
Abstract
Objective
: This study assesses how providers delivered telehealth services to pregnant Medicaid enrollees, using multistate Medicaid claims data. It also examines how provider rurality and state-level telehealth policies influenced provision.
Methods
: We analyzed claims data on telehealth provision from the Transformed Medicaid Statistical Information System Technical Analytic File from January 2020 to April 2021. Monthly telehealth provision was estimated for family physicians, obstetricians and gynecologists, nurse practitioners, and physician associates, and variations therein were examined by rurality and state policy.
Results
: Telehealth provision peaked in April 2020, when 19.5% of providers delivered at least one telehealth service. At the peak in April 2020, rural providers were less likely to provide telehealth than urban providers (15.2% vs. 20.6%), and states with telehealth-supportive policies saw higher provision of telehealth by providers (20.9%) than those without (14.3%). Throughout the study period, rural providers from all specialties in nonsupportive policy states showed the lowest telehealth provision.
Conclusions
: Provider location rurality and state policy environments significantly influenced telehealth provision. Sustained policy support is essential to ensure equitable access to perinatal care.
Introduction
The United States lags behind other developed nations in maternal health outcomes, a gap often driven by disrupted perinatal care access. 1 Structural factors such as systemic racism, health professional shortages, hospital closures, and transportation barriers contribute to these disparities, particularly in rural and underserved communities.2,3 Telehealth has emerged as a promising strategy to mitigate some of these barriers by offering remote access to care, especially when in-person services are limited or unavailable.
Before the COVID-19 pandemic, telehealth use for prenatal care was minimal. However, the onset of the pandemic catalyzed a rapid expansion in telehealth delivery, particularly during the early months of the COVID-19 Public Health Emergency (PHE). Claims-based analyses show that telehealth provision surged in early 2020. This increase was especially pronounced among providers serving patients with high-risk pregnancies and those with chronic conditions such as anxiety and gestational diabetes.4–6 Utilization was consistently lower in rural areas, reflecting longstanding disparities in digital infrastructure and provider availability.7,8 Notably, while rural and underserved communities were less likely to use telehealth prepandemic, this trend appears to have reversed in the years following the initial surge.9–11
In this study, we examined how telehealth was delivered to pregnant women enrolled in Medicaid during the early period of the PHE, with a focus on rural providers and on states that had policies supportive of telehealth adoption. Medicaid covers more births than any other payer in the United States, yet it remains unclear how rural providers deliver telehealth to care for this population. This gap in evidence is particularly concerning since multiple telehealth flexibilities that were introduced under the PHE have expired or are set to expire, raising concerns about a potential “telehealth policy cliff”-a sudden reduction in access due to the expiration of temporary flexibilities. 12 This could disproportionately affect rural communities.
State-level telehealth policies, particularly payment parity laws, have played a significant role in shaping access. For example, obstetricians and gynecologists (Ob/Gyns) practicing in states with telehealth payment parity laws delivered more telehealth visits on average, likely due to expanded coverage and reimbursement policies. 6 Prior research also indicates that expanded telehealth flexibility in commercial insurance and Medicare during the COVID-19 pandemic was associated with a substantial increase in telehealth utilization.13,14 Thus, understanding the combined impact of rurality and policy environment is essential for informing Medicaid strategy and ensuring equitable access to care. Building on prior evidence, we hypothesize that supportive telehealth policies, such as payment parity laws, may have spillover effects that enhance telehealth provision for Medicaid enrollees, particularly in rural areas.
Given the substantial policy variation across states, our findings offer timely insights to inform state policymakers amid impending Medicaid budget pressures. They are also relevant as states consider which strategies to adopt under the Rural Health Transformation Program, which can potentially improve maternal health outcomes and reduce disparities for rural pregnant women through innovative care delivery models. 15
Methods
We examined the provision of telehealth to Medicaid-covered pregnant enrollees just before and during the COVID-19 pandemic using data from the Transformed Medicaid Statistical Information System Technical Analytic File (TAF). Since we did not have full information about enrollees who were pregnant during 2022 and who may have received telehealth during the latter part of 2021, the analytic period was restricted from January 2020 to April 2021. We began by identifying pregnant Medicaid enrollees using algorithms developed by the Centers for Medicaid and Medicare. 16 Telehealth services were identified using Current Procedural Terminology codes, as well as modifiers that appear on medical claims (see Supplementary Tables S1 and S2). The main study outcome was the proportion of providers who delivered any telehealth services to pregnant Medicaid enrollees during each month of the study period.
