
Abstract
We aimed to determine pathogen microorganisms, their antimicrobial resistance patterns, and the effect of initial treatment on clinical outcomes in patients with diabetic foot infection (DFI). Patients with DFI from 5 centers were included in this multicenter observational prospective study between June 2018 and June 2019. Multivariate analysis was performed for the predictors of reinfection/death and major amputation. A total of 284 patients were recorded. Of whom, 193 (68%) were male and the median age was 59.9 ± 11.3 years. One hundred nineteen (41.9%) patients had amputations, as the minor (n = 83, 29.2%) or major (n = 36, 12.7%). The mortality rate was 1.7% with 4 deaths. A total of 247 microorganisms were isolated from 200 patients. The most common microorganisms were Staphylococcus aureus (n = 36, 14.6%) and Escherichia coli (n = 32, 13.0%). Methicillin resistance rates were 19.4% and 69.6% in S aureus and coagulase-negative Staphylococcus spp., respectively. Multidrug-resistant Pseudomonas aeruginosa was detected in 4 of 22 (18.2%) isolates. Extended-spectrum beta-lactamase-producing Gram-negative bacteria were detected in 20 (38.5%) isolates of E coli (14 of 32) and Klebsiella spp. (6 of 20). When the initial treatment was inappropriate, Klebsiella spp. related reinfection within 1 to 3 months was observed more frequently. Polymicrobial infection (p = .043) and vancomycin treatment (p = .007) were independent predictors of reinfection/death. Multivariate analysis revealed vascular insufficiency (p = .004), hospital readmission (p = .009), C-reactive protein > 130 mg/dL (p = .007), and receiving carbapenems (p = .005) as independent predictors of major amputation. Our results justify the importance of using appropriate narrow-spectrum empirical antimicrobials because higher rates of reinfection and major amputation were found even in the use of broad-spectrum antimicrobials.
Keywords
Introduction
Foot infections in patients with diabetes mellitus are one of the most common infectious complications that require hospitalization and result in lower extremity amputations. 1 The diagnosis of diabetic foot infection (DFI) should be based on both clinical findings consistent with infection and the results of a wound culture. There are various factors that influence prognosis and outcomes of the patients with DFI such as wound depth and extension, microbiological agents and their susceptibility, accompanying diseases, previous antibiotic use, and the duration of infection (acute or longstanding). 2
Initial antibiotherapy for patients with DFI is mostly empirical. Treatment for DFI needs a certain diagnosis including a proper sampling for culture, performing any needed surgical procedures, and selecting an empirical antimicrobial therapy. Empirical therapy should be modified based on microbiological test results and definitive therapy needs to be tailored to the clinical response. The use of unnecessary and inappropriate antibiotics has become a major problem for the management of DFIs with multidrug-resistant microorganisms. Multidrug-resistant pathogen rates have been increasing to alarming levels. Since DFI is frequently chronic and polymicrobial, the microbiological evaluation of DFI is often grueling.3-5 Clinicians should avoid unnecessary broad-spectrum antibiotics, only the causative pathogens should be targeted. DFI management and antimicrobial stewardship should include a multidisciplinary team approach including surgeons, endocrinologists, infectious disease specialists, and microbiologists. 6
In this multicenter prospective observational study, we aimed to determine pathogen microorganisms and their antimicrobial resistance patterns and to investigate the effect of initial treatment on clinical outcomes including reinfection/death and major amputation in patients with DFI.
Materials and Methods
This observational prospective study was conducted by the DFI Study Group of the Turkish Society of Clinical Microbiology and Infectious Diseases. Patients with DFI from 5 centers were included between June 20, 2018, and June 20, 2019. DFI was diagnosed by trained infectious diseases physicians. Patients with DFI were observed for a 6-month follow-up period. Specimens were obtained using wound curettage after debridement, needle aspiration of purulent material, or tissue biopsy and/or bone biopsy. Swabbing of the wound was not allowed in order to avoid contamination. Standard clinical laboratory methods were used for the identification of the microorganisms. For microbiological identification, modern methods were used as well as traditional methods including staining, culturing, and simple biochemical tests, following the European Committee on Antimicrobial Susceptibility Testing guidelines. Microbiological isolates were processed for identification and antibiotic sensitivity tests by the Vitek 2 Compact system (bioMérieux), when necessary. Multidrug resistance (MDR) was defined as acquired nonsusceptibility to ≥3 different antimicrobial classes.
The demographic data including age, gender, underlying diseases, wound characteristics, laboratory parameters, microbiological, and radiological examination results were collected and assessed prospectively. Chronic artery disease was defined as a composite of coronary artery disease, cerebrovascular disease, and peripheral artery disease and was identified using medical records and self-reports. Vascular insufficiency which refers to lower extremity peripheral vascular disease was assessed with symptoms, physical examination, and Doppler ultrasound. Additionally, conventional angiography or computed tomographic angiography was performed, when necessary. Vascular insufficiency was qualitatively recorded. DFI severity score was grouped as mild, moderate, or severe according to the perfusion, extent, depth, infection, and sensation (PEDIS) classification system. 7 All patients with severe infection and patients with a moderate infection with complicating features were hospitalized. Each patient was followed up for 6 months, and treatment failures were recorded. Major amputation was defined as any lower extremity resection proximal to the ankle. Minor amputation was defined as any resection at the level of the ankle, foot, or toe. 8 Healing was defined as the complete and uniform skin formation in the wound area. Our primary and secondary endpoints were reinfection or in-hospital death and major amputation, respectively.
