
Abstract
The objective was to determine multidrug-resistant organisms’ (MDROs) profile in diabetic foot ulcers (DFU), antibiotic resistance of MDROs, and to find the potential risk factors for infection with MDROs. In 157 patients with DFU admitted to Tianjin Metabolic Disease Hospital, China, from January 2011 to January 2012, microbiological specimens were taken on admission. The patients were divided into 2 groups according to the infection of MDROs. Potential risk factors for MDRO-positive specimens were examined using univariate and multivariate analyses. Seventy-eight MDRO strains were isolated from patients in the MDRO+ group, among which the top 3 were Staphylococcus aureus (16.7%), Enterobacter spp (16.7%), and Pseudomonas aeruginosa (15.4%). Most of the MDROs were resistant to at least 8 kinds of commonly used antibiotics. Gram-negative MDROs showed 23% to 50% resistance to third-generation cephalosporins. The resistant rates of Gram-positive MDROs to fluoroquinolone were more than 70%; penicillin and semisynthetic penicillin were 57% to 100% resistant. Previous hospitalization (odds ratio [OR] = 3.000; 95% confidence interval [CI] = 1.100-8.182; P = .032), previous duration of antibiotic therapy (OR = 1.078; 95% CI = 1.001-1.160; P = .046), ulcer type (OR = 7.185; 95% CI = 2.115-24.408; P = .002), ulcer size (OR = 1.403; 95% CI = 1.042-1.888; P = .026), and osteomyelitis (OR = 3.390; 95% CI = 1.178-9.756; P = .024) were associated with MDRO infection in patients with DFU.
Diabetic foot is a complex and challenging pathological state, characterized by high complexity of management, morbidity, and mortality. The prevalence of type 2 diabetes is increasing rapidly around the world, parallel to the increase in obesity, the reduction in physical activity, and dietary changes. It has been estimated that 366 million persons had diabetes (mostly type 2) in 2011, and the number has been projected to increase to 552 million by 2030. 1 It has been estimated that up to 25% of type 2 diabetes mellitus patients may develop diabetic foot ulcer (DFU) once in their life time. 2 Infection is a frequent (40% to 80%) and expensive complication of the ulcers. 3 In a 2-year study of 1666 patients with diabetes, Lavery and coworkers identified 199 infections in 151 individuals. 4 They found a 56-fold increase in risk of hospitalization and a 155-fold risk of amputation among those who developed foot infections. Another study reported amputation rates of 2.8%, 46%, and 77.7% in mild, moderate, and severe infections, respectively. 5
Proper management of these infections requires a multidisciplinary approach including surgery and revascularization when needed and an appropriate antibiotic selection, based on the culture and the antimicrobial susceptibility testing results.6,7 In addition, other methods to reflect the infection and the ulcers should be studied and applied; for example, Michail et al 8 reported the use of serum markers to monitor bone infection, and Löffler et al 9 reported the useful study of wound exudates. Several studies found methicillin-resistant Staphylococcus aureus (MRSA) in as much as 15% to 30% of diabetic wounds.6,10,11 Infection with MDROs may increase the duration of hospital stay, cost of management, and may cause additional morbidity and mortality.12-14 The emergence and spread of MDROs are considered to be causing a global crisis. 15 In recent years, the difficulty in controlling diabetic foot infection has been increasing along with the growing number of MDROs. The increasing prevalence of MDROs is disconcerting because infection with these organisms limits the choice of antibiotic treatment and may lead to a worse outcome. 16 Therefore, to analyze antibiotic resistance and the risk factors of DFU with MDROs is important for reducing and controlling MDRO infection and improving the outcomes of DFU.
This study aimed to investigate the MDROs’ profile, antibiotic resistance, and risk factors of DFU with MDROs so as to provide better guidance for the treatment of DFU.
Patients and Methods
Patients
All patients who were hospitalized in the Metabolic Disease Hospital of Tianjin Medical University from January 2011 to January 2012 with diabetes mellitus presenting with foot ulcer were included. Patients who had a life expectancy shorter than 1 year or had an ulcer above the ankle or lost to follow-up were excluded. The complete data from 157 patients enrolled in this retrospective study were used. According to the result of microbial identification and drug susceptibility, 118 patients with infected foot ulcers were classified into the MDRO+ group and MDRO− group. The study was approved by the institutional ethics committee, and all the patients gave their informed consent.