To better understand how providers from different specialties and professions delivered telehealth to pregnant Medicaid enrollees, we used data from the National Plan and Provider Enumeration System (NPPES) and focused on those most involved in perinatal care, including: Ob/Gyns, family physicians (FP), nurse practitioners (NPs), and physician associates (PAs). We categorized the rurality of each provider’s practice location by first identifying the ZIP code of their practice in the NPPES and then linking this information to data from the Federal Office of Rural Health Policy. 17
To evaluate the impact of state-level telehealth policies, we classified states according to the presence or absence of laws mandating coverage and payment parity. Using the methodology outlined by Yen et al., we identified states without such laws; all others were considered to have telehealth-supportive policies (see state categorization in Supplementary Table S3). 18
All providers from selected specialties who provided any service to pregnant Medicaid enrollees were part of the study sample. We included providers from states whose TAF (Medicaid claims) data met quality standards. Data quality assessment was based on two criteria: (1) The percentage of claims missing information about the service-providing provider and (2) The consistency between the total number of deliveries identified in TAF and the total number of Medicaid-funded births reported using birth certificate information in CDC WONDER data system. 19 As a result, providers from 13 states were excluded due to poor data quality (Arkansas, Connecticut, Delaware, Florida, Massachusetts, Maine, Minnesota, New Hampshire, New Jersey, Oklahoma, Rhode Island, Tennessee, Texas, and Utah). The final sample included data on 260,744 unique providers from 37 states.
We conducted two-sample t-tests to compare the proportion of providers who delivered telehealth to pregnant Medicaid enrollees across (1) states with and without telehealth-supportive policies and (2) rural versus urban settings. These tests assessed whether observed differences were statistically significant in each month from January 2020 to April 2021, using a threshold of p < 0.05 to indicate statistical significance. All analyses were conducted using Stata 19. This study was determined to be exempt by the institutional review board of the author’s organization.
Results
Telehealth provision peaked during April 2020, when about 19.5% (20,003 out of 102,763) providers delivered at least one telehealth service to pregnant Medicaid enrollees (Table 1). By April 2021, this proportion declined to about 10% (10,782 out of 109,463). Specialties differed in terms of telehealth provision; at the peak (April 2020), 20.9% FPs, 23.3% Ob/Gyns, 19.4% NPs, and 10.7% PAs provided at least one telehealth service (Supplementary Table S4). Telehealth provision differed by the rurality of providers’ practice locations. During April 2020, 15.2% (3,196 out of 21,011) of rural providers provided telehealth, compared with 20.6% (16,807 out of 81,752) of urban providers (Table 1). By April 2021, these rates had declined to 6.3% (1,366 out of 21,553) for rural providers and 10.7% (9,416 out of 87,910) for urban providers. State policies also influenced telehealth provision: in April 2020, only 14.3% (3,254 out of 22,741) of providers in states without telehealth-supportive policies provided telehealth, compared with 20.9% (16,749 out of 80,022) in states with supportive policies (Table 2). These proportions declined to 6.6% (1,632 out of 24,687) and 10.8% (9,150 out of 84,776), respectively.
