
Abstract
Ileocolic pseudoaneurysmal disease is a rare splanchnic aneurysm that affects 3 out of 100 000 patients, and only 7 cases have been described in the past 40 years in patients without preexisting connective tissue disorders. Abdominal pain is the most common presenting symptom and nearly 30% of patients present with hemorrhage. Ileocolic pseudoaneurysms are diagnosed by contrasted computed tomography scans and verified by arteriography. We present a case report and review of the literature in which a patient was initially managed by coil embolization, followed by laparotomy and suture ligation due to pseudoaneurysm rupture.
Introduction
Aneurysmal disease of the splanchnic circulation is uncommon, affecting less than 3 out of 100 000 hospitalized patients. 1 The most commonly affected vessel is the splenic (60%), followed by the hepatic (20%), superior mesenteric artery (SMA; 5.5%), and other visceral arteries (<15%). Branches of SMA, including the jejunal, ileal, and colic branches, have aneurysmal disease less than 3% of the time.2-6 Anomalous anatomy appears to be associated with a somewhat higher risk of developing aneurysmal disease, such as an ileocolic artery that branches directly from the aorta. 7
Unlike other splanchnic pseudoaneurysms, those affecting branches of the SMA are more likely to be symptomatic.2-5 Abdominal pain, nausea, and vomiting are precursors to more serious symptoms associated with frank rupture, such as hypotension, tachycardia, and hemorrhagic shock. Of the branches of the SMA, the ileocolic, right colic (when present), and middle colic arteries are most likely to rupture.3-5,8 Mortality can exceed 20% regardless of whether free rupture occurs into the intestinal lumen presenting with blood per rectum or a contained rupture leading to a pulsatile mass occurs into the mesentery. 6
Case Report
BC is a 25-year-old man with severe Crohn’s disease cared for at our institution over the previous 5 years. His symptoms started at the age of 21 years leading to perianal fistulas requiring Seton placement. A high-grade small bowel obstruction required laparotomy and diverting loop ileostomy in 2008; an extended resection with lysis of adhesions was not performed as he became hemodynamically unstable intraoperatively. The following day his fascia was closed and he was discharged home 2 weeks later. Four months after his initial operation, the patient underwent an exploratory laparotomy with loop ileostomy takedown, and ileocecectomy after a bladder fistula occurred.
One month later, the patient presented with nausea, vomiting, and severe abdominal distention and pain. Oral and intravenous contrast computed tomography (CT) scan revealed a lobulated, hyperdense structure in the mid-right abdomen (Figure 1A). A neck was emanating from this structure and appeared to be confluent with the ileocolic artery. Ultrasound demonstrated arterial flow within the hyperdense structure (Figure 1B) but arteriogram revealed active extravasation (Figure 2A). Arteriogram with coil embolization of a 3 cm pseudoaneurysm was completed (Figure 2B).
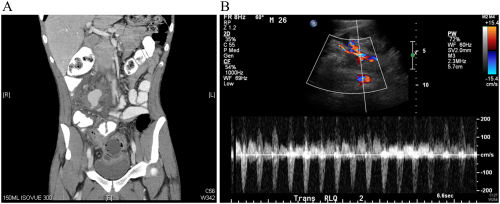
(A) Coronal image portraying the neck of the pseudoaneurysm (arrow) and its proximity to the superior mesenteric artery. The terminal ileum (arrowhead) can also be seen in this image. (B) Ultrasound demonstrating flow within the large 3 cm pseudoaneurysm at the ileocolic artery and its flow into the superior mesenteric artery (arrow).
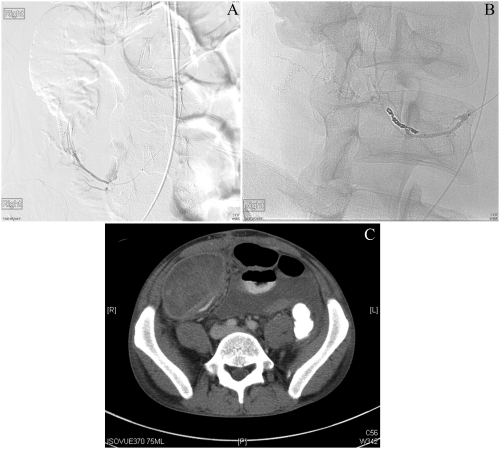
(A) Arteriography demonstrating extravasation from the ileocolic artery into the peritoneum. What had been demonstrated as a pseudoaneurysm on ultrasound was revealed to be a ruptured pseudoaneurysm by arteriography. (B) Coil embolization of the ileocolic artery branch with subsequent resolution of extravasation. (C) (a) Axial image demonstrating increase in size of the ruptured pseudoaneurysm cavity with continuing active extravasation (arrowhead). (b) Coronal image better shows flow from the superior mesenteric artery into the branch of the ileocolic artery (arrowhead).
The patient developed severe abdominal pain 2 days after the coil embolization. CT scan indicated active extravasation from the pseudoaneurysm consistent with a contained rupture (Figure 2C). The patient was taken for an exploratory laparotomy and ligation of the pseudoaneurysm. Due to concern over perfusion to the original anastomosis, the ileocolic anastomosis and end ileostomy were resected and a new end ileostomy was created. He has done well since his surgery.
Methods
English language articles published in PubMed since 1960 on ileocolic pseudoaneurysms were identified through a literature search. Our search queries included “ileocolic pseudoaneurysm” (7 results) and “ileocolic aneurysm” (22 results). We additionally searched for the incidence of aneurysmal disease in conjunction with Crohn’s disease using the queries “Crohn disease pseudoaneurysm” (3 results) and “Crohn disease aneurysm” (15 results). A total of 5 articles were identified after eliminating duplicates, non–English language articles, ileocolic aneurysms from anomalous anatomy, and articles not pertinent to the presentation, diagnosis, or management of ileocolic pseudoaneurysms (Table 1).9-13 Patients with connective tissue disorders were excluded because of their propensity toward pseudoaneurysm formation, limited response to conventional management, and atypically high morbidity and mortality.