Clinical diagnosis of infection was based on the presence of at least 2 of the following criteria: local swelling or induration, erythema greater than 0.5 cm in any direction around the ulcer, local tenderness or pain, local increase of temperature, and purulent discharge. 17 The diagnosis of osteomyelitis in patients with foot ulcers is based on clinical examination and imaging. 18 Deep and large ulcers, ulcers with exposed bones, and those that do not heal after appropriate wound care and off-loading are more probable to be complicated by osteomyelitis. 18 Our flowchart for diagnosing diabetic foot osteomyelitis was based on a combination of probing-to-bone test and plain x-ray, which has been published elsewhere. 19 Ischemia was defined by an ankle brachial index < 0.9. Diabetic peripheral neuropathy was defined as the absence of perception of the Semmes-Weinstein monofilament (5.07, 10 g) at 2 of 10 standardized plantar sites on either foot or vibration sense <5/8 grade when a 128-Hz tuning fork (Rydel-Seiffer tuning fork) was used to check the vibration sense.20,21 Diabetic nephropathy was defined as microalbuminuria (≥30 mg/24 hours) or clinical albuminuria (≥300 mg/24 hours). Hypoproteinemia was defined as serum albumin <30 g/L. lower extremity arteriosclerosis obliterans was defined as ankle brachial index <0.9, history of intermittent claudication or ischemic rest pain, weakening or loss of palpation of foot pulses.
Evaluated Variables
In both groups, data recorded were the following: gender; age; antibiotic usage in 6 months prior to hospitalization; ulcer size (expressed in cm2; determined by multiplying the longest and widest diameters) and Wagner’s grade, 22 which assesses ulcer depth and the presence of osteomyelitis or gangrene using the following grades: grade 1 (partial/full thickness ulcer), grade 2 (probing to tendon or capsule), grade 3 (deep with osteitis), grade 4 (partial foot gangrene), and grade 5 (whole foot gangrene); ulcer type (ulcers were classified as neuropathic ulcers or ischemic ulcers, including pure ischemic ulcers and neuroischemic ulcers); osteomyelitis; complications or concomitant disease (which refer to the history or clinical records of the patient including coronary heart disease, cerebrovascular disease, diabetic nephropathy, diabetic retinopathy, diabetic peripheral neuropathy, lower extremity arteriosclerosis obliterans, dyslipidemia, anemia, hypoproteinemia); HbA1c (measured by a HLC-T OSOH 723 G7 automated glycated hemoglobin analyzer); and other biochemical data.
Microbiological Studies
Culture specimens were obtained at the time of admission. The area surrounding the wound was cleaned with povidone iodine solution. After the surface of the wound had been washed vigorously by saline, there was debridement of superficial exudates. Specimens were then obtained by scrapping the base of the ulcer or the deep portion of the wound edge with a sterile curette after cleaning the base of ulcer with a sterile swab stick. None of the specimens was obtained as superficial swabs. All specimens were transported by sterile containers and taken to the microbiology laboratory in 30 minutes. Bacteria were identified using the VITEK2 automatic bacterial analyzer (bioMérieux, France). The antimicrobial susceptibility of the bacterial isolates was determined using the disk diffusion method, according to the guidelines of the CLSI. 23 MDROs were defined according to an International Expert Proposal. 24 If MDROs and susceptible strains co-existed in the same patients, we classified these patients as the MDRO+ group.
Statistical Analysis
Quantitative variables were expressed as means ± SD whereas qualitative variables were expressed as percentages. All clinical characteristics were compared by the χ2 test or Fisher’s exact test for categorical variables. For continuous data, the Kolmogorov–Smirnov test was employed to determine whether the distribution of the acquired data was well modeled by a normal distribution. For nonparametric data, comparisons between the groups were performed using the Mann–Whitney test. By contrast, one-way ANOVA or Student’s t test was employed to parametric data. Multivariate analysis was performed using stepwise logistic regression. All statistical analyses were performed using SPSS 18.0 software. Two-sided P values were calculated, and a difference was considered statistically significant if P < .05.
Results
Of the 157 specimens of patients with diabetes with foot infections, 118 (75.2%) specimens were culture positive and the remaining 39 (24.8%) were negative. A total of seventy-eight MDROs were isolated from 64 patients, among which the top 3 were Staphylococcus aureus (16.7%), Enterobacter spp (16.7%), and Pseudomonas aeruginosa (15.4%). 68 sensitive strains were isolated from 54 patients. The isolation rate of MDROs was 53.4%: 72.2% Staphylococcus aureus were MRSA, and 75% Pseudomonas aeruginosa were MDROs (Table 1).
Isolated Bacteria and Resistance Distribution in Patients With Diabetic Foot Ulcer.
