
Abstract
Background
Early identification of diabetic foot infection (DFI) patients at risk for clinical deterioration is critical for timely intervention. Serum lactate reflects tissue hypoperfusion, whereas hypoalbuminemia indicates systemic inflammation and poor nutritional status. The aim of this study is to evaluate the ability of the lactate-to-albumin ratio (LAR) to predict ICU admission in patients with DFI.
Methods
This retrospective study was conducted in the emergency department of a tertiary care center between 01.01.2022 and 01.01.2025. Adult patients (≥18 years) with confirmed DFI were included. DFI diagnosis was established
Results
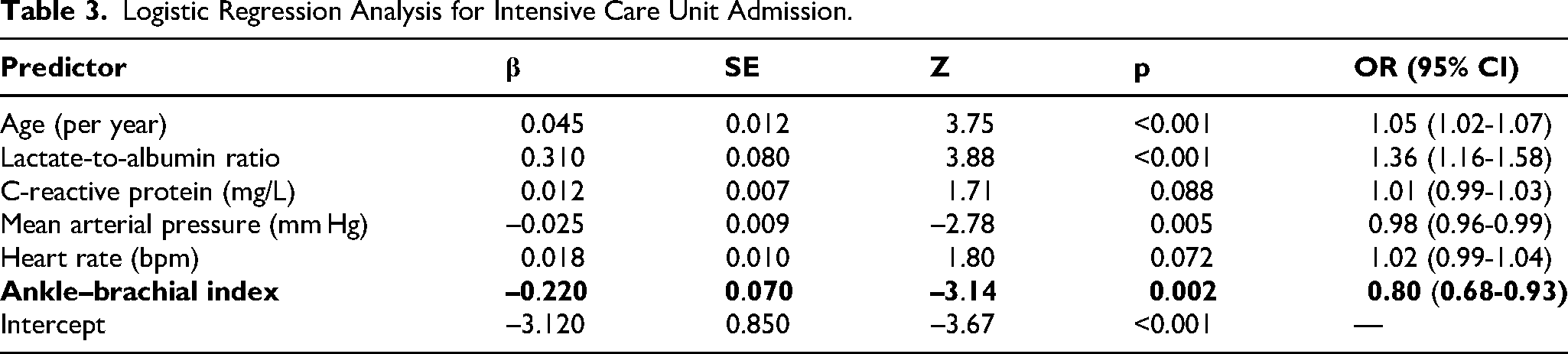
Among 494 patients (median age, 64 years; 40.3% female), 91 (18.4%) required ICU admission. ICU patients had higher lactate (2.5 vs 1.8 mmol/L, P < .001), lower albumin (3.2 vs 3.4 g/dL, P < .001), and higher LAR (0.8 vs 0.5, P < .001). LAR demonstrated the best discrimination for ICU admission (AUC, 0.717; 95% CI, 0.658-0.777), outperforming albumin (AUC, 0.626; P = .009) and similar to lactate (AUC, 0.702; P = .134). A cut-off of ≥0.73 yielded 57.1% sensitivity and 78.2% specificity. LAR (OR, 1.36; 95% CI, 1.16-1.58; P < .001), older age, lower mean arterial pressure, and lower ankle–brachial index were independent predictors of ICU admission.
Conclusions
The lactate-to-albumin ratio is a simple, cost-effective biomarker that independently predicts ICU admission in DFI patients and may aid early risk stratification. Although LAR did not demonstrate statistically superior discrimination over lactate alone, it integrates systemic metabolic stress with the host's inflammatory and nutritional reserve, offering a composite measure of physiological vulnerability in this high-risk population.
Keywords
Introduction
Early identification of critically ill patients at risk of deterioration remains a central challenge in emergency and intensive care medicine. Among routinely available biomarkers, serum lactate is widely recognized as a marker of tissue hypoperfusion, impaired oxygen utilization, and anaerobic metabolism.2–4 Elevated lactate levels are independently associated with mortality in a broad spectrum of acute illnesses, including sepsis, septic shock, community-acquired pneumonia, and acute heart failure. However, lactate concentrations may also rise due to non-hypoxic mechanisms such as adrenergic stimulation or impaired clearance, which can limit its specificity as a prognostic marker.5–7
Serum albumin, on the other hand, is a negative acute-phase reactant whose decline reflects systemic inflammation, increased vascular permeability, and poor nutritional status. Hypoalbuminemia has been associated with worse outcomes in critically ill patients and contributes to capillary leak, reduced oncotic pressure, and impaired drug distribution.8–10 Furthermore, low albumin levels may decrease hepatic lactate clearance, indirectly amplifying lactate accumulation during severe illness.
