
Abstract
Preventive policies have been devised with the aim of curbing health-related violence, and their efficacy is believed to furnish evidence for their continued implementation, thereby enhancing their effectiveness. This study undertakes a retrospective analysis of these policies in the context of Türkiye. A comprehensive examination involved the review of 26 documents, employing a progressive scanning approach for data collection. This methodology encompassed the utilization of gray literature databases (OECD iLibrary and WHO Iris), extensive Google searches, thorough website scans, and consultations with subject-matter experts. Data analysis was meticulously conducted within the framework of the Health Policy Triangle. The findings reveal active participation from diverse stakeholders, including governmental bodies, political entities, professional organizations, and trade unions, in various preventive initiatives aimed at mitigating health-related violence. Notably, the adoption of legislation for health violence prevention, perceived as a paramount achievement, can be attributed to persistent efforts by both the media and other influential actors and stakeholders. These endeavors have sustained the topic's prominence on the policy agenda, positioning it as a promising source for the development of novel violence prevention and management strategies. This study underscores the necessity for a comprehensive investigation into the working conditions, personal rights, and wage policies of healthcare workers, in light of documented factors that frequently precipitate violence. Concomitantly, it advocates for the development of effective mechanisms to address these issues.
Introduction
Violence in healthcare settings is defined as verbal/behavioral threats and physical or sexual assaults against healthcare professionals by patients, their relatives, or any other persons (Annagür, 2010). In the realm of occupational hazards, the healthcare sector presents the most elevated level of risk (Bloom, 2019; Kim et al., 2019). According to the World Health Organization (WHO), it is estimated that a range of 8–38% of healthcare professionals experience physical violence at some point during their careers. Additionally, a significant number of healthcare workers are subjected to or face the risk of verbal aggression (WHO, 2022). The sources of violence in the workplace include reform pressures, increased workload and stress, social instability, and workplace violence resulting from the breakdown of personal relationships (ILO/ICN/WHO/PSI, 2002). It has been stated that personal factors, environmental factors, insufficient personnel, inadequate working environment, insecurity and miscommunication, and various other organizational factors may increase the risk of violence (Krug et al., 2002). Other factors that increase violence include the inadequacy of the healthcare system and technology in meeting the expectations of society and deficiencies in preventing and managing violence (Annagür, 2010).
Violence against healthcare professionals in developing countries is a persistent problem that is often overlooked and under-reported, affecting employee performance and motivation (Phillips, 2016). In recent years there has been an increase in workplace violence at a national and international level, and this has now become a public health problem. Poland, the Czech Republic, Slovakia, and Türkiye have all reported numerous cases of nurses experiencing physical assaults and verbal harassment within their workplace settings (Babiarczyk et al., 2019). While nurses are often identified as the most vulnerable group to workplace violence in various regions globally, in Türkiye, physicians and dentists have been reported as the most susceptible groups to workplace violence within the healthcare sector (Bayram et al., 2017). Studies have reported that the risk of violence against healthcare workers in the USA is 16 times higher than in other sectors, and the healthcare sector accounts for half of all violence complaints (Cooper & Swanson, 2002; Di Martino, 2002).
In Türkiye, several studies have been conducted to investigate the causes and types of violence, and these have shown a high incidence of violence in healthcare institutions and have concluded with certain suggestions (Cevik et al., 2020; Hamzaoglu & Turk, 2019). It is notable that most studies have focused on the frequency and type of violence, with very few examining and analyzing the policies used to prevent violence. Analysis of the success of a policy in achieving its objectives provides evidence for the development of future policies and contributes to their effectiveness (Pew-Macarthur, 2014). Health policy analysis entails the examination of legislation that exerts influence, whether directly or indirectly, upon health and its multifaceted dimensions. The implementation of health policy can be undertaken within both the public and private sectors, as documented in Mulcahy et al. (2022). Policy analysis is a multidisciplinary endeavor aimed at scrutinizing the interplay among institutions, concepts, and their contributions within a political process (Browne et al., 2019). In this context, there was seen to be a need for analysis of the policies in Türkiye for the prevention of violence in the healthcare system, both to evaluate current policy performance and to guide future policy-making processes. Therefore, the aim of this study was to examine the relevant documents and analyze the policy implemented for the prevention of violence in healthcare settings in Türkiye based on the Walt and Gilson (1994) policy analysis triangle.