Monthly Trends in Provision of Telehealth to Pregnant Medicaid Enrollees by Rurality, January 2020 to April 2021
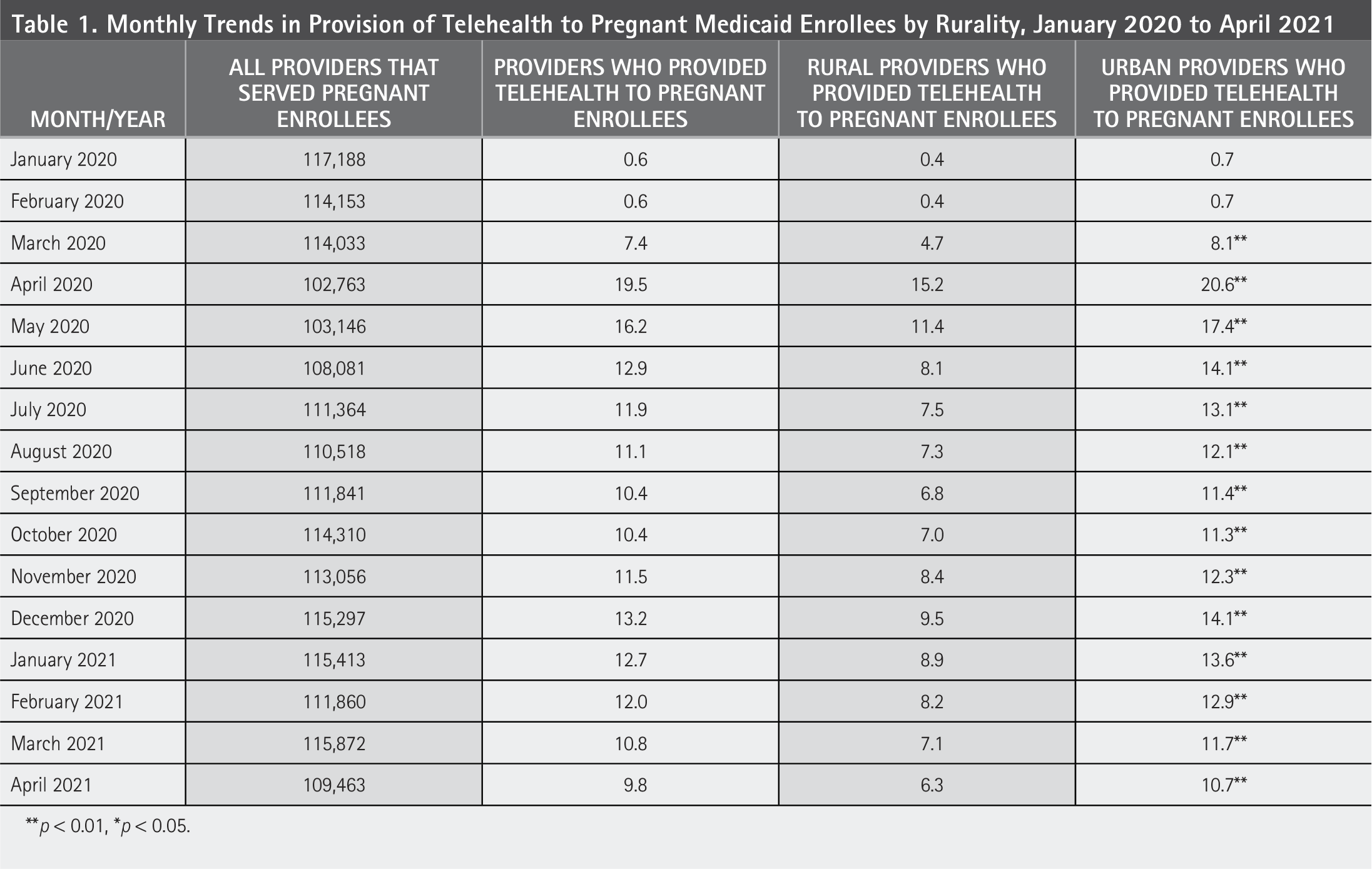
p < 0.01, *p < 0.05.
