
Abstract
The International Classification of Diseases–11 th Revision (ICD-11) includes the diagnosis of complex posttraumatic stress disorder (CPTSD). Clinical practice guidelines support the use of phased care for individuals with CPTSD. This case study illustrates the use of synchronous telehealth to deliver phased treatment to a rural woman veteran with CPTSD. Mrs. A experienced sexual, physical, and emotional abuse throughout her life, perpetrated by family members, intimate partners, and military authority figures. She sought treatment for posttraumatic nightmares and body image issues; she also had pain related to fibromyalgia and chronic migraine headaches. Mrs. A participated in 19 sessions of Skills Training in Affective and Interpersonal Regulation (STAIR) Narrative therapy via synchronous telehealth. Trauma and eating disorder symptoms were assessed before and after treatment and the patient demonstrated clinically significant improvement on measures of these disorders. Patient-provider working alliance and quality of life were assessed post-treatment. Synchronous telehealth use drastically increased with the onset of COVID-19; however, little information on treating CPTSD via synchronous video teleconferencing is available. This case study illustrates an evidence-based, phased therapy for CPTSD while highlighting the feasibility and value of in-home delivery of psychotherapy for CPTSD via synchronous telehealth.
Keywords
1 Theoretical and Research Basis for Treatment
The diagnosis of Complex Posttraumatic Stress Disorder (CPTSD) includes symptoms reflective of chronic exposure to interpersonal trauma compared to symptom profiles of exposure to non-relational and single episode traumatic events (Herman, 1992). The International Classification of Diseases–11 th Edition (ICD-11) diagnosis for Posttraumatic Stress Disorder (PTSD) consists of three symptom clusters: (1) re-experiencing of the trauma, (2) avoidance of traumatic reminders, and (3) a persistent sense of current threat (World Health Organization; WHO, 2019). In ICD-11, the diagnosis of CPTSD adds three symptom clusters distinguishing it from PTSD (WHO, 2019). These symptom clusters are collectively referred to as disturbances in self-organization (DSO) with individual clusters labeled: affective dysregulation, negative self-concept, and disturbances in relationships (WHO, 2019). This recent diagnostic addition is preceded by a body of research examining factor structure, comorbidity and associated symptoms, mediators, and etiology (Karatzias & Levendosky, 2019). In 2015, the International Society for Traumatic Stress Studies (ISTSS) established a Guidelines Committee to update published treatment guidelines for children, adolescents, and adults with PTSD and/or CPTSD. In 2018, the Committee undertook a narrative review and published a position paper considering the definition of complex PTSD in order to support the identification of evidence based treatments (ISTSS Guideline Committee, 2018).
With a recognized diagnosis, there is now promise to add to the extant literature. In a meta-analysis of RCTs for CPTSD, the current evidence based psychotherapies (EBPs) for PTSD (Prolonged Exposure Therapy, Cognitive Processing Therapy) demonstrated inferior benefit for individuals who had experiences of adverse childhood events and childhood trauma, a risk factor for CPTSD (Karatzias et al., 2019). Additionally, EBPs for CPTSD had varied effect sizes for DSO symptoms with the strongest support (moderate-to-large-large or large effect sizes) for cognitive behavioral therapy and exposure alone on negative self-concept symptoms (Turgoose et al., 2018). The aim of this meta-analysis was to synthesize evidence of CPTSD treatments that may be effective for DSO symptoms of CPTSD by including trials where participants were also likely to have clinically significant levels of DSO symptoms (Turgoose et al., 2018). Another systematic review and component network meta-analysis examined interventions for PTSD in samples of individuals exposed to complex trauma and concluded that phased treatments that included skills and trauma focused strategies were most promising for some DSO symptoms (emotion dysregulation and interpersonal problems; Coventry et al., 2020). Phased treatment includes three sequential stages: safety and stabilization (phase one ), remembrance and mourning (phase two ), and reconnection and integration (phase three ; Herman, 2015). These few studies are the best available evidence, however, it is important to note that to date, there are limited data and no single treatment has emerged as a gold standard or front-line modality for CPTSD.
Skills Training in Affective and Interpersonal Regulation (STAIR) is a phase-one 12-session EBP for PTSD related to childhood abuse, and it targets coping skills for addressing the DSO symptoms of CPTSD (Cloitre et al., 2002). The addition of four to eight phase-two, narrative/exposure-based sessions are called “STAIR Narrative Therapy” (previously called STAIR-modified PE and STAIR Exposure); the phase-two sessions focus on trauma processing (Cloitre et al., 2002).
Telehealth has seen a rise in use over the past decade to increase access to care, with a surge in use during the recent COVID-19 pandemic. While many psychotherapies have research supporting their implementation via telehealth modalities, there is a paucity of research on treating CPTSD via synchronous telehealth (Turgoose et al., 2018). Limited telehealth research suggests that some EBPs (e.g., Prolonged Exposure, Cognitive Behavioral Therapy, Cognitive Processing Therapy, and Behavioral Activation) and concurrently delivered psychotherapies (e.g., for substance use and PTSD or depression and PTSD) is associated with improvements on a range of outcomes including PTSD symptom severity (Jaconis et al., 2017; Strachan et al., 2012; Turgoose et al., 2018). One recent feasibility and effectiveness pilot trial (N = 10) found that STAIR therapy delivered to rural women veterans who experienced military sexual trauma via clinic-to-clinic synchronous video teleconferencing demonstrated significant improvements on measures of social functioning, PTSD, depression, and emotion regulation (Weiss et al., 2018). STAIR Narrative Therapy delivered in person has been shown to improve PTSD symptoms, affect regulation, interpersonal skills, and reduce dropout rates (Cloitre et al., 2002, 2010). Because no research examines current practices for synchronous telehealth treatment of CPTSD using STAIR Narrative Therapy, descriptive literature is warranted to support quality of care while ongoing research develops in tandem with clinical practice.