Methods
The aim of this research was to retrospectively understand the successes and failures in Türkiye of the policies for the prevention of violence in the healthcare system, and to generate evidence that could be used by policymakers to design and implement future policies.
Policy Analysis Framework
The health policy triangle consists of four subcomponents: context, actors, content, and process. Content includes policy objectives, current policies, legislation, regulations, and guidelines. Actors refer to individuals, groups, and organizations that are influential in the policy-making process. The context describes the impact on policy of social, economic, political, cultural, and other environmental conditions. Process refers to the time when the policy is initiated, developed or formulated, negotiated, implemented, and evaluated (Buse et al., 2012).
Data Collection
This study used the qualitative research method of document analysis, which is a systematic process for reviewing and evaluating documents (Bowen, 2009). While collecting data, systematic review steps and procedures were applied, using a progressive scanning strategy developed by Godin et al. (2015) which allows all clear, repeatable, and relevant documents to be identified.
Inclusion Criteria
The inclusion criteria for documents in this study were defined as relevant policy documents produced by the government or nongovernmental interest groups, published reports (meeting, symposium, and congress), regulations, legal regulations, strategic plans, media, and activities of nongovernmental organizations. The most recent versions of the documents were included, those published in Turkish and English, and the year of publication was limited to the period 2003–2021.
Search Strategy
A stepwise scanning strategy was applied to access the documents appropriate for the study. According to this, (1) gray literature databases were searched, (2) specialized Google searches were conducted, (3) relevant websites were searched, and (4) expert consultations were conducted.
In the first step, gray literature databases were searched on November 18, 2021. Databases that catalog gray literature documents provide indexing, and in some cases, both print and online resources (Godin et al., 2015). Keywords in the search strategy were “violence,” “workplace violence,” “health,” “health workers,” “politics,” “Turkey.” Keywords were searched in all fields of the OECD iLibrary (482 results) and WHO IRIS (259 results) databases. The search results were imported to Microsoft Excel, and title analysis was used to eliminate duplicates. For further study, relevant documents (OECD iLibrary 1 and WHO IRIS 4) were selected.
The second stage involved conducting an extensive Google search using specific keywords. Given the challenge of analyzing all the search engine results, we limited our review to the first 10 pages, as suggested by O’Connell et al. (2018), to obtain the most relevant results for this study. Subsequently, we attempted to access additional documents through manual searches. A manual search was then conducted on the sites of the Ministry of Health, the Turkish Medical Association (TMA), the Grand National Assembly of Türkiye (TBMM) reports, the Health and Social Workers’ Union (Saglik-Sen), related organizations, nongovernmental organizations, and news sites. The on-site search engine was used to scan for keywords. Finally, experts in the field of health policy were consulted on the quality and accuracy of the scanned documents. The study included 26 documents related to the subject (Appendix A. Document List).
Selection and Synthesis of Documents
Two independent researchers (FS and YA) conducted title and content analysis on the documents retrieved from the scan results. The titles of relevant documents, potentially eligible for the study, were imported into Excel to create a list (document name, year, issuing institution/organization, and document type) for detailed text scanning. Subsequently, two researchers analyzed the text in detail and arrived at a final list of documents for review through consensus. Following a comprehensive review of each document included in the study, we analyzed the gathered information. To minimize bias, four different experts working in the field of health management and policy were given a work list and appropriate opinions were obtained.
Results
The findings of the study have been examined through the lens of the policy triangle analysis framework, which dissects the components of context, actors, content, and process within the policy domain.
Context
Violence in healthcare settings has increased significantly in recent years and has become a priority problem for both developed and developing countries. The WHO defines workplace violence as an important primary public health problem as well as a healthcare management problem (World Health Assembly, 1996). This situation has been defined by the World Medical Association (WMA) as an international emergency that undermines the foundations of health systems and critically affects the health of the patient. (WMA, 2020).
