
Abstract
Background:
Rocket Health Africa (formerly The Medical Concierge Group) pioneered telehealth in Uganda by integrating technology with personalized care, providing consultations, diagnostics, pharmacy services, laboratory services, clinics, and vaccination services on a single platform.
Methods:
This study examined the diagnostic and demographic profiles captured through Rocket Health’s digital health platform from 2019 to 2023, across the prepandemic, pandemic, and postpandemic periods, using descriptive statistics.
Results:
A total of 2,677 users were recorded on the telehealth platform during the prepandemic period, 47,072 during the pandemic, and 99,904 during the postpandemic period. Male users accounted for the largest proportion of platform users across all three periods. Married individuals constituted the largest proportion by marital status categories, while users aged 25–34 accounted for the highest proportion within the age group distribution. A range of diagnostic categories was documented across the study period. Diseases of the respiratory system, such as acute upper respiratory infection, were the most frequently recorded diagnostic category, followed by symptoms, signs, and abnormal clinical and laboratory findings not elsewhere classified, including fever, headache, and cough. Certain infectious and parasitic diseases, such as coronavirus infection, candidiasis of the vulva and vagina, and Plasmodium falciparum malaria, constituted the third most frequently recorded diagnostic category.
Conclusions:
Telehealth utilization in Uganda was documented across diverse demographic groups and diagnostic categories over three distinct periods. These findings inform future telehealth policy and planning in Uganda and sub-Saharan Africa.
Introduction
Access to healthcare remains a significant challenge in low- and middle-income countries (LMICs), with over two-thirds of the population living in underserved or hard-to-reach areas. 1 Telehealth services have expanded globally over the last decade, with many countries incorporating them into their healthcare systems 2 to improve healthcare accessibility by addressing barriers such as high costs, mobility issues, stigma, staffing shortages, resource constraints, long waiting times, and travel time to health facilities. Telehealth grew out of telemedicine, and these two terms are often, but not always, used interchangeably. Telemedicine is the remote delivery of healthcare services that allow medical information to be exchanged for disease diagnosis, treatment, and prevention, to improve community health. 3 Telehealth, while similar to telemedicine, includes nonclinical healthcare services beyond the doctor-patient relationship. These include patient education, remote monitoring, public health initiatives, and administrative functions. 4
The COVID-19 pandemic accelerated the adoption of telehealth services in both developed and LMICs. 5 With lockdowns, movement restrictions, social distancing, and an overwhelmed healthcare system during the COVID-19 pandemic, the demand for telehealth services surged worldwide, 5 with 13.8% of countries showing advanced telehealth adoption and 22.6% at the developing stage. 6 Before the pandemic, telehealth adoption rates in developed countries were realizing telehealth’s potential. 6 Despite the numerous benefits of telehealth, such as increased accessibility, improved service utilization, and reduced healthcare costs, among others, its uptake in LMICs is still low due to infrastructural limitations, data security, and privacy concerns, which need to be addressed to ensure sustainable and widespread adoption of telehealth in these countries.2,7
In East Africa, Kenya, Uganda, Tanzania, and Rwanda are embracing telehealth services due to the rapid expansion of mobile technology and the convenience and accessibility it offers. 8 For instance, M-Pesa mobile money in Kenya has enabled the development of M-Tiba, which provides telehealth services to improve healthcare accessibility and affordability. 9 The Rwandan government collaborates with Babyl to provide smartphone-based remote consultation, lab test codes, and prescription services. 10 PANDA, a telehealth system in Tanzania, which uses mobile technology to provide services on maternal and neonatal health. 11
In Uganda, Rocket Health, a digital health company, pioneered virtual care delivery over the past decade. Rocket Health developed a comprehensive telehealth platform that offers teleconsultations, diagnostic sample pickup, pharmacy delivery, and chronic disease management. 12 It has become a valuable resource not only for individuals paying out of pocket but also for holders of private health insurance who are increasingly turning to the service for routine and specialist care. Its success reflects both the region’s growing demand for convenient and dignified care, as well as the potential of technology to transform healthcare delivery models. 13 It launched operations in 2013 to deliver telehealth and information and communications technolocy (ICT) solutions to the general public in Uganda, but in 2019, it began providing physical clinical services to its users.
This study, therefore, aimed to explore the diagnostic and demographic profiles captured on Rocket Health’s platform across prepandemic, pandemic, and postpandemic. By examining the clinical conditions most commonly presented and managed via telehealth, the study seeks to provide insights into how digital care is being utilized in Uganda.