2 Case Introduction
Mrs. A was a 51 year-old, White, cis-gendered, heterosexual, married, female Air Force veteran residing in a rural area of the Southwest. The therapist was a clinical psychologist located in a United States Department of Veterans Affairs (VA) Health Care System in the Pacific Northwest and working in a clinic which provided synchronous telemental health care to understaffed satellite clinics of the VA located in rural areas of the Western and Southwestern United States. Treatment for Mrs. A took place between May, 2019 and January, 2020. Of note, ICD-11, which provides diagnostic criteria for CPTSD, was released in May 2019. The name and identifying characteristics have been changed to protect the confidentiality of Mrs. A.
3 Presenting Complaints
Mrs. A presented to therapy with complaints of trauma-related nightmares two to three times per month, and more during times of increased stress. She demonstrated insight to the relationship between her symptoms of PTSD and problems with body image and aging: she described recent distress with aging and increased attention to her food consumption and exercise in order to avoid/reduce weight gain as a “control behavior” connected to her history of sexual trauma. She was previously diagnosed with major depressive disorder, generalized anxiety disorder, low back pain, sleep-related bruxism, fibromyalgia, chronic migraine headache, and sleep apnea. Mrs. A was prescribed buspirone (10 mg), fluoxetine (20 mg), and trazodone (50 mg); she was untreated for sleep apnea.
Mrs. A identified a relationship between her sexual trauma and eating disordered behavior occurring over the previous several months to a year, though she reported she had always attempted to keep a small size and maintain her weight and physique to be within standards she considered “attractive.” While she preferred to eat a healthy, nutritional diet and exercise regularly, she reported that this was also motivated by her body image. She described additional thoughts and behaviors indicating disordered eating and body image. She endorsed often feeling she was “disgusting,” that she would count and reduce calories to decrease weight that she had put on as her hormones changed while aging.
4 History
Mrs. A and two brothers were raised by her mother and father in the Midwest before moving to the Southwest when she was 10 years old. Mrs. A had a good relationship with her younger brother and father. Her mother was deceased, and she kept a distant relationship with her older brother and his wife. During the therapy intake, she reported that in childhood her mother had depression and a severe alcohol use disorder. Mrs. A reported her mother was verbally and emotionally abusive to her and her siblings. She described that her mother would protect her older brother when he would physically and emotionally “torment” Mrs. A. She reported behaviors of her brother consistent with antisocial personality disorder. Mrs. A reported a good relationship with her father in childhood and at the time of treatment.
In addition to adverse childhood events of abuse and mistreatment perpetrated by her mother and brother, Mrs. A experienced traumas including rape by a similar-aged peer as a teenager and multiple incidents of military sexual trauma. Mrs. A had five previous marriages and reported stalking, physical, and sexual violence in two of them, with attempted violence directed towards her children. Mrs. A had completed several episodes of trauma-focused treatment, including rape counseling in early adulthood, couples counseling on several occasions, and group therapy for military sexual trauma 5 years before initiating this episode of care.
Mrs. A described a stable relationship with her current husband. She identified as a member of the Baptist faith and regularly volunteered in a pregnancy clinic. Mrs. A reported overall happiness with her life with the exception of fibromyalgia and migraine related pain. Mrs. A was knowledgeable about fitness and nutrition and kept healthy habits such as taking daily walks, working out on her exercise bike, and eating nutritious food. Mrs. A had a master’s level of education; weight, hygiene, and social interactions were within normal limits, and she was generally soft-spoken in session. For sessions conducted in the VA satellite clinic, Mrs. A was accompanied by a PTSD Service Dog trained to stand between her and others to help her feel safe, and to perform tasks like bring her attention to the present moment by nudging her hand to pet him.
5 Assessment
Intake
Mrs. A’s psychosocial history was evaluated during a 1 hour intake session. A semi-structured interview collected information about her current symptoms, upbringing, family of origin, as well as history of relationships, education and work, military service, health and treatment history, and risk for suicidality. During the intake session, Mrs. A was educated about expectations of assessment and treatment in the VA Health Care System, synchronous telehealth care, confidentiality and its limits, and what to do in case of health emergencies while engaged with virtual care. Mrs. A was oriented to person, place, time and circumstance, pleasant, cooperative, and engaged. She was soft spoken, made good eye contact, and affect was constricted. Throughout the intake, her mood was euthymic, her memory appeared to be within normal limits, and judgement and decision-making were fair. Her thought processes were cogent and goal directed and she denied any experience or history of hallucinations or delusions.
