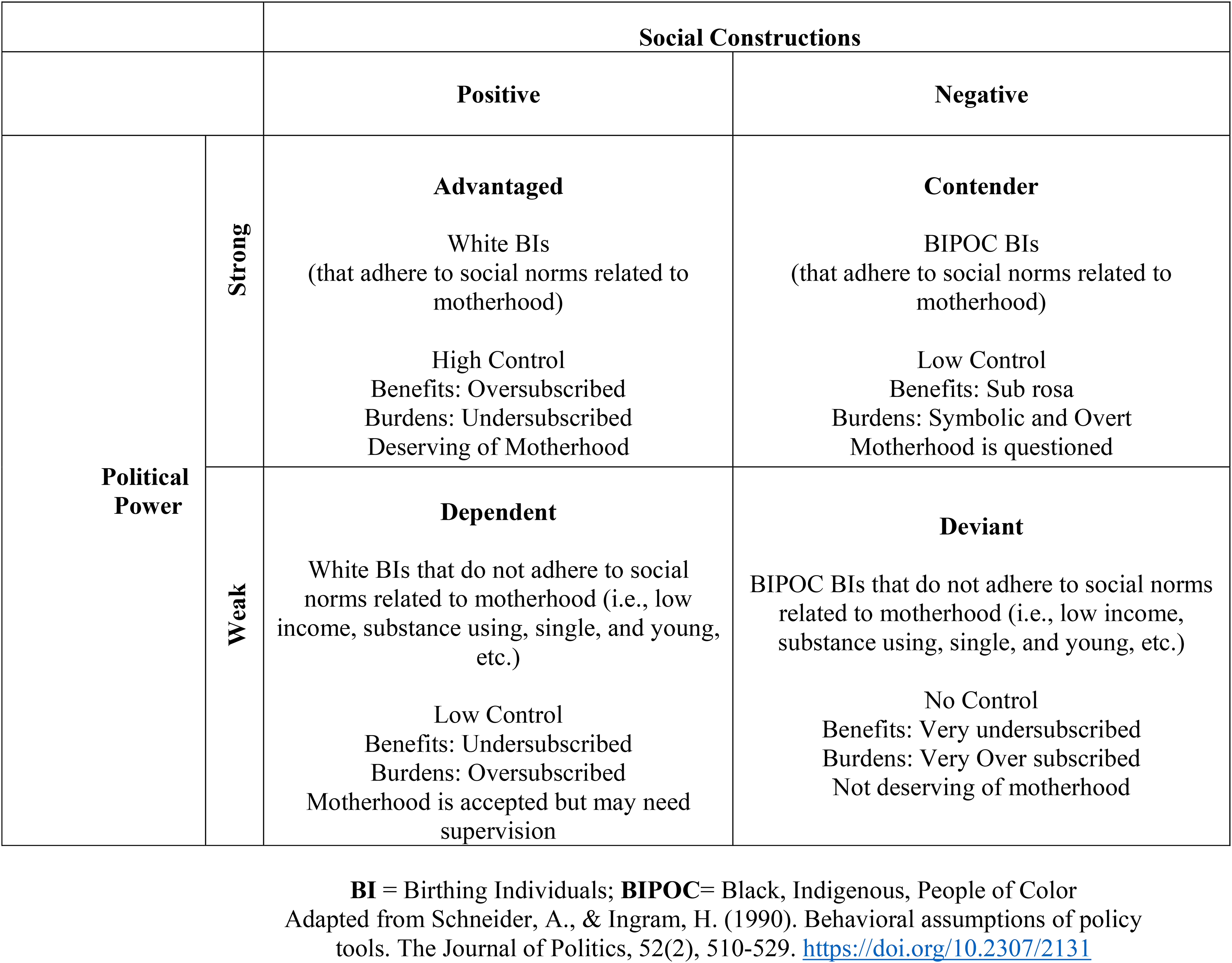
The social construction of target populations theory is used to explore policy designs specific to perinatal illicit substance screening. It is important to mention that the target group for screening can be seen as unitary —birthing individuals—the theory has been modified to reflect four intra-target groups: white birthing individuals that adhere to social norms related to motherhood, BIPOC individuals that adhere to social norms related to motherhood, white birthing individuals that do not adhere to social norms related to motherhood, and BIPOC birthing individuals that do not adhere to social norms related to motherhood (Figure 1). Social norms include but are not limited to income, marital status, ability to care for and birth healthy children, and abstinence from illicit substances.
Target populations of birthing individuals informed by the social constructions of target populations.
Target Populations
White birthing individuals who adhere to social norms related to motherhood are members of the advantaged target population and their placement within this group is based on a social construction of motherhood largely based on white middle-class birthing individuals (Fouquier, 2011; Springer, 2010). Those who meet or adhere to social norms related to motherhood are able to avoid detection, not because they do not use illicit substances but because society is not suspicious of them (Netherland & Hansen, 2016).