Methods
DATASET AND SAMPLE
We analyzed a cohort of telehealth clients who received remote or virtual teleconsultation services, and last-mile doorstep laboratory and pharmacy services offered by Rocket Health in Uganda. The dataset comprised records of individual patients, referred to as users, defined as unique beneficiaries who accessed at least one service during the study period. Each user was assigned a unique identifier at the point of first encounter, which remained consistent across all subsequent interactions throughout their lifetime of service use. Users could present multiple encounters during the reporting period for different service requests, and all repeat encounters were linked back to the originating unique identifiers assigned during the first encounter. All clients who accessed the digital health service through various contact platforms available from 2019, before COVID-19 was declared in the country, to 2023, after all COVID-19 restrictions were lifted, were included in the analysis.
HOW ROCKET HEALTH SERVICE IS ACCESSED
The service has been conveniently and inclusively built to allow access through any mobile communication platform and channel, including voice calls, short message serived (SMS), WhatsApp, unstructured supplementary service data (USSD), and e-commerce sites. The multichannel optionality allows for inclusion and access for all socioeconomic categories, especially in the current context of widespread phone ownership.
HOW USERS PAY FOR THE SERVICE
The service is generally financed through the following mechanisms:
Cash-based/mobile money payments for services for one-time payments; Private health insurance premiums, as Rocket Health has existing contracts with up to 16 top insurance players in East Africa; Grant subsidies through development partners and philanthropy that allow low earners to access the services at massively subsidized or free options; and A mobile money wallet that allows users to save with Rocket Health and draw from their wallet whenever they or their family members use the service.
NUANCES OF ROUTINE DATA COLLECTION
For most contact platforms, during the first encounter, client demographic characteristics, including date of birth, sex, marital status, and area of residence, are recorded into the client database. Additionally, the service provided, payment method, laboratory tests, and diagnosis are documented. A trained medical team assigns each diagnosis following the International Classification of Diseases (ICD), Tenth Revision (ICD-10). However, the comprehensive collection of demographic data is often constrained by the specific access modality. On purely virtual platforms such as voice calls, data capture relies heavily on user self-reporting and completion rates. This leads to systematic missingness within the demographic records for some users. In the analysis, we calculated each client’s age at the time of encounter from the recorded date of birth.
STATISTICAL ANALYSIS
The demographic and diagnostic profiles of patients were analyzed using descriptive statistics. Demographic characteristics, including sex, marital status, and age group, were summarized using frequencies and proportions and presented in tables across prepandemic, pandemic, and postpandemic. Diagnoses were grouped according to ICD-10 classifications, and the frequency and percentage of each diagnosis were also calculated. These results were presented in tables to show the overall distribution of diagnoses across the entire study period, from 2019, before the COVID-19 pandemic was declared in the country, to 2023, after restrictions were lifted. All analyses in this study were limited to descriptive statistics, and no inferential analysis or hypothesis testing were performed. All analyses were conducted using Stata 15 and R statistical software version 4.3.2.
ETHICS STATEMENT
The management of Rocket Health Africa approved the study at the time it was conducted, and no further approvals were required since the study focused on summarizing routinely collected data. However, as per routine practice, Informed consent for diagnostic assessment, tele-consultations, and last-mile pharmacy services was obtained from all the patients whose data were analyzed for this report. All patients and participants provided written consent, administered by Rocket Health field agent or clinic personnel before any procedure were conducted. This was done at every encounter, regardless of previous consent status.
The data were securely stored and handled to protect patient privacy, in accordance with the Uganda Data Privacy and Protection Act, for which Rocket Health Africa and the Africa Centre for Applied Digital Health are officially certified data handlers and custodians.
Results
Table 1 presents the demographic characteristics of users on the telehealth platform across the prepandemic, pandemic, and postpandemic periods. During the prepandemic period, a total of 2,677 users were recorded on the platform. Male users accounted for the largest proportion at 55.5%, followed by females at 44.5%. Among marital status categories, married individuals represented the highest proportion at 49.3%, followed by single individuals at 49.1%, and divorced/widowed individuals at 1.6%. Users aged 25–34 accounted for the highest proportion within the age group distribution across all three periods. During the pandemic, a total of 47,072 users were recorded on the platform. Male users continued to account for the largest proportion at 55.4%, with female users representing 44.6% of platform users. Among marital status categories, married individuals continued to represent the largest proportion at 56.1%, followed by single individuals at 43.1%. During the postpandemic, a total of 99,904 users were recorded on the platform. Male users accounted for 60.7% of platform users, while female users represented 39.3%. Among marital status categories, single individuals accounted for the largest proportion at 54.2%, followed by married individuals at 44.4%.