The lactate-to-albumin ratio (LAR) combines these two complementary pathophysiological signals — acute metabolic stress and the host's inflammatory/nutritional reserve — into a single, easily obtainable metric. Recent studies suggest that LAR predicts mortality more accurately than either biomarker alone in patients with sepsis and septic shock, community-acquired pneumonia, and other critical conditions.11–13 By integrating metabolic and inflammatory pathways, LAR may provide a more robust assessment of disease severity and guide early resuscitative interventions.
Diabetic foot infection (DFI) patients carry a particularly high risk of systemic deterioration: sepsis has been reported in approximately 9.6% of DFI-related emergency department presentations, with mortality and amputation rates each exceeding 10%. 14 Furthermore, patients with diabetic foot ulcers face markedly elevated risks of sepsis-related organ dysfunction compared with non-diabetic populations, 15 making early risk stratification at the time of ED presentation critical.
Despite these promising findings, data on the prognostic performance of LAR in patients with diabetic foot infection remain limited. The present study was therefore designed to evaluate the ability of LAR to predict ICU admission in this population.
Methods
Study Design and Setting
This retrospective observational study was conducted at the Emergency Department (ED) of a training and research hospital, a tertiary care center with an annual census of approximately 280,000 patient visits. 16 The study period extended from 01.01.2022 to 01.01.2025. The institutional ethics committee approved and waived the requirement for informed consent because of the noninterventional design and anonymized data analysis. All diagnostic accuracy results were reported in compliance with the STARD guidelines (16). The study was conducted as a collaboration between the Emergency Medicine and Orthopaedics and Traumatology departments; an orthopaedic surgeon was involved in the clinical evaluation and data verification process throughout the study period.
Study Population
Adult patients (≥18 years) who presented to the ED during the study period and had both serum lactate and serum albumin levels measured within the first hour of admission were eligible. Patients were included if they were diagnosed with diabetic foot infection based on clinical and laboratory parameters, in accordance with IWGDF/IDSA 2023 criteria. 1 Exclusion criteria were: (1) missing or delayed laboratory measurements, (2) transfer from another facility with incomplete records, (3) known chronic liver failure, nephrotic syndrome, or other conditions causing baseline hypoalbuminemia, and (4) pregnancy.
Data Collection
Demographic data (age, sex), comorbidities, vital signs at ED presentation, and laboratory parameters (lactate, albumin, complete blood count, creatinine, C-reactive protein, etc) were extracted from the electronic medical record system. LAR was calculated by dividing serum lactate (mmol/L) by serum albumin (g/dL) obtained at ED arrival. Wound severity was graded according to the Wagner classification and recorded for all patients. Clinical outcome — ICU admission — was recorded as the primary endpoint. Wagner grade assignment and wound morphology were independently verified by a consultant orthopaedic surgeon, who also confirmed the accuracy of DFI diagnosis and the presence or absence of surgical indications for each patient. Discrepancies between the emergency physician's initial wound assessment and the orthopaedic review were resolved by consensus.
Outcome Definition
The primary outcome was direct ICU admission from the emergency department, determined at initial triage and disposition by the treating emergency physician and intensivist based on clinical severity criteria including hemodynamic instability, respiratory compromise, altered mental status, or failure to respond to initial ED resuscitation. In cases where surgical urgency was a factor in the disposition decision — such as the presence of necrotizing infection or limb-threatening ischaemia — the orthopaedic surgeon was consulted and contributed to the decision regarding the level of care required. Patients initially admitted to a general ward who were subsequently transferred to the ICU during hospitalization were not included in the ICU admission group, as the focus of this study was on early risk stratification at ED presentation.
Statistical Analysis
Continuous variables were expressed as mean ± SD or median with IQR depending on distribution, and categorical variables as counts and percentages. Group comparisons were performed using the independent samples t-test or Brunner–Munzel test for continuous variables 17 and the chi-square or Fisher's exact test for categorical variables. ROC curve analysis was used to assess the discriminatory ability of LAR and to identify optimal cut-off values using the Youden index. Pairwise AUC comparisons were performed using DeLong's test. Variables with p < 0.10 in univariate analysis were entered into a multivariable logistic regression model; results were expressed as ORs with 95% CIs. Variance inflation factors (VIF) were examined to assess multicollinearity among model predictors. Prediction model development and reporting followed TRIPOD guidance. 18 A two-tailed p value <0.05 was considered statistically significant. Statistical analyses were performed using Jamovi software, version 2.6.26.0.