Diagnosis of ICD-11 Complex Posttraumatic Stress Disorder
According to the ICD-11, CPTSD is diagnosed when an individual meets diagnostic criteria for DSO in addition to symptoms of PTSD (WHO, 2019). The primary instrument used to diagnose Mrs. A was a semi-structured clinical interview designed to gather ample history and experiences of DSO symptoms in addition to the use of the PTSD Checklist for DSM-5 (PCL-5; Weathers et al., 2013). The diagnostic instruments and techniques selected reflected the best available evidence at the time (addressed in Section 12, Recommendations to Clinicians and Students).
Exposure to an Event or Series of Events of an Extremely Threatening or Horrific Nature
Mrs. A’s first exposure to sexual trauma occurred during childhood and was perpetrated by her brother who she reported exposed himself to her. Over her lifetime, from childhood through adulthood (not including her current marriage), Mrs. A had survived various forms of mistreatment perpetrated by family, intimate partners, and military service members. Mrs. A reported adverse childhood events, including neglect and emotional abuse perpetrated by her mother, and physical and sexual abuse (flashing) perpetrated by her brother. Mrs. A’s mother had major depressive disorder and severe alcohol use disorder. Mrs. A reported her mother often humiliated, embarrassed, or neglected Mrs. A when intoxicated. Mrs. A experienced intimidation and physical abuse from her brother, without intervention from a parent. She reported her mother would often blame her for the abuse perpetrated by her brother. She reported she was orally raped at age 16 and experienced multiple events of military sexual trauma while in the service. Two of Mrs. A’s previous husbands were physically and emotionally abusive. Additionally, one husband perpetrated marital rape shortly after childbirth which resulted in a severe infection, and another threatened physical abuse to one of her children, on one occasion.
Re-Experiencing the Traumatic Event after it has Occurred
Mrs. A reported traumatic nightmares two to three times a month with distress upon waking and increased nightmare frequency during times of increased life stress. She indicated this frequency and intensity of nightmares had been occurring for the last 6 months and confirmed that nightmares occurred during other stressful periods in her life, in varying levels of frequency and intensity.
Deliberate Avoidance of Reminders of the Traumatic Event
Mrs. A avoided talking to or being alone with men with whom she was unfamiliar. She reported avoiding close friendships and gynecological exams due to a pervasive sense of mistrust. Mrs. A reported “shutting down” or “cutting off” emotion when triggered. Mrs. A reported the inability to fully recall details of traumatic events. She reported avoidance had been a symptom she experienced over the course of her entire life, from childhood through the present.
Persistent Perceptions of Heightened Current Threat, Hypervigilance, or Enhanced Startle Reaction
Mrs. A relied on the assistance of medication to aid in the onset of sleep. Despite this, she reported sleep was frequently interrupted by pain and nightmares. She reported her use of a service dog for the last 3 years correlating with the onset of persistent feelings of being “unsafe.”
Severe and Pervasive Problems in Affective Regulation
Mrs. A reported hyperarousal symptoms such as a history of outbursts of anger particularly in the context of intimate relationships. Mrs. A described a current emotional disposition was prone to a “hypo”-arousal response indicated by a pervasive numb feeling when triggered (Briere & Eadie, 2016). She described this as occurring often, in situations that others would perceive as “safe,” and reported she felt without the ability to cope aside from leaving or avoiding such situations. Based on her description of the frequency and intensity of this symptom occurring over three decades in a variety of contexts perceived as safe by others, it was determined to meet diagnostic criteria for “severe and pervasive.” Mrs. A indicated cognitive distortions regarding emotional expression as a weakness that were cultivated in her family (i.e., “If I show emotions, that makes me weak”), which reinforced her constricted affect.
Persistent Beliefs about Oneself as Diminished, Defeated, or Worthless With Feelings of Shame, Guilt, or Failure Related to the Event
Mrs. A reported avoiding deep friendships and the fear that “once others got to know the real [her]” they would not see her as worthy of friendship. She reported that her aging and body image issues were a facet of a pervasive feeling of being “disgusting” that she related to realizing she resembles her mother. These beliefs evoked feelings of shame when memories of her mother’s abuse arose. She reported the onset of this feeling in her teenage years and persisting into the present.
Persistent Difficulties Sustaining Relationships and Feeling Close to Others
Mrs. A reported a history throughout adulthood of having difficulty managing intimate and other close relationships and having a high degree of conflict in those relationships. Her stable current marriage was preceded by 5 marriages which were physically, emotionally, and sexually violent. Mrs. A reported being ashamed of this relationship history. She reported pervasive mistrust and a total lack of friendship, with her family relationships and husband being her only significant relationships. As a result, Mrs. A was slow to warm up, and avoided making close friendships, preferring the company of her husband, children, grandchildren, and father.
Co-Occurring Conditions and Assessment
The Columbia Suicide Severity Rating Scale was administered during the intake session and was negative. In session two, following the intake, self-report measures were used to assess PTSD (PCL-5), CPTSD (clinical interview), and Anorexia Nervosa (Eating Attitudes Test [EAT] and SCOFF questionnaire), (Garner & Garfinkel, 1979; Garner et al., 1982; Hill et al., 2010; Luck et al., 2002; Posner et al., 2011; Weathers et al., 2013). The PCL-5 was administered pre-, mid-, and post-treatment. The EAT and SCOFF were administered pre- and post-treatment.
