
Abstract
The current case describes the implementation of Acceptance and Commitment Therapy (ACT) and self-compassion interventions with a 37-year-old Queer Hispanic woman “Cynthia” (pseudonym). Cynthia presented to a university training clinic, reporting pervasive difficulties with anxiety, an associated pattern of depressive episodes, and a trauma history. The therapist conceptualized Cynthia’s presenting problems through an ACT-based psychological flexibility framework. Functional analysis indicated intolerance of uncertainty, fusion to self-critical thoughts, and experientially avoidant behaviors (e.g., pervasive worry) contributed to Cynthia’s anxiety. Values clarification, as well as mindfulness- and acceptance-based interventions, were met with gains in quality-of-life scores and decreases in worry scores as treatment progressed. Additionally, self-compassion interventions were implemented to address pervasive self-criticism and feelings of low self-worth. Across 37 sessions, from pre-to-post treatment, Cynthia’s quality of life scores increased by 62.5%, and worry decreased by 52.8%. These results provide support for using ACT and self-compassion interventions for anxiety and co-occurring depression with a Queer, Hispanic woman.
Keywords
1 Theoretical and Research Basis for Treatment
Generalized anxiety disorder (GAD) is characterized by excessive anxiety and worry about everyday events or activities (e.g., health, finances, work, household chores), including difficulty controlling worry, over a period of six months (American Psychiatric Association [APA], 2013; World Health Organization [WHO], 2018). The lifetime prevalence of GAD is estimated to be nine percent (APA, 2013). Individuals with GAD experience worry as uncontrollable, disruptive, and often report physical symptoms such as muscle tension, sweating, diarrhea (APA, 2013; WHO, 2018).
Females are twice as likely as males to experience GAD, and comorbidity for females most often includes other anxiety disorders and unipolar depression (APA, 2013). Indeed, most individuals with GAD also meet criteria for major depressive disorder (MDD; 59.0%) or another anxiety disorder (55.9%; Sunderland et al., 2010). In adults with comorbid GAD and MDD, approximately two-thirds (66%) experience recurrent MDD (Moffitt et al., 2007). The robust relationship between GAD and MDD suggests common underlying cognitive and behavioral processes; a view consistent with recent research and intervention development focused on common “transdiagnostic” processes (Hayes & Hoffman, 2018Hayes & Hofmann, 2018).
Common processes thought to underlie anxiety and mood disorders include, but are not limited to, cognitive misappraisals (i.e., unhelpful, negative predictions of events and their consequences; Barlow et al., 2016); experiential avoidance (i.e., unwillingness to experience unwanted private events); and emotion-driven behavioral responding (i.e., negatively reinforced behavioral efforts driven by emotional states; Barlow et al., 2016). Targeting transdiagnostic processes ought to result in improvements for those with anxiety and mood disorders, as well as those with comorbid presentations, largely because such interventions address root sources of suffering that give rise to the symptoms. Indeed, transdiagnostic cognitive-behavioral therapies have been found to be as effective as disorder-specific cognitive behavioral therapy for anxiety (g = .15), and superior in effectiveness for depression alone (g = .58; Newby et al., 2015) and comorbid presentations of anxiety and depression (Norton et al., 2013).
Acceptance and Commitment Therapy (ACT)
Acceptance and Commitment Therapy (ACT) is an evidence-based transdiagnostic treatment that belongs to a family of mindfulness and acceptance-based interventions within cognitive behavioral therapies (Hayes et al., 2012). Over the past 20 years of research, ACT has assisted in developing Process-Based Therapy (PBT) and has moved toward a unified, personalized model of treatment (Hayes et al., 2022). From an ACT perspective, the presence of anxious thoughts, feelings and physical sensations (i.e., symptoms) are not necessarily viewed as problematic or “disordered.” No direct effort is made to alter unwanted thoughts, sensations, and emotions. Instead, ACT introduces skills to help clients accept unwanted thoughts, emotions, and physical sensations whose form and frequency are beyond their control and commit to taking actions that embody valued living (Eifert & Forsyth, 2005). Accordingly, the ACT intervention model of psychological health is comprised of mindfulness/acceptance processes and commitment/behavior change processes (Hayes et al., 2012). This model is also consistent with other acceptance-related processes important for well-being, including self-compassion (i.e., the practice of treating oneself with kindness, understanding, and acceptance in times of suffering, failure, or inadequacy; see Neff & Tirch, 2013).
More broadly, the primary aim of ACT is to increase psychological flexibility and decrease psychological inflexibility. Psychological flexibility offers a unified transdiagnostic model of human flourishing and behavior change and is comprised of six related processes: self-as-context (i.e., flexible perspective taking of oneself as an aspect of “I-here-nowness”); defusion (i.e., seeing private events as mere experiences vs. literal truths); acceptance (i.e., willingness to experience unwanted private events just as they are); flexible attention to the present moment (i.e., ability to flexibly, voluntarily, and purposefully be in contact with events in the present); chosen values (i.e., clarification of, and connection to, what a given client really cares about in this life); and committed action (i.e., engaging in overt behaviors in line with what matters most; Hayes et al., 2012). Psychological inflexibility denoted the inverse of these processes (e.g., experiential avoidance instead of acceptance; see Hayes et al., 2012) and can be described as a pattern in which behavior is excessively influenced by unwanted private events (e.g., thoughts, feelings, physical sensations) or avoidance of these experiences at the expense of more effective and value-guided actions (Levin et al., 2014). Together, core processes within psychological flexibility and psychological inflexibility provide an understanding of processes that maintain client problems and those that may serve as intervention targets.
