
Abstract
Since infectious foot ulcers represent one of the major causes of lower-limb amputation, it calls for an appropriate action for early detection and sufficient treatment of diabetic foot infection (DFI). The present study aimed at investigating the bacterial epidemiology and antimicrobial resistance (AMR) patterns of DFIs in Iran. We have conducted a systematic search in PubMed, Embase, Web of Science, Scopus, Google Scholar, and Scientific Information Database to identify all articles reporting the proportion of different kinds of bacteria isolated from Iranian DFI samples. Quality was assessed using Joanna Briggs Institute tool. A pooled estimate of proportion with a corresponding 95% confidence interval (95% CI) was calculated using the random effect method. Fifteen studies were eligible, of which 1970 bacterial isolates were obtained from 1316 patients. The most predominant isolates recovered from DFIs was Staphylococcus aureus with a pooled proportion of 24.29% (95% CI: 20.25%, 28.57%) from which 55% (95% CI: 38%, 72%) were methicillin-resistant S. aureus (MRSA). Among Gram-negative strains, Escherichia coli had the highest proportion (17.19%; 95% CI: 13.96%, 20.68%) followed by Pseudomonas aeruginosa, 7.54% (95% CI: 4.56%, 11.14%). The highest pooled estimates of resistance against cotrimoxazole and ciprofloxacin were found in S. aureus 66% (95% CI: 48%, 82%) and E coli isolates 68% (95% CI: 51%, 84%), respectively. Our study revealed that AMR is at a high level in Iran and clinicians should be aware of bacterial resistance patterns to prescribe appropriate antibiotic regimens.
The prevalence of diabetes was 10.3% in 2016 in Iran. Considering the high prevalence of people with overweight (60.5%), obesity (25%), and physical inactivity (32%), this number is expected to rise greatly.1,2 Foot ulcers are one of the most feared complications that patients with diabetes might face. Approximately 15% to 25% of patients with diabetes develop foot ulcers. Diabetic feet contribute to the majority of nontraumatic lower-limb amputations 3 and impose a considerable psychological and economical burden on both the individuals and society. 4 This burden can be decreased considerably with early detection and appropriate treatment of diabetic foot infections (DFIs). Clinicians need to be aware of the microorganisms involved in DFI pathogenesis and their antimicrobial resistance (AMR) patterns to efficiently prescribe an appropriate antibiotic regimen. 5 Currently, the primary treatment of DFIs is often empirical and based on existing clinical guidelines, which usually are originated from western countries. That said, knowing the prevalence of the pathogenic microorganisms and their AMR patterns in a local area is crucial to have the best empiric antibiotics for its residents.5,6
DFIs can be monomicrobial or polymicrobial. They are caused by aerobic Gram-positive cocci (eg, Staphylococcus aureus, Staphylococcus epidermidis, and Enterococcus spp.), Gram-negative bacilli (eg, Escherichia coli, Pseudomonas spp., Klebsiella spp., and Proteus spp.), and anaerobes (eg, Bacteroides spp., Peptostreptococcus spp., Fusobacterium spp., and Clostridium spp.). 7 However, the prevalence of common microorganisms isolated from DFIs varies noticeably among different studies conducted in different parts of the world.5,6 Furthermore, AMR patterns might be different based on geographic differences. Therefore, the unique characteristics of each region should be taken into account to have the most appropriate and efficient antibiotic regimen. 6
The discrepancy observed in the prevalence of DFIs' bacteria and its AMR patterns in various regions of the world, and the fact that most existing guidelines come from developed countries,5,6 prompted us to evaluate these factors in a nationwide frame. This systematic review and meta-analysis aimed to investigate the prevalence of the common pathogenic bacteria isolated from DFIs in Iran and their AMR patterns.
Material and Methods
This systematic review and meta-analysis were conducted in accordance with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines, 8 and a PRISMA checklist was completed. The study protocol has been registered at the Isfahan University of Medical Sciences with the national ethics code of IR.MUI.MED.REC.1399.239
On August 10, 2019, we conducted a thorough search in PubMed, Embase, Web of Science, and Scopus for the following terms: microb*, bacter*, diabetic foot, diabetic feet, and Iran. The English search strategy includes the following keywords: (microbiology OR bacteriology OR bacteria OR microb* OR bacter*) AND (“diabetic foot” OR “diabetic feet”) AND (Iran). Google Scholar and Scientific Information Database, an Iranian database, were also searched using both English and Persian keywords.
This systematic review has included original Iranian Laboratory-based cross-sectional studies published in English or Persian, which had evaluated the bacteriology of DFIs and reported the prevalence of individual isolates recovered from them. We excluded review articles, original articles with inadequate or vague results, and studies that used animal infection samples.
Two independent reviewers (SSE and AT) assessed the titles and abstracts of retrieved articles and excluded irrelevant records. A third reviewer was consulted in cases of disagreement. Then, the full-text of the remaining articles was screened. Studies meeting the inclusion criteria were considered to be eligible and were included in the present study. One reviewer extracted the data, and a second reviewer checked their accuracy. The following data were extracted: city, language, the study period, the number of patients, the number of DFI samples, the number of positive cultures, the number of isolates, the sampling method, and the related outcomes.
The quality of selected studies was evaluated using standard critical appraisal tools prepared by the Joanna Briggs Institute (JBI) for prevalence studies. 9 The purpose of this appraisal is to assess the methodological quality of a study and to determine the extent to which a study has addressed the possibility of bias in its design, conduct, and analysis. The JBI critical appraisal checklist contains 9 questions (Q1-Q9). The scores given by the 2 authors were used to make the final decision. A third author was consulted in the case of disagreement between the 2 authors' appraisal opinions. Studies with 5 or more “YES” responses (55% YES response rate) were included in the meta-analysis.
The following data were extracted from each included study:
The number of bacterial isolates recovered from infected diabetic foot ulcers. The AMR patterns of clinically relevant bacterial isolates.
Only bacterial isolates and antimicrobial agents that were mentioned in at least 3 or more studies were included in the systematic review and meta-analysis.
The point estimates of the proportion of each bacterium and its 95% confidence interval (95% CI) were estimated for each study. To estimate the pooled proportions, we used Metaprop, a statistical procedure in STATA (version 14). 10 A random-effects model including the Freeman–Tukey double arcsine transformation of the proportions was used to stabilize variance and reduce the effect of the between-study heterogeneity. The 95% CIs were computed around the study-specific and pooled proportion of each bacterium based on the score test statistic. Between-study heterogeneity was evaluated with Cochran's Q-test 11 and heterogeneity across studies was assessed with the I2 measure. 12
Publication bias was tested by Egger's test, Begg's test, and funnel plot. Subgroup analysis and meta-regression were also conducted based on the nature of the sampling methods (swabbing and other methods such as biopsy and needle aspiration) and types of isolated bacteria (gram positives or gram negatives) to find potential sources of heterogeneity. P values <.05 were considered statistically significant.
Results
Study Selection
A comprehensive literature search was carried out in electronic databases including PubMed, Embase, Web of Science, Scopus, and SID, and 54 articles were retrieved. After removing duplicates, 11 articles were excluded in the first scan of titles and abstracts. In assessing the remaining full texts for eligible studies, we excluded 8 more articles. Finally, 15 studies were included in this systematic review and meta-analysis. The study selection process is detailed in Figure 1.