In Türkiye, the rise in violence against healthcare workers is related to certain structural reforms and policies implemented in recent years. The “Health Transformation Program (HTP),” which was implemented in 2003, is the most evident cause for this (TBMM, 2013; TMA, 2019, 2021). The HTP aims to organize, finance, and present healthcare services in an effective, efficient, and equitable manner. There are also reports and scientific studies claiming that HTP has increased health-related violence. For example, in the report entitled “Coping with Violence” published by the TMA Health Workers’ Health Working Group (2019), reasons stated to trigger violence include the inability to implement the referral chain, the payment of health services with differential fees and the increase in wages, the discrediting of healthcare professionals, and the transition to a performance-based system.
Actors
From the development of health policies to their implementation, national and international official/informal organizations, nongovernmental organizations, professional groups, trade unions, political parties, and the media all play a significant role.
According to a report violence in the healthcare sector has begun to gain more importance in public and government priorities. In addition to this report, organizations such as International Labour Organization, WHO, and OECD have laid the groundwork for governments’ policy-making agendas by discussing ways to deal with violence in healthcare globally through scientific studies, reports, and workshops (de Bienassis et al., 2021; ILO/ICN/WHO/PSI, 2002; WHO, 2020).
In Türkiye, the Ministry of Health is the most powerful entity in charge of ensuring patient and employee safety as well as the effective and efficient delivery of healthcare services. According to the data of the General Directorate of Health Services, as of 2020, 1,142,469 healthcare workers affiliated to the Ministry of Health are working in the provision of services (Ministry of Health, 2020b).
Professional organizations and trade unions make significant efforts to prevent violence in healthcare settings. According to data from the Resmi Gazete, Saglik-Sen is the authorized union of health and social workers with 248,951 members. The Strategic Research Center (SASAM), which is affiliated to Saglik-Sen, plays an important role in the policy and implementation process by producing evidence-based information on health, social, and labor policies in Türkiye (SASAM, 2015a). The TMA is one of the important actors in establishing a policy agenda and taking concrete steps for the prevention of violence in health. TMA, which is a public institution, was established with the law numbered 6,023 and represents approximately 100,000 physicians. Its main purpose is to protect and improve the level of health, as well as to protect the rights of the profession and its members. In addition, professional organizations, and trade unions such as the Federation of Family Physicians Associations (AHEF), Turkish Nurses Association (THD), Nurses and All Health Professionals Union (HEP-SEN), Turkish Intensive Care Nurses Association (TYBH), POLMEDER Association, and Health Services Union (SAHIM-Sen) play an active role in the policy-making process by carrying out activities to prevent violence.
Political parties are another actor that plays an important role in the formulation of health policies and decision-making processes, supporting the policies implemented by the current government or opposing them because they are not appropriate. The health policy monitoring board, formed within the party, puts pressure on the government to make the necessary arrangements and sets the agenda, where the policies for the prevention of violence in health are insufficient with the science platform policy notes. The media brings forward the activities of interest groups, political parties, professional associations, and other organizations to prevent violence in health and can communicate these to large sections of the population.
Contents
Significant changes in the delivery of healthcare were implemented because of the HTP. Several initiatives have been enacted to improve healthcare access. According to the data of the General Directorate of Health Services, while the average number of applications to a physician in primary, secondary, and tertiary health institutions was 3.1 in 2002, the number of applications to a physician per person increased to 9.8 in 2019. In Türkiye, the number of physicians per 1,000 people is 1.93, and the number of nurses and midwives per 1,000 people is 3.42 (Ministry of Health, 2020b). In OECD countries, the number of physicians per 1,000 persons is 3.6, whereas the number of nurses per 1,000 persons is 8.8 (OECD, 2021). The number of healthcare professionals in Türkiye is said to be insufficient to meet the delivery of services. The lack of time given to the patient puts pressure on healthcare professionals. Some legal arrangements have been implemented, and various policies have been given prominence to prevent an increase in health-related violence. Politicians from differing perspectives have provided proposal drafts, and various legal regulations and legislative initiatives have been approved due to the work of the Ministry of Health and other relevant actors. Reports, press releases, and advertisements have been made by professional organizations, trade unions, and various nongovernmental organizations. For example, the TMA acted against the regulation allowing physicians to see two patients in 10 min in the Central Physician Appointment System. As a result of the press statements they made and the related regulation to the judiciary, the execution of the regulation was stopped on December 9, 2021, by the decision of the administrative court, due to the lack of any scientific basis, not protecting the public interest, and the problems experienced between physicians and patients (TMA, 2022).