In session two, the provider discussed the results of the self-report measures and educated Mrs. A on symptoms of eating disorders and the possibility of increased symptoms while doing a trauma focused psychotherapy. On that occasion, she disagreed with the provider’s concern over the possible presence of an eating disorder and was hesitant to discuss the risks of this behavior. In early sessions, her stance on discussing her eating behaviors remained closed off from discussion. However, as treatment progressed, she initiated conversation, incorporating these symptoms into her overall constellation of symptoms and was open to the provider doing so as well.
Diagnostic Clarification and Differential Diagnosis
Other conditions that were considered for the emotional, cognitive, and intra- and inter-personal relationship symptoms and patterns described by Mrs. A included Borderline Personality Disorder (BPD), and Anorexia Nervosa (AN).
Due to the overlap of ICD-11 CPTSD and personality disorder (ICD-11/BPD; DSM-5), the provider considered, but ultimately ruled out an additional diagnosis of BPD (White & Hudson, 2022). Symptoms of affect dysregulation and interpersonal disturbances accounted for by CPTSD have symptom overlap with criteria for BPD (White & Hudson, 2022). However, Mrs. A did not meet criteria for BPD based on the absence of frantic efforts to avoid abandonment impulsivity in areas that are self-damaging, recurrent suicidal behavior, affective instability, chronic feelings of emptiness, and inappropriate or intense anger. She exhibited a pattern of unstable and intense interpersonal relationships, identity disturbance, and severe dissociative symptoms. However, these were better accounted for by CPTSD and were insufficient to warrant a diagnosis of BPD.
Mrs. A endorsed limiting calorie consumption, fear of gaining weight/rumination on losing weight, distorted body image, excessive exercise and a hyperfocus on nutritional food as symptoms indicating the need to screen for AN. At the time of assessment, Mrs. A reported she was 5′5″ tall and weighed 110 pounds, this was consistent with information available in her electronic medical record. Her pre-treatment scores on the EAT (31; positive screen) and SCOFF Questionnaire (score 2; negative screen) provided mixed support for an AN diagnosis. Ultimately, while she evidenced eating disorder symptoms, she did not meet diagnostic criteria for AN and this was ruled out. Due to her insight to the relationship between her body image/eating behaviors and sexual trauma, she agreed to the provider’s suggestion to observe and track these symptoms alongside treatment targeting CPTSD.
6 Case Conceptualization
This case study describes the diagnosis and treatment of CPTSD in a rural veteran using STAIR Narrative Therapy delivered via synchronous telehealth to the veteran in the satellite clinic and her home. Mrs. A reported various interpersonal traumatic events, many sexual in nature, over the span of most of her life. The interpersonal nature of each event indicated the need to assess for CPTSD.
Mrs. A had previously completed episodes of care using EBPs for PTSD in both individual and group therapies which were either phase-one or -two in scope. Symptoms of PTSD were reduced in Mrs. A’s previous therapy episodes of care. Her engagement with rape counseling, marital therapy, and a military sexual trauma support group in previous treatment episodes was beneficial for some of her CPTSD symptoms. Despite the success of those therapies, symptoms continued and were thought to correlate with exacerbating pain conditions and disordered eating. In this episode of care, therapy for Mrs. A was conducted in accordance with the most current and best available, but limited evidence base, for CPTSD using a phased treatment targeting coping skills and then trauma processing—STAIR Narrative Therapy (Cloitre et al., 2012; Herman, 2015; ISTSS Guideline Committee, 2018). In this episode of care, integrated phase-one and -two therapies targeted reduction of DSO symptoms of CPTSD, which manifested in co-occurring trauma, pain, and eating-disordered behavior for Mrs. A.
Following the clinical interview and baseline assessment, a collaborative decision to utilize STAIR Narrative Therapy was made. Mrs. A identified goals for emotion regulation, self-criticism, and feeling distant and cut off from others (consistent with DSO symptom criteria of CPTSD). Mrs. A set a goal to learn to feel comfortable to make requests of others and be assertive without feeling guilty. She also set a goal to reduce excessive dieting and exercise and to be kind to herself around her value/worth relative to her body image and aging. Sessions 1–10 were delivered with the therapist located at the Pacific Northwest VA hospital and Mrs. A located in a clinic office at her nearest CBOC. After session 10, in-home synchronous telehealth was used to minimize the veteran’s commute burden.
7 Course of Treatment and Assessment of Progress
Sessions 0–2
The primary goals of these sessions are education to the therapy model and on PTSD/CPTSD diagnoses, introduction to STAIR narrative, overview of the sessions, introduction of the three channels of emotion coping skills model, and cultivating emotional awareness.
Using a STAIR session 2 handout, Mrs. A identified problems with the following: awareness and expression of emotions, having a delayed emotional response, being irritated by others, believing others will not respect her if they knew what happened to her or that they will be overwhelmed or vicariously traumatized, not trusting others, wanting to avoid or escape emotions, feeling numb or nothing, feeling distant or cut off, feeling overwhelmed by negative feelings in relationships, believing most people will disappoint her, holding in a lot, not wanting to get close, and avoiding relationships (Cloitre et al., 2002). These endorsements were consistent with DSO symptoms identified during the intake interview and captured via the PCL-5.