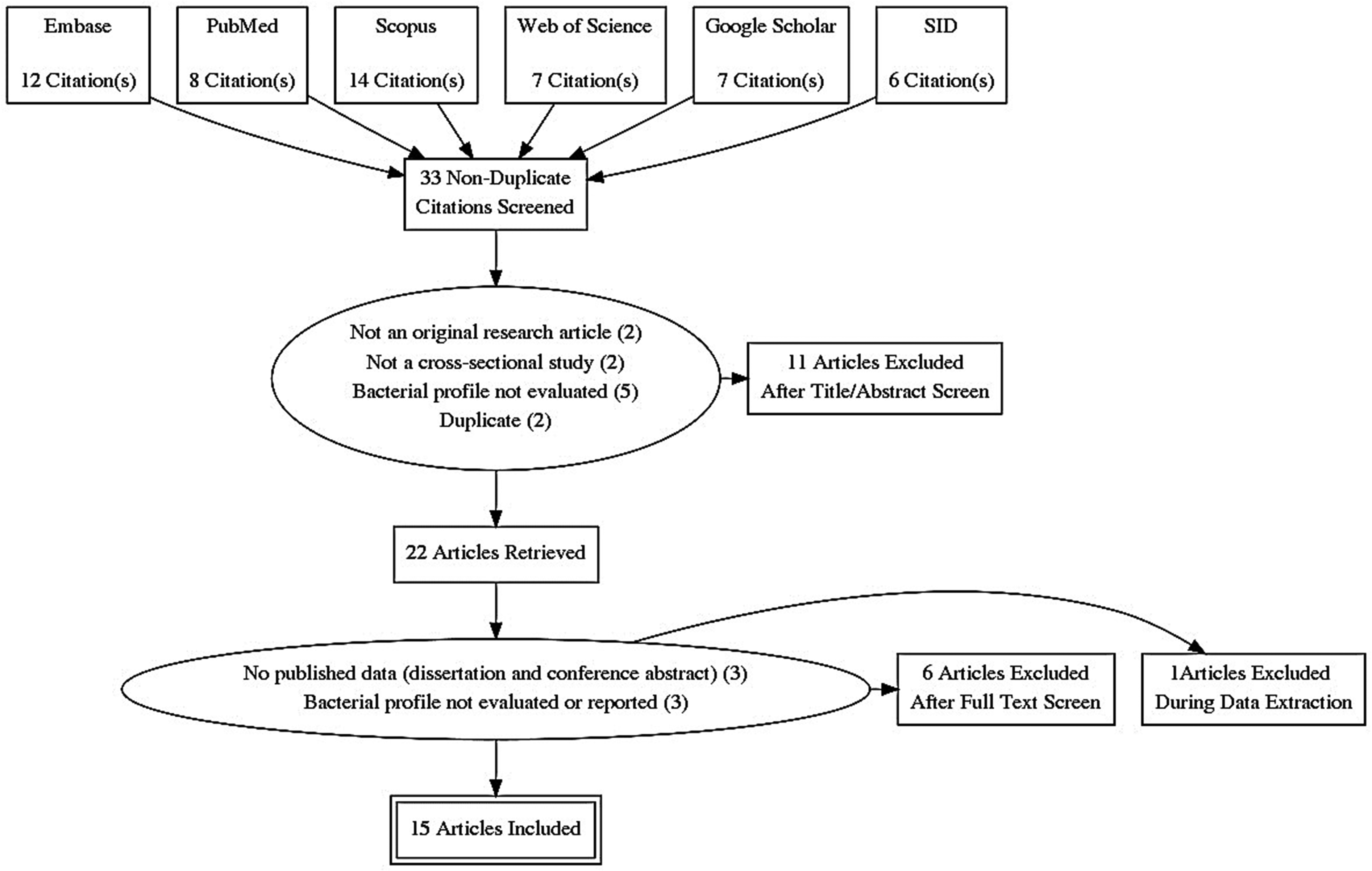
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow diagram depicting the selection process.
Characteristics of Included Studies
Among 15 included studies, 1970 bacterial isolates were obtained from 1316 patients. The number of positive cultures ranged from 26 13 to 147. 14 The number of DFI specimens ranged from 52 15 to 165. 14 The mean age of patients ranged from 52 7 to 62 16 years. All 15 articles evaluated bacterial profile,7,13–26 8 of them assessed antibiotic susceptibility as well.7,13–16,18,19,25 The included studies were conducted in 6 different provinces of Iran, of which, Tehran (the capital of Iran) had the most contribution (7 out of 15 studies). These studies were published in a 20-year period. The majority of them (8 articles) were published in the last 5 years. Samples were taken by 3 different methods, namely, swabbing, biopsy, and needle aspiration (Table 1).
Characteristics of the Included Studies.
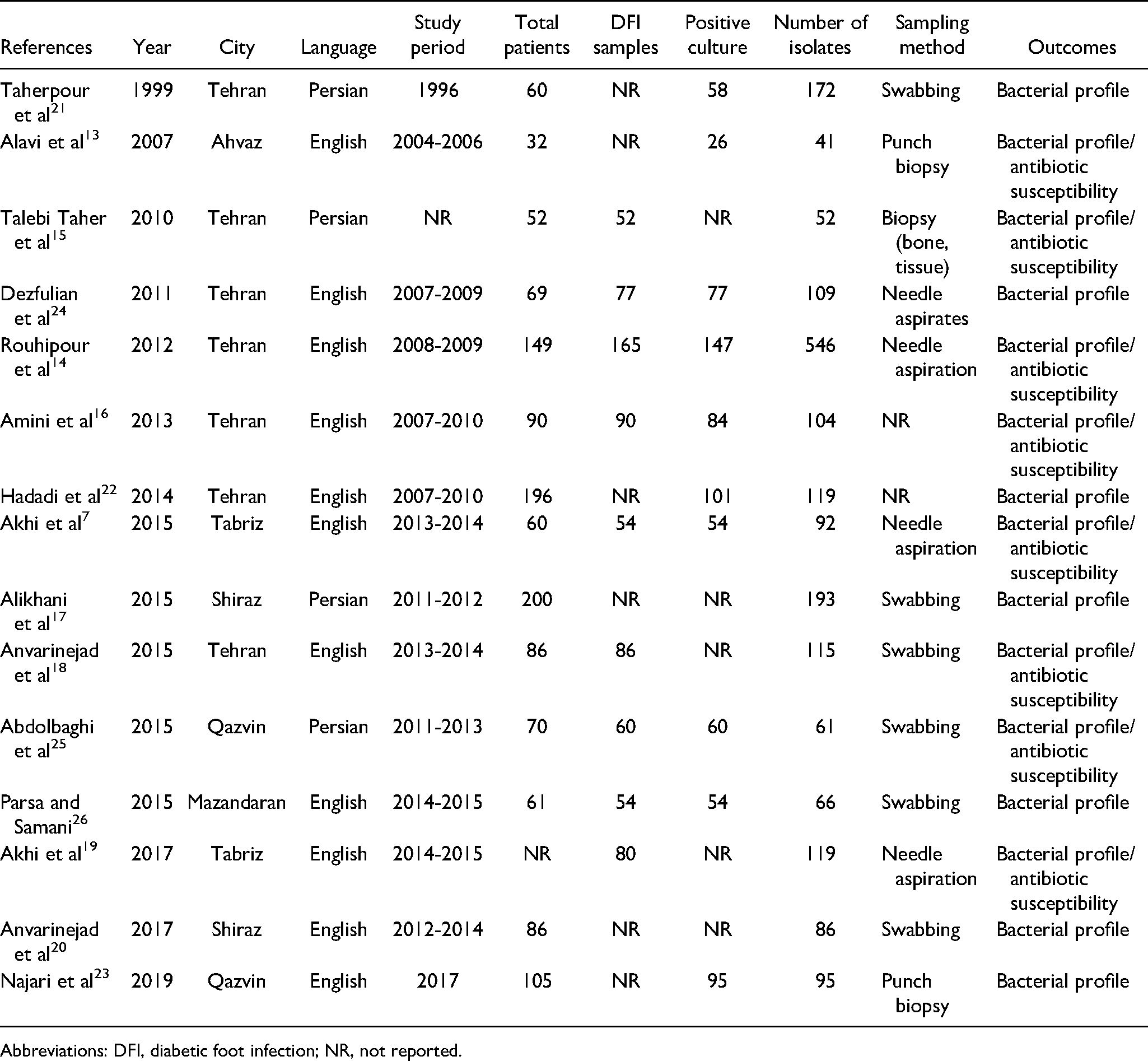
Abbreviations: DFI, diabetic foot infection; NR, not reported.