Monthly Trends in Provision of Telehealth to Pregnant Medicaid Enrollees by State Telehealth Policy Environment, January 2020 to April 2021
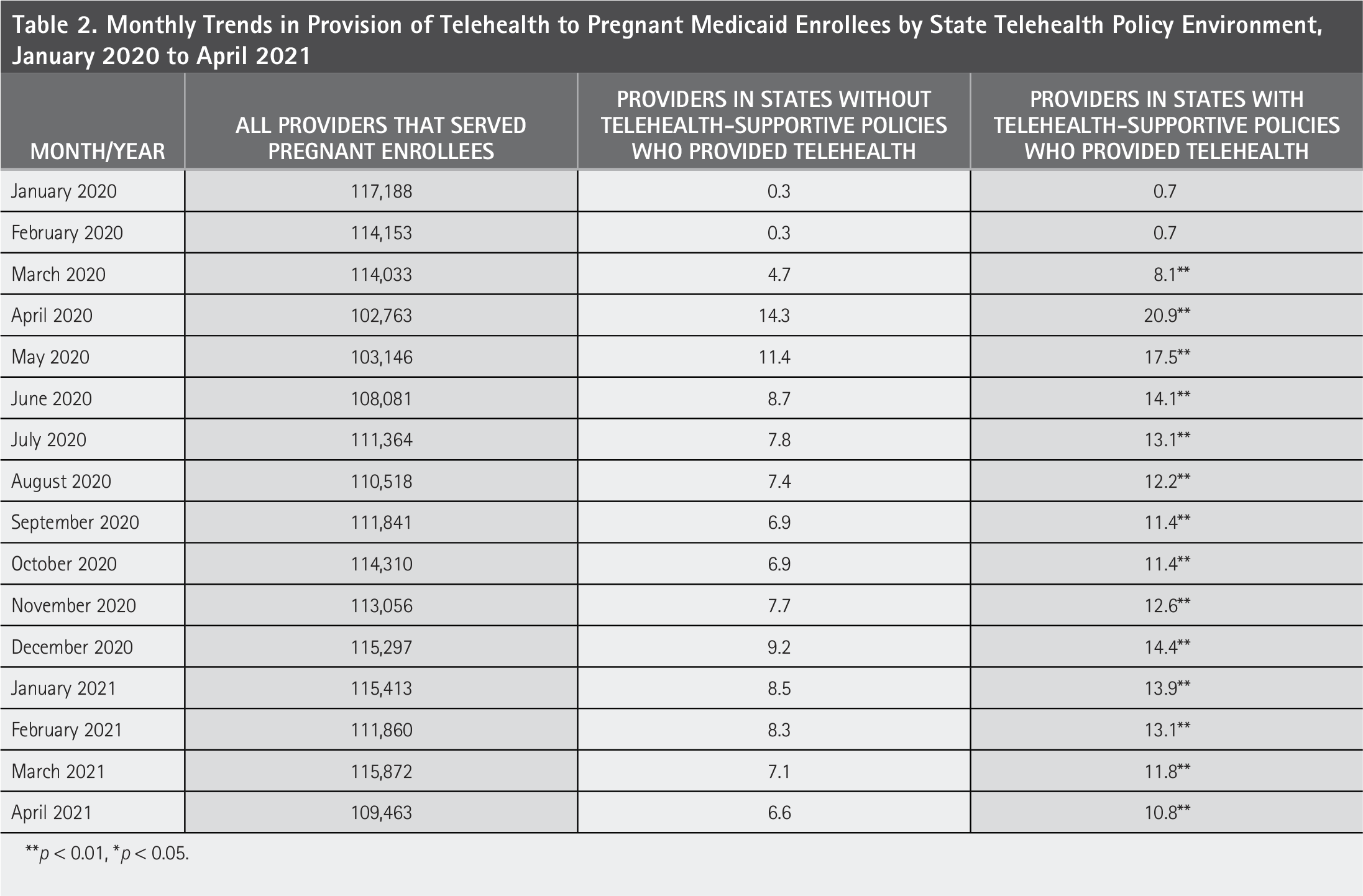
p < 0.01, *p < 0.05.
Notably, across all specialties and professions, urban providers practicing in states with telehealth supportive policies consistently showed higher levels of telehealth provision compared with those in states without such policies (Fig. 1, Panels A and C). Among urban providers in supportive-policy states (Fig. 1, Panel A), NPs and Family Physicians reached early pandemic peaks near 25%, while Ob/Gyns peaked slightly lower (20%) and followed a similar trajectory. These groups maintained elevated provision through 2021, with NPs and family physicians sustaining higher levels relative to their initial surge. In nonsupportive states (Fig. 1, Panel C), all three specialties exhibited comparable initial increases but declined more sharply after mid2020, stabilizing around 10% to 15% by late 2021.