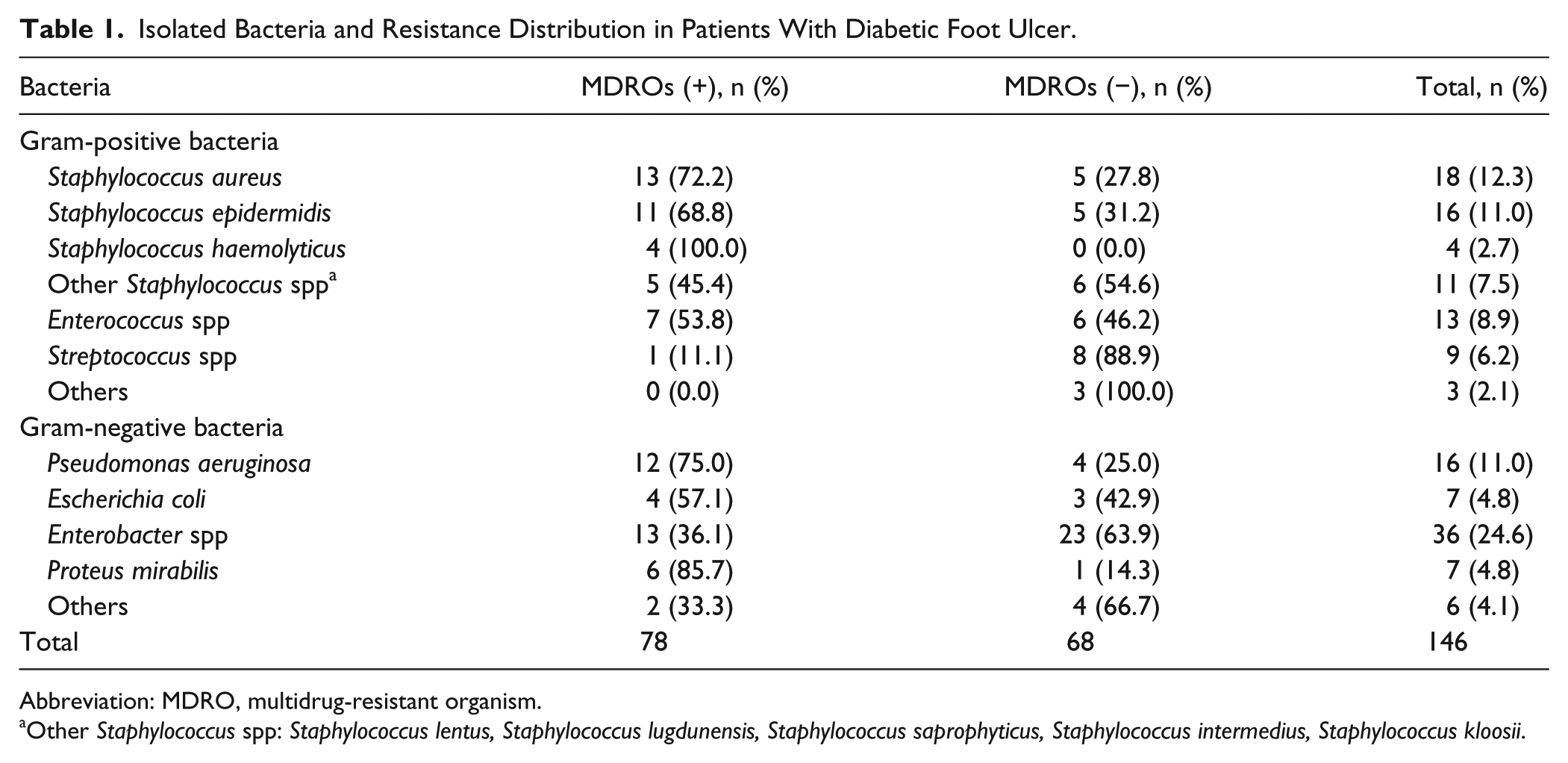
Abbreviation: MDRO, multidrug-resistant organism.
Other Staphylococcus spp: Staphylococcus lentus, Staphylococcus lugdunensis, Staphylococcus saprophyticus, Staphylococcus intermedius, Staphylococcus kloosii.
Gram-negative MDROs showed 23% to 50% resistance to third-generation cephalosporins, 66.7% to 100% to semisynthetic penicillins, and 46.2% to 75% to semisynthetic penicillins + β-lactamase inhibitors. However, they were susceptible to amikacin and fluoroquinolones, with the resistance rates being 0% to 25% and 15.4% to 25%, respectively. Major multidrug-resistant Gram-negative bacteria were still sensitive to imipenem. Enterobacter spp showed 15.4% resistance to imipenem, whereas for Pseudomonas aeruginosa it was 8.3% (Table 2).
Resistance Rate of Gram-Negative MDROs to Commonly Used Antimicrobial Drugs.