Results of Quality Assessment
The quality of the studies was assessed using the JBI tool. All of the 15 included studies received at least 5 “YES” answers and were included in the meta-analysis (Table 2).
Quality Assessment of Studies Using JBI's Critical Appraisal Tools Designed for Prevalence Studies.
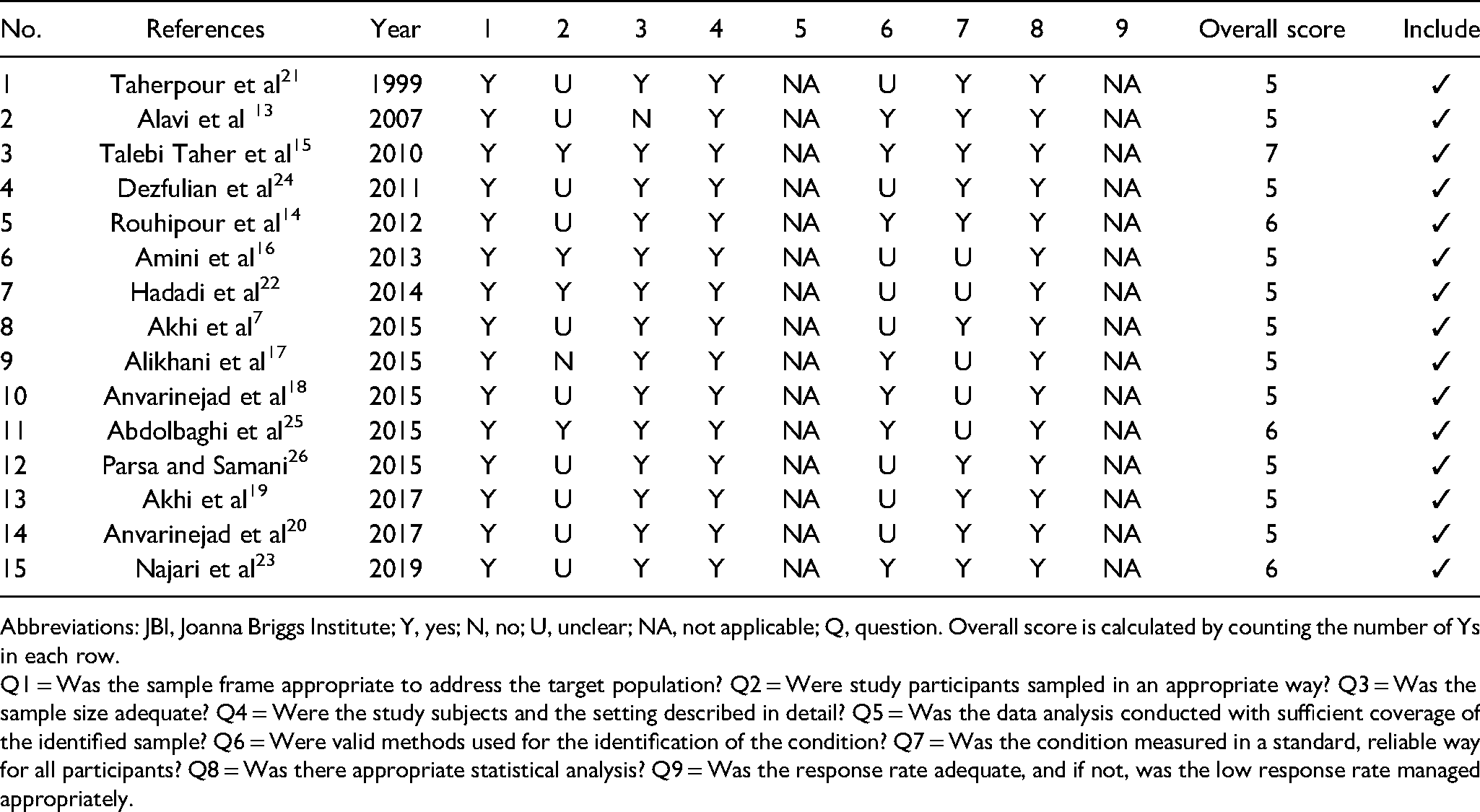
Abbreviations: JBI, Joanna Briggs Institute; Y, yes; N, no; U, unclear; NA, not applicable; Q, question. Overall score is calculated by counting the number of Ys in each row.
Q1 = Was the sample frame appropriate to address the target population? Q2 = Were study participants sampled in an appropriate way? Q3 = Was the sample size adequate? Q4 = Were the study subjects and the setting described in detail? Q5 = Was the data analysis conducted with sufficient coverage of the identified sample? Q6 = Were valid methods used for the identification of the condition? Q7 = Was the condition measured in a standard, reliable way for all participants? Q8 = Was there appropriate statistical analysis? Q9 = Was the response rate adequate, and if not, was the low response rate managed appropriately.
Bacterial Epidemiology
According to this systematic review and meta-analysis, the pooled proportion of culture-positive cases from DFI samples was found to be 73.58% (95% CI: 51.72%, 90.72%). Based on the subgroup analysis, the prevalence of total Gram-positive and Gram-negative isolates from DFIs was estimated to be 50.57% (95% CI: 43.62%, 57.51%) and 35.57% (95% CI: 24.06%, 47.97%), respectively (Supplemental material; Figure S1). The most common Gram-positive isolates were S. aureus 24.29% (95% CI: 20.25%, 28.57%), followed by coagulase-negative staphylococci (CoNS) (14.80%; 95% CI: 11.82%, 18.03%), Enterococcus spp. (13.58%; 95% CI: 7.40%, 21.19%), and Streptococcus spp. (4.04%; 95% CI: 2.78%, 5.50%).