Frequencies (n) and percentages (%) were used to present the descriptive characteristics of the data, while numerical variables were represented through mean ± standard deviation (SD) and median. The Kolmogorov–Smirnov test was used for normal distribution analysis. The independent-sample t-test and the Mann–Whitney U test were used to compare the two groups in terms of the continuous variables. Categorical data were compared with the Chi-square test or Fischer’s exact test. Univariate analysis was applied to evaluate the strength of association between predictors. The significant independent variables in univariate analysis were included in the multivariate analysis. Multivariate analysis was performed for the predictors of the primary composite endpoint including reinfection and in-hospital death, and secondary endpoint including major amputation. The odds ratio (OR) and 95% confidence interval (95% CI) were calculated from the beta coefficients of the variables with a significant p-value. A p-value <.05 was considered to be statistically significant. The analyses were performed using IBM SPSS-22 (Statistical Package for Social Sciences).
This study was conducted in accordance with the ethical standards of the Declaration of Helsinki.
Results
A total of 284 patients were recorded. Of whom, 193 (68%) were male, the median age was 59.9 ± 11.3 years (range, 30-90 years). A total of 184 (64.8%) patients had a moderate infection, and 54 (19%) patients had severe infection according to the PEDIS classification. Osteomyelitis was diagnosed in 181 (63.7%) patients. Of the 284 patients, 119 (41.9%) had amputations, as the minor (n = 83, 29.2%) or major (n = 36, 12.7%). Four patients (1.7%) died. Initial treatment was inappropriate in 33 (11.6%) patients. In 135 (47.5%) patients, erythrocyte sedimentation rate (ESR) was >70 mm/h, in 106 patients (37.3%) C-reactive protein (CRP) level (reference range: 0-5 mg/dL) was >26-fold (>130 mg/dL), in 201 (70.8%) patients leukocyte count was >10 000/mm3 (Table 1).
The Demographic Characteristics
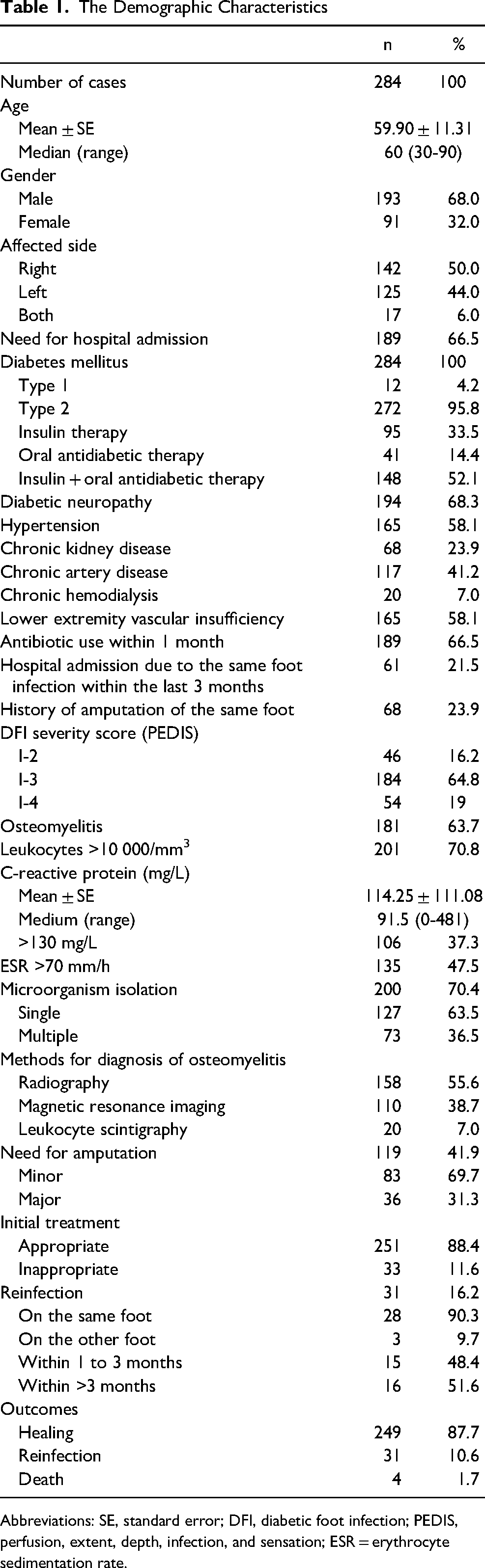
Abbreviations: SE, standard error; DFI, diabetic foot infection; PEDIS, perfusion, extent, depth, infection, and sensation; ESR = erythrocyte sedimentation rate.
A total of 247 microorganisms were isolated from 200 patients. Of whom, 73 (36.5%) had polymicrobial DFI. Gram-negative bacteria (GNB) and Gram-positive bacteria were isolated from 66 (33.0%) and 61 (30.5%) patients, respectively. The most common microorganisms were Staphylococcus aureus (n = 36, 14.6%) and Escherichia coli (n = 32, 13.0%). Methicillin resistance rates were 19.4% in S aureus and 69.6% in coagulase-negative Staphylococcus spp. MDR Pseudomonas aeruginosa was detected in 4 of 22 (18.2%) isolates. Extended-spectrum beta-lactamase-producing GNB were detected in 20 (38.5%) isolates of E coli (14 of 32) and Klebsiella spp. (6 of 20) (Table 2). A total of 120 microorganisms were obtained in 73 patients with polymicrobial infection. The most common isolated bacteria in the polymicrobial isolates were Enterococcus sp. (n = 19, 15.8%), E coli (n = 17, 14.2%), and S aureus (n = 16, 13.3%).