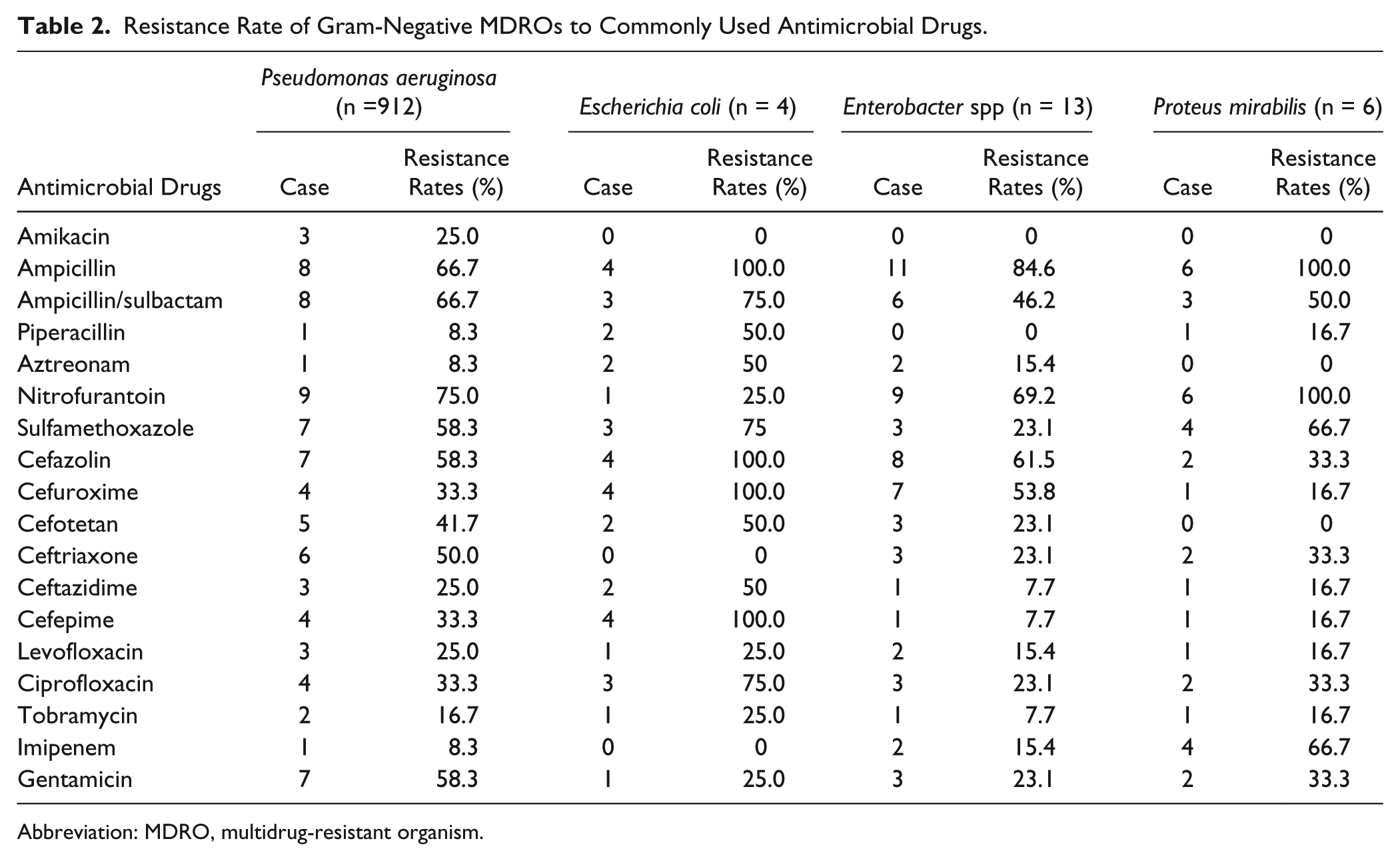
Abbreviation: MDRO, multidrug-resistant organism.
Gram-positive MDROs showed more than 70% resistance to quinolone, 57% to 100% to semisynthetic penicillin and penicillin, and 71.4% to 100% to macrolides. However, they were susceptible to amikacin and levofloxacin, with the resistance rates being 0% to 25% and 0% to 36.4%, respectively. Major multidrug-resistant Gram-positive bacteria were sensitive to vancomycin. The resistant rate of multidrug-resistant Enterococcus spp to vancomycin was 28.6%. Vancomycin-resistant Staphylococcus aureus was not found in our study (Table 3).
Resistance Rate of Gram-positive MDROs to Commonly Used Antimicrobial Drugs.