Among Gram-negative strains, E. coli had the highest proportion 17.19% (95% CI: 13.96%, 20.68%) in DFIs. Pseudomonas spp. was second to E. coli with a pooled proportion of 7.54% (95% CI: 4.56%, 11.14%). The next 3 prevalent Gram-negative bacteria were as follows: Klebsiella spp. 4.77% (95% CI: 2.77%, 7.23%), Proteus spp. 4.32% (95% CI: 2.05%, 7.27%), and Acinetobacter spp. 4.32% (95% CI: 2.54%, 6.50%). The proportion of bacterial profile in Iranian DFIs is shown in Table 3, and corresponded forest plots are depicted in Figures 2 and 3.
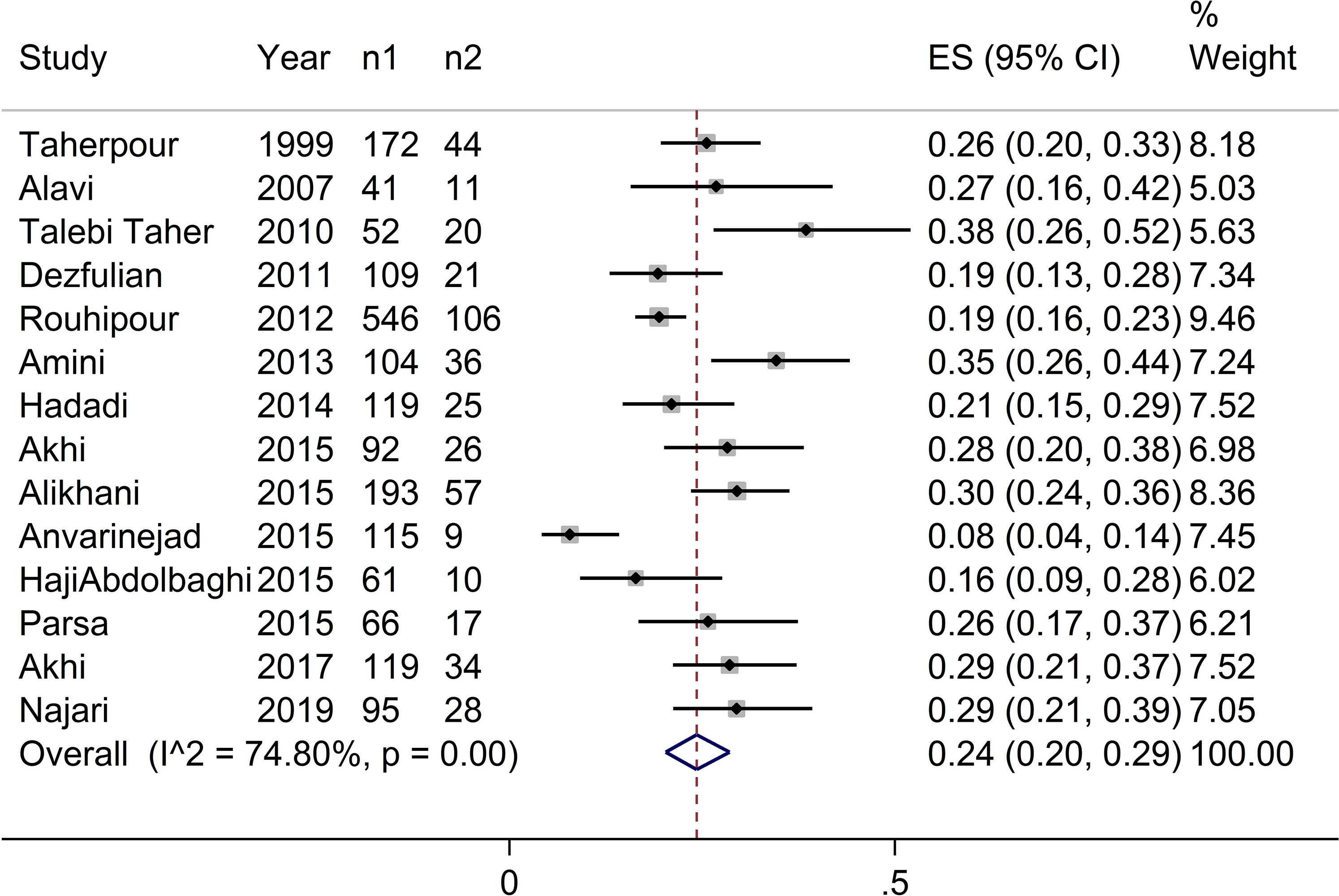
Forest plot showing the pooled proportion of Staphylococcus aureus isolates in diabetic foot infection (DFI) samples in Iran (n1: total number of isolates; n2: number of S. aureus isolates).
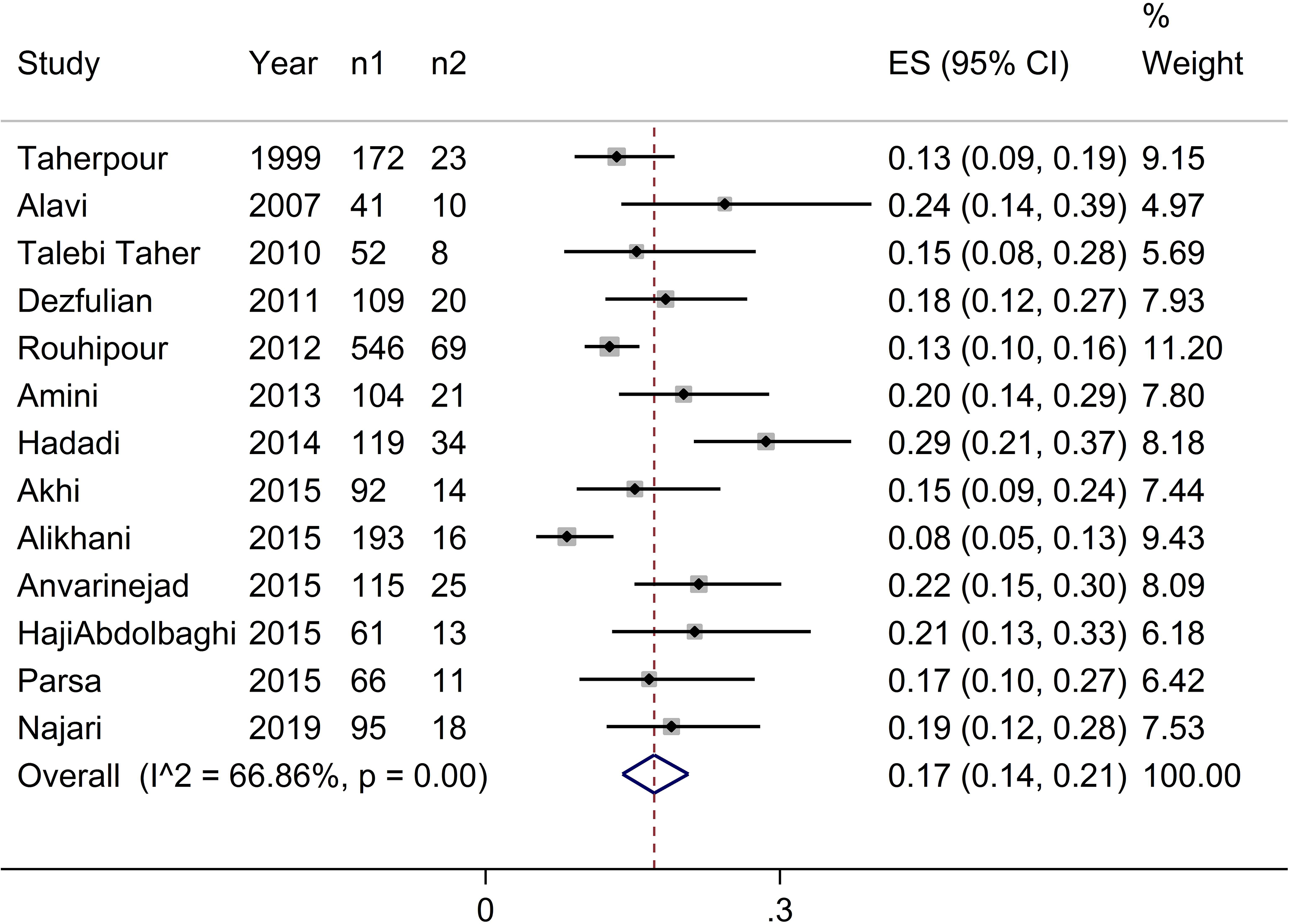
Forest plot showing the pooled proportion of Escherichia coli isolates in diabetic foot infection (DFI) samples in Iran (n1: total number of isolates; n2: number of E. coli isolates).