To date, ACT has been applied to numerous presenting problems and evidence supports the effectiveness of ACT in comparison to active and inactive controls for a variety of conditions, including anxiety, depression, and transdiagnostic presentations (Gloster et al., 2020). Relative to comparison conditions, ACT yields small to medium effect sizes (g = 0.18–0.57) for anxiety and depressive disorders (g = 0.24–0.76), and small to large effect sizes (g = 0.17–0.96) for transdiagnostic clinical presentations (Gloster et al., 2020). Evidence also supports the utility of ACT across populations and groups, including members of the LGBTQI + community (Fowler et al., 2022), individuals of low socioeconomic status (Gregg et al., 2007), women with a history of interpersonal victimization (Fiorillo et al., 2017), and individuals of Hispanic descent (Kwon et al., 2022). Collectively, this work suggests that ACT ought to be useful for diverse individuals with comorbid anxiety and depressive concerns.
2 Case Introduction
“Cynthia” (a pseudonym) was a 37-year-old cisgender, Queer, Hispanic woman who self-referred to the psychological training clinic of a large northeastern university for difficulties with pervasive anxiety and an extensive history of past recurrent depressive episodes. The therapist was a clinical psychology doctoral student in their second year of training supervised by licensed clinical psychologists. The therapist received weekly hour-long individual and group supervision throughout treatment. Identifiable details in this case have been changed to protect client confidentiality and comply with clinic policies.
3 Presenting Complaints
Cynthia’s primary presenting concern was anxiety and worry surrounding multiple life domains including work, romantic relationships, health, finances, and miscellaneous everyday activities. She reported several distressing physical symptoms associated with her anxiety, such as lightheadedness, racing heartbeat, and fatigue. She reported that increased anxiety symptoms often led to depressive episodes and an intense fear of future depressive episodes.
4 History
Cynthia was born and raised in a medium-sized metropolitan area in the northeast. She is an only child and reported not being close to immediate or extended family members. She recalled that her parents fought often and separated when she was three years old. When Cynthia was eight years old her mother moved to Puerto Rico, and she indicated being raised mostly by her father. She reported being estranged from her mother and having a tumultuous relationship with her father since early childhood. She dropped out of high school and experienced brief homelessness at age 17, which she attributed to arguments with her father.
Cynthia denied current substance abuse and reported a suicide attempt at 17, involving an overdose of sleeping pills following a fight with her father. While conscious, she contacted a friend and was transported to the hospital where she was evaluated and discharged within 24 hours. She then briefly moved to Puerto Rico to develop a relationship with her mother but moved back after six months. While in Puerto Rico Cynthia reported being sexually assaulted by a family member.
Since age 17, Cynthia indicated a history of anxiety and depression, marked by intense worry and fear of the unknown. She reported worrying about numerous issues, such as the health of herself and loved ones, financial insecurity, potential future depressive episodes, being a burden to others, and everyday events. She also reported a history of difficulties in her intimate relationships (e.g., partners not respecting her boundaries, feelings of worthlessness). Cynthia indicated that prolonged anxiety spikes often precipitated her previous depressive episodes (around 20 episodes over the past 20 years, each lasting up to three months).
Cynthia had an associate degree from a local community college and reported a varied work history as a landscaper, housecleaner, and grocery store employee. At intake, Cynthia’s yearly income was estimated at $8000 USD. She also stated she was a few thousand US dollars in debt, which contributed to her stress. Cynthia reported having a Queer identity, relationship history dating individuals of all genders, and indicated having a cisgender identity. She noted being Queer as an important and salient part of her identity, as she had found community and close relationships in Queer spaces throughout her life. Cynthia reported being in a long-distance non-monogamous relationship for the last two years and noted a positive aspect of her recent move was being geographically closer to her partner.
5 Assessment
The formal assessment process involved one two-hour intake interview and included a comprehensive psychosocial and medical history and a structured diagnostic interview. Symptom and outcome measures were given weekly in accordance with measurement-based care (Boswell et al., 2022). Cynthia presented as well-groomed, casually dressed, and was cooperative throughout. She was fully oriented to person, place, and time, demonstrated clear, logical, and coherent verbal processing, and appeared to be in a euthymic mood. Her short-term memory was intact, but her long-term memory was slightly diminished, making it difficult for her to recall specific years of life events, patterns of depressive episodes, and details of her psychological history and previous treatment. There was no indication of hallucinations or delusions, and reality testing was intact. She reported daily passive suicidal ideation but denied any plan or intent to complete suicide or any homicidal ideation.
Measures
The Quality-of-Life Enjoyment and Satisfaction Questionnaire- Short Form
The Valued Living Questionnaire (VLQ; Wilson et al., 2010) is a two-part instrument designed to assess valued living. Individuals rate (a) the importance of 10 domains of living on a 10-point Likert-style and then (b) how consistently they have lived in accord with their values within each domain over the past week. Cynthia’s Importance score (55) was higher than her Consistency score (48), suggesting a discrepancy in her ability to engage with her values. The largest discrepancies were in work and self-care in which Cynthia reported she was “working too much” and “not taking care of herself enough.” This scale was administered once at intake to establish a foundation for introducing values and committed action in treatment and to guide the therapist and Cynthia in identifying key treatment targets.
The Penn State Worry Questionnaire (PSWQ; Meyer et al., 1990) is a 16-item measure assessing the generality, excessiveness, and uncontrollability of worry. The PSWQ is sensitive to changes in worry and GAD symptoms across treatment (Dear et al., 2011). Cynthia’s baseline PSWQ score of 72 is comparable to scores of patients with GAD (Turk et al., 2001) and exceeds the cut score of 65 for optimal specificity and sensitivity (Fresco et al., 2003).
