
Abstract
Telehealth may improve access to specialized oncology care for Medicaid beneficiaries with hematological malignancies who face geographic and financial barriers. During the COVID-19 public health emergency, telehealth use expanded rapidly, yet state policies governing telehealth coverage/payment parity varied. Evidence is limited on how these policy differences influenced oncology telehealth use for Medicaid patients. We conducted a cross-sectional analysis of 2020–2021 multistate Medicaid claims. Adult and pediatric oncology specialists were identified based on board certification data. Telehealth video visits were measured monthly at the extensive margin, defined as the proportion of specialists providing any telehealth, and the intensive margin, defined as average monthly telehealth visits among telehealth providing specialists. States were categorized by private insurance telehealth policy environment: coverage and payment parity, coverage parity only, or no or unspecified parity. Telehealth use increased sharply across all states in early 2020, rising from less than 1% of specialists before the pandemic to peak levels by April 2020. Specialists practicing in coverage and payment parity states demonstrated higher and more sustained telehealth use through 2021 compared with those in coverage only or no parity states. By December 2021, 15.1% of adult specialists in coverage and payment parity states provided telehealth, compared with 8.1% in coverage-only states and 7.8% in no-parity states. Pediatric specialists showed similar patterns, though overall telehealth use remained lower. Specialists in parity states also maintained higher monthly telehealth visit volumes over time. State-level coverage and payment parity policies may have been associated with greater and sustained telehealth provision by oncology specialists treating Medicaid beneficiaries with hematologic malignancies. Maintaining supportive telehealth policies may be essential for promoting equitable access to specialized cancer care and reducing disparities among underserved populations. These findings inform future telehealth policy decisions nationally statewide.
Introduction
Telehealth is viewed by providers and payors as a promising strategy to increase access to care, particularly for rural populations and those with unmet social needs that prevent them from traveling to regional cancer centers.1,2 Patients with hematological malignancy frequently require highly specialized services such as evaluation for allogeneic hematopoietic stem cell transplantation (HCT), CAR-T cell therapy, intensive chemotherapy regimens, immunotherapies, and clinical trial enrollment, which are typically available only at major academic medical centers. Distance from HCT centers is substantial for many Medicaid beneficiaries. 3 For instance, in one study of 1,136 patients from 6 centers in the United States the median driving distance was 82 miles, and 44% of survivors lived 100 miles or more from their HCT center, underscoring the considerable travel burden. 4 These access challenges are compounded in states with restrictive Medicaid coverage policies for HCT or limited networks of transplant-capable hospitals. As a result, patients may be forced to cross state lines or wait extended periods to receive necessary evaluation and treatment.
Telehealth offers a critical bridge in these scenarios by improving access to specialist for assessment and potentially curative therapies such as alloHCT. Telehealth helps to reduce the frequency of in-person visits and improves care continuity for patients facing logistical and financial barriers to specialty hematologic care. 5 Additionally, for follow-up care and ongoing surveillance, telehealth can alleviate out-of-pocket expenses for travel and lodging and reduce missed work, which is often a crucial issue for patients and caregivers facing financial hardships.6,7 While there is limited research, a study conducted prior to the pandemic suggests telehealth provided by oncologists to rural cancer patients can be a sustainable model to reduce patient costs and travel time. 8 Despite evidence of the rapid uptake of telehealth for hematologic care, no study has estimated its provision to Medicaid beneficiaries with hematologic malignancies.
Prior to the pandemic, Medicare telehealth coverage was limited, and there was wide variation across states about what services were covered for which population, payer, or provider type and how much reimbursement they would receive.9,10 However, as telehealth use surged in response to the COVID-19 pandemic, the Center for Medicare and Medicaid Services (CMS) quickly adopted telehealth coverage and payment parity policies for Medicare beneficiaries, making them consistent with Medicaid, where states were required to offer payment parity unless they seek a CMS exception, resulting in de facto payment parity across states. 11 However, while the number of states with private insurance parity laws expanded during the pandemic, variation across states remained, with some mandating both coverage and payment parity, others only coverage, and some neither.12,13
Variation in state and federal telehealth rules creates a natural experiment to test whether alignment across dominant payers (Medicare, Medicaid, and commercial insurers) drives broader telehealth adoption through spillover effects on physician behavior. In health care, physicians typically standardize workflows across payer panels; when a large payer changes rules or reimbursement, those practice norms often diffuse to patients with other coverage, an externality repeatedly documented for Medicare policies. 14
Emerging oncology-specific evidence shows that states with alignment of coverage and payment parity saw more sustained telehealth use among privately insured cancer patients, compared with states that had coverage-only or no parity. 12 Because Medicare and large commercial plans set the operational “default” for practices, their telehealth rules (e.g., covered services, modality, payment levels) can shape how oncologists design visits for all patients, not just the patients in those plans. If similar spillovers occur, greater alignment such as private-payer parity paired with stable Medicare telehealth flexibilities could encourage oncologists to offer telehealth to Medicaid patients through standardized workflows. What remains unclear is whether these spillover effects extended to oncologists’ provision of telehealth to Medicaid patients with hematologic malignancy. To explore this, we examine telehealth use among oncology specialists treating Medicaid beneficiaries with hematological malignancy across states with differing private-insurance parity policies.