The Distribution of Isolated Microorganisms.
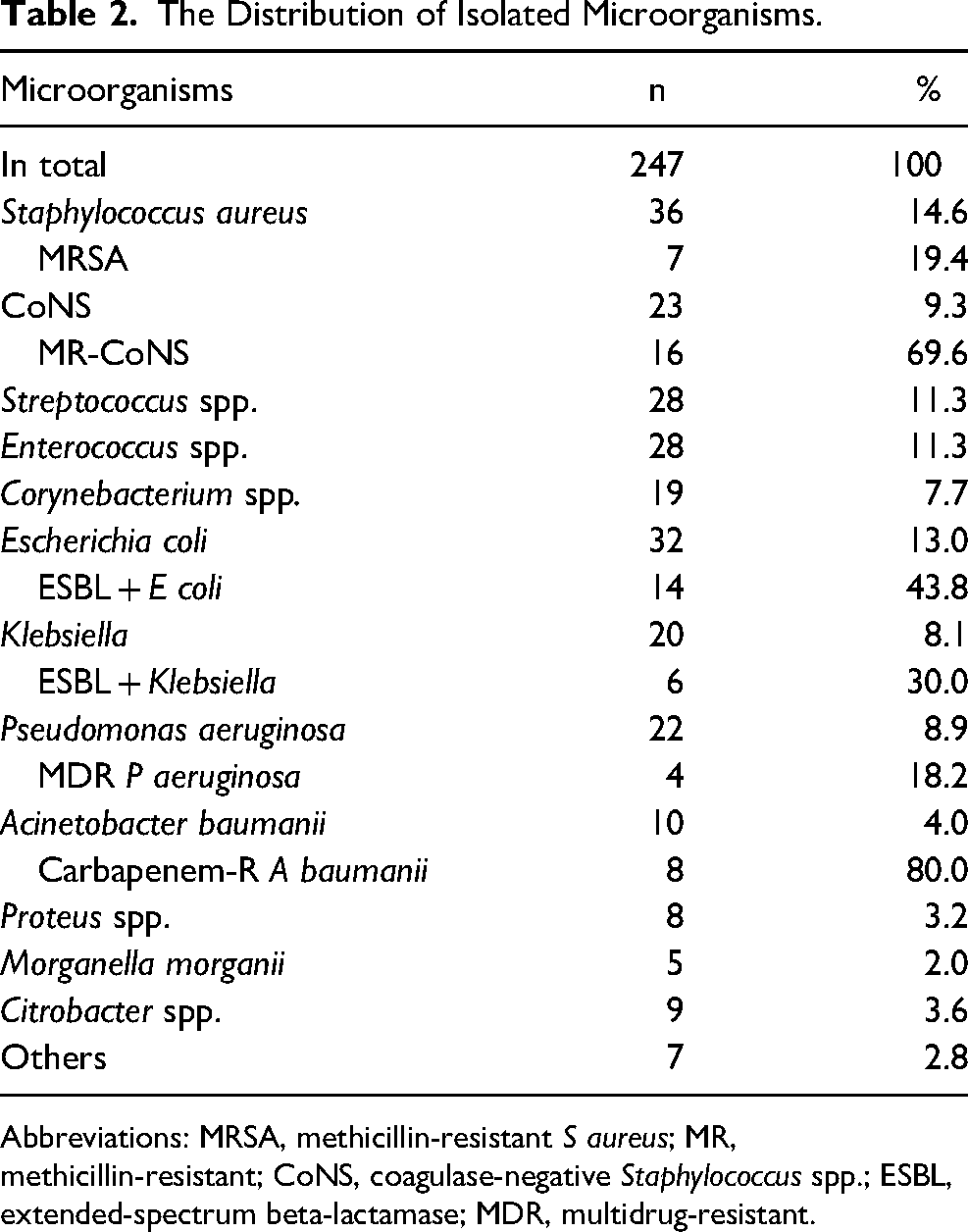
Abbreviations: MRSA, methicillin-resistant S aureus; MR, methicillin-resistant; CoNS, coagulase-negative Staphylococcus spp.; ESBL, extended-spectrum beta-lactamase; MDR, multidrug-resistant.