Sessions 3–6
The focus of sessions 3–6 is developing coping skills for the three channels of emotions (i.e., body, thoughts, and behavior) and distress tolerance. In these sessions, the provider incorporated interventions targeting pain management and eating disordered behavior. Mrs. A was open to these interventions, particularly those that were pain focused. She demonstrated awareness of the relationship between emotional suppression and increased pain flare-ups. To this end, she set a goal to be more cognizant of setting limits with behaviors related to diet and exercise.
Between STAIR protocol sessions five and six, Mrs. A reported she began reading a book on complex trauma that was enhancing her understanding of the holistic, biopsychosocial impact of a lifetime exposure to trauma and positively impacted her engagement in therapy. Mrs. A asked to share a list she had journaled of her trauma events to prepare for exposure sessions. There were multiple traumas that had occurred frequently (e.g., domestic violence, sexual harassment, and coercive sex). She elected to list composites of those events when constructing the exposure hierarchy. During these sessions, Mrs. A demonstrated an increased range of affect and emotion regulation skills evidenced by her willingness to express tearfulness and her endorsement of the following feelings: abandoned, sad, vulnerable, afraid, and anxious.
In sessions devoted to developing coping skills for emotions, interventions targeting pain management and disordered eating were integrated. During these sessions, Mrs. A demonstrated an increased range of affect and emotion regulation skills evidenced by her willingness to express tearfulness and decreased alexithymia.
Sessions 7–12
These sessions focus on interpersonal and relationship skills beginning with examining relationship schemas, and using assertiveness, flexibility, and closeness to change relationship patterns.
Of particular importance, in these sessions, Mrs. A worked to reformulate relationship schemas developed in childhood with her abusive brother and mother. Mrs. A called these “deep rooted” and noted “Asking for something I need or want is a burden to others.” She demonstrated insight to emotional and behavioral responses of these beliefs that developed and persisted throughout most of adulthood including suppressing emotions and avoiding close relationships with friends and intimate partners. Mrs. A created a goal related to learning to make requests of others in session nine which focused on assertive communication. A significant pattern Mrs. A noticed when doing relationship patterns worksheets is that she is able to use assertiveness, but assertiveness triggered self-critical thoughts, perfectionism, and feeling bad about her appearance; her goal was to reduce that consequence of assertive communication. Most notably, after session ten, as a result of the recent work on relationship boundaries and completion of the Basic Rights worksheet, Mrs. A demonstrated a marked shift in perspective. In session ten, she spoke openly about her tendency to use distance in relationships for safety. She noted that she had been “realizing more” the effect of her mother’s abuse/neglect and erratic behavior on her ability to deal with emotions and function well in relationships. Prior to this, she was prone to cognitive distortions, minimizing these adverse childhood events with statements like, “It was a long time ago and I need to just get past it,” “I’m making something out of nothing,” and “It couldn’t have been that bad if I’m fine now.” After this point, she made it a goal to be more kind to herself around her value/worth relative to her body image and aging. Beliefs evidencing self-compassion and kindness were observed in session.
In sessions targeting relationship skills, Mrs. A worked to reformulate relationship schemas developed in childhood with her abusive brother and mother. She demonstrated insight to cognitive, affective, and behavioral patterns that had developed in childhood and persisted throughout adulthood. After session ten, Mrs. A demonstrated a marked shift in perspective. She was more willing to self-validate the impact of her mother’s abuse/neglect and erratic behavior on her ability to deal with emotions and function in relationships, whereas prior to this, she was prone to cognitive distortions minimizing the abuse.
STAIR Narrative: Sessions 12–19
Prior to starting STAIR, Mrs. A’s symptoms of PTSD were measured using the PCL-5 (total = 54). Her total score after completing sessions 1–12 (STAIR) focused on developing coping skills was 51. To facilitate narrative sessions, Mrs. A was guided through creating an exposure hierarchy. For traumas that had occurred frequently (e.g., interpersonal violence, sexual harassment, and coercive sex), Mrs. A elected to list composites of those events on the exposure hierarchy. The subjective units of distress scale were employed during the hierarchy construction to enhance her proficiency using this tool. Seven narrative/exposure sessions were completed.
Exposure sessions contained significant events for the presentation of this case. Following the first exposure session, Mrs. A demonstrated an increased range of affect and marked openness. Integration and perspective shifting was demonstrated in her increased self-validation and self-compassion. She reported talking with her daughter and husband about her therapy as well. After the third narrative session, Mrs. A reported a change to how she “carried” the memories after doing the between-session in vivo and imaginal exposure practice; she regarded this as an improvement. In exposure session four, eight IPV events (as a composite event) were processed. Mrs. A reported exposure session four was “easier” than she expected due to her familiarity with the process; she reported feeling “relieved” after the exposure, demonstrating habituation of the memory. Mrs. A demonstrated significant insight, relating her distress around aging and body image with the exposure conducted in session four. She elected to end the exposure early stating she was “done with it.” At the beginning of exposure session five, Mrs. A reported the previous week was “horrible” and she reported increased irritability, pain, panic, and use of medication to manage anxiety. Mrs. A reported it was “hard” to hear her expressed emotions (on the imaginal recordings) and it felt “surreal” to hear her own voice telling the stories of those events; “I can’t believe I survived those things. They actually happened. I also feel guilty for what my children went through.” Mrs. A was asked about the decision made to end the exposure during the processing session addressing IPV and she reported her distress was too prolonged to continue at that time. She expressed that by completing between-session imaginal exposures, the memory had become easier to recall without severe distress. To be sure, she elected to revisit the memories in this session via a brief exposure (25 minutes) while monitoring SUDs, which remained low, confirming the memory had habituated. In the sixth exposure session, Mrs. A reported an uptick in migraines. She ceased her volunteer work due to having too much to do around the holidays. In the seventh and final exposure session, Mrs. A demonstrated marked increase in her range of affect, laughing and smiling freely, and showing a somber tone when reflecting on milestones of therapy. Discussion of the need to continue therapy resulted in her decision to terminate therapy after one more session to summarize and close this episode of care. Mrs. A stated, “I hate to think I’m fooling myself but I’m feeling so different lately.” She provided examples: feeling better about her self-image and weight, feeling validated about her adverse childhood experiences and how they impacted her, resuming interests she previously stopped (i.e., creative writing), and increased depth in relationships with children, father, and spouse. She reported remembering pleasant dreams more frequently, self-validating the pain of events from childhood, and feeling more at ease around unfamiliar men.