Methods
We conducted a cross-sectional analysis of 2020–2021 multistate Medicaid claims using the Transformed Medicaid Statistical Information System Analytic Files (TAF). TAF includes diagnosis and procedure codes and provider identifiers. Patients with hematologic malignancy were identified by having at least 2 claims of relevant ICD-10 diagnosis codes in a 90-day period. 15 Specialists were included: board certified medical oncologists, hematologists, hematologist-oncologists (hereafter adult specialists), and pediatric hematologist-oncologists with at least one patient with hematologic malignancy. Telehealth video visits were defined using procedure codes/modifiers and calculated monthly at the extensive margin (proportion of specialists providing any telehealth) and intensive margin (average monthly telehealth visits among specialists who provided telehealth) by state policy categories: coverage parity only, coverage and payment parity, or no parity. 12 Additional details are included in the Supplementary Data.
Results
Telehealth provision by adult and pediatric specialists increased sharply in response to the public health emergency and varied by state coverage/payment parity status. While less than 1% of specialists offered telehealth in early 2020, it surged for all by April 2020. Among adult specialists, 28.9% (n = 988) in 17 coverage/payment parity states offered telehealth, 28.2% (n = 663) in 16 coverage-only states, and 19.2% (n = 311) in 10 states with no/unspecified telehealth parity (
Fig. 1
Panel A
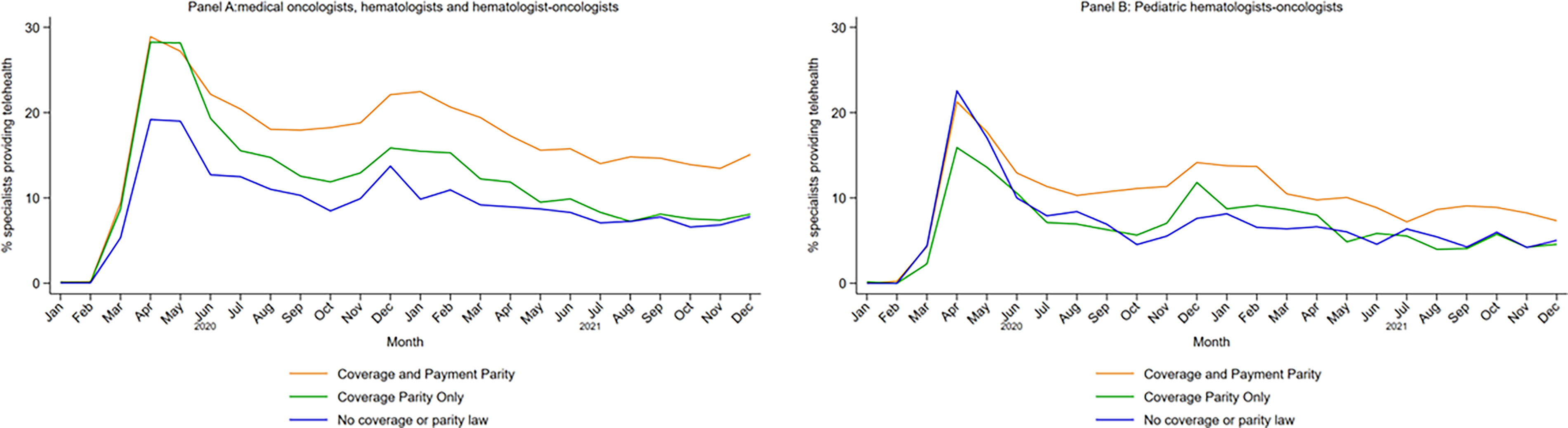
Proportion of Specialists Providing Telehealth by adult and pediatric specialty. This figure has two panels.
For adult specialists in coverage/parity states, telehealth visits spiked to 2.3/month in April 2020 and hovered at or above 2.0/month through December 2021, while coverage-only and no-parity states stayed below 2.0/month after August 2021 ( Fig. 2 , Panel A; Supplementary Table S2A). After August 2020, pediatric specialists in coverage/payment parity states maintained higher telehealth visit rates than in no-parity states, while coverage-only rates nearly matched or exceeded parity rates by late 2021.