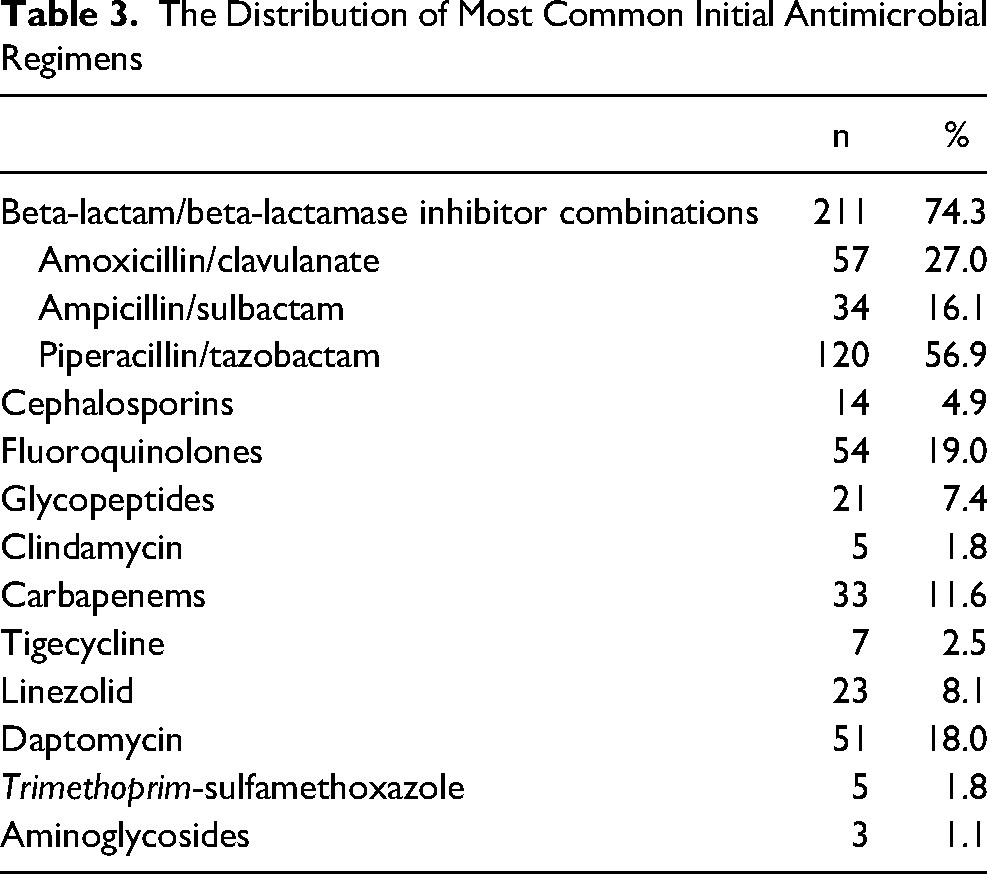
Most common initial antimicrobial regimens were beta-lactam/beta-lactamase inhibitor combinations (n = 211, 74.3%), fluoroquinolones (n = 54, 19.0%) and daptomycin (n = 51, 18.0%) (Table 3).
The Distribution of Most Common Initial Antimicrobial Regimens
In univariate analysis, statistically significant differences were observed in 9 predictors for reinfection/death (Table 4).
Univariate Associations of Various Variables with Reinfection/Death
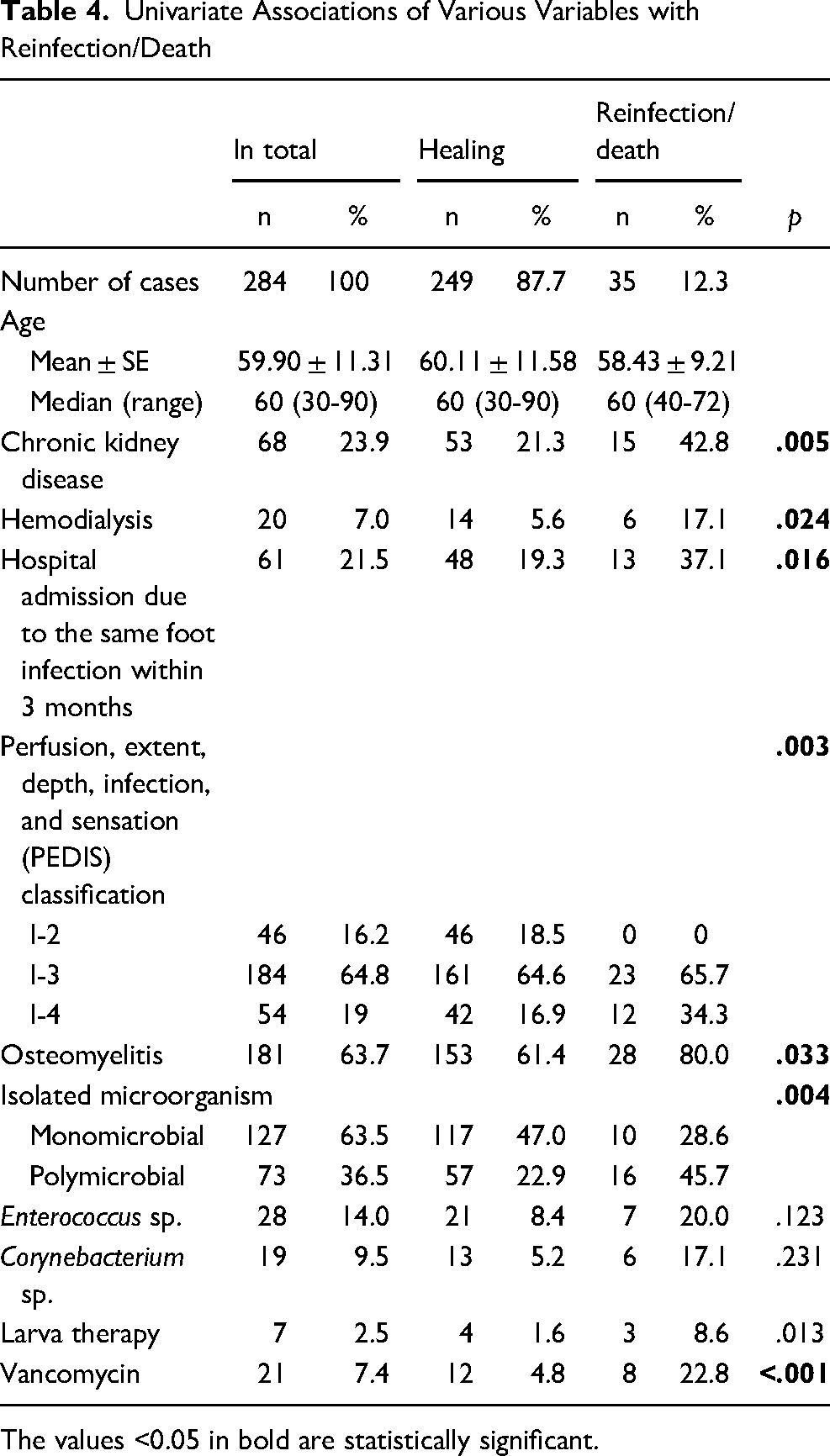
The values <0.05 in bold are statistically significant.