The Mini-International Neuropsychiatric Interview (MINI; Sheehan et al., 1998) 7.0.2 is a brief structured diagnostic interview assessing symptom criteria for 17 common psychiatric disorders in a manner consistent with the Diagnostic and Statistical Manual of Mental Disorders - 5th ed. (DSM-5; APA, 2013). Cynthia endorsed symptoms of anxiety, worry, and several previous major depressive episodes but did not endorse any other psychopathology.
Primary and Differential Diagnosis
At the time of intake, Cynthia met DSM-5 criteria for Generalized Anxiety Disorder (F41.1) as her primary presenting diagnosis. Though she did not meet diagnostic criteria for Major Depressive Disorder at intake, she did met criteria for Major Depressive Disorder (F33.42), with recurrent past major depressive episodes, in full remission. Additionally, several other differential diagnoses were considered and ruled out as described below.
Adjustment Disorder With Mixed Anxiety and Depressed Mood
Cynthia reported multiple discrete stressors in the 12 months before intake, including the loss of her grandmother, dog, and best friend, as well as moving cross-country to help take care of her sick father, losing social support of her housemates, and experiencing financial instability. However, an adjustment disorder diagnosis was not appropriate, as her anxiety-related distress predated these events, and her responses to her losses appeared appropriate and proportionate to their severity.
Post Traumatic Stress Disorder (PTSD)
Cynthia reported experiencing a traumatic event at age 16 when a family member sexually assaulted her, along with other PTSD-consistent symptoms such as avoidance of her mother’s side of the family and negative self-beliefs (e.g., “I will never be good enough.”) However, she denied intrusive symptoms and indicated that she had successfully addressed this trauma in her previous therapy work. Cynthia’s avoidance of her mother’s family was not related to the assault. Rather, her avoidance was a boundary established after her previous successful PTSD-specific treatment to address her mother’s verbal abuse.
6 Case Conceptualization
Cynthia’s difficulties were conceptualized in accordance with the six processes of the ACT psychological (in)flexibility model (Hayes et al., 2012). From an early age, Cynthia attributed her parents’ unhappiness and escalating conflicts during custody to her own perceived shortcomings as their child (e.g., “I am not enough to make them happy”). Further, when Cynthia’s mother relocated to Puerto Rico, it exacerbated her feelings of being unwanted and inadequate (e.g., “I’m unlovable, why else would my mom leave?”). Such thoughts, in turn, were taken as literal truths and subsequently organized her behavior in unhelpful ways (i.e., cognitive fusion). Moreover, the believability of such thoughts was further reinforced during a later visit to Puerto Rico. After Cynthia was sexually assaulted, her mother displayed no concern for her well-being and instead protected the perpetrator. As a result, Cynthia learned to isolate and keep to herself when experiencing pain and feared rejection if she were to reach out to others for support. Collectively, these events contributed to Cynthia having a rigid and largely unhelpful view of herself (i.e., attachment to the conceptualized self) that persisted from childhood to intake.
Additionally, Cynthia’s anxiety associated with perfectionistic, reassurance-seeking behaviors (e.g., asking her father to review homework she had checked multiple times) was reinforced by evoking words of comfort and affirmation from her otherwise “never impressed” father. Her worry and self-isolation, in turn, appeared to be adaptive in the short term (e.g., worry prepared Cynthia for difficult conversations; isolation and avoidance prevented future painful rejection). However, these behaviors appeared unhelpful and seemed to interfere with her life.
Cynthia’s pervasive worry was often expressed in-session (e.g., “I have so much to do after this appointment”) and was consistent with her quantitative self-report (e.g., PSWQ scores). As a process level, Cynthia’s worry appeared to function as a form of experiential avoidance. Here, worry distanced her from contacting emotions associated with feared outcomes while also altering physical and emotional sensations accompanying her anxiety and fear. Worry offered Cynthia temporary relief from intense emotions and unwanted physical sensations. Yet, worry also seemed to increase the intensity of her anxiety (e.g., fatigue, gastrointestinal discomfort, muscle tension, racing heart) and get in the way of what she cared about (i.e., inaction, impulsivity and avoidant persistence).
Cynthia appeared to be cognitively fused with various self-critical thoughts (e.g., “I am not good enough) and memories of perceived personal failings from the distant (e.g., her mother’s abandonment) and recent (e.g., accrued debt) past. This cognitive fusion and worry made it difficult for Cynthia to be in the present moment. She added that her coworkers, acquaintances, and close friends often perceived her lack of presence as a sign of disinterest and would judge her for that (i.e., inflexible attention). As a result, Cynthia avoided rejection by avoiding social interactions or seeking reassurance in close relationships.
Cynthia appeared to have a clear understanding of her chosen values and related actionable behaviors. However, Cynthia’s learning history and desire for short-term relief from undesired emotions kept her stuck in a self-perpetuating cycle where thoughts related to her values and goals operated as antecedents for avoidance behaviors. Further, her recent move and change in environment served as a constant reminder of the most challenging time in her life. Cynthia’s need to control and escape her anxiety effectively interfered with her ability to engage in actions consistent with her values, leaving her feeling depressed, unmotivated, and inadequate (i.e., lack of contact with values).
