
Abstract
Diabetic foot ulcers (DFUs) are common, complex, costly complications, associated with frequent recurrences and increased morbidity and mortality. DFUs can be prevented and their healing can be mostly influenced by appropriately and aggressively managing any infection, but the role of antiseptic therapies in reducing healing time lacks sufficient evidence. Several therapeutic interventions have been developed based on the principles of photomedicine to overcome the issue of poor drug circulation in infected areas, with the aim of killing microbial agents while leaving the surrounding host cells unharmed. Such techniques use absorption of photons by specific chromophores. Among these, RLP068 is a tetracationic Zn(II) phthalocyanine derivative activated by exposure to red light, used as a topical treatment for superficial bacterial and fungal infections. The photoactivation of RLP068 results in the production of singlet oxygen and other reactive oxygen species, able to affect a range of cellular targets, including cell membrane and/or wall, cytoplasm, and cellular components, resulting in a rapid, broad range, bactericidal and fungicidal effect. The phase IIa study showed that photoactivated RPL068 is capable of inducing a dose-dependent reduction in total and pathogen microbial load in infected diabetic foot ulcers. In this article, a case series of 22 DFU treated with photoactivated RLP068 at 5 different centers in Italy is presented. Considering microbial agents reduction, ulcer healing facilitation, healing rate (9 DFUs out of 22), and amputation rate (only 1 case over 22), the decrease in the cost of DFU seems to be a point in favor of RLP068 and its cost-effectiveness.
Foot ulcers and other lower limb complications due to diabetes are common, complex, costly, and associated with increased morbidity and mortality.1-3
Unfortunately, even after the resolution of a foot ulcer, recurrence is common. Recurrence is about 40% in the first year, 60% in 3 years, and at least 65% within 5 years. 1
According to a recent study that compared the cost of diabetic foot in 5 European countries (France, Spain, Italy, Germany, and the United Kingdom), the total cost of amputation ranged from US$15 046 in 2001 to US$38 621 in 2005. All countries incur a heavy cost from diabetic foot and its complications, highlighting an unmet need for the identification of cost-cutting strategies, as diabetic foot costs more than major cardiac diseases.4,5
Diabetic foot ulcers may, therefore, be prevented and their healing can be favored appropriately by paying attention to 4 factors: tight glycemic control, adequate arterial inflow to the removal from wound and its margins and, mostly, appropriate and aggressive management of any infection. 6
Treatment of chronic wounds is based on the simple principles of eliminating infection, using dressings to maintain a moist wound bed and to absorb exudate, offloading high pressure from the wound bed, and using debridement to accelerate endogenous healing and facilitate the effectiveness of topically applied substances, ensure adequate perfusion. 7
Diabetic ulcer healing is often thwarted by microbial infection. A recent survey on diabetic foot among Italian experts highlighted that the scarce evidence available on the role of antiseptic therapies in reducing healing time hampered the achievement of a consensus on the topic. 8
Widespread and increasing bacterial antibiotic resistance and limited penetration of drugs in infected areas (aggravated by concurrent ischemia) caused the need to find alternative therapies.
Several therapeutic interventions have been developed based on the principle of photomedicine to overcome the issue of poor drug circulation in infected areas, with the aim of killing microbial agents while leaving the surrounding host cells unharmed. 9
Such techniques use absorption of photons by specific chromophores, and among these, photodynamic therapy is a novel strategy. RLP068 (VULNOFAST plus, Molteni Therapeutics SRL, Italy) is a tetracationic Zn(II) phthalocyanine derivative activated by exposure to red light, developed as a topical treatment for superficial bacterial and fungal infections. Its mechanism of action is based on the photoactivation of RLP068, which results in the production of singlet oxygen and other reactive oxygen species (ROS), able to affect a range of cellular targets, including cell membrane and/or wall, cytoplasm, and cellular components, resulting in a rapid, broad range, bactericidal and fungicidal effect.
The phase IIa study showed that photoactivated RPL068 is capable of inducing a dose-dependent reduction in total and pathogen microbial load in infected diabetic foot ulcers. The trial confirmed in the clinical setting safety and effectiveness found with animal models, with a negligible systemic absorption through the wound and a dose-dependent reduction in total and pathogen microbial load. The effect of the drug vanished over the time, suggesting a recommended administration every other day or 3 times a week. 10
A case series of 22 DFUs treated with photoactivated RLP068 at 5 different centers in Italy is presented here.
Materials and Methods
Design and Population
The purpose of this article is to present the clinical experience of 5 different DFU centers in Italy (Abano Terme, Milano, Monfalcone, Pistoia, and Pordenone) with photoactivated RLP068 during a 1-year period (from December 2018 to November 2019). Because of the retrospective nature of data collection, a board approval was not required, since individual patient consent was obtained for all the procedures.