Client Demographic Characteristics Across the Prepandemic, Pandemic, and Postpandemic Periods
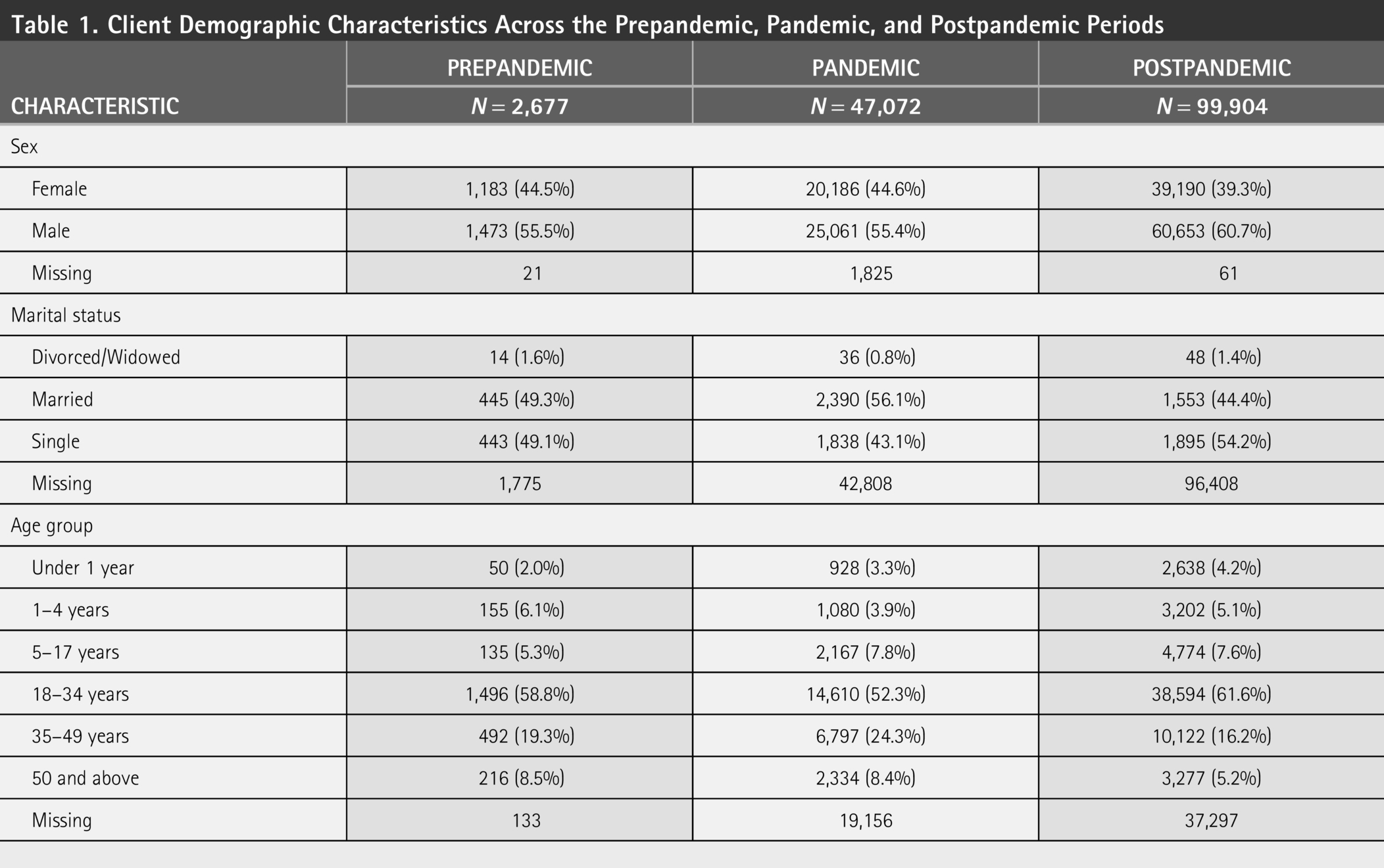
As shown in Table 1 , missing demographic data across the three time periods indicates that some users chose not to share all their personal details. However, this did not prevent them from accessing or benefiting from the telehealth services. The platform was designed to stay accessible and responsive to clinical needs, even without complete user disclosure, showing a flexible approach that prioritized timely care while respecting user privacy and convenience. Detailed frequencies and percentages of missingness for the demographic variables stratified by period are presented in Supplementary Table S1.
Table 2 presents the distribution of diagnostic categories recorded on the telehealth platform across the study period. All diagnoses were determined through symptom-based assessment and laboratory testing. Respiratory system diseases represented the most frequently recorded diagnostic category, accounting for 31.8% of all documented diagnoses. Symptoms, signs, and abnormal clinical and laboratory findings not elsewhere classified represented the second most frequently recorded category at 21.1%, followed by certain infectious and parasitic diseases at 12.9%. These three diagnostic categories accounted for 65.8% of all recorded diagnoses. The least frequently recorded diagnostic categories were neoplasms (0.1%), other external causes of morbidity and mortality (0.0%), and conditions originating in the perinatal period (0.0%).