Black, Indigenous and People of Color who adhere to social norms related to motherhood are members of the contender target population. Their placement within this group is based on historical devaluation of their roles in motherhood and procreation, questions concerning their ability to parent, and the fact that the social construction of a good mother is Eurocentric (Roberts, 1997). Although policies targeting contenders tend to be burdensome, group members may achieve some level of protection if they are able to meet all other social norms. However, provider beliefs, discretionary screening practices, and institutional protocol criteria often result in BIPOC individuals undergoing perinatal illicit substance screening.
White birthing individuals who do not adhere to social norms related to motherhood are members of the dependent target population. Their placement within this group is historical; birthing individuals have long been viewed as dependents (Schneider & Ingram, 1993). Furthermore, white birthing individuals who use illicit substances have been viewed through a sympathetic lens; they are seen as just trying to meet the demands of motherhood and not (like birthing individuals of color) as moral failures. This pattern is consistent with each group's placement in the social construction of target populations theory (Netherland & Hansen, 2016).
Black, Indigenous and people of color who do not adhere to social norms related to motherhood are members of the deviant target population. Their placement within this group is based on the historical accounts of institutional surveillance, restricted reproductive autonomy, and the criminalization of BIPOC individuals who deviate from socially construction norms of motherhood (Roberts, 1997, 1999). Policies targeting the deviant population are punitive, harmful, and burdensome. Members of the deviant population will almost certainly undergo screening, as they have very few protective measures.
Having explained group membership and target populations, we now examine both the crack cocaine and opioid epidemics using the social construction of target populations theory.
The Social Construction of Target Populations and Perinatal Illicit Substance use
The social construction of target populations theory can be used to explain both the design of screening policies and the actions taken against birthing individuals placed within different target populations. The crack cocaine and opioid epidemics demonstrate the relevance of the social construction of target populations for exploring actions taken against birthing individuals who use illicit substances; meanwhile, targeted or risked-based screening is used to examine policy design.
Crack Cocaine Epidemic
Elected officials, the media, and flawed research contributed to sensationalism concerning crack cocaine use among Black birthing individuals and the impact of crack cocaine on the fetus or newborn (Hart, 2020; Netherland & Hansen, 2016; Omori, 2013). These individuals were demonized, labeled as unfit, charged with birthing damaged babies, and characterized as a blight on society—lacking the maternal instinct needed to safely care for their children (Netherland & Hansen, 2016; Toscano, 2005). The rhetoric used by elected officials and the media sought to punish individuals for their substance use and label them as deviant. These individuals were not cared for or regarded as people living with a disease in need of treatment or support (Netherland & Hansen, 2016). Sensational rhetoric about crack cocaine spurred a variety of policies to criminalize, prosecute, confine, or restrict the parental rights of Black birthing individuals who used crack cocaine while pregnant (Paltrow, 2005). The rationales behind such punitive approaches centered on the protection and safety of innocent babies (Paltrow & Flavin, 2013).
These policy designs limited access to beneficial policies, such as substance use treatment (Ingram et al., 2007). Conversely, they promoted arrest and prosecution, coercion to seek treatment, child removal, institutional surveillance by government agencies, which is consistent with incentive policy tools that rely on force, sanctions, or charges (Paltrow, 2005; Paltrow & Flavin, 2013; Table 2; Schneider & Ingram, 1990). These same policy approaches were seen with heroin, which was also largely constructed as an illicit substance used by Black individuals.
The rhetoric used to describe those who used crack cocaine and/or heroin, and the approach to address such use, is consistent with messaging related to members of the deviant population as defined by the social construction of target populations theory. Additionally, such authoritative or incentive policy tools and fear-based rationales were used to justify punitive policy designs, as the social construction of target populations perspective implies. The threat of negative consequences as a result of perinatal illicit substance use further reflects the social construction of target populations. In summary, this theoretical approach can be used to explain not only how this target population is socially constructed but also the rationale behind specific policies designed to penalize illicit substance use among Black birthing individuals and the consequences levied against them.
Opioid Epidemic
The social construction of the opioid epidemic of the 2000s has been in sharp contrast to the ways the crack cocaine epidemic of the 1980s had been interpreted (Netherland & Hansen, 2017; Springer, 2010). Elected officials and the media largely constructed the opioid epidemic as a crisis largely among white suburban individuals (James & Jordan, 2018; Netherland & Hansen, 2016). In shifting the target group from Black birthing individuals to white suburban birthing individuals, the target population classification, policy tools, rationales, and consequences for noncompliance have undergone corresponding shifts. White birthing individuals found to use illicit substances are members of the dependent target population and are viewed as sympathetic and deserving of support and resources.