Process
In Türkiye, policy strategies to prevent health-related violence have been studied under two headings: legal regulations and other activities related to the policy-making process.
Legal Regulations
The first of the legal regulations made for the prevention of violence is the “Communiqué on the Implementation Procedures and Principles of Emergency Services in Inpatient Health Facilities” that came into force in 2009 (Resmi Gazete, 2009). The Communiqué makes it compulsory for the relevant institution to take the required precautions to ensure the safety of patients, their families, and workers when providing emergency services. Subsequently, in 2011, the “Regulation on Ensuring Patient and Employee Safety” came into force (Resmi Gazete, 2011a). The main purpose of the regulation is to ensure patient and employee safety in secondary and tertiary healthcare institutions providing healthcare services. To provide a safe working environment, determining and eliminating risk factors and planning for the implementation of necessary methods are explained. The Ministry of Health and its affiliates issued Decree-Law No. 663 on the Organization and Duties of the Ministry of Health and its Affiliates in 2011, to provide legal assistance to personnel if they requested it because of crimes committed against them while providing health services (Resmi Gazete, 2011b). In connection with this regulation, the “Regulation on the Procedures and Principles of Legal Aid to be Provided for Crimes Committed Against the Ministry of Health Personnel” was published in 2012 (Resmi Gazete, 2012). The regulation ensures the provision of legal assistance for healthcare workers against whom a crime is committed during the provision of healthcare services or due to their duties. Within the scope of patient and employee safety, the “Patient and Employee Safety Circular” was published in 2012 (Ministry of Health, 2012). The circular included the creation of a committee to ensure employee safety, the preparation of a program, a regulation for the prevention of violence, training, and the “White Code” application, which would be implemented for the first time, as well as the decision to establish the “113 White Code Call Center,” which would be available regularly. Within the scope of patient and employee safety, the “Patient and Employee Safety Circular” was published in 2012 (Ministry of Health, 2012). The white code application has been in use since 2015, and according to the Ministry of Health (Ministry of Health, 2020a), 11,691 applications were submitted in 2020. The “Circular on Investigation of Crimes Committed Against Healthcare Professionals” was published by the Ministry of Interior on April 26, 2012 (Ministry of Interior, 2012). The circular states that if a healthcare worker is injured, threatened, or abused, the “hospital police” will intervene without requesting a complaint, and the appropriate legal procedures will be started. Despite all legal regulations and efforts, violence against healthcare workers has not decreased. Therefore, most recently, the “Draft Law on Amending the Health Services Fundamental Law,” also known as the “Violence in Health Law,” was adopted in 2020 with the joint decision of the political parties (Resmi Gazete, 2020). According to the legislation, the penalty for injuring, threatening, insulting, or hindering healthcare personnel should be increased by half, and the prison sentence should not be suspended. Penalties range from 3 months to 4 years, depending on the type and severity of the crime committed in the relevant legislation. However, in the case of violence, the legislation states that healthcare services shall be provided by another healthcare worker if one is available. Figure 1 depicts the timetable for the above-mentioned procedure.