7 Course of Treatment and Assessment of Progress
Including the initial diagnostic interview, Cynthia attended 37 weekly, 50-min psychotherapy sessions over about 10 months. While the average number of ACT sessions for anxiety disorders is between 6-12 (Ferreira et al., 2022), ACT is flexible in nature. Case studies have indicated that persons may continue to derive benefits from longer episodes of care (Brem et al., 2020). More pragmatically, the focus of ACT is on tailoring the intervention to meet the unique needs of each person, with the aim being to help the client change in ways that are durable and meaningful.
Psychoeducation and Treatment Orientation (Sessions 2–3)
The first two therapy sessions focused on establishing rapport, providing psychoeducation about anxiety and fear, introducing the interactive and participatory nature of ACT, and defining the goals of ACT in the context of the client’s values (Eifert & Forsyth, 2005). Further, these sessions also focused on establishing a queer-oriented, accepting space in the therapy room. The therapist used a metaphor of two people climbing individual mountains (i.e., the “Two Mountains Metaphor”; Harris, 2019), to exemplify the collaborative journey that would be taken together. Though many of Cynthia’s treatment goals focused on valued behaviors, she also voiced an emotional goal of wanting to experience less anxiety The third session introduced the unworkability and paradoxical nature of anxiety control efforts and set the scene for an alternative response to anxiety: acceptance.
Phase 1. Creating an Acceptance Context in the Face of the Unexpected (Sessions 4–9)
Evaluating the Workability of Control
Building upon the previous session, the therapist and Cynthia explored the workability of strategies she used to cope with anxiety and stress (e.g., avoiding family and friends), what made her “feel better” (e.g., watching television, drinking a high ABV beer), and the costs associated with these strategies. Though the short-term effects of these strategies appeared to work (e.g., “takes the edge off,” temporary relief), these efforts often exacerbated Cynthia’s anxiety, led to self judgement and guilt (e.g., “I am a bad friend”), and cost her in many other ways (e.g., feeling sluggish and disconnected after drinking, missed time and memories with friends and family). Through this process Cynthia began to see the costs of her avoidance and continued unworkable nature of these behaviors, despite her continued efforts. Ten years of previous therapy, though at times helpful, left Cynthia feeling like a failure.
Creative Hopelessness
Throughout the early sessions, it became clear that wanting to “be less anxious” was a primary goal for Cynthia. Knowing that it would be impossible to continue with ACT and accomplish this goal, the therapist guided Cynthia through experiential exercises that demonstrated the futility of struggling with anxiety. For example, Cynthia engaged in the “Tug of War with A Monster” (Hayes et al., 2012) exercise. The therapist played the role of anxiety, and Cynthia played herself as both pulled on opposite ends of a rope. This experiential exercise made salient the futility of the struggle with anxiety (i.e., she never wins for good).
Cynthia quickly caught on to acceptance and an alternative to struggling, and this entailed her willingness to drop the rope. The therapist periodically swung the rope towards Cynthia during the session, creating an opening to re-engage the exercise. Cynthia found herself with the rope in hand, pulling against the therapist multiple times, and laughed in bewilderment at how automatic it was for her to grab the rope. Cynthia identified with this metaphor, recognizing that her control efforts (e.g., avoidance, drinking) were like “picking up the rope.” In future sessions, when she described unworkable attempts to change her anxiety, the therapist gently reminded her to consider if she was holding the rope and, if so, she can let go and chose acceptance.
Attending to the Present With Mindful Acceptance
Five sessions into treatment, Cynthia experienced a sudden breakup from her long-term partner. Though the breakup could have hindered progress, it became a motivating factor for Cynthia. The therapist observed Cynthia’s pain showing up in the room and helped her distinguish between “clean” pain (i.e., pain from the breakup) and “dirty” pain (i.e., pain associated with avoiding clean pain; see Hayes et al., 2012). Cynthia found this distinction helpful in processing her emotions related to the breakup.
The therapist often introduced one to two in-session experiential exercises per week to help Cynthia develop greater psychological flexibility with her anxiety and life. Exercises such as “Acceptance of Thoughts and Feelings” (Forsyth & Eifert, 2016) and “Dropping the Anchor” (Harris, 2019) offered Cynthia the opportunity to notice, name, and accept her internal experiences rather than avoid them.
Despite high motivation, Cynthia often struggled with practicing exercises outside of sessions. To address this discrepancy, the therapist and Cynthia worked to identify exercises that seemed most helpful while also discussing how she could make them “her own.” The therapist also noticed her own frustrations arising from this discrepancy and shared her observations with Cynthia. This conversation, in turn, prompted a shift in the spirit of the therapy sessions. Throughout this process, the therapist attempted to embody the spirit of Motivational Interviewing; an approach that seemed to weaken Cynthia’s resistance while supporting her self-efficacy and ability to choose to practice the skill building exercises on her own (Bundy, 2004). Cynthia responded more favorably to between session experiential exercises and enjoyed taking a creative approach to the work.
Creating Distance From Struggle
Once Cynthia developed skills in noticing and naming thoughts, emotions, and physical sensations, the focus shifted to undermining the believability of these experiences using cognitive defusion strategies. For example, Cynthia was asked to pick an anxious thought that she often “bought into” and practiced saying it aloud. The therapist then asked her to practice saying, “I notice I’m having the thought that…” followed by the distressing thought (i.e., “I’m having the thought that…”; Harris, 2019). Simple exercises like this allowed Cynthia to begin looking at thoughts rather than from them.