Mrs. A arrived to the final session maintaining the improvements observed in the previous session. She reported feeling “good” and shared a creative writing exercise she completed of her own volition related to a self-compassion focused assignment. She read a creative nonfictional account of her journey through this episode of care and her “new life.” She was tearful on occasion when reading this. She reported that “talking about the traumas from childhood was the significant work this time. I had talked about so much of the other stuff before. Talking about it and coming to grips with it and making realizations that it was abuse and neglect were significant.” She reported she had a newfound sense of “what’s going on inside of me.” Therapy was summarized and reviewed and a plan was made to check in by phone in a few months; post-treatment assessment was completed.
Pre- and Post-treatment Assessments.
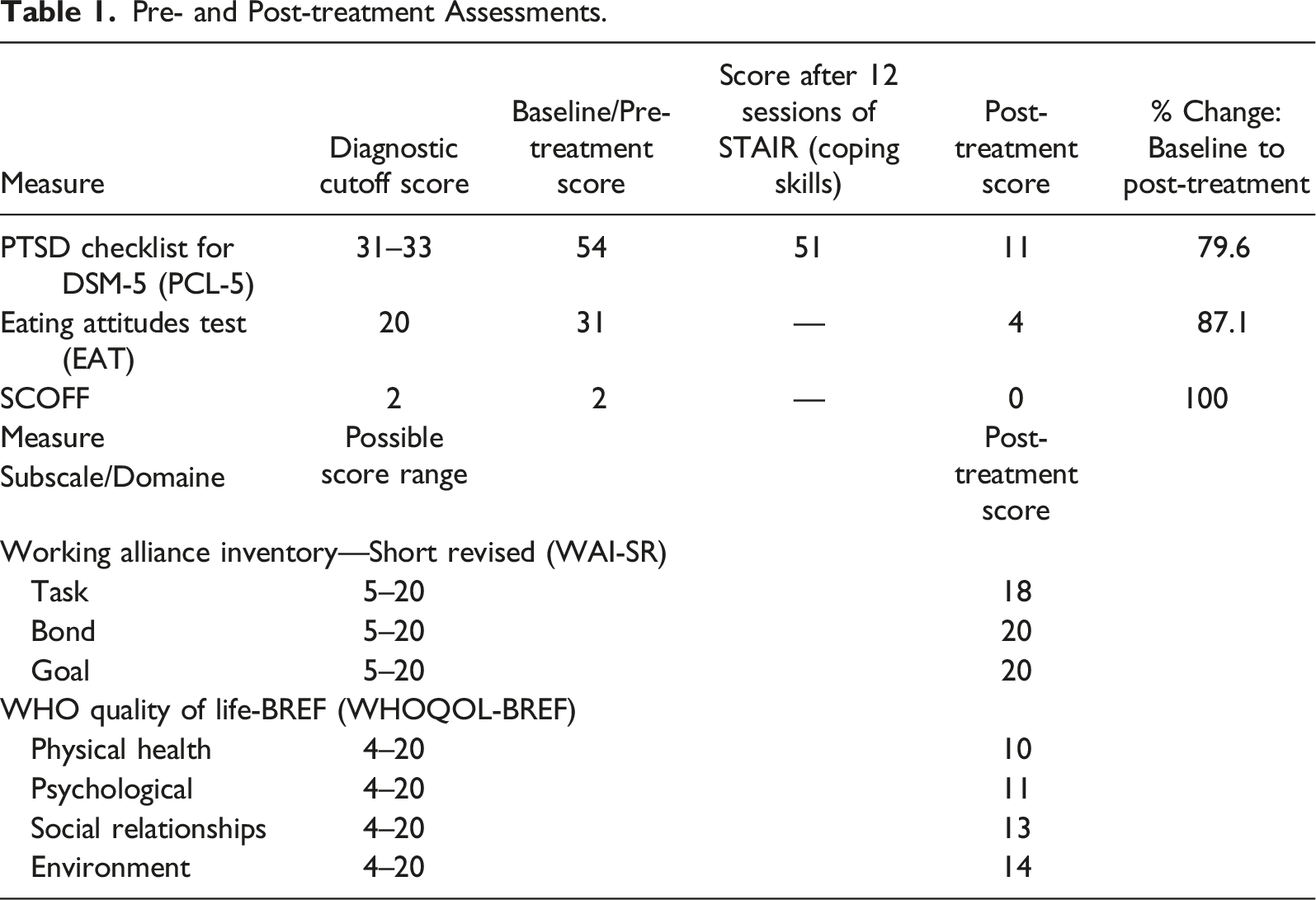
A qualitative review of Mrs. A’s change in CPTSD symptoms demonstrates the success of this episode of care, to be considered alongside the presentation of the self-report measures changes. Through focusing therapy on the DSO sequelae and interpersonal traumas sustained in childhood and adulthood, Mrs. A was able to gain a deeper level of recovery than in previous trauma-focused episodes of care. Following therapy, Mrs. A reported decreased symptoms of re-experiencing such as having pleasant dreams replace traumatic nightmares. Her statement touting the benefits of this episode of care that focused on childhood traumatic events for the first time demonstrated how her willingness to confront things previously avoided, denied, and minimized opened up a different level of recovery from CPTSD. Reduction in avoidance was further indicated by her willingness to talk about her history with her family, and feeling more willing to be around men she does not know (this also indicated her reduced hyperarousal/hypervigilance and increased ability to monitor and regulate cognitive distortions and affect dysregulation). Mrs. A reported improved sleep as an example of improvements to hypervigilance/hyperarousal. Her most significant improvements were in DSO symptoms. Following therapy, Mrs. A reported being increasingly at ease in situations previously perceived as threatening. She demonstrated increased range of affect, observed by the provider as, laughing and smiling freely, allowing herself to be tearful when reading a self-compassion statement she had written, and showing a more somber tone when reflecting on milestones of therapy. She reported she had a newfound sense of “what’s going on inside of me” as evidence of her decreased avoidance and increased ability to regulate emotions. Symptoms of both CPTSD and disordered eating shifted significantly alongside changes to distortions related to negative self-concept, such as “If I show feelings, then I am weak,” “If I ask something of someone, I am a burden,” and “I am disgusting.” Following therapy completion, she indicated feeling better about her self-image and weight, feeling validated about her adverse childhood experiences and how they impacted her, resuming things she previously stopped (i.e., creative writing). Her improvements in self-concept and avoidance had a cascading effect on interpersonal functioning; her relationships with her father, husband, and children improved as she shared more of her personal history and therapy work with them.