Results
Baseline Characteristics
A total of 494 patients were included, of whom 91 (18.4%) required direct ICU admission from the emergency department. ICU patients were older (median age 66.0 vs 64.0 years; P = .008), had higher lactate (2.5 vs 1.8 mmol/L, P < .001), higher LAR (0.8 vs 0.5, P < .001), and lower albumin (3.2 vs 3.4 g/dL; P < .001). Systolic and diastolic blood pressures, peripheral oxygen saturation, ankle–brachial index, heart rate, and respiratory rate also differed significantly (all P < .01). Importantly, Wagner grade distribution and surgical intervention rates did not differ significantly between ICU and non-ICU groups (P = .828 and P = .462, respectively), nor did inflammatory markers including C-reactive protein and systemic immune-inflammation index. This pattern indicates that systemic physiological parameters, rather than local wound severity indices, were the primary drivers of ICU triage decisions in this cohort. Other comorbidities and laboratory parameters did not differ significantly between groups (Table 1).
Baseline Characteristics (Unchanged).
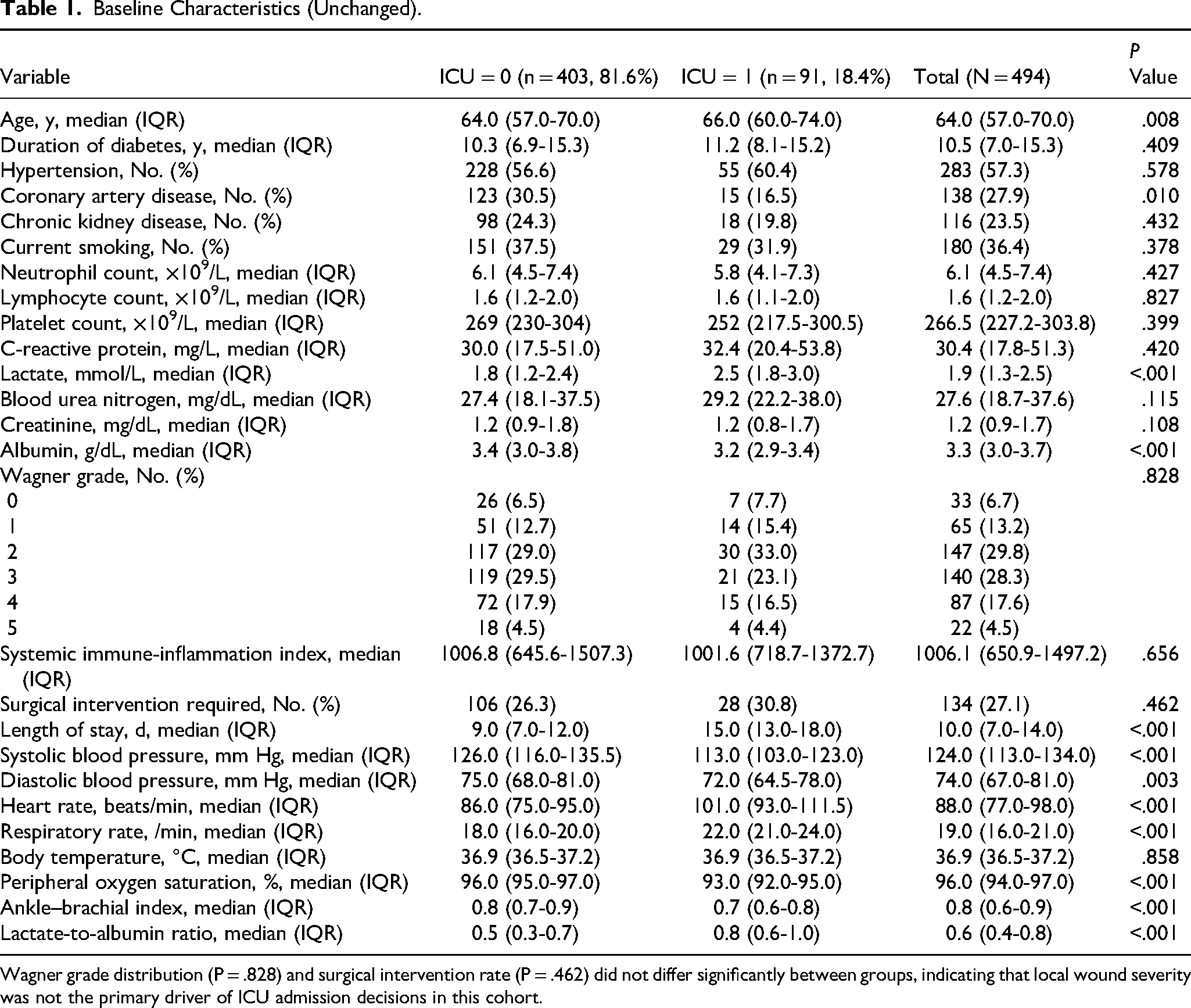
Wagner grade distribution (P = .828) and surgical intervention rate (P = .462) did not differ significantly between groups, indicating that local wound severity was not the primary driver of ICU admission decisions in this cohort.