Individual Reports of Patients With Ileocolic Pseudoaneurysm, Including Demographic Data, Presentation, Diagnosis, Treatment, and Complications. a
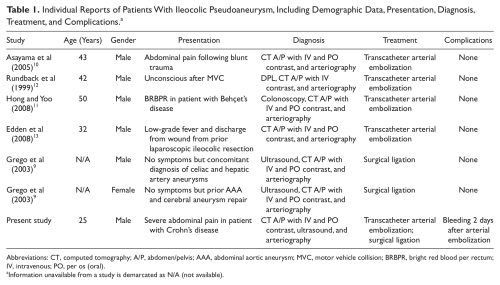
Abbreviations: CT, computed tomography; A/P, abdomen/pelvis; AAA, abdominal aortic aneurysm; MVC, motor vehicle collision; BRBPR, bright red blood per rectum; IV, intravenous; PO, per os (oral).
Information unavailable from a study is demarcated as N/A (not available).
Results
These 5 reports discuss ileocolic pseudoaneurysm formation and various aspects of its presentation, diagnosis, and management. Four are case reports and discuss ileocolic pseudoaneurysm formation following trauma, Behçet’s disease, and Crohn’s disease.10 -13 The remaining study is a presentation of 16 patients who underwent splanchnic artery aneurysm repair at a single center over a 14-year period. 9 Two of these patients had ileocolic pseudoaneurysms. Combining these reports, there are a total of 6 cases in the modern literature that specifically discuss ileocolic pseudoaneurysms in patients without connective tissue disorders.
The majority of patients with ileocolic aneurysmal disease were males (6/7), between 25 and 50 years of age (excluding Grego et al 9 ), and with solitary disease (5/7). All patients with solitary disease underwent a CT scan (80% success at diagnosis) and arteriogram (100% success at diagnosis) followed by ileocolic artery embolization (100% initial success). Only one patient had complications following coil embolization and required suture ligation of the ileocolic aneurysm intraoperatively. Two patients had free rupture of their aneurysm at the time of diagnosis (one intraperitoneal, the other into bowel lumen), one had a contained rupture within the mesentery, and the others without complications. All conscious patients with solitary lesions presented with abdominal pain.
One patient was found to have a ruptured pseudoaneurysm on CT following blunt abdominal trauma; he responded well to coil embolization of his ileocolic artery. 10 A second patient with a similar mechanism of injury underwent the same procedure, but was subsequently taken to the operating room for an exploratory laparotomy because of free air on CT scan. 12 A third patient presented with bright red blood per rectum secondary to Behçet’s disease, an inflammatory ulcerative disease that rarely affects the vascular system. Continued hemorrhage despite a negative CT scan led to an arteriogram that revealed a small aneurysm of the ileocolic artery with extravasation into the bowel. He was treated successfully by embolization. 11
A fourth patient underwent coil embolization of a 3 cm ileocolic pseudoaneurysm identified after continuing abdominal pain following an ileocolic resection for ileal stricture disease. 13 One study identified 2 patients with multiple splanchnic aneurysms. The first patient underwent sac incision of celiac, hepatic, and ileocolic aneurysms, aorto-hepatic graft with polytetrafluoroethylene, and partial aneurysmectomy and suture ligation of the hepatic and ileocolic arteries. The second patient had an abdominal aortic aneurysm and ileocolic artery aneurysm and subsequently underwent aortobifemoral bypass with ligation of the ileocolic aneurysm. Both patients were diagnosed by ultrasound, CT, and arteriography. Embolization was not attempted. 9 Interestingly, 2 of the 7 patients reviewed through the literature had Crohn’s disease requiring operative intervention.
Discussion
The diagnosis of visceral pseudoaneurysms is based on clinical assessment in conjunction with diagnostic imaging. Mesenteric angiography is the gold standard test, but the initial diagnosis is often made by CT with intravenous contrast.14,15 Arterial cuts and delayed cuts are valuable as the pseudoaneurysm sac may be conclusively identified by filling during the arterial phase and emptying thereafter. CT angiography has a sensitivity and specificity of 94.7% and 90%, respectively, in detecting visceral pseudoaneurysms. 16
Selected patients may be amenable to coil embolization. 15 Branches that supply bowel that have sufficient collateral are suitable targets if an appropriately sized pseudoaneurysm neck exists. Selective embolization of branches of the ileocolic artery has a low risk for causing ischemia of the bowel due to excellent anastomoses via the marginal artery, right colic artery, and branches of the ileocolic artery.17 -20 The success rate of visceral pseudoaneurysm embolization has been reported as 81% to 96%. 16 Bleeding can occur following coil embolization particularly in patients who presented with ruptured ileocolic pseudoaneurysms.3 -6 Patients who develop further bleeding following embolization may be candidates for surgical ligation.
Unstable patients with free rupture of their pseudoaneurysm into the intestinal lumen or the peritoneum should be resuscitated aggressively and managed operatively. Simple suture ligation of the ileocolic pseudoaneurysm at its neck is sufficient management. Careful evaluation of preoperative imaging should be made to exclude any other aneurysms.
Footnotes
Authors’ Note
This study was presented at the 40th Annual Symposium of the Society for Clinical Vascular Surgery, Orlando, Florida, March 17-20, 2011.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.