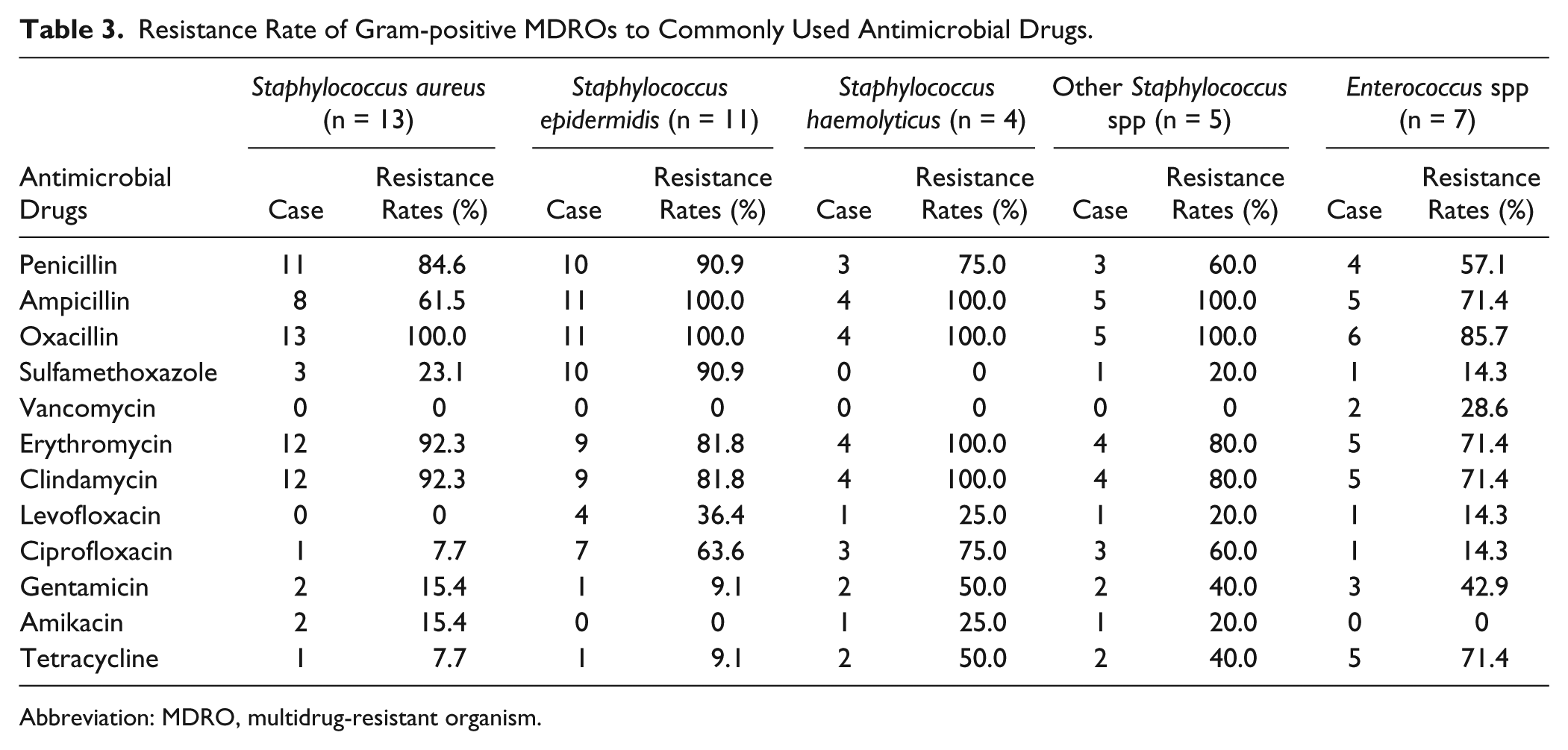
Abbreviation: MDRO, multidrug-resistant organism.
Demographic and clinical feature of patients from the MDRO+ group and the MDRO− group are summarized in Table 4. There were 105 males and 52 females in the present study. In both groups, the mean age was more than 60 years, and the duration of diabetes mellitus was more than 10 years. None of the patients had nephropathy severe enough to cause end-stage renal failure. Compared with the MDRO− group, the MDRO+ group had a longer duration of diabetes mellitus (P = .003), higher frequency of hospitalization (P = .000), longer duration of previous antibiotic therapy (P = .005), larger ulcer size (P = .007), more ischemic ulcers (P = .014), and osteomyelitis (P = .014); patients with osteomyelitis had longer duration of previous antibiotic therapy (20.5 ± 20.9 vs 12.6 ± 17.9), with the difference being significantly different (P = .004; (Table 4).
Univariate Analysis of MDRO Infection in PATIENTS with Diabetic Foot Ulcer.