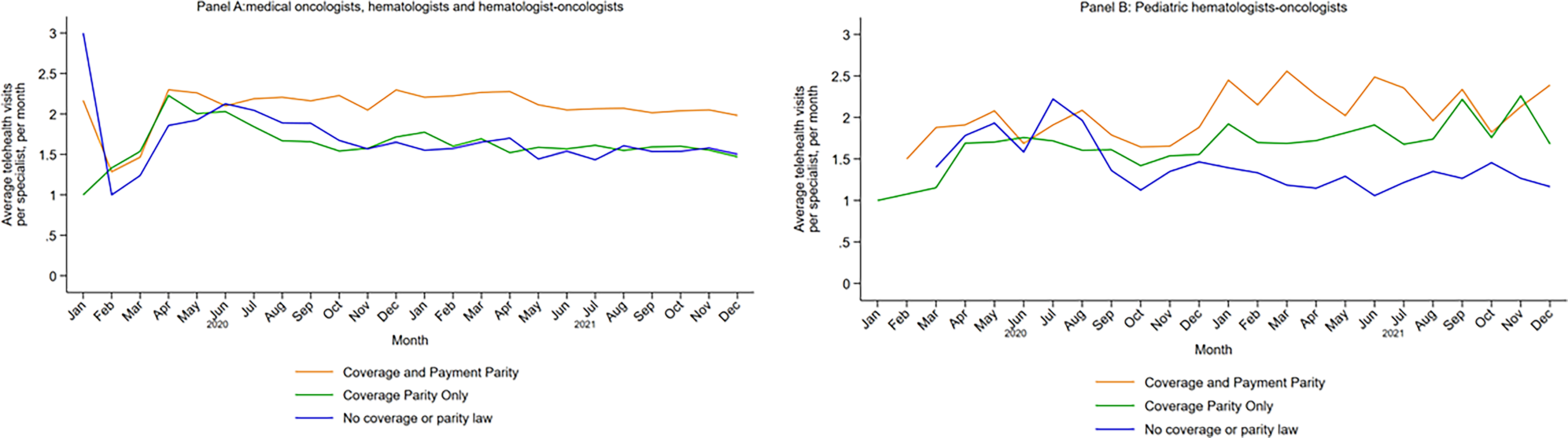
Average Telehealth Visit Per Specialist Per Month. This figure has two panels.
Discussion
In this Medicaid database of hematologic malignancies, adult and pediatric specialists in coverage/payment parity states had higher telehealth use compared to coverage-only and no-parity states. Our data confirm what has been previously reported: coverage and payment parity laws were associated with higher, sustained telehealth provision by oncology specialists treating Medicaid patients with hematologic malignancies, echoing evidence that payment parity facilitates sustained telehealth utilization.16,17 Our findings underscore the importance of supportive policies to facilitate access, as telehealth enhances access to specialty care, promotes care continuity, reduces exposure and travel burdens, and improves patient satisfaction. 18 This is particularly important because hematologic malignancies carry high risks for mortality if not diagnosed and treated promptly an adult and pediatric specialists, sometimes at a large tertiary center. Lack of access to specialty care results in early mortality, and telehealth has the role to bridge the gap, particularly for patients of lower socioeconomic status, as reported in our study. Ongoing advocacy and policy changes are warranted to enhance telehealth utility in the management of patients with hematologic malignancies. Telehealth is vital to support hematologic care by developing shared care models between specialty center, and community oncology practice. Telehealth can be even more important as the need for cancer care continues to grow among patients with hematologic malignancies.
In 2022, about 150,000 people in the United States were newly diagnosed with hematologic malignancies, with 10–15% insured by Medicaid. 19 Alongside rising incidence, survival rates have improved, increasing demand for oncology care. 20 Yet projected workforce shortages and uneven clinician distribution may create a gap between growing care needs and available oncology services; further widening existing inequities in the burden of cancer in patients from disadvantaged backgrounds.21–27 Telehealth flexibilities can help mitigate these gaps by supporting consistent access to cancer care, particularly for Medicaid patients in states with limited resources, where distance to oncology centers remains a major barrier.5,28–30
Although the data analyzed reflect the 2020–2021 period, this study captures a critical policy inflection point whose implications extend well beyond the acute phase of the COVID-19 pandemic. The pandemic served as a large-scale natural experiment, rapidly revealing how telehealth utilization responds to changes in coverage and payment policy. Importantly, we find that telehealth use did not simply surge and disappear uniformly; rather, states with coverage and payment parity demonstrated more sustained use among oncology specialists treating Medicaid patients, even as overall utilization declined from its early-pandemic peak. This pattern suggests that post-pandemic retrenchment in telehealth reflects a normalization toward selective, clinically appropriate use rather than a wholesale reversal and that policy design plays a central role in determining which services persist. These findings are highly relevant to current policy debates, as federal telehealth flexibilities sunset and states reconsider parity requirements.
For Medicaid patients with hematologic malignancies who continue to face substantial travel burdens, workforce shortages, and geographic maldistribution of specialty care, the access challenges that prompted telehealth expansion remain largely unchanged. Our results therefore offer actionable insight into which state-level regulatory frameworks are most likely to support equitable, sustainable telehealth integration in oncology care moving forward.
Limitations
Our study is not without limitations. Because it relies on cross-sectional data, causal inference is not possible, and generalizability is constrained by the exclusion of states with low-quality TAF data. Nonetheless, the patterns observed highlight the importance of sustained policy attention. Given the uncertainties surrounding federal telehealth flexibilities, maintaining state-level regulatory mandates for coverage and payment parity will be essential to ensuring equitable access to care for remote and underserved populations.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by Blood Cancer United, formerly The Leukemia & Lymphoma Society.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.