Thereafter, the therapist introduced Cynthia to the guided defusion exercise “Leaves on the Stream” (Hayes et al., 2012). Cynthia was asked to imagine sitting by a stream and placing all her thoughts one-by-one on a leaf and then watching it as a drift downstream and out of sight. Cynthia immediately noticed that her stream quickly filled with leaves, and she struggled with the urge to push the slow-moving leaves along. The therapist encouraged her to notice these judgments and urges and place them on their own leaves. Further, the therapist modeled a more defused stance in session with self-disclosure (e.g., “I notice myself having the thought this is a sticky subject”). Over time, Cynthia became more proficient at creating distance from difficult thoughts and feelings. She showed an increased ability to name her thoughts and catch repetitive thinking (e.g., “Yikes, that thought was pretty harsh!”). As her relationship with worry shifted, she continued to experience worrisome thoughts but was less distressed by them. Importantly, Cynthia’s committed action increased; she spent time with local friends and prepared meals for her father and stepmother, connecting with what was important to her despite her anxiety.
Being Kind to Oneself
During the weeks of uncertainty about her romantic relationship, Cynthia reported an uptick in self-critical thoughts (e.g., “I must not be good enough”). The therapist introduced her to self-compassion using guided exercises such as “Changing your Self-Critical Talk” (Neff, 2011). Cynthia readily identified her self-critical thoughts but struggled with “finding the good in [her]self” and became tearful describing her struggle. Her struggle with being kind to herself evoked discomfort and sadness in the therapist. Yet, both Cynthia and the therapist agreed that increasing self-compassion was a worthwhile therapy goal. Thus, instead of pivoting away from self-compassion work, an effort was made to find non-verbal self-compassion exercises. For instance, Cynthia practiced hugging herself (i.e., “Hugging Practice”; Neff, 2011) and found it easier to accept this gesture of kindness. She also began giving herself a squeeze or rub in session as an act of self-compassion. During this time, therapy also focused on strengthening Cynthia’s cognitive defusion, acceptance, and perspective-taking skills, which are closely aligned with self-compassion. Notably, for the first time since her move, Cynthia began drawing and painting again. She also continued to show sustained progress, and thus, treatment shifted to Phase 2, where the goals included identifying values and increasing mindful acceptance and perspective-taking skills when experiencing anxious thoughts and feelings (Eifert et al., 2009; Eifert & Forsyth, 2005).
Phase 2. Moving Non-Linearly Towards Valued Living, Sessions (10–19)
Acceptance of Anxiety
Cynthia’s gains in present-moment awareness and cognitive defusion was evident in her ability to notice and name worrisome and self-critical thoughts despite struggling with the mere presence of these thoughts. The therapist revisited acceptance, and during an in-session guided acceptance exercise, Cynthia described her anxiety as “nearly swallowing [her] whole.” Yet, she also noticed her ability to create space for her anxiety. The therapist validated her choice to continue the exercise despite feeling overwhelmed, and highlighted how choosing acceptance can be empowering. Cynthia and the therapist revisited this experience throughout treatment to reaffirm the rationale for acceptance.
Personifying the Mind
To further develop an accepting observer perspective, the therapist encouraged Cynthia to personify her self-critical mind, considering its personality, tone of voice, fashion sense, age, and so on. Cynthia drew the physical representation of her mind and brought it to the next session (see Image 1). As can be seen, her drawing depicted a large, black, reptile-like monster with spines, covering Cynthia in darkness and trying to consume her. She used cartoon faces to represent the more human-like parts of her mind that are trying to help her (see Image 1). Cynthia frequently referred to this “self-critical” part of her mind often and eventually felt compassion and understanding for it, stating “It’s just trying to protect me, in its own way.” Though this exercise is often used for cognitive defusion, her acceptance and compassion towards this part of her mind opened the door for radical self-acceptance and self-compassion later in therapy. Representation of Cynthia’s Mind by Cynthia. Note. Client permission was obtained to copy and use this artwork for academic purposes. In the image, a large, black reptile-like monster with spines is attempting to eat Cynthia in the bottom left portion of the drawing, covering her in a dark abyss, and human-like parts of her mind that make attempts to help her, are revealed to make up the monster.
Values Clarification and Valued Directions
Though some of Cynthia’s values were clear at intake, further clarification added depth and specificity (Eifert & Forsyth, 2005), helping to define workability and what successful treatment might look like. As part of this process Cynthia participated in a values card sort, which she later described as fun but challenging. She completed the card sort and identified two main value clusters: “the inner fun child within” (i.e., play nature, fun, imagination) and “serious values” (i.e., safety, compassion, partnership, feelings). While Cynthia wanted to move toward these values, she often felt “stuck” in her thoughts and feelings. To illustrate her ability to move in valued directions, the therapist introduced the “Passengers on the Bus” metaphor (Hayes et al., 2012). Cynthia imagined herself as the bus driver, filled with “passengers” representing her thoughts and feelings. Cynthia quickly identified her anxiety and thoughts as “rude passengers” trying to obstruct her path.
Cynthia found the “self-critical monster” to be the loudest on her bus, while noticing how the encouraging passengers were much quieter. Cynthia described isolating herself to “quiet down” the unruly passengers. The therapist noted that isolating behaviors kept her bus immobile. Soon after, Cynthia began dating, connecting with her values of partnership and fun, despite the noisy, doubtful, and self-critical passengers.
Phase 3. Staying Committed During the Onset of COVID-19 (Sessions 20–26)
The COVID-19 pandemic disrupted daily life and impacted the continuity and modality of treatment. To reduce transmission risk per CDC guidelines, the university training clinic – including other clinics around the globe (see Scharff et al., 2020) – transitioned all services to telehealth. This resulted in a one-week disruption of services during this period. During this time, Cynthia was given emergency contact information. Thereafter, she indicated being most comfortable continuing therapy by phone. This phase of treatment focused on identifying and increasing Cynthia’s valued behaviors while responding to barriers and challenges in a mindful and accepting way, including new stressors associated with the pandemic.