Diagnosis Categories
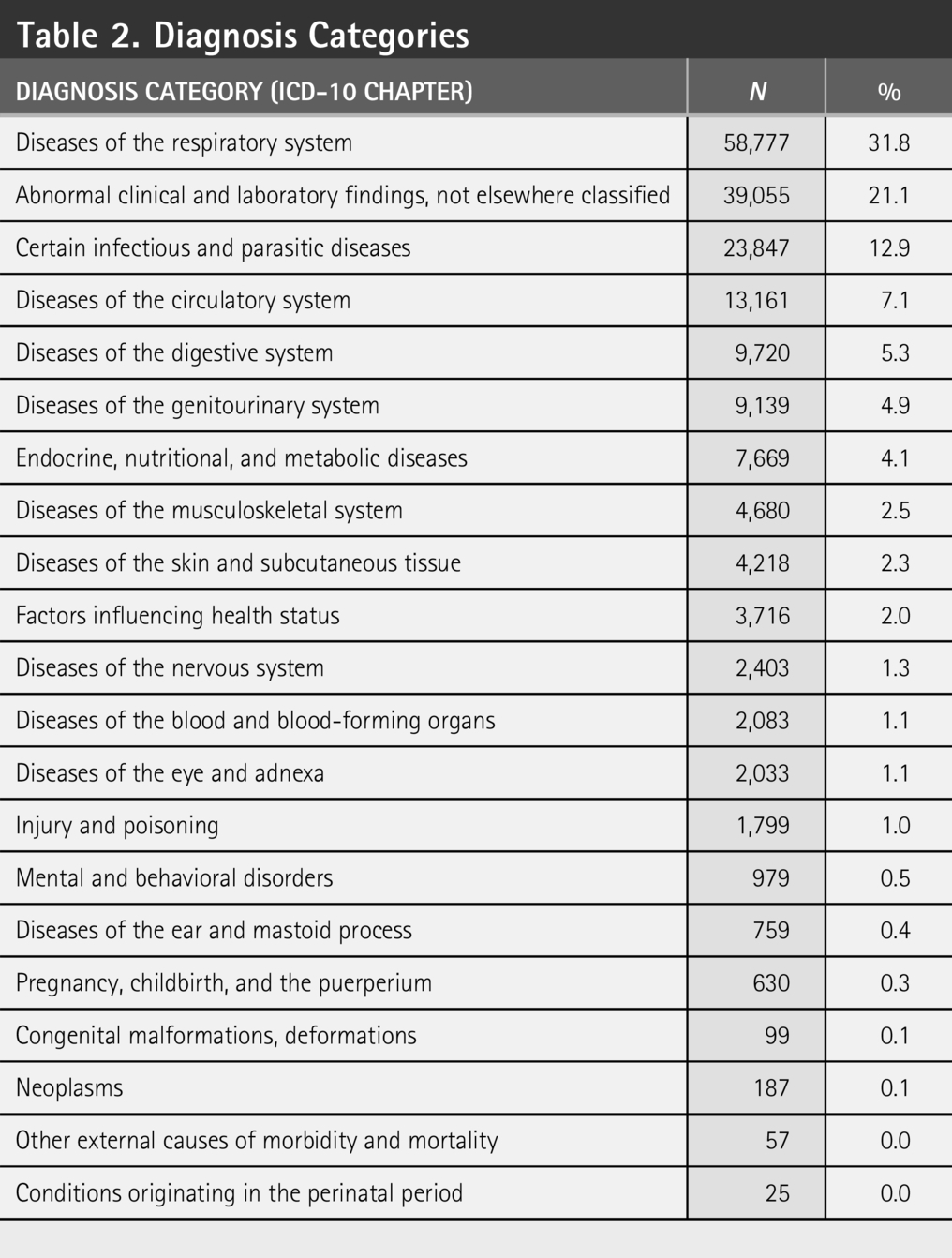
Fig. 1 presents the distribution of respiratory diseases recorded on the telehealth platform. Within this diagnostic category, acute upper respiratory infection accounted for the highest proportion of documented cases at 54.1%, followed by common cold at 26.6% and acute pharyngitis at 3.2%. Fig. 2 presents the distribution of symptoms, signs, and abnormal clinical and laboratory findings, not elsewhere classified. Within this category, cough represented the highest recorded proportion at 21.8%, followed by fever at 16.3%, and headache at 12.8%. Fig. 3 presents the distribution of certain infectious and parasitic diseases recorded on the platform. Within this category, coronavirus infection, unspecified, accounted for the highest proportion of documented diagnoses at 32.4%, followed by candidiasis of the vulva and vagina at 11.9%, and Plasmodium falciparum malaria at 9.4%.