Logistic multivariate analysis identified polymicrobial infection (p = .043, OR = 2.64 [1.03-6.73]) and receiving vancomycin treatment (p = .007, OR = 4.57 [1.50-13.86]) as independent predictors of reinfection/death (Table 5).
Logistic Regression Analysis of Predictors for Reinfection/Death
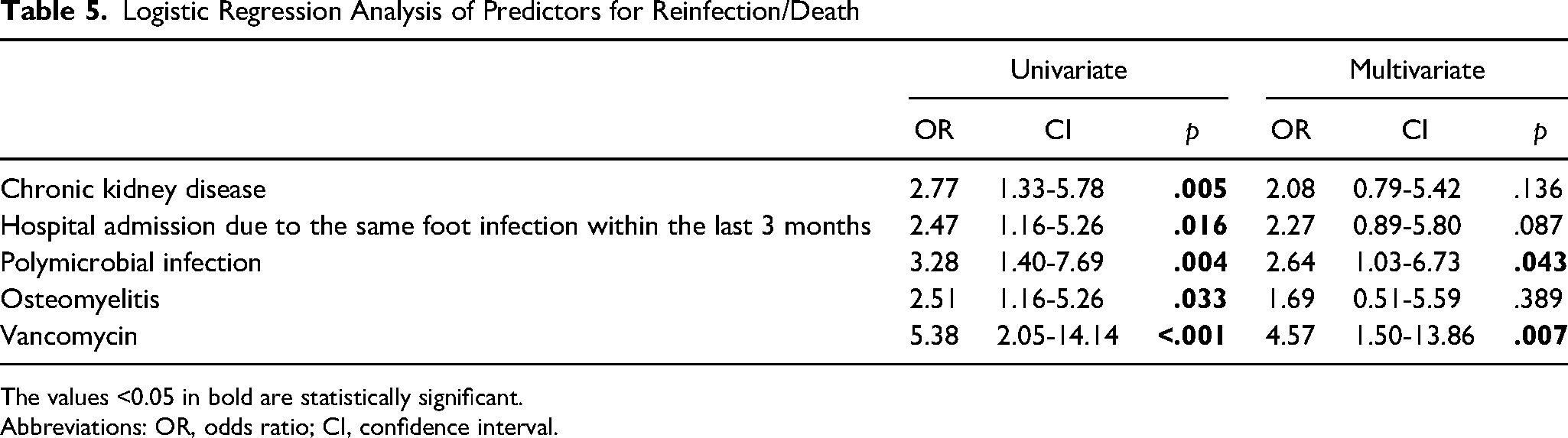
The values <0.05 in bold are statistically significant.
Abbreviations: OR, odds ratio; CI, confidence interval.
When the initial treatment was inappropriate, isolation of Klebsiella sp. related reinfection within 1 to 3 months was observed more frequently (Fischer’s exact test, p = .019) (Table 6).
Microorganisms Associated With Reinfection Within 1 to 3 months in Treatment Inappropriateness
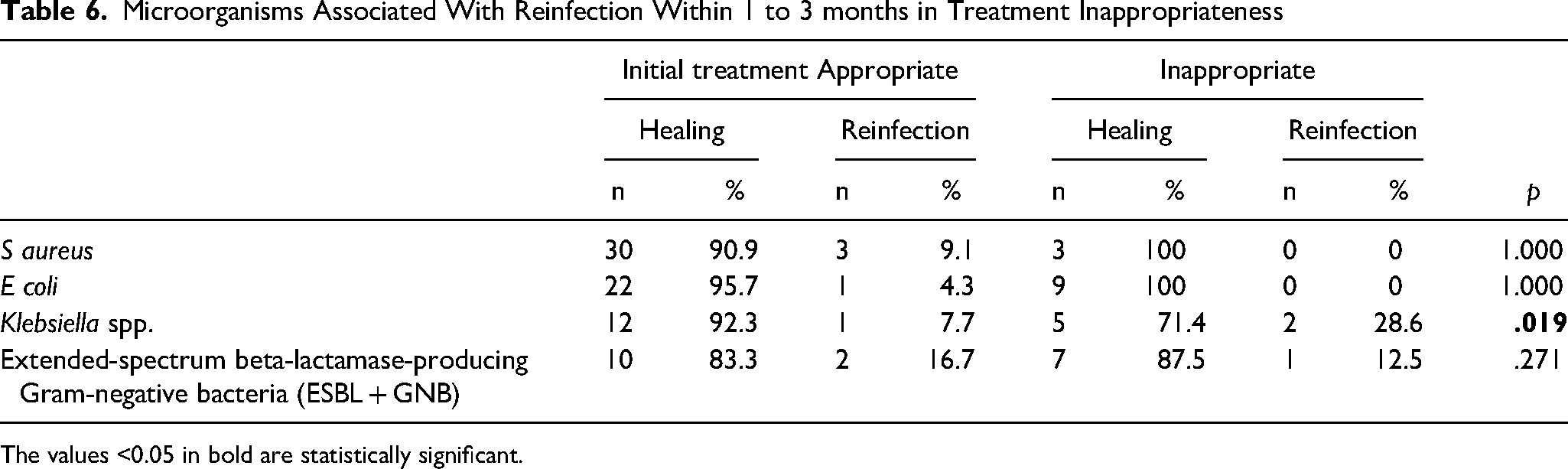
The values <0.05 in bold are statistically significant.