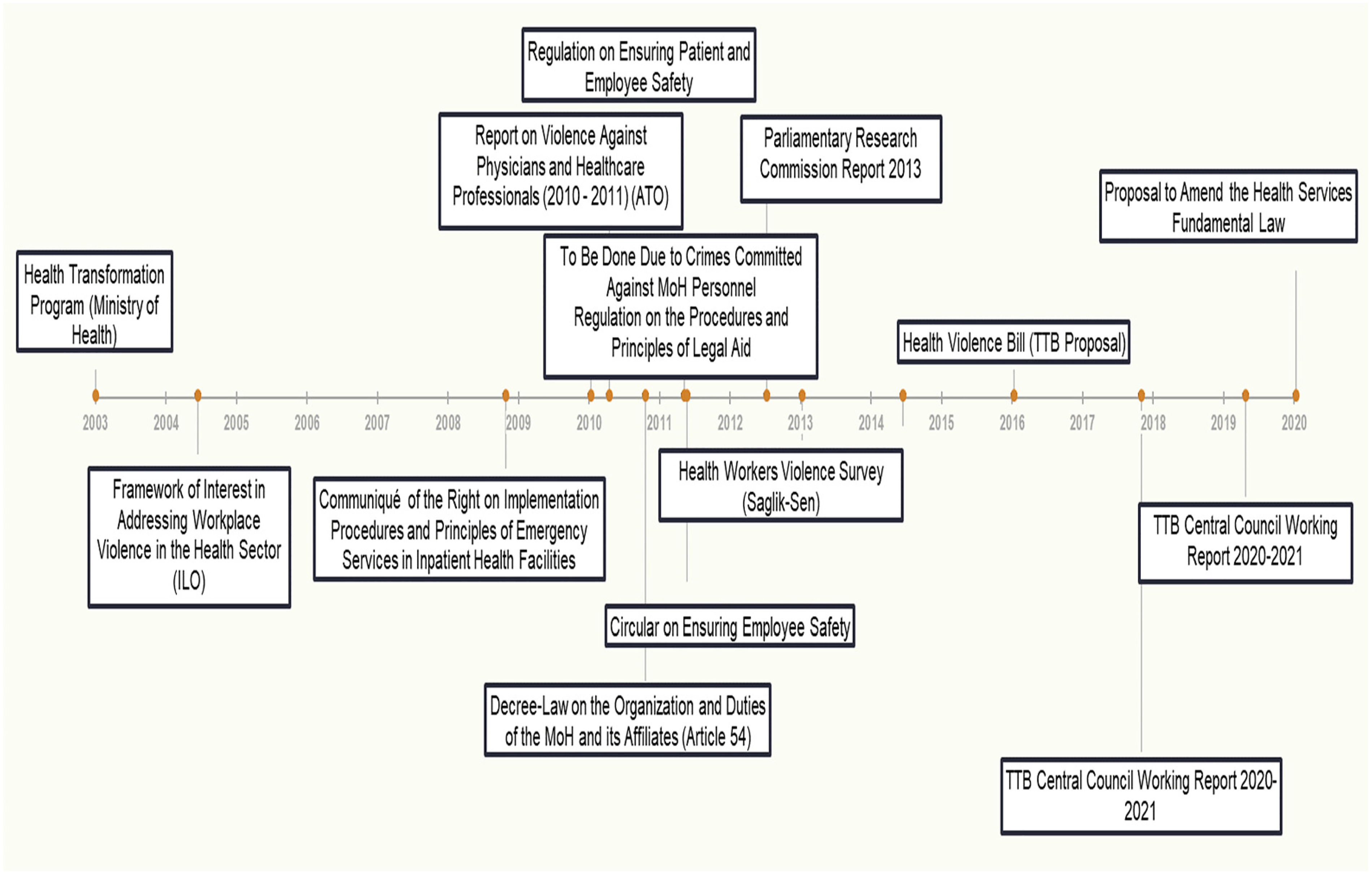
Timeline of policy implementations and related documents to prevent violence.
Other Activities Related to the Policy-Making Process
Ankara Medical Chamber (AMC) published a report on the activities carried out to prevent violence against physicians and other healthcare professionals (AMC, 2011). In the report, the health policies applied, neo-liberal policies, and negative attitudes of the media, politicians, and administrators are shown as the causes of violence in healthcare settings. It was emphasized that the working conditions of healthcare professionals are inadequate for providing services. In addition, the “Violence Notification Line” was established, the applications were evaluated, and the reports were shared with the public and the parliamentary health commission. In a report published by Saglik-Sen, it was stated that 86.8% of health workers have been exposed to violence at least once during their professional life (Saglik-Sen, 2013). In the report, comparisons were made regarding demographic characteristics, concerns of healthcare professionals about violence, and the extent and scope of violence. To prevent violence, suggestions were made regarding security, education and social services, legal regulations, working conditions, and the media. In parliament, 10 proposals signed by a total of 246 deputies have been presented at different times by politicians to investigate the causes of violence against healthcare workers. Among the common points of the proposals are the exposure of healthcare workers to violence, the HTP, the performance system, the attitudes of managers triggering violence in health, inadequate working conditions, and problems related to worker safety. In April 2012, a commission “To Investigate Increasing Incidents of Violence Against Healthcare Professionals and Determine the Measures to be taken” was agreed to be formed as per the recommendations. A report was published by the commission in 2013. The report discussed the healthcare system and policies while the phenomenon of violence against healthcare workers was also another point under scrutiny, and the methods of coping with violence in other countries were examined. The extent and causes underlying the increase in violence toward healthcare workers in Türkiye were researched, and suggestions were made in organizational, institutional, social, and environmental terms. Launched in 2004, “Ministry of Health Communication Center (SABIM)” and “ALO 184” telephone line applications aimed to increase patient satisfaction and expectations as a component of the HTP. However, they were not adequately promoted to the public, put pressure on healthcare workers, and are perceived as a complaint channel by the public. “Respect for Labor Zero Tolerance to Violence Symposium” was held with the participation of various nongovernmental organizations. A “Zero Tolerance for Violence” campaign was launched at the national level (TBMM, 2013). In the “Health Quality Standards (Version 6)” guide issued by the Ministry of Health, the standard for making the necessary arrangements for the prevention of violence against healthcare workers was determined as an indicator (Ministry of Health, 2020c). The Turkish Health Policy Institute (TUSPE) carries out research and development activities for health management and related fields by adopting the philosophy of an evidence-based approach in the process of creating health policies. It defines violence in health as a public health and occupational health problem as well as a safety problem. To understand the theoretical framework of violence in health, it published the analytical research “Violence in the Health Workplaces: A Theoretical Framework.” This highlights the concept and extent of violence, root causes of violence, and possible consequences and urges the management of violence in health-related workplaces (Yildirim, 2018).