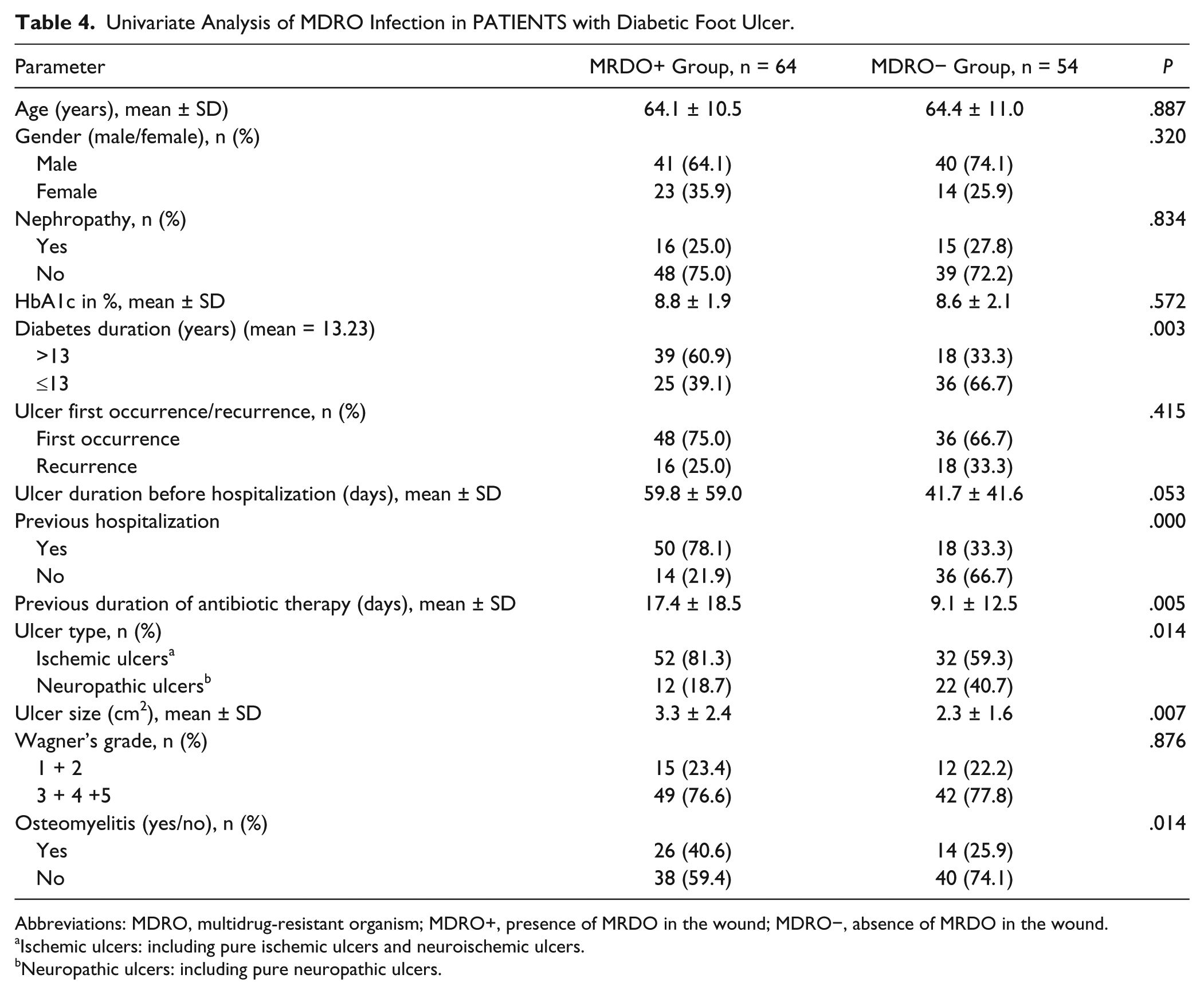
Abbreviations: MDRO, multidrug-resistant organism; MDRO+, presence of MRDO in the wound; MDRO−, absence of MRDO in the wound.
Ischemic ulcers: including pure ischemic ulcers and neuroischemic ulcers.
Neuropathic ulcers: including pure neuropathic ulcers.