Meta-analysis for the Proportion of Bacterial Profile in DFIs, Iran.
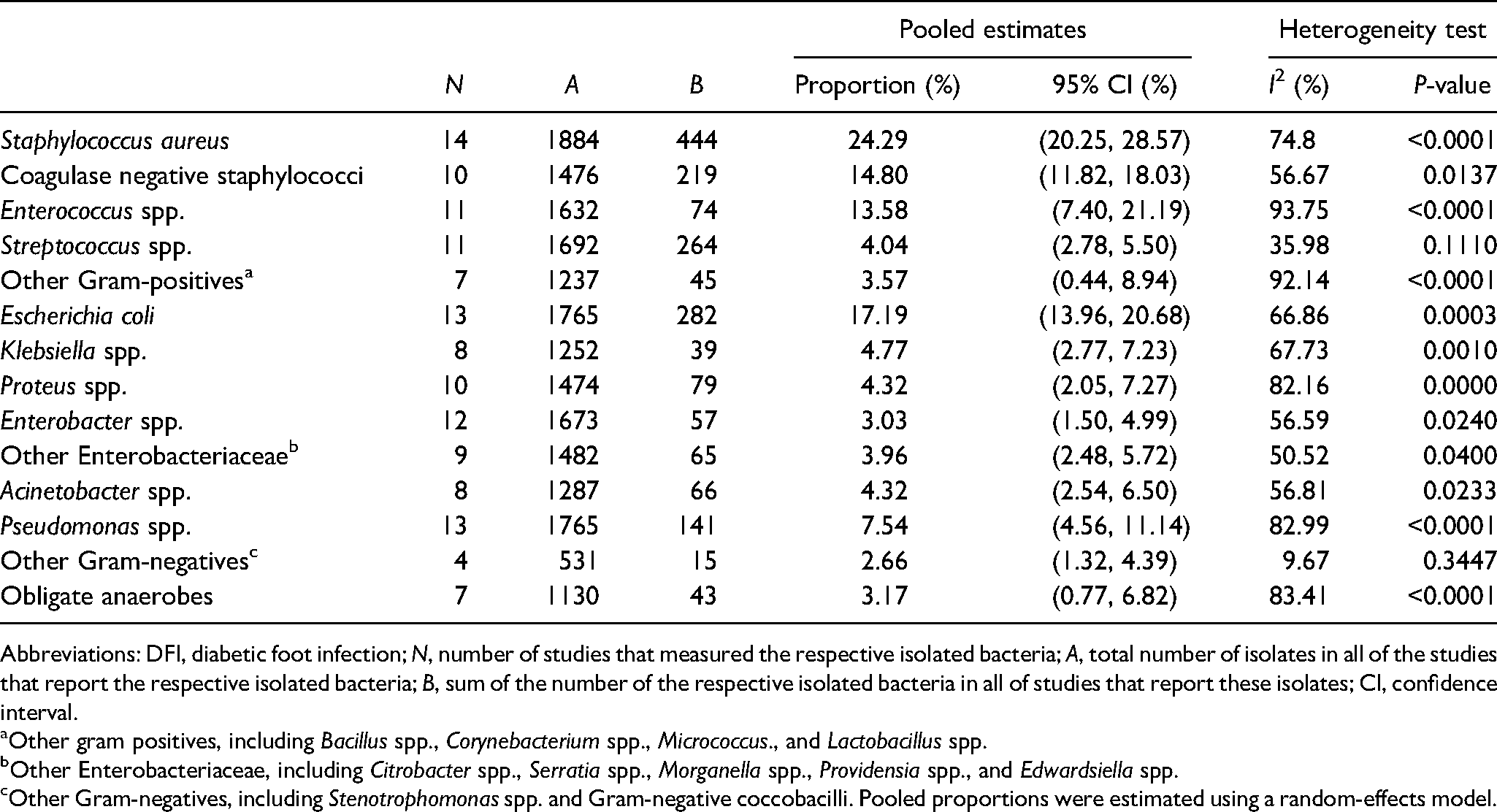
Abbreviations: DFI, diabetic foot infection; N, number of studies that measured the respective isolated bacteria; A, total number of isolates in all of the studies that report the respective isolated bacteria; B, sum of the number of the respective isolated bacteria in all of studies that report these isolates; CI, confidence interval.
Other gram positives, including Bacillus spp., Corynebacterium spp., Micrococcus., and Lactobacillus spp.
Other Enterobacteriaceae, including Citrobacter spp., Serratia spp., Morganella spp., Providensia spp., and Edwardsiella spp.
Other Gram-negatives, including Stenotrophomonas spp. and Gram-negative coccobacilli. Pooled proportions were estimated using a random-effects model.
A further subgroup analysis was also performed to assess if the proportion of bacteria can be influenced by various sampling methods. The results showed that the pooled proportion of S. aureus isolates using swabbing and biopsy or needle aspiration methods were 20.5% (95% CI: 12.5%, 29.9%) and 25.9% (95% CI: 20.8%, 31.3%), respectively (Supplemental material; Figure S2). In parallel, the pooled proportion of E. coli isolates using swabbing and biopsy or needle aspiration methods were 15% (95% CI: 10%, 21%) and 16% (95% CI: 13%, 19%), respectively (Supplemental material; Figure S3).
Antimicrobial Resistance Patterns
The pooled estimates of resistance rates against several antibiotics for Gram-positive and Gram-negative bacteria are shown in Tables 4 and 5, respectively. The most predominant isolate recovered from DFIs was S. aureus with a frequency of 24.29% (95% CI: 20.25%, 28.57%), from which 55% (95% CI: 38%, 72%) were methicillin-resistant S. aureus (MRSA). Ten out of 15 studies had identified MRSA using the phenotypic disk diffusion method. Table 6 shows the characteristic of these studies in detail.