TMA conducts “Violence Working Group” initiatives to prevent health-related violence. To report violence against healthcare workers, a “Violence Hotline” was established in some provinces, and a “Violence Notification Form” section was created on its website. In addition, the Health Workers’ Health Working Group has published a brochure on “Dealing with Violence.” The TMA emphasizes that one of the reasons for the increase in violence against healthcare workers is the lack of or insufficient legal sanctions against individuals who perpetrate violence. For this reason, they prepared a “Violence in Health Draft Law” and proposed an additional article to the Turkish Penal Code (Tip Dünyasi, 2017). AHEF (2014) stated in a press release that lack of healthcare provider standards, constantly changing health legislation, increasing workloads, negative media attitudes toward healthcare professionals, and frequent changes in cost recovery institution regulations all contribute to increased violence in healthcare. SASAM (2015b) has emphasized the need for joint action with proactive approaches to prevent the phenomenon of violence. In a joint press release made by THD and some professional organizations, it was stated that the legal regulations for the prevention of violence are insufficient and that violence continues at the same pace (THD, 2021). The Ministry of Health plans to increase training and awareness activities to prevent violence as well as preventative actions by conducting root cause analyses of healthcare institutions (Ministry of Health, 2019). The Ministry of Health 2021 Institutional Financial Status and Expectations Report states that “Prevention of Violence in Health Action Plan 2021–2023” studies will continue (Ministry of Health, 2021a). The “Mobile Color Code Application” is given as an example of good practice in Kayseri City Hospital affiliated with the Ministry of Health. The application was completed in the high-security forensic psychiatry unit, where personnel violence is much more frequent. It was stated that the access to the white code incidents with an electric scooter shortened the response time making it possible to intervene in incidents before they escalated (Ministry of Health, 2021b).
Discussion
Especially in the process of adopting the law on the prevention of violence in health, which is seen as the most important gain, it has been seen that the long-term efforts of both the media and other actors and stakeholders have maintained their place on the agenda. In particular, the research taught an important lesson for each stage of the cycle of policies aimed at preventing violence in health.
As a result of the documents examined in the study, it was seen that the government, politicians, professional organizations, and trade unions all participate in certain preventative initiatives aimed at reducing health-related violence. In the policy-making process, although it is sometimes only the political power that determines the policy or puts it into practice, other actors are involved in the process in some way. It can be said that the agenda, which is determined as high-level and hegemonic, is aimed at achieving a social consensus on the prevention of violence in health by creating a consensus between nongovernmental actors and stakeholders.