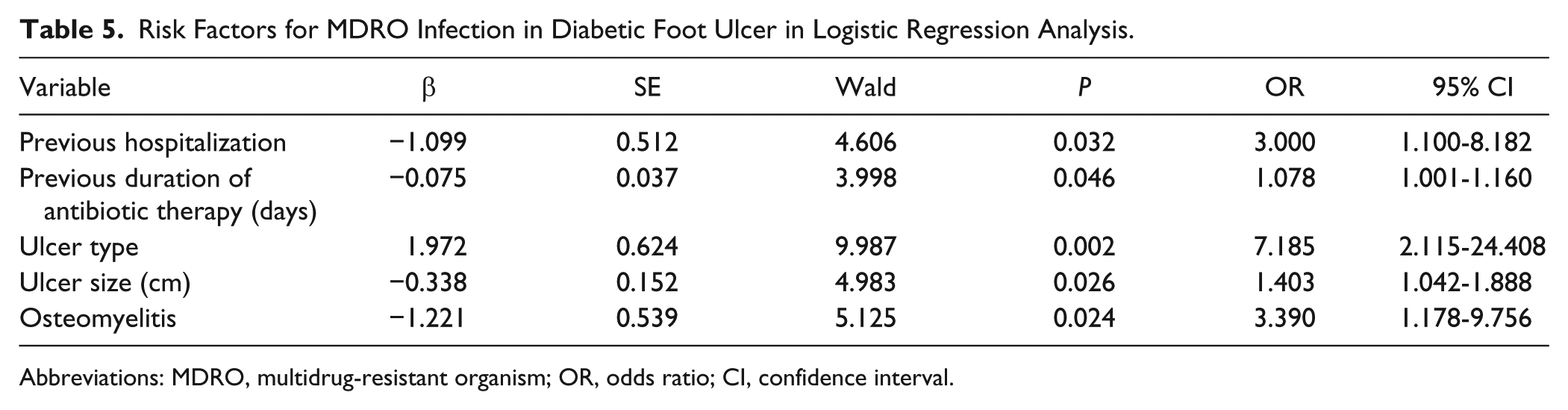
Logistic regression analysis demonstrated that previous hospitalization (odds ratio [OR] = 3.000; 95% confidence interval [CI] = 1.100-8.182; P = .032), previous duration of antibiotic therapy (OR = 1.078; 95% CI = 1.001-1.160; P = .046), ulcer type (OR = 7.185; 95% CI = 2.115-24.408; P = .002), ulcer size (OR = 1.403; 95% CI = 1.042-1.888; P = .026), and osteomyelitis (OR = 3.390; 95% CI = 1.178-9.756; P = .024) were associated with MDRO infection in patients with DFU (Table 5).
Risk Factors for MDRO Infection in Diabetic Foot Ulcer in Logistic Regression Analysis.
Abbreviations: MDRO, multidrug-resistant organism; OR, odds ratio; CI, confidence interval.
Discussion
MRSA was first identified in the United Kingdom in 1961. 25 Up to this day, a variety of MDROs have been prevalent. In recent years, nosocomial infection caused by MDROs has received attention. Once the DFU is infected by MDROs, they entail a sustained increase in hospitalization, risk of cutting the toe/limb, and associated increase in expenses. 26
The present study confirms that MDRO infection is extremely common in hospitalized patients with DFUs, similar to the results of Hartemann-Heurtier et al 12 and Kandemir et al. 27 In our study, 78 MDROs were isolated from 64 patients of the MDRO+ group. A total of 51.3% of MDROs were Gram-positive bacteria, among which the top 3 were Staphylococcus aureus, Staphylococcus epidermidis, Enterococcus spp; Gram-negative bacteria accounted for 48.7%, mainly including Enterobacter spp, Pseudomonas aeruginosa, Proteus mirabilis bacteria. These findings correlated well with related literature,7,28 and most of the MDROs were opportunistic pathogens. The prevalence of MRSA production was similar to previous studies.12,16,29
Gram-negative MDROs showed higher resistance to third-generation cephalosporins, semisynthetic penicillins, semisynthetic penicillins + β-lactamase inhibitors, with the rate being 23% to 100%. However, they were susceptible to amikacin, fluoroquinolones, and imipenem. This correlated partly with the findings of a study that was done in Mahatma Gandhi Medical College and Research Institute, Pondicherry, which showed that the members of Enterobacter spp were found to be susceptible to amikacin, piperacillin, tazobactam, and imipenem. 7 Mainly Gram-positive MDROs showed a high resistance rate to macrolides, penicillins, and semisynthetic penicillin, but high sensitivity to vancomycin. The antibiotic resistant rates of MRSA to penicillin and the macrolides was high (84.6% and 92.3%, respectively), which was consistent with the study of Heijer et al. 30 But MRSA strains had high sensitivity to amikacin and vancomycin. Raja also reported that vancomycin was effective against Gram-positive cocci. 29 Relatively newer antibiotics, such as tigecycline, daptomycin, linezolid, ceftobiprole, ertapenem, doripenem, and dalbavancin, can be chosen for multidrug-resistant strains, and some “forgotten” antibiotics, such as polymyxin and fosfomycin, can be considered for some cases of infections in patients with diabetes mellitus. 31 Continuous surveillance of resistant bacteria is necessary for providing the basis for empirical therapy and reducing the risk of complications.
