
Abstract
Integra dermal regeneration template has been well established in treating deep extensive burns, but there are very few cases reported of treating large full-thickness skin defects such as giant nevi. Apart from psychological and cosmetic burdens, the giant congenital nevus carries increased risk of malignant alteration. We present the case of a 9-year-old girl with a giant congenital nevus on her left lower leg. A total excision was done and she was successfully treated with Integra (LifeSciences Corp, Plainsboro, NJ). Three weeks later, a thin split-skin graft was applied over the neodermal skin layer. The takeoff was 91%. Protected with the silver wound dressing, the rest of the wound healed. A donor site morbidity was minimal, and the final result was excellent both in aesthetic and functional aspects.
Case Report
A 9-year-old girl was referred to our hospital for removal of a giant hairy nevus overlying the whole circumference of the right lower leg and foot. The same type of lesion, but smaller, was found on thorax as well. The size of the nevus on the leg was 16 × 15 × 1 cm. Preoperatively, the patient was protected with antibiotic prophylaxis—clindamycin. The lesion was completely excised and covered with 2 plates (20 × 25 cm) of Integra (LifeSciences Corp, Plainsboro, NJ). The superficial silicon layer was removed 3 weeks later and the matrix was found to be well-integrated with adequately implemented cellular elements and neovascularization. A 0.03-cm-thick autologous split-thickness skin graft was harvested from the left upper leg and placed over the matrix. A Vaseline gauze dressing was placed over, and the whole lower leg and foot were immobilized with a special hospital-made elastic bandage splint made of tiny wire sponge wrapped in cotton linen. After 3 weeks, 91% takeoff of the autologous split-thickness skin graft was achieved. A small defect was left behind above the lateral malleolus and the wound was treated with silver wound dressings for another 6 weeks. The wound healed completely afterwards. Physical therapy was started 10 days after wound grafting and the patient was followed-up. According to the physiatrist, 2 years and 8 months after the initial operation, the patient had 95% of the original function of lower leg and foot. She had some difficulties with the plantar side of the foot after extensive physical activities, with the epithelium peeling. The cosmetic and functional results are also rated excellent by the girl and her parents (see Figure 1-3).
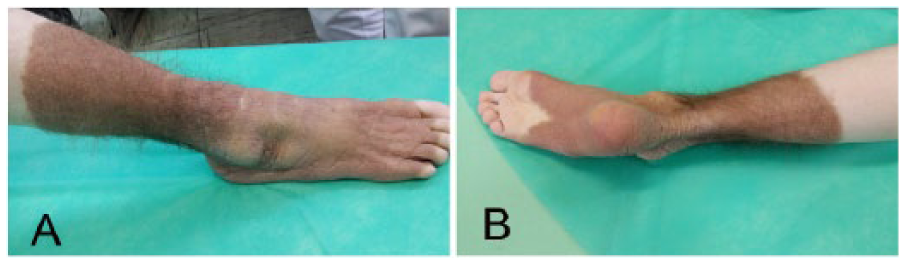
(A, B) Giant congenital nevus in a 9-year-old girl on her lower leg.

(A) The wound bed after total excision of the nevus. (B) The wound with Integra 2 weeks after excision. (C) A 0.03-cm autologous split-thickness skin graft placed over neodermis.
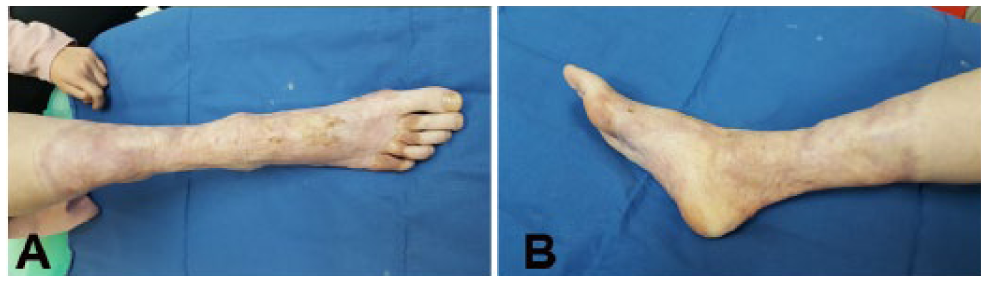
(A, B) Final result of the treatment 2 years and 8 months after the excision of the lesion.