The phenomenon of violence in the world is considered to require an important struggle policy that cannot be reduced to the basis of legal regulations. The cases of violence in health, which continue after the legal regulations entered into force, reveal this reality. Studies conducted in the process from the HTP process to the present day (2003–2021) show that the violence has not decreased when examined. In the studies, the frequency of violence faced by physicians has been reported to vary between 68% and 96.2%. 9–13 with verbal violence the most common type, at an incidence varying between 41.8% and 89.3% (Acik et al., 2008; Aksakal et al., 2015; Aytac et al., 2011; Hamzaoglu & Turkoglu, 2019; Pinar et al., 2017). At this point, the evaluation strengthens the assumption that only increasing the punishment for the perpetrator of violence will not be sufficient to prevent violence. Therefore, in terms of the crime and punishment policy carried out, whether the aggravation of sanctions provides an adequate level of prevention is a different research topic that needs to be evaluated. In addition, it is considered that the feedback mechanism is not sufficient for the evaluation of policy outcomes and reporting of the results. In a study by Çelik et al. (2017), it was stated that most healthcare professionals believe that the current policies of healthcare institutions and the Ministry of Health are insufficient to effectively prevent workplace violence. In some other studies, the style used in the policies followed in Türkiye, the lack of security personnel and their inadequate authority, the inadequacy of the laws to prevent violence against healthcare professionals (Hamzaoglu & Turkoglu, 2019), income-oriented approaches, and market-based restructuring (Cevik et al., 2020) have been stated to increase violence, and patients and their relatives see healthcare professionals as responsible for the problems, and these situations are reflected as violence against healthcare workers (Sevimli, 2020). There are also studies with findings presenting different aspects, such as the fact that many victims of physical violence or verbal abuse did not report the incident because they did not believe it would be of any help (Pinar et al., 2017). A review of the literature highlights the lack of a set of policies and procedures that reveal the consequences of violence and the necessity of prevention in similar studies (Civilotti, 2021). Furthermore, it is effective in attracting public attention by emphasizing the importance of violence in health. However, it has been stated that the media has both a positive and negative role in preventing health-related violence and that administrators’ rhetoric and attitudes are among the aspects that influence increased health-related violence in cases of violence represented in the media (Baykan et al., 2015).
Conclusion
In this study, a retrospective analysis of the policy of preventing violence against health workers, which is accepted as a global public health problem, was made. Actors set the agenda by evaluating and analyzing the causes of violence in health and producing solutions. It is also noteworthy that they serve as a strong lobbying force in the development of legal regulations. The enactment of the law on the prevention of violence in health is an important step taken. The relevant regulation can be described as an important legal reform in terms of occupational safety of health workers who provide health services with great devotion, especially during the pandemic period. Occupational health providers and policymakers can create a centralized feedback system to find the success of established policies and the root cause of violence. Legal counseling services, psychological and social support opportunities can be provided to health workers who have been subjected to violence.
This study detailed a retrospective analysis of the policy for violence prevention against healthcare professionals, which is considered a global public health concern. It can be considered a source for new policies to be put forward in terms of violence prevention and management strategies. Based on the reasons stated in the documents that often lead to violence, the health worker’s working conditions, personal rights, wage policy should be examined in detail and solution mechanisms should be developed. Future research can explore the root causes of problems by enabling all stakeholders to work together to create a lasting and sustainable strategy. Community-level interventions can have a universally positive impact on reducing the violence that occurs in all healthcare settings. Instead of addressing the problem from the perspective of individual factors and micro-management, it can be addressed more broadly with a broader systematic structure through inclusive macro-management. By taking examples of policy analysis research from different countries and cultures, comprehensive and permanent solutions can be produced for violence in healthcare settings, which is a global problem. By analyzing the policies implemented to prevent violence in healthcare settings, the article highlights the need for additional research on the phenomenon of violence in health, especially more detailed analyses to understand the causes and social dimension of violence in health and its impact on society.
Supplemental Material
sj-docx-1-ppn-10.1177_15271544241232382 - Supplemental material for Why Violence Cannot be Prevented in Healthcare Settings in Türkiye?: A Retrospective Policy Analysis
Supplemental material, sj-docx-1-ppn-10.1177_15271544241232382 for Why Violence Cannot be Prevented in Healthcare Settings in Türkiye?: A Retrospective Policy Analysis by Ferit Sevim and Yasemin Akbulut in Policy, Politics, & Nursing Practice
Footnotes
Authors’ Contributions
All authors contributed equally to the writing of this paper.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.