In univariate analysis, statistically significant differences were observed in 25 predictors for amputation (Table 7). Receiving hemodialysis, hospital admission due to the same foot infection within the last 3 months, affected sides (right foot, metatarsal part, midfoot), neuropathy, vascular insufficiency, high PEDIS score, osteomyelitis, leukocytes >10 000, CRP >130, ESR >70, polymicrobial infection, growth of Enterococcus spp., Morganella morganii, Citrobacter spp., extended-spectrum beta-lactamase [ESBL] (+) GNB, need for vascular intervention, combined antibiotherapy, receiving carbapenems or daptomycin, increased age, high levels of CRP, urea, and creatinine were associated with higher major amputation rates.
Univariate Associations of Various Variables With Amputation
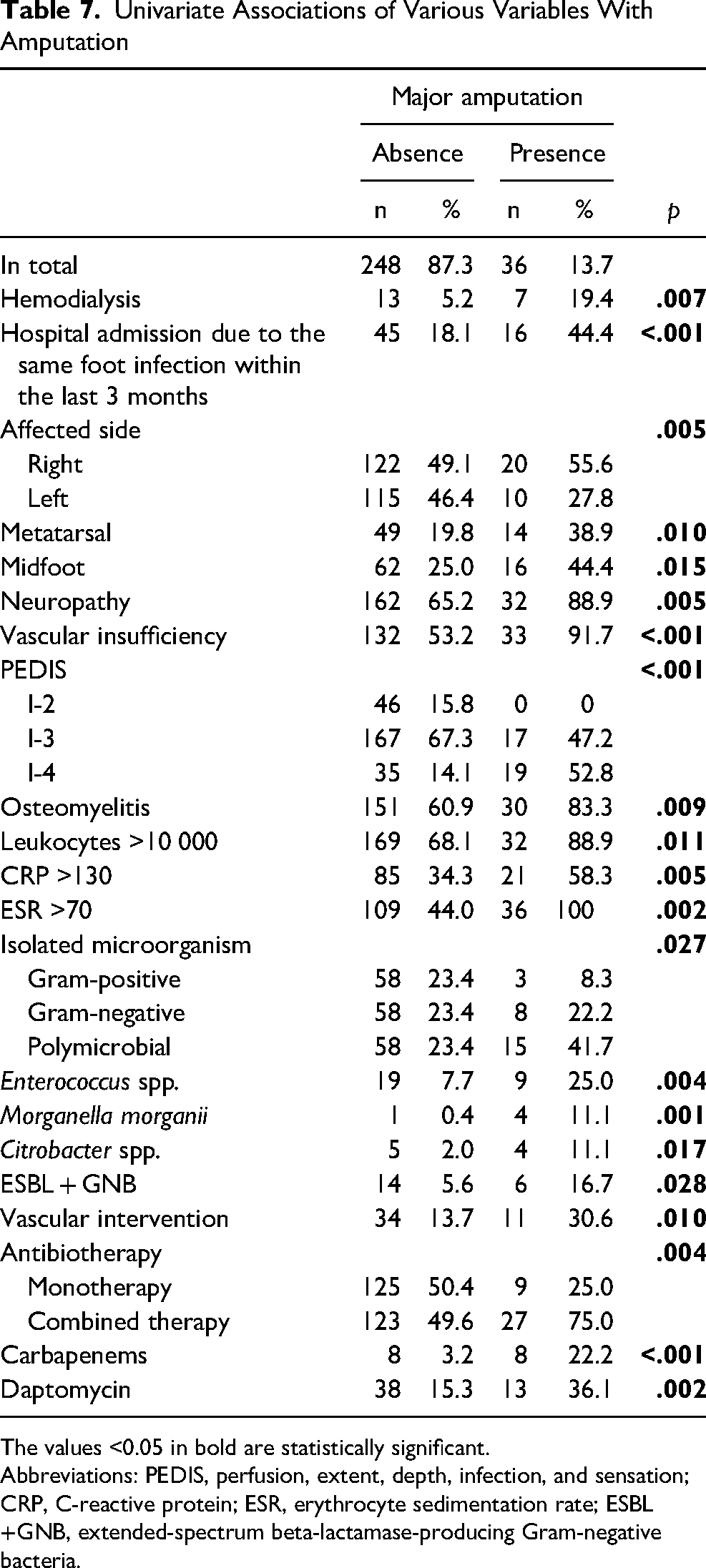
The values <0.05 in bold are statistically significant.
Abbreviations: PEDIS, perfusion, extent, depth, infection, and sensation; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; ESBL+GNB, extended-spectrum beta-lactamase-producing Gram-negative bacteria.
Logistic multivariate analysis identified vascular insufficiency (p = .004, OR = 6.46 [1.81-23.04]), hospital admission due to the same foot infection within the last 3 months (p = .004, OR = 3.25 [1.34-7.92]), CRP >130 (p = .007, OR = 3.30 [1.38-7.92]), receiving carbapenems (p = .005, OR = 6.60 [1.79-24.43]) as independent predictors of major amputation (Table 8).