The rhetoric used to describe the opioid crisis took a more therapeutic approach, compared to the punitive approach used for crack cocaine—it was described not as a moral failing but as a systemic failure and a disease deserving of medical treatment (James & Jordan, 2018). This softening of the rhetoric surrounding the opioid epidemic aided in shaping the social construction of the target group as deserving and informed the national conversation about the policy designs that should target this group. In this case, supportive policies called for treatment and treatment programs, an approach not afforded to Black individuals during the crack epidemic (Netherland & Hansen, 2016). The use of symbolic, hortatory, and capacity policy tools helped shape policies targeting this population, in lieu of authoritative or incentive policy tools (Table 2; Schneider and Ingram, 1990).
Demands for institutional changes in regard to opioid prescribing practices among healthcare workers and within the pharmaceutical industry were loud and swift. Pharmaceutical companies were blamed, and their deceptive opioid marketing practices criticized. Culpability shifted from white suburbanites to healthcare providers, thus rendering white individuals who used illicit opioid substances as blameless victims (Netherland & Hansen, 2016). The lack of acknowledgement of illicit substance use among white individuals is rooted in racism and oppression and serves as the rationale for a more sympathetic approach to the opioid epidemic. White illicit substance users are often depicted as helpless victims or hard-working individuals who use substances in order to meet the demands of everyday life (Netherland & Hansen, 2017).
The use of symbolic and hortatory policy tools by policy makers and elected officials is strategic, in that they perpetuate traditional beliefs related to whiteness and substances. Consequences for substance use no longer centered on the carceral system and family separation; instead, white substance-using individuals are offered treatment and compassionate care (Netherland & Hansen, 2017). For example, buprenorphine and naloxone, a medication for treating opioid addiction, is often marketed toward white individuals (Netherland & Hansen, 2017). This medication can be prescribed from the privacy of an outpatient clinician office. This practice affords white individuals the opportunity to seek treatment while shielding them from public scrutiny, allowing these individuals to maintain a positive social image (Netherland & Hansen, 2017).
Targeted/Risked-Based Screening
Regardless of the specific substance of focus (crack cocaine in the 1980s, heroin in the 1990s, and opioids in the 2000s), all of these epidemics have one element in common: illicit substance screening. This analysis will focus on policies implemented at the institutional level. Targeted and universal screening are the two most commonly used policies. Universal screening requires all birthing individuals to undergo screening, while targeted or risk-based screening is triggered based on a list of established criteria. A variety of specimens can be used for perinatal illicit substance screening, with urine being the most widely used specimen (Price et al., 2018).
The next section is focused on targeted or risk-based screening criteria. More specifically, late entry into prenatal care and preterm birth which are among the most frequently used screening criteria.
Late Entry into Prenatal Care
Late entry into prenatal care is defined as the initiation of care in the third trimester of pregnancy (Kotelchuck, 1994). According to the National Center for Health Statistics, in 2019, late entry into prenatal care was highest among non-Hispanic Black women at 9.6%, followed by Hispanic women at 8.2%, and non-Hispanic white women at 4.5%. That said, individuals may enter into prenatal care in the third trimester as a result of many factors, such as age, residency (i.e., rural vs. inner city), access to quality care, and insurance status, all of which reflect socioeconomic status and are not necessarily an indication of substance use (Baer et al., 2019). The use of this criterion subjects BIPOC and low-income individuals to excessive scrutiny because of their inability to afford or participate in routine standards of care, ultimately penalizing poverty.
Preterm Birth
In 2020, the rate of preterm births in the United States among Black women was 14.39%, compared to 9.83% among Hispanic women and 9.10% for white women (Hamilton et al., 2021). Substance use is just one of many risk factors for preterm birth; its impacts are difficult to separate from other risk factors such as structural racism, poor nutrition, use of licit substances (e.g., alcohol and tobacco), psychosocial factors (e.g., stress), and socioeconomic status (Goodwin, 2017; Ocen, 2017). The continued use of preterm birth as a screening criterion makes Black birthing individuals more susceptible to undergo screening, as preterm birth rates are nearly 1.5 times higher than those of Hispanic and white birthing individuals.
In examining these two commonly used screening criteria, it is clear that many of the members in the advantaged target population are typically able to avoid screening—due to socioeconomic status, health-related protective factors, and privilege—thus insulating them from negative consequences or experiences. By contrast, contenders, dependents, and deviants are usually unable to avoid detection because these screening tools incorporate issues of socioeconomic status and health risk factors that often plague this population.
Clinical Implications
Using the social construction of target populations as a lens revealed several clinical implications from an examination of perinatal illicit substance use and screening. The punitive nature of such screening is largely driven by who society has constructed as substance users; its consequences are counterintuitive to the goal of these policies, which are to improve birth outcomes. Although the behavioral assumptions around the use of coercive policy tools suggest that the target population will comply with the desired behavior (in this case, by ceasing to consume illicit substances), that has not been found to be true (Schneider & Ingram, 1990). In fact, the use of a punitive approach has been found to drive birthing individuals away from care, (Stone, 2015).