Phase 4. Accepting Self-Compassion (Sessions 27–35)
Cynthia adjusted to changes imposed by COVID-19, reconnected with her values, and felt settled in her new living situation and job. She then expressed a desire to revisit self-compassion interventions.
Compassion and Lovingkindness
The therapist led Cynthia in a Loving-Kindness (Metta) meditation (LKM), instructing her to direct phrases of compassion to herself, a person she admired, a neutral person, a difficult person, and lastly all living beings. Cynthia responded favorably but found it difficult to direct the phrases “May I be happy” and “May I be healthy” to herself. The difficult person that came to mind was her mother. Though she wanted her mother to be happy, she also felt the strain of their tumultuous relationship. To address Cynthia’s difficulties with certain phrases, the therapist assessed her reactions to a list of popular metta phrases. To personalize LKM and improve acceptability, Cynthia chose three metta phrases that resonated with her, as tailoring metta phrases it is widely recommended (Germer & Neff, 2019). Compared to the previous week, Cynthia had a “much easier” time with LKM, as she could use her personalized phrases for herself and others. She remarked that her phrases were “well fitted for where [she was] at, as well as where the world [was] at.” Thereafter, Cynthia approached everyday behaviors with more self-compassion (e.g., “caring for my garden is really how I care for myself”) and began practicing lovingkindness daily. Consequently, she reported feeling “more connected” to others “even with masks and social distancing.”
Addressing Unmet Needs
To promote self-acceptance and compassion and connect with Cynthia’s childhood wounds, the therapist led her through the “Child Guided Imagery” exercise (Walser & Westrup, 2007). In this exercise, Cynthia envisioned herself as a child, asking for a value or actionable value from each parent and her adult self. During the debrief, she became tearful, reporting that she fully engaged in and enjoyed the exercise, particularly the opportunity to comfort herself and heal old wounds. Cynthia recognized that her parents were unable to provide what “little her” needed (i.e., to be wanted, loved, and receive attention), as her mother was busy playing video games, and her father was always at the kitchen table watching the news. However, she readily accepted the “little her” and gave her “exactly what she needed.”
Phase 5. Preparing for Termination (Sessions 36–37)
Cynthia reflected on her treatment, noting her increased ability to notice and respond to her worry, greater confidence in navigating difficulties, and overall improved engagement in valued activities. Further, Cynthia reported that therapy was immensely helpful and looked forward to applying the skills she learned in daily life. Thus, for the first time in 10 years, Cynthia chose to end therapy due to observed gains. The therapist affirmed her progress highlighting growth in her career and relationships, and shared how enjoyable it was to work with her as her therapist.
Cynthia’s treatment was considered successful based on convergent evidence from quantitative (e.g., PSWQ & Q-LES-Q-SF) and qualitative assessments. Baseline quantitative scores were collected during the first session after intake and were administered weekly throughout treatment. Both Cynthia and the therapist observed clinically significant changes in quality of life and symptoms, which are described below.
Symptoms
Pre-to-post Treatment Self-Report Assessment Scores.
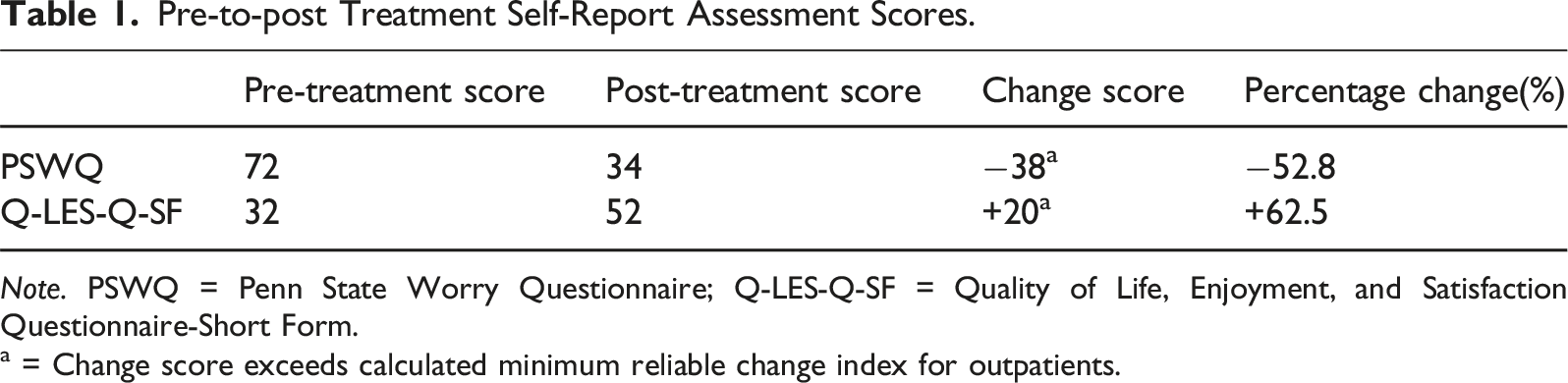
Note. PSWQ = Penn State Worry Questionnaire; Q-LES-Q-SF = Quality of Life, Enjoyment, and Satisfaction Questionnaire-Short Form.
a = Change score exceeds calculated minimum reliable change index for outpatients.