Patients were selected on the following criteria: (1) presence of a chronic DFU and (2) photoactivated RLP068 treatment. Data from 22 patients (15 males, 7 females) were analyzed. Age ranged from 53 and 90 years (mean = 69.2, median = 67), while years since diabetes diagnosis ranged from 2 to 44 years (mean = 19.2, median = 19). A total of 21 patients were diagnosed also with peripheral neuropathy, 14 with peripheral arterial disease, but without critical limb ischemia, 8 with retinopathy, and 7 with ischemic heart disease. One patient was included for 2 different wounds. Main characteristics of patients at baseline are shown in Table 1.
Main Characteristics of Patients at Baseline.
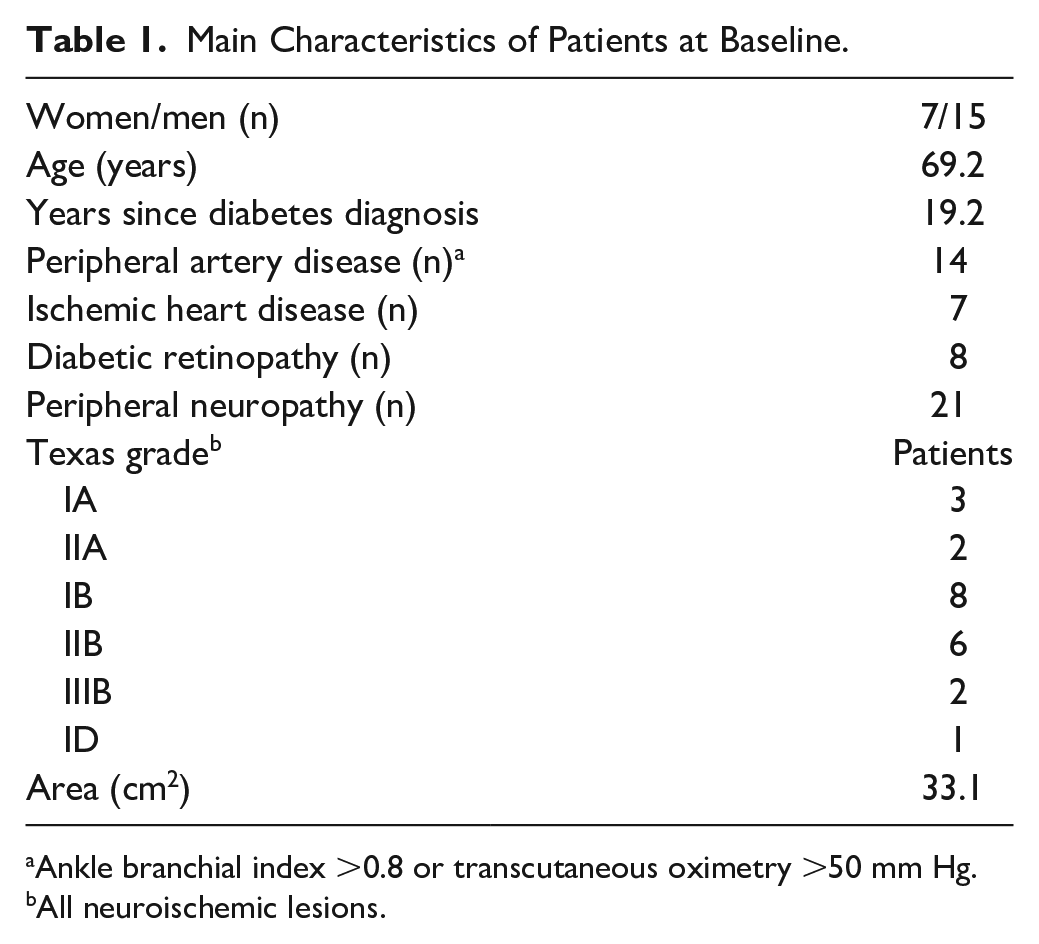
Ankle branchial index >0.8 or transcutaneous oximetry >50 mm Hg.
All neuroischemic lesions.
Wound Evaluation
Each ulcer was assessed at the initial visit (T0), intermediate visits (T1, T2), and final visit (T final).
Wound Treatment
All chronic DFUs were treated with RLP068 (VULNOFAST plus, Molteni Therapeutics) twice a week according to the manufacturer’s instructions. Thirty minutes after the application, the ulcer was illuminated for 8 minutes by a portable LED light device (VULNOLIGHT, Molteni Therapeutics) with a red light at 630 nm wavelength, providing a total energy of 60 J/cm2. The total number of applications ranged from 4 to 16 times (mean = 7.5, median = 7), depending on clinicians’ choice. Antibiotic therapy was added when needed (N = 10) based on bacteriological analysis and bacterial load results (Table 1). A silver-based dressing and a foam with TLC-NOSF (Technology Lipido-Colloid combined with Nano-Oligo Saccharide Factor) matrix dressing were also used in 2 cases each, and hydrogel-based dressing was used for one patient.