Logistic regression analysis demonstrated that previous hospitalization (more frequent readmission with MDROs), previous duration of antibiotic therapy (longer with MDROs), ulcer type (more ischemic ulcers with MDROs), ulcer size (greater in cases of MDROs), and osteomyelitis (more frequent in patients with MDROs: 40% vs 26%) were independently associated with risk of MDRO infection. Long-term repeated use of a variety of antimicrobial agents would easily induce mutations of drug-resistant gene, resulting in multidrug resistance. In patients hospitalized several times for the same ulcers, in the course of repeated hospitalizations, owing to lapses in hygiene favoring cross-transmission, the risk of being directly infected by nosocomial MDROs is increased.32-35 Hartemann-Heurtier et al also reported that previous hospitalization within the last year for management of the same wound increased the risk of MDRO infection 3.8-fold. 12 However, data from a single center showed that prior antibacterial treatment and hospitalization were not associated with increased prevalence of MRSA in DFU, 36 which might reflect the high prevalence of MRSA in the community. 37 In the present study, MDRO included MRSA and other Gram-positive and Gram-negative multidrug-resistant bacterium, and MDRO infections were associated with prior hospitalization, which might be due to cross-transmission. Further studies using larger series of patients are needed to confirm these findings.
Continuous state of high blood sugar and nonenzymatic glycation of proteins, lipid metabolism disorders, high blood viscosity, hypercoagulablity, and many other factors in patients with diabetes led to lower extremity vascular endothelial cell dysfunction and made the patients prone to vascular lesions.38,39 Nerve ischemic wounds are characterized by microcirculation and microcirculation complications, which may lead to poor penetration of antibiotics into the lower limb tissues.40,41 Antibiotic concentrations measured in DFU could not reach optimal concentration, and poor bactericidal effect resulted in longer exposure times of antibiotics. 40 Longer duration and low concentrations of antibiotic in DFU would easily induce bacterial resistance. This study showed that ulcer types (ischemic ulcers) were independent risk factors for DFU with MDROs infection.
Jeffcoate and Lipsky 42 reported that in patients initially treated with antibiotics, the mean rate of eradication of osteomyelitis was over 60%. One of the problems of adopting a primarily nonsurgical treatment approach to osteomyelitis is the need for a prolonged antimicrobial treatment. For those patients in the Nottingham series who received outpatient treatment mainly with empirical oral broad-spectrum antibiotics (82%), the median length of treatment was 61 days. 43 Other studies have reported even more prolonged courses of antibiotic treatment. Valabhji et al showed that, in the United Kingdom, over 50% of patients received antibiotic treatment for 6 months or longer. 44 Use of prolonged courses of broad-spectrum antibiotics in this way undoubtedly increased the risk of the emergence of MDROs. In our study, patients with osteomyelitis exhibited usage of antibiotics for a longer time period before admission and higher infection rate of MDROs than patients with osteomyelitis. Logistic regression analysis showed that osteomyelitis was an independent risk factor for DFU with MDRO infection. Hartemann-Heurtier et al also reported that osteomyelitis increased the risk of MDRO infection 2.8-fold. 12 Therefore, patients with risk factors for MDROs should be closely monitored in the course of using antibiotics, thus reducing the probability of patients with diabetic foot ulcer being infected by MDROs, reducing the duration of hospital stay, reducing the cost of management, and reducing the additional morbidity and mortality.
Admittedly, our study has some limitations. One of the limitations of the present study was the use of curettage and not tissue cultures. Swab cultures have a very high sensitivity and NPV both for the confirmation of infection and for the identification of pathogens in patients with clinically infected diabetic foot ulcers, but their specificity is low. 45 Confirmation in larger patient series would be desirable. Other limitations of this study were its retrospective nature and the fact that we did not perform anaerobic cultures, although obligate anaerobes were rarely isolated from DFU. In spite of the above limitations, our findings highlight that certain risk factors for DFUs infected with MDROs.
In conclusion, MDROs had been prevalent in patients of diabetic foot ulcer and showed serious resistance to common antimicrobial agents. The frequency of hospitalization, previous duration of antibiotic therapy, ulcer type, ulcer size, and osteomyelitis were independent risk factors for DFU with MDROs. Hygiene measures, or isolation precautions in the event of admission of patients with such characteristics, should be implemented aggressively to prevent cross-transmission. Proper implementation of these measures, together with better management of antibiotics and continuous surveillance of resistant bacteria to provide the basis for empirical therapy, may prove capable of decreasing the incidence of MDRO infection of diabetic foot wounds.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Tianjin Natural Science Foundation of China (10JCZDJC19800), Tianjin Medical University Science Foundation (2008KY17), and Tianjin Health Bureau Technology Fund (09KZ87).