Quality of Life
Cynthia demonstrated clinically significant improvement in her quality of life. Cynthia’s Quality of Life Enjoyment and Satisfaction (Q-LES-Q-SF) scores increased by 28.57 across treatment (i.e., pre-treatment = 45.71% to post-treatment = 74.29%; see Table 1). This change score is significantly larger than the minimum clinically important Q-LES-Q (SF) change score (i.e., 6.80 points in those with GAD; Wyrwich et al., 2009), indicating clinically meaningful change. Though severity bands have not been established for the Q-LES-Q-SF, patients considered responders in psychiatric treatment typically score in the mid-60s or above (Wyrwich et al., 2009). Upon the last administration of the Q-LES-Q-SF at termination, Cynthia noted improvements in her feelings of connection to others, increased engagement in personally meaningful and important activities, and increased financial stability and job security.
8 Complicating Factors
Cynthia’s partner of two years unexpectedly ended their relationship during the second month of treatment, resulting in increased worry and decreased quality of life (see Figure 1). Cynthia reported symptoms of hopelessness, gastrointestinal difficulties, anhedonia, and decreased energy related to this loss. The therapist dedicated time in subsequent sessions to provide reflective listening to help support Cynthia’s exploration and processing of the breakup, while also moving forward with ongoing ACT interventions (e.g., present-moment awareness exercises and values clarification). Penn State Worry Questionnaire and Quality of Life, Enjoyment, and Satisfaction Questionnaire-Short Form Scores Scores Across Treatment. Note. Left Y-axis = PSWQ & Q-LES-Q-SF total score range; X-axis = session number. Client began taking 25 mg of Sertraline between weeks 6 & 7. Assessment reduced greatly reduced in frequency after session 17. Nine sessions passed between session 17 & 27, as well as between 27 & 37.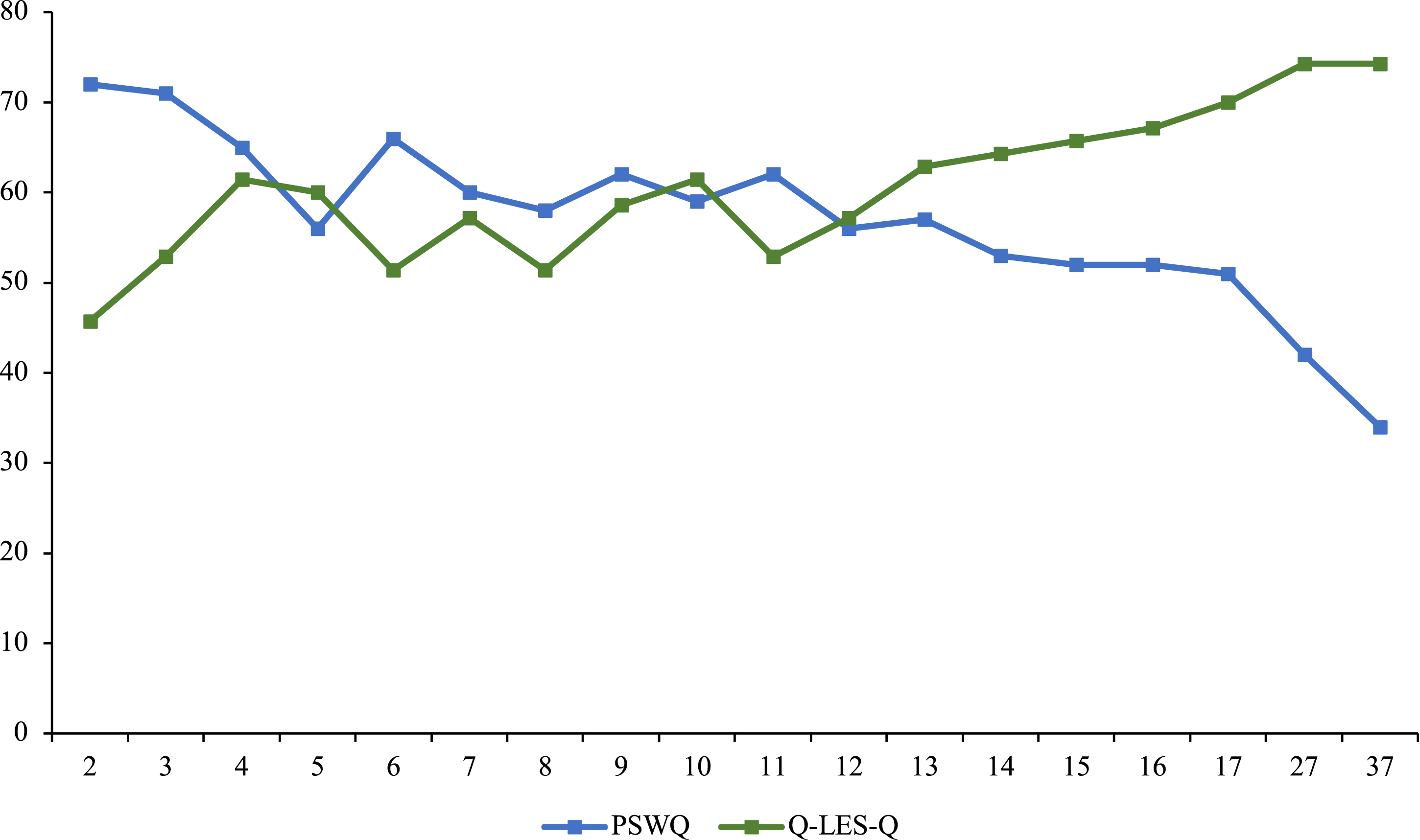
Additionally, Cynthia began receiving pharmacological treatment (i.e., Sertraline then Venlafaxine) prescribed by her primary care provider. She started low-dose Sertraline between session 6 and 7 and later switched to low-dose Venlafaxine between sessions 27 and 28. Pharmacological treatment likely contributed to symptom reduction over time, as SSRIs are effective in reducing GAD symptoms such as worry in the short-term (Wetherell et al., 2013). However, psychotherapy is necessary for sustained remission without requiring long-term pharmacotherapy (Wetherell et al., 2013). Though Cynthia’s symptoms began decreasing before starting medication, one cannot attribute her gains solely to ACT. Finally, Cynthia was encouraged to discuss her depression, particularly if it resurfaced as a concern during treatment. It was encouraging that her depression did not recur during the treatment, but we don’t know if that is because of the treatment or due to the timing of her depressive episodes.