Logistic Regression Analysis of Predictors for Major Amputation
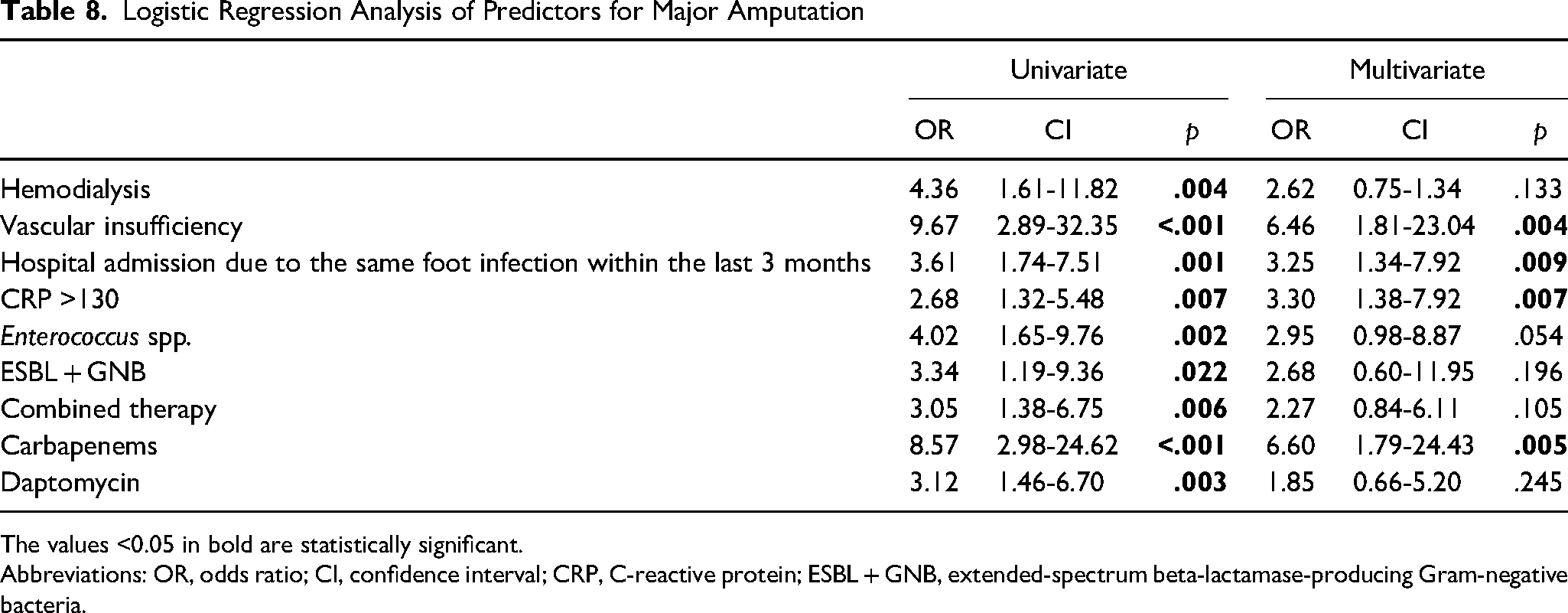
The values <0.05 in bold are statistically significant.
Abbreviations: OR, odds ratio; CI, confidence interval; CRP, C-reactive protein; ESBL + GNB, extended-spectrum beta-lactamase-producing Gram-negative bacteria.
Discussion
In this multicenter prospective study with 6 months follow-up, we investigated microorganisms isolated from patients with DFI, antimicrobial resistance profiles, and the effects of compatibility of initial antibiotic treatment on patient outcomes including reinfection, death, and major amputation. In univariate analysis, chronic kidney disease (p = .005), hemodialysis (p = .024), hospital admission due to the same foot infection within the last 3 months (p = .016), high PEDIS score (p = .003), osteomyelitis (p = .033), polymicrobial infection (p = .004), receiving larva therapy (p = .013), and vancomycin treatment (p < .001) were associated with higher reinfection/death rates. We found 2 independent predictors for reinfection/death in DFI; polymicrobial infection (OR = 2.64) and receiving vancomycin treatment (OR = 4.57).
In the study of Gariani et al, 9 they proposed that reinfection of DFI was not associated with antibiotic-related variables. In the present study, receiving vancomycin treatment was independently associated with 4.5-fold increased reinfection/death. This finding is in conflict with the study of Gariani et al. 9 This result may be due to both increased severity of DFI and renal insufficiency in our study population.
In recent years, while increasing in MDR Gram-negative has been reported in studies conducted from Southeast Asia, Gram-positive microorganisms are predominant agents in studies conducted from the West, consistent with our study from Turkey. 10 Multidrug-resistant organisms (MDROs) have been increasing due to frequent health care exposures and repeated antibiotic treatment in DFI patients.11-13 When the relationship between reinfection and causative microorganisms was evaluated, Klebsiella spp. (p = .019) was found to be associated with reinfection, but S aureus (p = 1.000) was not associated with reinfection in our study. In the study of Lebowitz et al, 14 S aureus was the predominant pathogen in all episodes. They found that PEDIS perfusion grade, multiple foot ulcers, and ulcer duration were independent predictors for healing. Methicillin-resistant S aureus (MRSA) is more often isolated from patients with DFI. The prevalence of MRSA is 15% to 30% in patients with DFI. 15 However, we did not find an increased prevalence in MRSA as opposed by others. In our study, the most common microorganisms were S aureus (14.6%) and E coli (13.0%). Methicillin resistance rates among S aureus and coagulase-negative Staphylococcus spp. isolates were 19% and 67%, respectively.