Results
At baseline assessment (T0), University of Texas classification for DFU (N = 22) resulted in the following: IA for 3 ulcers, IIA for 2, IB for 8, IIB for 6, IIIB for 2, and ID in one case. Wound area ranged from 0.91 to 200 cm2 (mean = 33.1, median = 4.5 cm2), with wound depth ranging from 0.1 to 1 cm (mean = 0.4, median = 0.25, data available for 20 wounds). Bacteriological analysis resulted positive in 19 lesions, with variable bacterial load. The germs detected at T0 are shown in Table 2.
Microbial Agents Isolated on Lesions at Initial (T0) and Final Assessment.
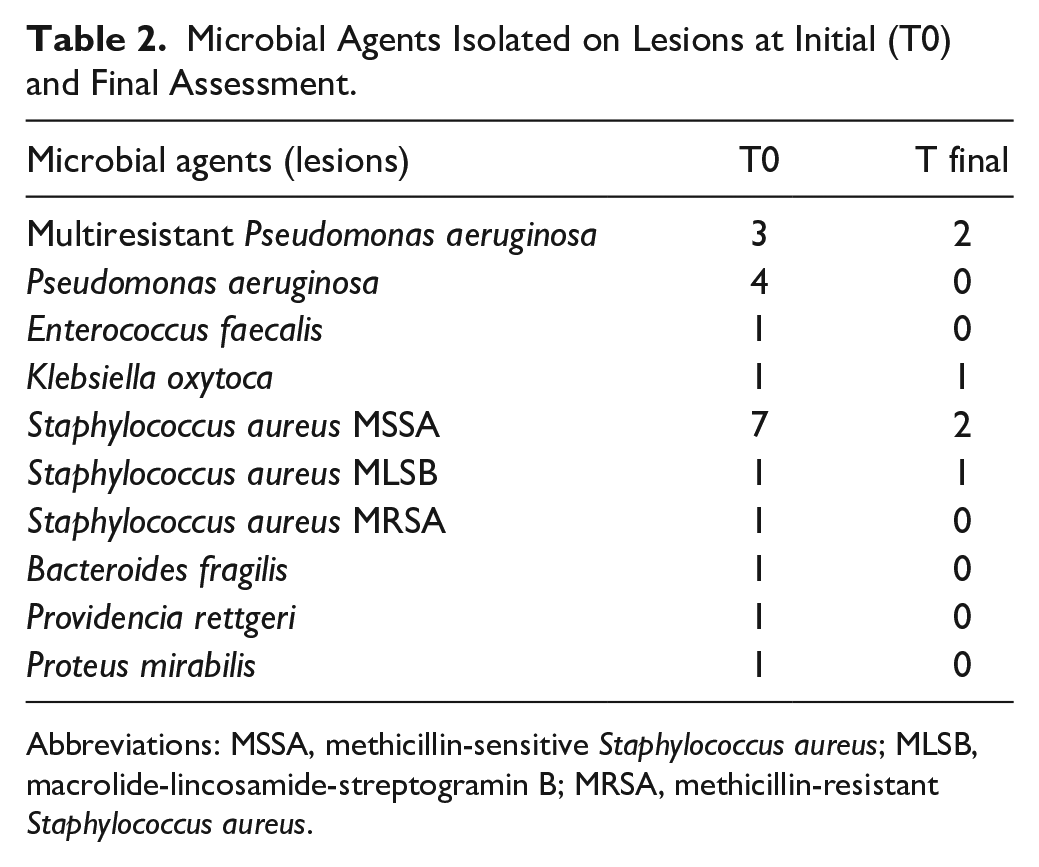
Abbreviations: MSSA, methicillin-sensitive Staphylococcus aureus; MLSB, macrolide-lincosamide-streptogramin B; MRSA, methicillin-resistant Staphylococcus aureus.
At an intermediate assessment (T1, from 4 to 46 days after T0, mean = 13.9, median = 7.5 days), University of Texas classification for DFU (N = 18) resulted in the following: IA for 6 ulcers, IIA for 5, IB for 4, IIB for 2, and IIIB for 1. Wound area lowered to 0.12 to 138 cm2 (mean = 27.1, median = 4.5 cm2), with wound depth ranging from 0.1 to 1 cm (mean = 0.3, median = 0.2, data available for 20 wounds). Bacteriological analysis resulted positive in 4 lesions (Table 1).
At another intermediate assessment (T2, from 10 to 277 days after T0, mean = 60.6, median = 17.0 days), healing was observed in 3 cases. University of Texas classification for DFU (N = 14) resulted in the following: IA for 3 ulcers, IIA for 4, IB for 3, IIB for 3, and IIIB for 1. Wound area was found from 0.5 to 90 cm2 (mean = 9.4, median = 3.5 cm2), while no changes were observed in wound depth. Bacteriological analysis resulted positive in 2 lesions (multidrug resistant Pseudomonas aeruginosa).