Pooled Estimate of Antimicrobial Resistance Patterns Against Gram-positive Bacteria from DFIs in Iran.
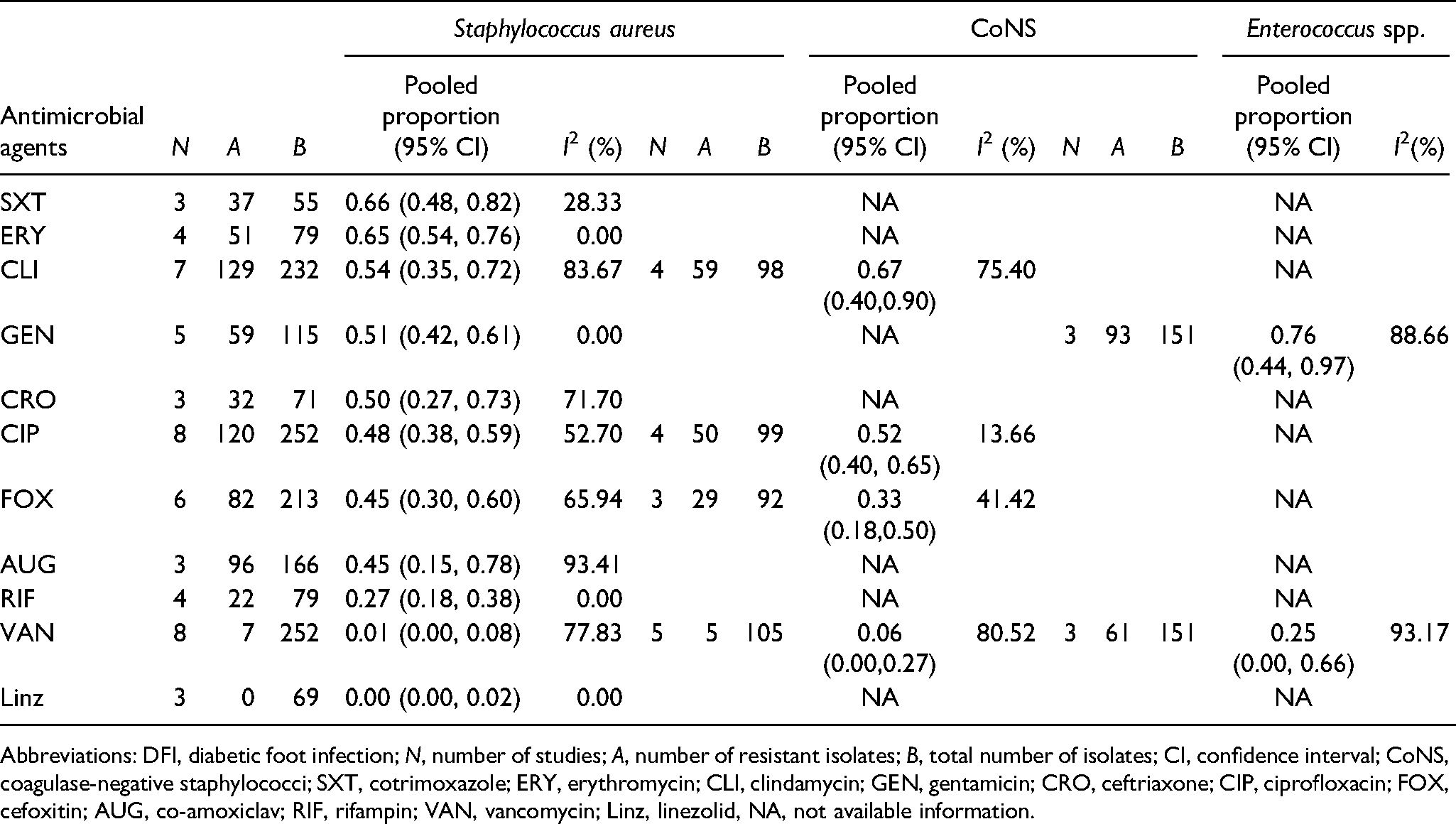
Abbreviations: DFI, diabetic foot infection; N, number of studies; A, number of resistant isolates; B, total number of isolates; CI, confidence interval; CoNS, coagulase-negative staphylococci; SXT, cotrimoxazole; ERY, erythromycin; CLI, clindamycin; GEN, gentamicin; CRO, ceftriaxone; CIP, ciprofloxacin; FOX, cefoxitin; AUG, co-amoxiclav; RIF, rifampin; VAN, vancomycin; Linz, linezolid, NA, not available information.
Pooled Estimate of Antimicrobial Resistance Patterns Against Gram-negative Bacteria from DFIs in Iran.
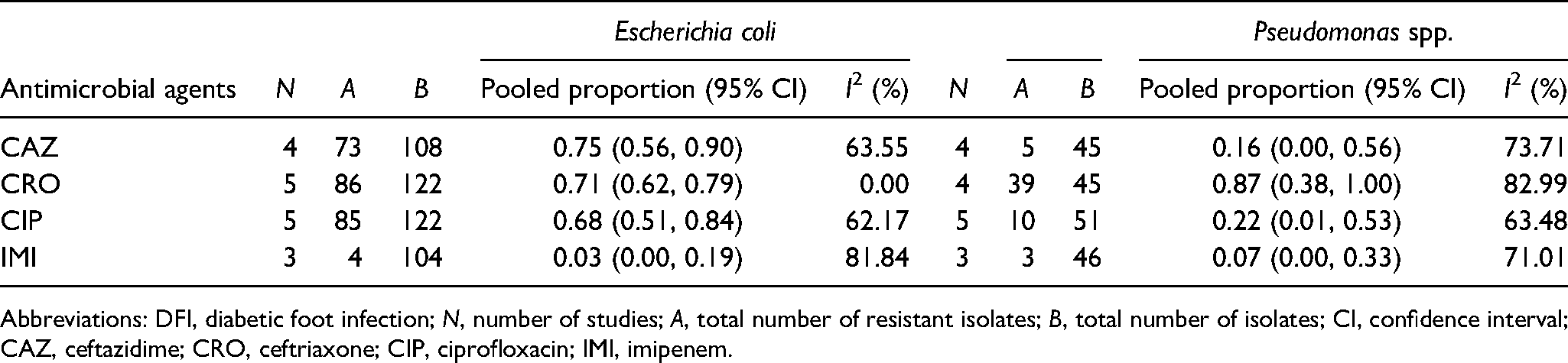
Abbreviations: DFI, diabetic foot infection; N, number of studies; A, total number of resistant isolates; B, total number of isolates; CI, confidence interval; CAZ, ceftazidime; CRO, ceftriaxone; CIP, ciprofloxacin; IMI, imipenem.
Characteristics of the Studies That Detect MRSA.