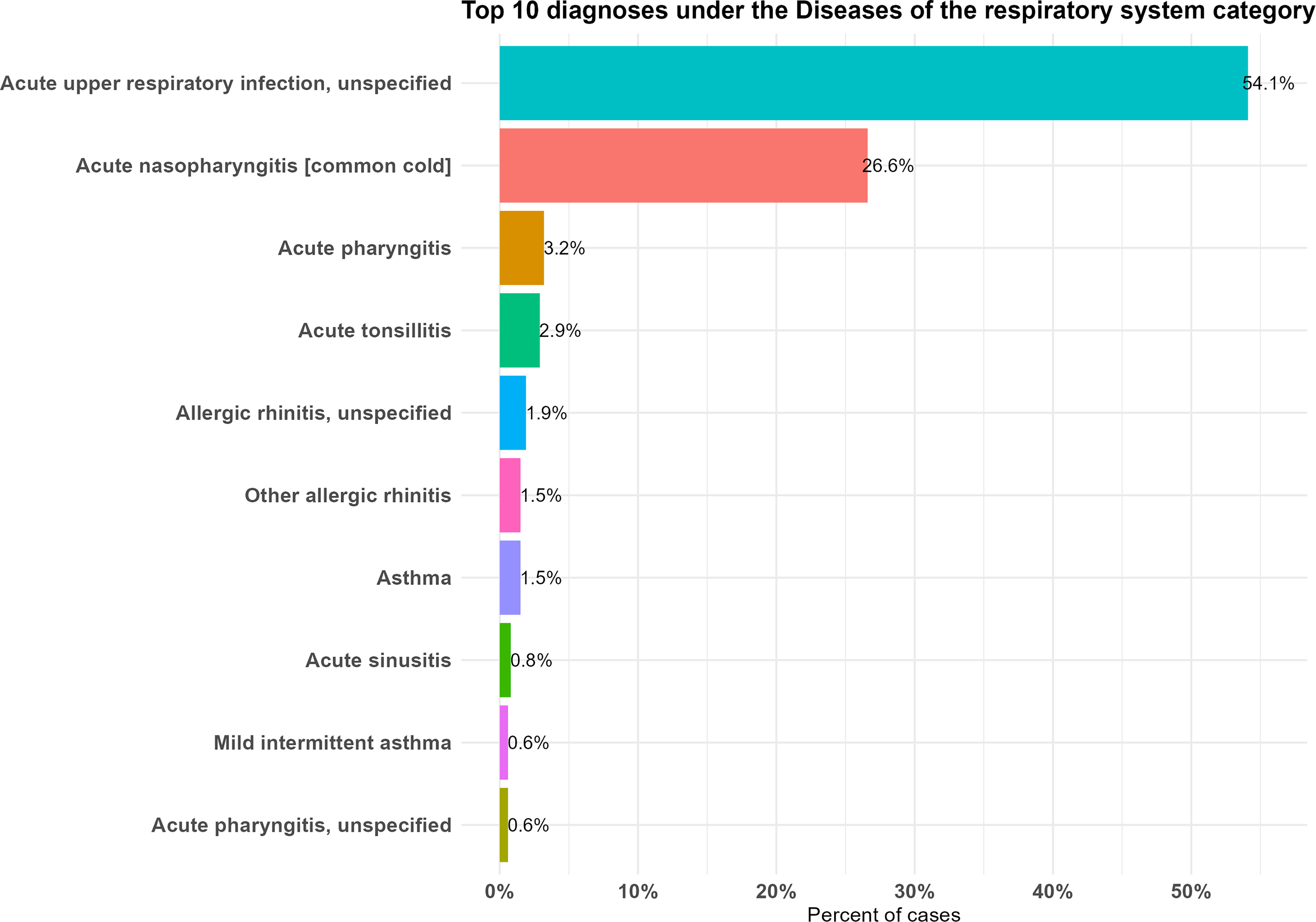
Diseases of the respiratory system.