The contrasting approaches taken to the crack cocaine and opioid epidemics in the United States, which were heavily influenced by the social constructions of the target populations (Black individuals vs. white suburban individuals), draws attention to the ways historical misperceptions and stereotypes influence policy design. Clinical practice should take into account how substance use has been defined—as a self-imposed problem rather than a disease—and how resources have been allocated. With both the crack cocaine and opioid epidemics, the resources allocated appeared inadequate to solve the problem. However, with the opioid epidemic, the language around the target population shifted, largely because of who was impacted. This change brought about an increase in the allocation of treatment options (i.e., buprenorphine and naloxone), some of which have traditionally been targeted toward white individuals (Lagisetty et al., 2019; Netherland & Hansen, 2016, 2017). These inequities in treatment options are the result of institutional and structural racism.
Specific to nurses and nursing, implementing polices that have been found to be biased and discriminatory reinforces institutional and structural racism and discrimination (Association of Women; Health, Obstetric, & Neonatal Nurses, 2021). By examining perinatal illicit substance screening policies using the social construction of target populations allows for one to make the connection between policy, practice, and impact. Further it provides an avenue for nurses to advocate for policy change on behalf of their patients.
Incorporating screening criteria that is nonspecific to detecting substance use but highly correlated with individuals’ socioeconomic status, race, and ethnicity allows for those who are not impacted by such constraints to be overlooked when assessing for perinatal illicit substance use. While many white birthing individuals are provided privilege and protection based on screening criteria, BIPOC birthing individuals usually are not, which increases their potential exposure not only to screening but, more importantly, to the consequences of screening. Again, this inequity is the result of institutional racism.
Critique
The social construction of target populations theory is generalizable and has been used by both qualitative and quantitative researchers on a variety of topics (Fording et al., 2011; Pierce et al., 2014). While multiple concepts and their relationships lend complexity to these perspectives, they are highly accessible because they contain many empirical indicators that can easily be identified within the policy design process. Finally, insights from the social construction of target populations are critical to understanding the policy design process because policies made at the federal, state, local, and institutional (i.e., hospital) levels impact who has access to care, what treatments are available, how care is delivered, and how information is shared among institutions, factors that ultimately shape individuals’ experiences of healthcare.
Limitations
Despite the theoretical versatility of social construction of target populations as a conceptual frame, key criticisms have been raised to it as well. A key criticism levied against the initial social construction of target populations theory was that upon its creation, little attention was paid to history and institutional power (Lieberman, 1995). Ingram and colleagues (2007) responded by stating that they viewed policy as an institution with deep-rooted historical significance; in subsequent publications, they explicitly identified degenerative politics and professionalized politics as institutional cultures.
Another criticism of the social construction of target populations is that they do not account for multiple interlocking identities when determining placement within one of the four target populations or groups. Perinatal illicit substance use cuts across all races, ethnicities, and classes, yet BIPOC and low-income birthing individuals often experience perinatal illicit substance screenings policies differently than do white birthing individuals, despite similar rates of illicit substance use. That said, the social construction of target populations theory can still be used to understand why intragroup members experience policies differently.
Conclusion
Due to the mounting concern about substance use among birthing individuals, illicit substance screening will remain an area of focus. Unless the influence of discrimination, racism, and biases in policy design and implementation are acknowledged, inequities will persist. The social construction of target populations provides the framework needed not only to gain insight into policy design but also to create pathways to pursue change. In this case, change will occur when the social constructions of substance use changes for everyone, not just specific intra-group members. The unique contribution of the application of the social construction of target populations to perinatal illicit substance screening is understood in relation to the varied experiences of individuals with interlocking identities, who are members of different target populations, with various sociocultural and economic influences but share a similar experience (i.e., pregnancy). Ultimately, this perspective provides another pathway for nurses and other healthcare providers to explore disparities in policy design.
Footnotes
Acknowledgments
We thank Dr. Sarah C.M. Roberts (University of California, San Francisco, School of Medicine, Department of Obstetrics, Gynecology and Reproductive Sciences) for her critical feedback and assistance with edit the manuscript. We thank Scribendi for their technical editing and proofreading services.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Author Biographies
At the University of California, San Francisco, Monica R. McLemore is a tenured associate professor in the Family Health Care Nursing Department, an affiliated scientist with Advancing New Standards in Reproductive Health, and a member of the Bixby Center for Global Reproductive Health. Dr. McLemore program of research is grounded in reproductive justice, a lens I use to understand reproductive health and rights for people with the capacity for pregnancy.