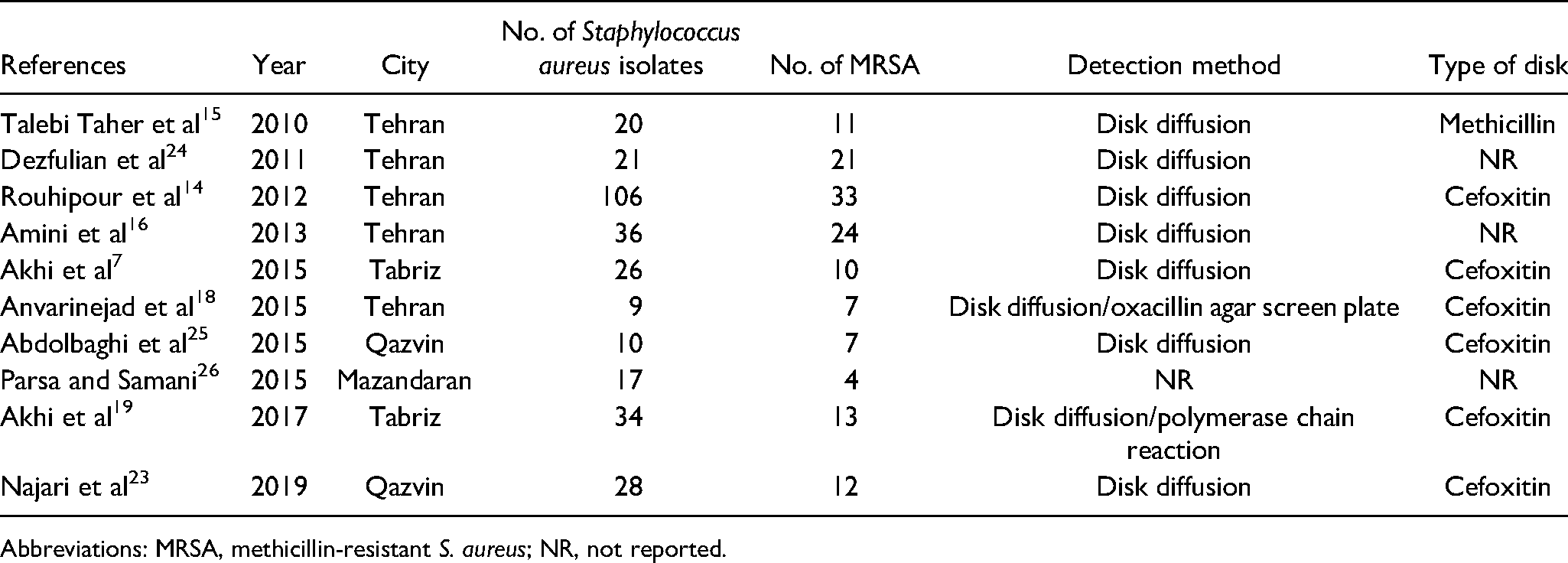
Abbreviations: MRSA, methicillin-resistant S. aureus; NR, not reported.
Among S. aureus isolates, the highest resistance rate was toward cotrimoxazole (66%; 95% CI: 48%, 82%). In addition, the pooled estimate of resistance rate to erythromycin (65%; 95% CI: 54%, 76%) was higher than clindamycin (54%; 95% CI: 35%, 72%). Half (50%; 95% CI: 27%, 73%) and more than half (51%; 95% CI: 42%, 61%) of S. aureus isolates were found resistant to ceftriaxone and gentamycin, respectively, in DFIs. The pooled estimate of ciprofloxacin resistance rate among S. aureus isolates (48%; 95% CI: 38%, 59%) and CoNS isolates (52%; 95% CI: 40%, 65%) was about 50%.
Regarding the AMR profiles of Gram-negative pathogens, E. coli isolates exhibited the highest resistance rate against ceftazidime (75%; 95% CI: 56%, 90%) followed by ceftriaxone (71%; 95% CI: 62%, 79%). The pooled estimate of resistance rate against ciprofloxacin in E. coli isolates was 68% (95% CI: 51%, 84%). Despite the existing concerns about treating Pseudomonas aeruginosa, these isolates showed the lowest resistance rate against ciprofloxacin and ceftazidime.
Publication Bias
Funnel plots of standard error with the prevalence of positive bacterial cultures revealed that there is some evidence of publication bias (Begg's test z = 2.68, P-value = .007; Egger's test: t = −2.38, P-value = .045) (Figure 4).
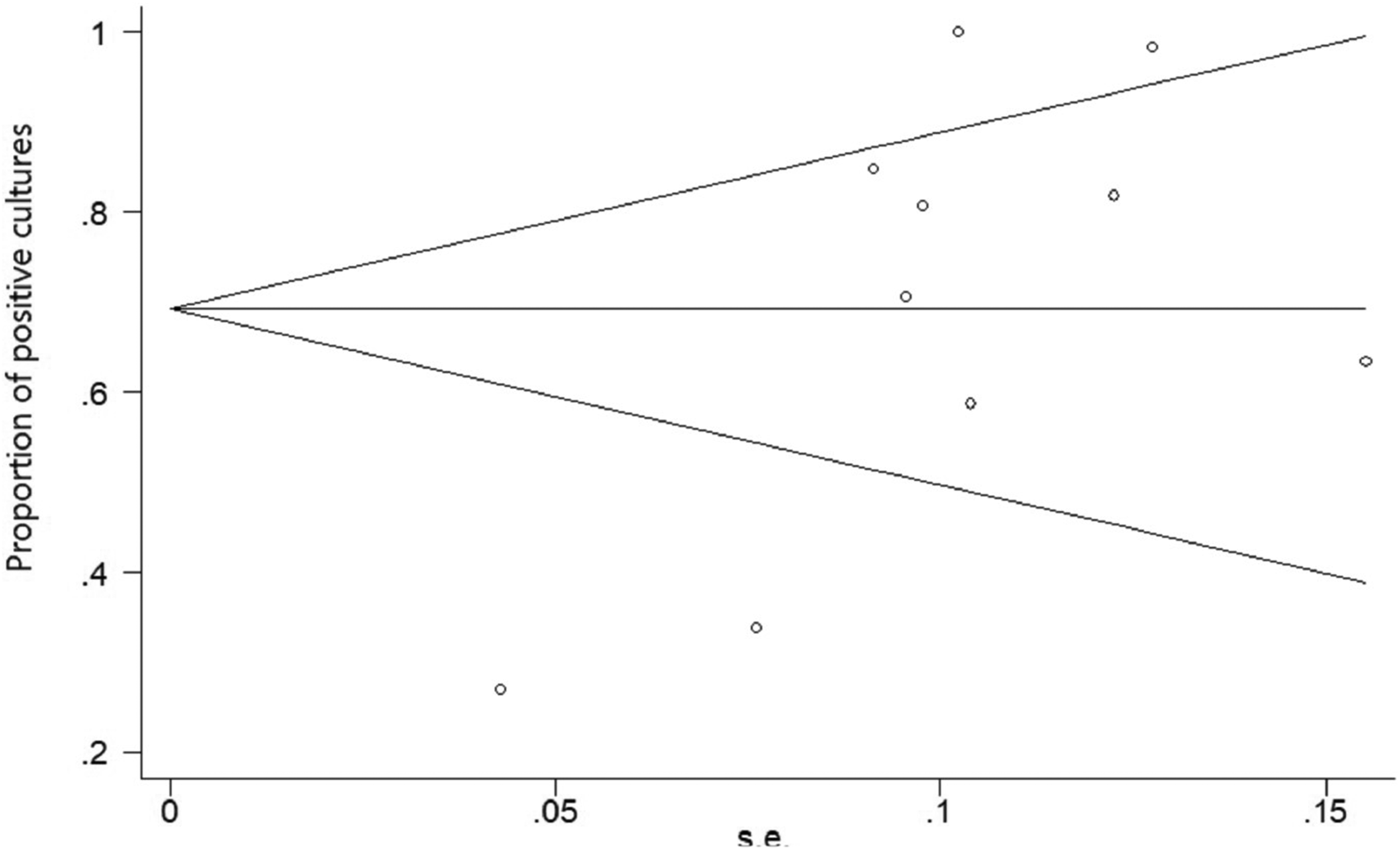
Funnel plot of the proportion of positive cultures from diabetic foot infection (DFI) samples.