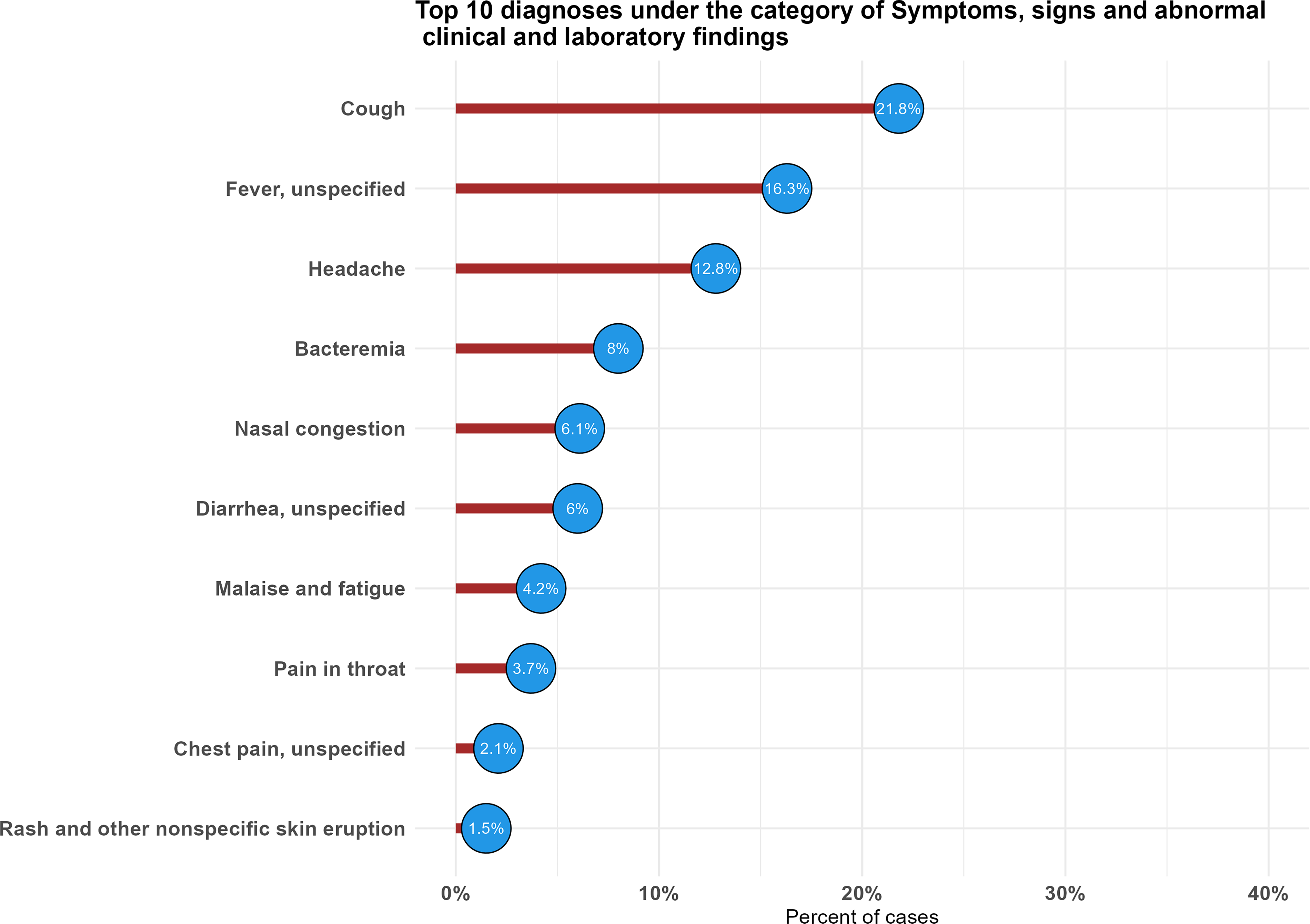
Signs, symptoms, and abnormal clinical and laboratory findings, not elsewhere classified.