8 Complicating Factors
Two complicating factors emerged in this episode of care. The first were issues related to telehealth. The veteran’s commute to the VA satellite clinic became burdensome, which we addressed by moving to in-home telehealth. However, she lived in a rural area where bandwidth at times was inadequate. To address this, Mrs. A and her therapist flexed to phone appointments as needed. Lastly, the application she used to record exposure sessions malfunctioned on two occasions.
The second complicating factor was the veteran’s low insight to eating disorder symptoms and concern. Over the course of therapy, as she was provided education on these symptoms in a non-judgmental and accepting manner by the therapist, the veteran gained insight and as the rapport built between provider and veteran, she became more open to sharing these symptoms, her challenges with them, and the changes to them.
9 Access and Barriers to Care
Synchronous telehealth offers access to qualified providers and treatments; however, it is not without service delivery complications. While STAIR therapy has a smart phone application for iPhone devices, it did not have an equivalent for Android devices at the time of this publication. Therefore, the therapist elected to use the PE Coach application for recording exposure sessions. At times, the application would malfunction and fail to record all or part of the session, and minor protocol deviations were made to accommodate these unpredictable failures of technology. In rural areas, Internet connectivity may be inconsistent. On a few occasions, Internet connectivity was insufficient to maintain audio and video. These issues were addressed in session; ultimately, Mrs. A elected to continue with synchronous telehealth in spite of temporary periods of poor connectivity.
10 Follow-Up
Following therapy, Mrs. A reported having pleasant dreams come back to her, feeling willing to talk about her trauma history with her family, and feeling increasingly at ease in situations previously perceived as threatening. Through focusing therapy on the DSO sequelae and interpersonal traumas sustained in childhood, Mrs. A experienced greater recovery and fewer residual CPTSD symptoms than in previous episodes of care. Symptoms of both CPTSD and disordered eating decreased alongside changes to distortions related to negative self-concept, such as “If I show feelings, then I am weak,” “If I ask something of someone, I am a burden,” and “I am disgusting.” Interpersonally, her relationships with her husband and children improved as she shared more of her personal history and therapy work with them. Emotion regulation demonstrated a marked improvement over the course of therapy in her increased range of affect and ability to tolerate emotions without “shutting down.”
11 Treatment Implications of the Case
The case study of Mrs. A presents delivery of STAIR Narrative therapy delivered via synchronous telehealth to a rural woman veteran with CPTSD. This veteran completed 19 sessions of STAIR Narrative (12 sessions of STAIR followed by seven sessions of narrative exposure therapy) targeting CPTSD with disordered eating. Mrs. A’s response to this intervention illustrates the successful treatment of a rural woman veteran with CPTSD and comorbidities using a phased, EBP over synchronous telehealth delivered clinic-to-clinic and in-home.