Discussion
This is the first systematic review and meta-analysis in the field of bacterial profile and AMR patterns of DFIs. Approximately 74% of diabetic foot ulcers of our included studies were culture-positive. The most predominant isolate recovered from DFIs was S. aureus with the pooled estimate of 24% (range: 7.8%-38.46%), from which 55% were MRSA. These results are in accordance with the results of 2 systematic reviews (Middle East North Africa and Turkey) that reported a range of 5% to 42% and 23.8% for S. aureus isolates, respectively.5,6 However, some studies conducted in Southwestern Nigeria and South India reported the prevalence of S. aureus in DFIs as 13% to 14%.27,28 The pooled estimate of MRSA proportion (55%) is in accordance with the results of another systematic review and meta-analysis which reported the pooled estimation of mecA-MRSA (52.7% ± 4.7%) in Iran. 29
E. coli (17.19%) and P. aeruginosa (7.54%) were the most prevalent Gram-negative bacteria isolated from DFIs. Our results were consistent with the prevalence reported in another systematic review and meta-analysis of wounds in Ethiopia (E. coli [13%] and P. aeruginosa [9%]). 30 In a prospective study in India, the most common pathogens in DFI samples were reported as Staphylococcus spp. (24.86%) (from which 41% were MRSA), E. coli (20%), Enterococcus spp. (14.59%), Klebsiella (11.89%), and Pseudomonas (11.89%). 31 Differences observed between our results and the above-mentioned studies may be related to the geographical location. 5
Since the quality of the swabbing method is still controversial for bioburden recovery, 32 we conducted a subgroup analysis for comparing the effect of the sampling method on the proportion of the top 2 prevalent isolated bacteria. The results of subgroup analysis indicated that using biopsy or needle aspiration methods estimated a higher proportion of S. aureus or E. coli isolates.
Compared to the study conducted in Ethiopia, 30 our results showed considerable differences in S. aureus isolates' resistance to the most commonly prescribed antibiotics (including cotrimoxazole [66% vs 35%], erythromycin [65% vs 34%], gentamicin [51% vs 13%], and ciprofloxacin [48% vs 12%]), which leads to limited antibiotics options for clinicians. However, these isolates were still susceptible to vancomycin and linezolid. Regarding Gram-negative bacteria, we also observed comparable differences in E. coli isolates' resistance to ceftriaxone (71% vs 45%). These differences may be related to the nature of wound types that have been evaluated in these studies.
Resistance to the third-generation cephalosporins among E. coli isolates may be due to the extensive distribution of extended-spectrum beta-lactamase among Enterobacteriacae. Since resistance rates against these 2 third-generation cephalosporins are >70%, we suggest that these antibiotics are “alarming empirical regimens” for E. coli infection in Iran and it might be better if they are not prescribed anymore. 33 Although data about AMR of DFIs were poor in Iran, we still can suggest that imipenem and amikacin can be appropriate antibiotics for E. coli infections.
Some of the limitations of the study are as follows: We only have the studies from 6 cities of Iran and there is no information from the East of Iran to be considered for describing the bacterial profile in DFIs. This might be of more importance in the case of MRSA, for which data are available only from 4 cities. The other limitations are that most of the included studies did not have large sample sizes and did not identify anaerobic bacteria. In addition, few studies have investigated the same classes of antibiotics for the same bacteria. Therefore, we could not present comprehensive AMR patterns even for dominant bacterial pathogens. There was considerable heterogeneity among the studies, which may limit interpretations about the pooled estimations. However, we tried to address the results of each individual study to compensate for this heterogeneity. Finally, there was no similar meta-analysis study in the field of DFI to compare our results efficiently. Some other Asian studies also differ in the aim of the study, 33 reporting manner, 31 or lack of similar data. 6
Overall, our study revealed that the top 2 bacterial profiles of DFIs in Iran are S. aureus and E. coli and their AMR is at a high level (>50%). This study warns clinicians to be aware of bacterial resistance patterns when prescribing appropriate antibiotic regimens. Also, the results call for conducting further original studies that work on the bacteriology of DFIs and investigate more various antibiotics to determine resistance patterns more precisely.
Supplemental Material
sj-jpg-1-ijl-10.1177_15347346211002715 - Supplemental material for Bacterial Profile and Antimicrobial Resistance Patterns of Infected Diabetic Foot Ulcers in Iran: A Systematic Review and Meta-Analysis of Cross-Sectional Studies
Supplemental material, sj-jpg-1-ijl-10.1177_15347346211002715 for Bacterial Profile and Antimicrobial Resistance Patterns of Infected Diabetic Foot Ulcers in Iran: A Systematic Review and Meta-Analysis of Cross-Sectional Studies by Samaneh Shahrokh, Tabatabaee Aliye, Maryam Yazdi, Mansour Siavash and Ashraf Aminorroaya in The International Journal of Lower Extremity Wounds
Supplemental Material
sj-jpg-2-ijl-10.1177_15347346211002715 - Supplemental material for Bacterial Profile and Antimicrobial Resistance Patterns of Infected Diabetic Foot Ulcers in Iran: A Systematic Review and Meta-Analysis of Cross-Sectional Studies
Supplemental material, sj-jpg-2-ijl-10.1177_15347346211002715 for Bacterial Profile and Antimicrobial Resistance Patterns of Infected Diabetic Foot Ulcers in Iran: A Systematic Review and Meta-Analysis of Cross-Sectional Studies by Samaneh Shahrokh, Tabatabaee Aliye, Maryam Yazdi, Mansour Siavash and Ashraf Aminorroaya in The International Journal of Lower Extremity Wounds
Supplemental Material
sj-jpg-3-ijl-10.1177_15347346211002715 - Supplemental material for Bacterial Profile and Antimicrobial Resistance Patterns of Infected Diabetic Foot Ulcers in Iran: A Systematic Review and Meta-Analysis of Cross-Sectional Studies
Supplemental material, sj-jpg-3-ijl-10.1177_15347346211002715 for Bacterial Profile and Antimicrobial Resistance Patterns of Infected Diabetic Foot Ulcers in Iran: A Systematic Review and Meta-Analysis of Cross-Sectional Studies by Samaneh Shahrokh, Tabatabaee Aliye, Maryam Yazdi, Mansour Siavash and Ashraf Aminorroaya in The International Journal of Lower Extremity Wounds
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The Isfahan Endocrine and Metabolism Research Center funded this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.