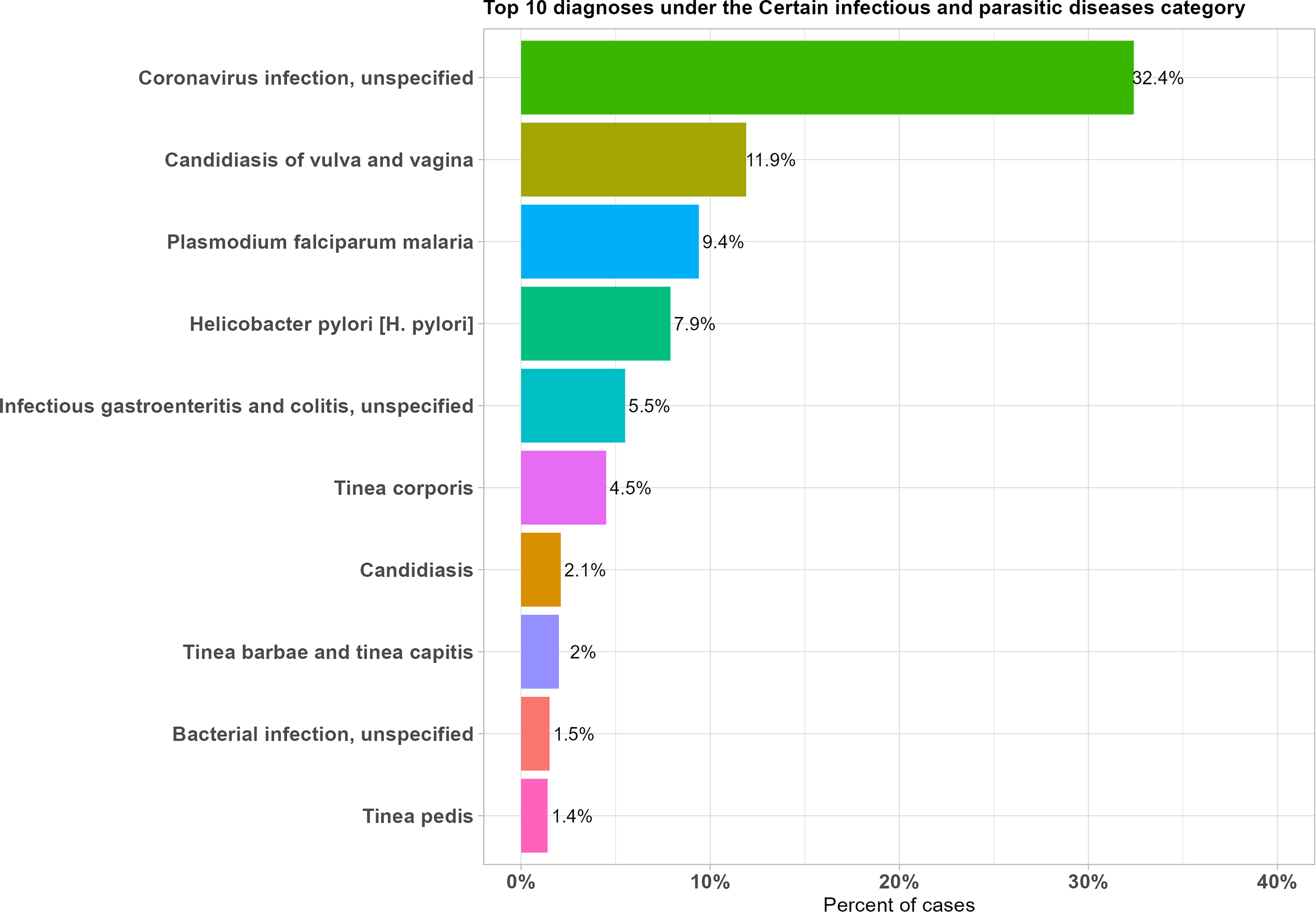
Certain infectious and parasitic diseases.
Discussion
This study described the diagnostic and demographic profile of Rocket Health, a digital health company that offers telehealth services in Uganda. The study documented variations in the number of users recorded on the telehealth platform across the prepandemic, pandemic, and postpandemic periods. Telehealth utilization recorded during the pandemic period aligns with descriptive patterns reported in other settings, where telehealth services were accessed amid disruptions to in-person care delivery.14,15 Across the study period, outpatient conditions, including respiratory illnesses and infectious and parasitic diseases, were among the top diagnostic categories recorded on the platform, reflecting the range of conditions for which telehealth services were accessed in Uganda.
In this study, male users represented a higher proportion of telehealth encounters across all three study periods. This pattern differs from utilization profiles reported in previous studies, where female users accounted for a greater proportion of telehealth encounters.16,17 Among the marital status categories, married individuals represented the largest proportion of platform users across the study period. Within the age group distribution recorded, users aged 25–34 years accounted for the highest proportion of encounters. These demographic patterns are consistent with utilization profiles reported in previous studies, where married individuals and younger adults were similarly represented among the telehealth users. 17 Although diagnoses were not disaggregated by pandemic phases, the overall diagnostic profile documented across the study period indicated that respiratory infections represented the largest proportion of recorded diagnoses, with acute upper respiratory infections accounting for more than half of the documented cases. These patterns are consistent with diagnostic profiles reported by Lahoz et al. 18 and Chandler et al. 19 in telehealth utilization.
The second most frequently documented diagnostic category was symptoms, signs, and abnormal clinical and laboratory findings, with cough, fever, and headache representing the highest proportions within this category. Certain infectious and parasitic diseases constituted the third most commonly recorded diagnostic category, with coronavirus infection, candidiasis of the vulva and vagina, and P. falciparum malaria accounting for the highest proportions of documented diagnoses within this group. The diagnostic profiles documented in this study are consistent with findings reported in previous literature describing telehealth utilization for primary care and chronic disease conditions. 18 Across the study period, outpatient conditions, including acute illnesses, chronic conditions, infectious and parasitic diseases, and mental health concerns, were among the diagnostic categories recorded on the platform, reflecting the range of conditions for which telehealth services were accessed.