Despite the technological challenges of delivering CPTSD therapy via synchronous telehealth, the need for mental health treatment using this modality drastically increased with the onset of the COVID-19 pandemic. Prior to 2020, literature examining the use of EBPs for CPTSD over synchronous telehealth was limited. This case study provides an overview of synchronous telehealth implementation of STAIR Narrative Therapy with a veteran who met ICD-11 criteria for CPTSD in order to support other providers using these types of treatments and synchronous telehealth modalities. Additional research on efficacy and effectiveness of STAIR Narrative Therapy and other CPTSD therapies conducted via synchronous telehealth is needed, particularly as they become offered more widely over this platform.
12 Recommendations to Clinicians and Students
Telehealth presents a significant opportunity for increasing access to care. However, it also presents various, at times unpredictable, challenges as well. It can collude with avoidance, minimize access to paralinguistics and behavioral data valuable in the context of therapy, present unpredictable failure or malfunction of technology, or highlight one’s lack of experience or proficiency with technology. These issues can be difficult to rebound from when the condition being treated has hallmark features of emotion dysregulation and negative self-concept as occurs with CPTSD. It is highly recommended that the provider model flexibility and humility in responding to the challenges of telehealth in order to assist with troubleshooting such issues without escalating them. Engaging additional staff or family/friends of the recipient of treatment is recommended in order to assist with limits to technology proficiency.
As part of the psychoeducation that typically is provided during assessment and treatment, we encourage the use of collaborative treatment planning with clients and patients diagnosed with CPTSD. Offering options for care and educating those engaging in care to the different approaches, while assisting them in weighing the pros and cons, contributes to rapport and empowerment of individuals who likely have been disempowered via their traumatic experiences. It is highly encouraged to collaborate on treatment planning to find appropriate treatment strategies and goals.
Similar to other individuals who have experienced multiple traumatic events, and recurring interpersonal traumas, it can be challenging to directly connect sequelae with the event in some instances, and in others, the connection may be consciously recognized. This was the case for Mrs. A. The relationship between symptoms like her self-concept that she was “disgusting” was consciously connected to trauma resulting from her mother’s abuse. She was able to identify that her eating disordered behavior was related to her experiences of sexual victimization. Other symptoms were difficult to connect to specific traumatic events.
Etiologically, CPTSD is characterized by trauma in the context of ongoing, interpersonal relationships. When trauma occurs in this context, and during developmental years in particular, often there are diverse and severe impacts to a person’s sense of self, nervous system and affect regulation capabilities, and interpersonal relationships. A position paper, developed by trauma experts addresses the implications of these characteristics through the recommendation for phase-based care (ISTSS Guideline Committee, 2018). Reprocessing trauma in the absence of skills to self-regulate threatens the success of interventions. As such, a phase for developing coping skills relative to the DSO symptoms is the foundation of phase-based treatment for CPTSD. While not all individuals with CPTSD may need this, it can be a beneficial bedrock upon which reprocessing therapies may follow.
There are important implications regarding the diagnosis, assessment, and treatment of CPTSD that should be addressed vis-à-vis this case presentation. When Mrs. A’s treatment commenced, the diagnostic criteria of CPTSD had been agreed upon. However, ICD-11 was not yet published. To date, the diagnosis of CPTSD is omitted from the DSM-5. At the time of her care, the International Trauma Questionnaire (ITQ; Hyland et al., 2017; International Trauma Consortium, n.d.), developed in 2017 and validated with a British clinical sample to be consistent with the ICD-11 diagnosis of CPTSD was not yet widely studied. From 2019 on, it has been translated into 32 languages and has been validated with additional samples (International Trauma Consortium, n.d.). In March of 2020, it was validated with veteran population (Murphy et al., 2020). This case highlights the dilemma of treating individuals amidst a developing research base. An international diagnostic manual was used despite the fact that the client, clinician, and treatment took place in the United States (where the DSM-5 is more commonly used) because it more appropriately represented her clinical presentation. The ITQ was not yet validated with military veterans, however, the PCL-5 was. The use of ICD-11 for diagnosis and the PCL-5 which measures DSM-5 PTSD symptom and was developed and validated with United States military veterans is not ideal, and the therapist used clinical interview data of DSO symptoms to supplement PCL-5 self-report data as a result. Since the case of Mrs. A, the empirical base of assessment and treatment for CPTSD has well advanced. We recommend that clinicians and students consult current clinical practice guidelines, position papers, and empirical literature prior to starting CPTSD treatment.
Lastly, though this case presentation illustrated phase-based care that followed the manual linearly from coping skills to trauma processing, a flexible modular approach has been advised by field experts (Karatzias & Cloitre, 2019). In this approach, it is recommended that flexibility in choosing empirically supported interventions and the order in which they delivered should be based on a triaging of client needs and relevance. This approach ensures the delivery of patient-centered care that is evidence-based. Both qualities enhance the likelihood of successful treatment, client satisfaction and relationship with provider, reduction of symptoms, and improvements in quality of life.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by grant number K12HS026370 from the Agency for Healthcare Research and Quality (BZ).
Informed Consent
The authors are appreciative of the patient presented in this case study. Her persistence, courage, and dedication provided valuable insights to the therapeutic process and facilitated the process of change. This material is the result of work supported with resources and the use of facilities at Veterans Affairs Portland Health Care System and Oregon Health & Science University, Portland, OR, USA.
Disclaimer
The contents of this article do not represent the views of the U.S. Department of Veterans Affairs or the United States Government or the Agency for Healthcare Research and Quality. All authors approved this manuscript and this submission.