In our study, we revealed that vascular insufficiency (OR = 6.46), hospital admission due to the same foot infection within the last 3 months (OR = 3.25), CRP >130 mg/dL (OR = 3.02), and administration of carbapenems (OR = 6.60) were independent predictors for major amputation. Approximately 66.5% of the patients had a previous antibiotic use within the last 1 month, and 21.5% had a history of hospitalization due to the same foot infection within the last 3 months. Approximately 84% of the patients were identified as PEDIS 3 and 4. Ugwu et al 16 reported that ulcer duration, vascular insufficiency, and osteomyelitis were independent risk factors for amputation. In the previous multicenter study, GNB was a significant predictor of amputation. 17 In a meta-analysis conducted by Sen et al, 18 male gender, smoking, history of amputation, history of osteomyelitis, peripheral arterial disease, retinopathy, International Working Group on the Diabetic Foot grades 3 and 4, Wagner grades 4 and 5, gangrene/necrosis, osteomyelitis, neuroischaemic DFI, severe infection, length of hospitalization, leukocytosis, mean ESR, mean CRP, tissue culture positivity, and GNB were detected as predictors for amputation in DFI.
In the present study, the distribution of diabetic complications in 284 patients was as follows: 68% with diabetic neuropathy, 58% with vascular insufficiency, 24% with chronic kidney disease, and 7% with chronic hemodialysis. Recurrent infections in the same foot frequently increase the risk of encountering nosocomial pathogens in DFI, especially, in patients with vascular insufficiency. DFIs may progress rapidly. Patients with moderate and severe DFI frequently need to be hospitalized, for the administration of empirical antibiotherapy and immediate surgical interventions. 19 Antibiotherapy should be initiated according to clinical findings rather than a microbiological examination of proper specimens in critical cases, to not delay antibiotic treatment. 20 Additionally, the selection of antibiotics should be based on the clinical characteristics, severity of DFI, and local epidemiological data. Recent microbiological results and history of antibiotic use of patients are also important in the management of DFIs. 21 A proper empirical antibiotic regimen is controversial, and there is no evidence that any antimicrobial agent is superior in DFI initial treatment. 22 In our study, initial treatments were appropriate in 88% of patients. Beta-lactam–beta-lactamase enzyme inhibitor combinations were the most common group.
MRSA is associated with worse outcomes than other pathogens in DFIs. 23 However, Aragón-Sánchez et al 24 reported that MRSA bone infections are not associated with worse prognosis with the help of early and aggressive surgical implementations. Since the prevalence of MRSA in DFI seems to be low in our study, we strongly suggest that the coverage of empirical antibiotic therapy for MRSA should be limited to severe infection in order to prevent antimicrobial resistance in similar settings.
In our study, the high rate of MDROs might be associated with previous antibiotic use and a history of hospitalization in the last 3 months. In the study of Richard et al, 25 MDROs were isolated in 45 (23.9%) patients. They showed that MDROs were associated with a deep and recurrent ulcer, previous hospitalization, HbA(1c) level, retinopathy, and nephropathy. In the study of Hartemann-Heurtier et al, 26 previous hospitalizations and osteomyelitis were the only factors associated with MDROs. In recent years, rates of MDROs have been increasing in DFIs. This makes the management of DFIs difficult. The emergence of multidrug-resistant bacteria, especially in Gram-negative rods, may have a negative impact on the chances of cure in these patients.20,27 The choice of appropriate empirical antibiotics is important in order to reduce treatment failure, the likelihood of antimicrobial resistance, adverse events.
For severe infections, prescription of a broad-spectrum regimen in the initial treatment is a safer method. 28 However, the implementation of antibiotic de-escalation is also important in terms of reducing resistant microorganisms. Obtaining appropriate samples, monitoring the surveillance results, and questioning the risk factors in empirical treatment selection can be effective. 29
The strength of our study lies in its prospective and multicentric design. In addition, multiple comorbidities and different types of variables such as laboratory parameters, microbiological agents, and radiological findings were included in multivariate regression analysis. However, our study has also several limitations including having a small sample size and the absence of a control group. Second, we did not include smoking status as a confounder, although smoking is an important risk factor for vascular disease and death. 30 Third, since anaerobic isolation methods were not routinely performed, we did not isolate anaerobic bacteria. Also, differences in applications of antimicrobial treatment, infection control policies, community characteristics, and resistance patterns of microorganisms between centers may affect the results. Thus, we need new large-scale studies providing important information to better understand DFIs.
Conclusion
In the present study, recurrent infections in the same foot and the use of unnecessary broad-spectrum antibiotics increased the risk of encountering poor outcomes. MDROs are increasing due to frequent health care exposures and repeated antibiotic therapy. The higher rates of reinfection and major amputation, even in the use of broad-spectrum antimicrobials such as carbapenems, glycopeptide, and lipopeptide antibiotics justify the importance of the administration of appropriate narrow-spectrum antibiotics. In the National Institute for Health and Care Excellence 2019 DFI guideline, individualization of treatment has been proposed to minimize the development of resistance in the community. 31 As a result, the clinicians should implement continuous surveillance and develop antibiotic use policies on each unit basis in DFI.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.