Provider telehealth provision by state policy environment and rurality. Description: This figure shows the differences in the proportion of providers that provided telehealth to pregnant Medicaid enrollees by specialty, rurality of location, and state telehealth policy characteristics. Explanation of symbols: Nurse Practitioners;  Obstetricians and Gynecologists;
Obstetricians and Gynecologists;  Family Medicine;
Family Medicine;  Physician Associates. Dotted lines indicate rural location.
Physician Associates. Dotted lines indicate rural location.
The difference in telehealth provision was also evident across the urban–rural spectrum (Fig. 1, Panels B and D). Rural providers in supportive-policy states (Fig. 1, Panel B) mirrored urban patterns but at lower levels: NPs and family physicians peaked near 20%, and Ob/Gyns at levels slightly below that, with moderate persistence over time. In contrast, rural providers in nonsupportive states (Fig. 1, Panel D) had the lowest telehealth engagement overall. NPs and family physicians peaked below 15%, and Ob/Gyns followed a similar downward trend, dropping to single digits by mid-2020 and remaining minimal thereafter. These patterns underscore how policy environment and rurality jointly shaped telehealth provision across specialties during the early years of the PHE.
Discussion
Results suggest that at the start of the COVID pandemic, nearly a fifth of providers provided telehealth services to pregnant Medicaid enrollees. However, this proportion fell by half in April 2021. Both state-level telehealth policies and rurality were important factors influencing the extent to which providers engage in the provision of telehealth services to pregnant Medicaid enrollees. While the first year of the COVID-19 pandemic was unique in terms of widespread policy flexibilities and relatively stable Medicaid enrollee populations, findings from this period remain relevant even in today’s shifting landscape. As states face Medicaid budget constraints and enrollment declines, provider engagement with Medicaid enrollees may diminish.
Our findings align with broader national trends in telehealth use during pregnancy. Acharya et al. (2023) found that telehealth utilization among commercially insured pregnant individuals peaked in April 2020. However, by late 2021, usage had declined significantly, mirroring the drop observed in Medicaid populations. In another analysis of commercial insurance claims data, Bodas et al. (2025) documented a sharp rise in telehealth provision by Ob/Gyns during the early pandemic, followed by a steady decline through 2022. This analysis also revealed that provider characteristics and state-level payment parity policies influenced the intensity of telehealth use. Further, results of the current study also align with Doza et al. (2025), who found that rural patients consistently had lower telehealth utilization rates for prenatal care than their urban counterparts, despite policy efforts to expand access.
Study findings are increasingly salient as states have indicated their intent to reduce Medicaid provider reimbursement in anticipation of federal budget cuts. 20 Early reductions in payment rates may further limit provider participation, particularly in rural areas where access is already constrained. 21 Telehealth service access was expanded under pandemic-era flexibilities, but is especially vulnerable to rollback. Without sustained reimbursement and policy support, the gains observed during the pandemic may not be maintained.
Limitations
This study has limitations. As a descriptive analysis of trends in telehealth provision, it does not support causal inferences. TAF data are known to have quality issues, which may have impacted study results.
Conclusions
This study offers one of the earliest estimates of telehealth provision to pregnant Medicaid enrollees during the PHE. The findings highlight how providers and enrollees in rural areas may face additional barriers in providing or accessing telehealth, even within states that have adopted supportive telehealth policies. Study findings underscore the importance of stable financing and regulatory frameworks to ensure continued access to telehealth for pregnant Medicaid enrollees, especially in regions facing potential provider shortages and declining enrollment.
Author Disclosures Statement
No competing financial interests exist.
Authors’ Contributions
M.B.: Conceptualization, methodology, software, validation, formal analysis, investigation, data curation, writing—original draft, writing—review and editing, visualization, supervision, project administration. Y.H.P.: Software, validation, formal analysis, data curation. Q.L.: Software, validation, formal analysis, data curation. A.V.: Conceptualization, methodology, investigation, writing—original draft, writing—review and editing, supervision, project administration.
Footnotes
Funding Information
This project was supported by the Bureau of Health Workforce (BHW), National Center for HealthWorkforce Analysis (NCHWA), Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) as part of an award totaling $450,000, with zero percent financed with nongovernmental sources. The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement by HRSA, HHS, or the U.S. Government.