Discussion
There has been only a few cases reported of treating giant congenital nevus (GCN) with Integra (LifeSciences Corp, Plainsboro, NJ). The largest study to date, which included 12 pediatric patients with GCN treated with the dermal substitute, was published by Schiestl et al. 1
Congenital nevi (CN) are present at birth with nevus cells originating from neural crest melanocytes. 2 The incidence of GCN is very low. It appears in only 1 in 200 000 children. 2 They differ from the acquired ones by melanocytic nevus cells distribution. The distribution of nevi cells in CN extends to deeper layers of dermis, subcutaneous tissue, and its structures. 3 They vary in size, and GCN is marked as nevus greater than 20 cm in largest diameter. 3
Indication for the treatment is based on psychological effect, cosmetic appearance, and functional reasons. According to Great Ormond Street Hospital studies, the CN can spontaneously lighten, and routine surgery did not demonstrate reduction of the risk of malignancy. There is even some evidence of surgery having adverse effect on nevus cells.4,5 This suggests that surgical treatment is necessary for cosmetic reason only. The precise magnitude of the risk of malignancy is disputable as well. Krengel et al found in 14 studies a risk of 0.7% of melanoma in CN, with risk increasing with size of nevus. 6 According to a systemic review by Watt et al, the risk of melanoma in patients with GCN is 2.8%. 7 The total lifetime risk is approximately 6.3%, which gives a 17-fold risk of melanoma compared to the general population. 8 Apart from melanoma, at least 5 cases of rhabdomyosarcoma arising in CN, measuring more than 12 cm in diameter, have been reported. 2 Malignant changes of giant nevus can occur at any age but occur most often in infants or toddlers, 9 and so the recommendation is for a total excision in early childhood.
Several options for the minimally invasive treatments have been reported such as dermabrasion, laser coagulation, and chemical peels. Superficial treatments remove pigmentation but repigmentation can occur. 10 Since minimally invasive treatments do not remove the deeper layers of nevus, they can also mask malignantly transformed nevus residue. Full surgical excision is the definitive treatment option for possible malignancy. Methods for covering large skin defect after excision include tissue expansion and skin grafting. Corcoran and Bauer suggest expanded transposition flap for better contour and scar position, less scar contracture, less tension, and a possibility to cover a large area. 11 Since we had a very large area to cover, a serial excision did not come into consideration because of the necessity of more than 2 operative procedures. Only skin grafting could create severe contractures and significant donor-site morbidity. The area was too large for tissue expander technique. Particular challenges presented were position of the defect above joints and strong tension forces in the lower extremity area as well.
Integra dermal regeneration template is a dermal regeneration system made in 2 layers. The dermal replacement layer is a porous matrix containing bovine collagen and shark glycosaminoglycan, a scaffold that prompts the body’s skin cells to migrate into the matrix bringing about neovascularization. Immunologic reaction to Integra is insignificant. 12 The superficial layer is an epidermal substitute created from silicone. 13 After 3 to 4 weeks, when neovascularization is achieved and the artificial dermis is being replaced by the patient’s dermis, the silicone layer is replaced with split-thickness skin graft. The wound bed prepared like this can takeoff of even the ultrathin skin grafts even when meshed. 14 It has been widely used in acute deep and extensive burn injuries, burn scar revisions, and the treatment of septic skin necrosis such as purpura fulminans and necrotizing fasciitis, 15 but there is not much experience in the treatment of GCN excisions published till now.
We decided to use Integra artificial dermal substitute followed by split-thickness grafting for several reasons. It provides a minimal number of surgical procedures (2-staged procedure) compared to other available surgical options, which is of great importance for the child. It reduces donor-site morbidity and allows harvesting a thinner split-thickness skin graft. When possible, vacuum-assisted closure system can also be used for better Integra fixation to the wound bed and for acceleration of neovascularization of the dermal layer. 16
Complications published by now are the following: shearing of the Integra, graft loss, silicone detachment, hematoma beneath the Integra, infection, incomplete takeoff, 13 and seroma. 17 We had an incomplete takeoff on the lateral malleolar region. This complication occurred in a place with high tension and possibly inadequate adherence to the wound bed for its natural uneven surface. The disadvantages of Integra are 2 operation procedures, recurrence of contraction seems to be higher than in full-thickness auto graft application, 18 and its high cost. 13 This remains to be further investigated.19,20
Giant congenital nevus present a significant burden to a child and its family weather as precancerous threat or a cosmetic defect. A total excision leaves large skin defects, which are a challenge to a plastic surgeon. Integra with autologous thin split-thickness skin grafting has been shown be a safe and efficient method of treating these big lesions with excellent cosmetic and functional final outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.