At final assessment (T final, 15-221 days, mean = 69.1, median = 34.0), healing was reported for another 4 lesions. University of Texas classification for DFU (N = 14) resulted in the following: IA for 6 ulcers, IIA for 5, IIB for 2, and IIIB for 1. Wound area for nonhealed ulcers ranged from 0.5 to 70 cm2 (mean = 12.5, median = 3.9 cm2). Bacteriological analysis resulted positive in 7 lesions. The germs detected at T final are shown in Table 2.
Discussion
Basic epidemiological data of the cases presented here seem in good general agreement with the global prevalence data.2,3
Of the 22 reported cases, healing was observed for 9 DFUs (40%) and amputation was required in only one case. The use of antibiotic or other treatment was not observed to influence ulcers healing.
In general, the area of the wound remained stable or decreased in all cases with only one exception, which, nevertheless, was found to decrease at the following control. At T1, the area of 13 ulcers presented a lower area and in 3 cases area reduction exceeded 50%. Another 2 ulcers decreased in diameter of at least 50% at final control.
So, at the final visit, 68% of the patients was healed or their ulcer area was reduced by >50%.
Moreover, there is a reduction of infected lesions.
RLP068 is a tetracationic Zn(II) phthalocyanine derivative activated by exposure to red light, developed as a topical treatment for superficial bacterial and fungal infections. Following photoactivation of RLP068, ROS are produced and endowed with a bactericidal and fungicidal effect.9,10
A phase II randomized, double-blind, parallel series, and placebo-controlled trial demonstrated the efficacy of photodynamic therapy with RLP068 on total and pathogen microbial load of diabetic ulcers. Our data, with all the limitations given by a case series, seem to be in line with the trial results. In particular, there is a trend toward a reduction in extent, depth, and infection, although the sample size is too small to perform a formal statistical analysis. The decrement in the area of the ulcer observed in most of cases already at T1, irrespective of the ulcer characteristics, might be correlated to the variability of cellular targets and to the rapidity of action of the ROS produced by photoactivated RLP068.
Ulcer healing takes weeks or months and one third of ulcers never heal with amputation as consequence, 11 so photoactivated RLP068 appears to positively influence ulcer healing.
No safety issues emerged from the report of adverse events.
We can recognize some limitations of the study: the reduced size of the sample, which could induce the need for further randomized, case-control prospective studies; the increase of the costs of lesions’ treatment, due to the need for suitable outpatient spaces to apply the therapy and the duration of the treatment.
Regarding the costs, we can argue that they are balanced by the reduction of the healing time of chronic ulcers that would otherwise take longer times with greater expenditure of economic and noneconomic resources.
Last, we can consider as a positive aspect the fact that this treatment allows to heal parts of such chronically infected ulcerative lesions that have already been treated unsuccessfully with all the available methods (local and systemic) for the eradication of the infections.
Conclusions
A standardized therapy aimed at the reduction of bacterial load in diabetic foot ulcer is currently a strong unmet need, considering that the frequency of persistent diabetic foot ulcers and the lack of consensus on the role of antiseptic therapies in reducing healing time among the experts.
Thanks to the data observed in this case series, it is possible to conclude the following:
Photoactivated RLP068 is demonstrated to reduce microbial agents, facilitate ulcer healing, and seems to be effective and safe in the management of DFU.
The use of photodynamic therapy is valuable for the antimicrobial treatment of patients already receiving several drugs, with ulcers infected by drug-resistant bacteria, or in addition to other therapies in serious cases.
Considering the healing rate (9 DFUs out of 22) and amputation rate (only 1 case over 22), the decrease in the cost of DFU seems to be a point in favor of RLP068 and its cost-effectiveness and its capability of become a cost-cutting strategy should be further studied.
Considering the importance of a multidisciplinary approach in achieving a good rate of limb salvage in people with DFU,12,13 management optimization should also be further studied.
Footnotes
Acknowledgements
Thanks are due to Enrica Barro, Marino Bruseghin, Antonella Quarantiello, Elisabetta Salutini, Secondina Viti, Giorgio Zanette (Medical collaborators), Tiziana Bruschi, Lisetta Butelli, Silvana Carlucci, Raffaele Corte, Raffaella Donzelli, Manola Gioffredi, Cinzia Perini, Rossella Picciafuochi, Alessandra Seregni, Silvana Azzano (Nursing collaborators), Valentina La Rocca, Beatrice Macchi, Michela Pinfi (Podiatrists), and to Sinergie Edizioni Scientifiche (project coordination and writing and editing contribution).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The publication was supported by an unrestricted grant from Molteni Farmaceutici.