9 Access and Barriers to Care
Cynthia’s financial instability did not hinder her access to care due to the treatment center’s sliding fee schedule based on household income. She also had reliable personal transportation and attended therapy sessions consistently. With the onset of the COVID-19 pandemic, the center transitioned to telehealth. As Cynthia lacked a reliable internet connection or a computer, it was decided to conduct sessions via telephone. Preliminary research suggests no significant differences between teletherapy (i.e., video and phone therapy) and in-person therapy for treating anxiety and related conditions, even when controlling for working alliance and client satisfaction scores (Krzyzaniak et al., 2021). Cynthia’s reported that the new format did not interfere with her progress.
10 Follow-Up
Long-term follow-up was not conducted in accordance with training clinic policies. At termination, Cynthia expressed that she greatly benefitted from therapy and looked forward to independently applying the skills she learned. The therapist reviewed Cynthia’s growth and encouraged her to reach out to the clinic if she needed therapy again.
11 Treatment Implications of the Case
This case illustrates a successful application of ACT that deviated from normative recommendations based on clinical trials regarding manual adherence and session limits (e.g., 7–12 weeks; Ferreira et al., 2022). Rather, all interventions were selected and adapted to meet Cynthia’s needs based on her treatment goals. The duration of treatment was affected, in part, by the COVID-19 pandemic. While 37 sessions exceed the average, this marked Cynthia’s first discontinuation of psychotherapy in 10 years. Thus, the present case may provide an example for other clinicians, both novice and seasoned, of a flexible and person-centered application of ACT.
Additionally, the present case adds to a growing literature supporting the effectiveness of ACT for individuals with stigmatized or marginalized identities. Though ACT clinical trials also support the approach with diverse populations, many of these trials are based on large samples from which nomothetic inferences are made based on aggregate data. Though important, such work does not readily translate to the unique needs of an individual client. Indeed, many mental health professionals rightly wonder where their client falls relative to the mean of those successfully treated within large clinical trials. Thus, there is a need for N-one-at-a-time case studies that offer insight into the application of various interventions in less controlled naturalistic mental health treatment contexts. Though Cynthia’s identity as a Queer Hispanic woman was not a focal point of treatment, the therapist strived to maintain awareness of their shared and differing identities. The therapist took a stance of cultural humility to provide affirming care in line with APA’s (2021) Guidelines for Psychological Practice with Sexual Minorities. Lastly, this case highlights the benefits of integrating self-compassion interventions within ACT (Neff & Tirch, 2013).
12 Recommendations to Clinicians and Students
We wish to conclude by offering several recommendations for clinicians, particularly those in training. Research suggests novice clinicians can successfully apply ACT (Kyllönen et al., 2018), and the present case supports that idea. Further, the present case underscores the importance of tailoring and re-introducing interventions based on patient feedback and preferences, particularly for clients with a history of avoidance.
Cultivating self-compassion can be challenging for clients with histories of trauma, abandonment, and high self-criticism. Thus, we recommend revisiting complementary processes—such as mindfulness, defusion, and values—to help clients create space for the successful introduction of self-compassion in treatment, even after initial resistance. Additionally, we recommend regular self-reflection on which processes are being targeted, as all ACT processes mutually influence one another. Accordingly, clients may show gains in non-targeted areas (e.g., cognitive defusion may weaken avoidance associated with thoughts, without targeting the avoidance directly).
We hope therapists in training not be discouraged if an intervention is not working as expected. Instead, we suggest viewing this as an opportunity to learn something about the client, you as the therapist, and perhaps the therapeutic relationship. How clients respond to interventions, including various ACT exercises, offers therapists useful information about where their clients are and areas that may require therapeutic attention. As such, even an ACT exercise that seems to fall flat can become a wonderful learning opportunity for therapists and clients alike.
Lastly, for cases with comorbid presentations, we recommend routine outcome monitoring and objective measures to track changes in psychological flexibility, stress, anxiety, and depression. For example, the Depression, Anxiety, and Stress 21 (DASS-21) scale would have been an appropriate measure to monitor Cynthia’s symptoms throughout treatment. Several values-based assessments are also available to adapt with various mental health concerns.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: John P. Forsyth is a co-author of Acceptance and Commitment Therapy for Anxiety Disorders: A Practitioner’s Treatment Guide to Using Mindfulness, Acceptance, and Values-Based Behavior Change Strategies, and The mindfulness and acceptance workbook for anxiety: A guide to breaking free from anxiety, phobias, and worry using acceptance and commitment therapy, and Anxiety Happens: 52 Ways to Find Peace of Mind but played no direct role in supervision or treatment of this case.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.