Rocket Health’s experience has proven that telehealth adoption is not dependent on complex or costly digital infrastructures like mobile applications; instead, it relies on low-tech and easily accessible platforms like SMS, USSD, and voice calls, which have demonstrated sufficient capabilities for most clinical interactions, especially in areas with high mobile penetration. 13 These simple tools help mitigate the digital divide, enabling users to access care through familiar technologies. 20 As observed in our demographic characteristics, there is a substantial proportion of missing information and the volume of missingness increased notably during the pandemic and postpandemic periods. The high rate of missing data suggests systematic omissions rather than random, likely driven by users skipping optional fields to expedite urgent care, as well as the use of simplified access modalities such as voice call, which do not prompt patients to fill out their profiles.
A key strength of this study is its ability to gather real-world usage data from a telehealth company across the prepandemic, pandemic, and postpandemic periods. This broad timeframe allowed for a comprehensive characterization of telehealth service utilization across these distinct phases. The use of standardized ICD-10 classification for documenting diagnoses enhanced the consistency and comparability of the diagnostic data recorded across the study period.
Conclusion
The study had several limitations. The diagnostic data were aggregated across the full study period and were not disaggregated by pandemic phase, thus limiting the ability to identify period-specific patterns. Future studies should disaggregate diagnostic data by pandemic phase to enable temporal characterization of telehealth utilization patterns. All analyses in this study were limited to descriptive statistics, specifically frequencies and proportions, with no inferential analysis or hypothesis testing performed. As a result, observed differences across time periods and demographic groups reflect distributional patterns in the data and should not be interpreted as tested comparisons or causal associations. The high rate of missing in demographic data restricts the representativeness of our user profiles and prevents these findings from being generalized to all telehealth users in Uganda. The data were collected from a single telehealth provider, which may not fully represent patient populations in other regions of Uganda. The dataset did not include variables such as socioeconomic status, education level, or digital literacy, limiting the ability to describe the distribution of telehealth utilization across these factors and equity in service access.
This study described the demographic and diagnostic characteristics of telehealth users across the prepandemic, pandemic, and postpandemic periods in Uganda. While utilization of the platform increased during the pandemic, the continued use of platform in the postpandemic period characterizes telehealth as an accessible service modality within the Uganda healthcare context. These findings provide a descriptive foundation for understanding the profile of telehealth users and the conditions for which services were accessed and may inform future investment, policy development, and planning decisions aimed at expanding equitable telehealth access in Uganda and sub-Saharan Africa.
Authors’ Contributions
F.O. drafted the original article. D.M., A.M., and L.K. performed the analysis and interpreted the results. J.M.B., D.K., and A.K. guided the conceptualization of the study and the design of the methodology and revised the original article. All authors reviewed and approved the final version of the article.
Ethical Considerations and Consent to Participate
The management of Rocket Health Africa approved the study at the time it was conducted, and no further approvals were required since the study focused on summarizing routinely collected data. However, as per routine practice, informed consent for diagnostic assessment, tele-consultations, and last-mile pharmacy services was obtained from all the patients whose data were analyzed for this report.
All patients and participants provided written consent, administered by Rocket Health field agent or clinic personnel before any procedure were conducted. This was done at every encounter, regardless of previous consent status.
Data Availability
The raw, deidentified data used for the study will be made available on request.
Supplemental Material
sj-docx-1-teh-10.1177_15305627261464772 — Supplemental material for Characterization of Clinical Diagnoses at a Community Telehealth Platform in Uganda
Supplemental material, sj-docx-1-teh-10.1177_15305627261464772 for Characterization of Clinical Diagnoses at a Community Telehealth Platform in Uganda by Flavian Otieno, Daniel Mwanga, Ashiraf Mawanda, Louis Kamulegeya, John Mark Bwanika, Damazo Kadengye, and Agnes Kiragga
Footnotes
Acknowledgments
The authors thank the staff and management of Rocket Health Africa, who continue to tirelessly serve thousands of telehealth users every day, for providing approval for this assessment and documentation.
Disclosure Statement
The authors declare no competing interests.
Funding Information
Rocket Health Africa was funded by multiple funders. The article preparation for this study was funded by the African Population and Health Research Center (APHRC) through the Lacuna Project, under Grant Number 19497.59, awarded to Principal Investigator Dr. Agnes Kiragga. The funders did not play any role in study design, data collection, decision to publish, or preparation of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.