Diagnostic Performance of LAR, Albumin, and Lactate
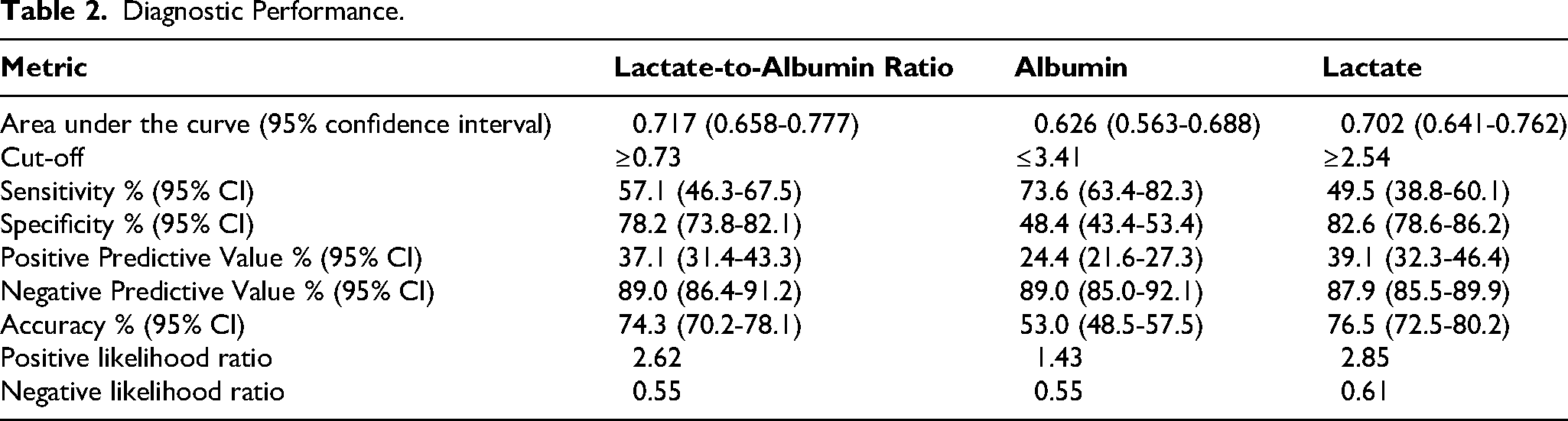
ROC curve analysis demonstrated that LAR had an AUC of 0.717 (95% CI, 0.658-0.777; P < .001). The AUCs for albumin and lactate were 0.626 (95% CI, 0.563-0.688; P < .001) and 0.702 (95% CI, 0.641-0.762; P < .001), respectively. Optimal cut-off values by Youden's index were ≥0.73 for LAR, ≤3.41 g/dL for albumin, and ≥2.54 mmol/L for lactate. At these thresholds, LAR showed sensitivity 57.1%, specificity 78.2%, positive predictive value 37.1%, negative predictive value 89.0%, and accuracy 74.3% (Table 2). Pairwise DeLong comparisons indicated that LAR had significantly better discriminative ability than albumin (AUC difference=0.091; P = .009), whereas the difference between LAR and lactate was not statistically significant (AUC difference=0.015; P = .134). Therefore, the incremental diagnostic utility of LAR over lactate alone, in terms of AUC, was modest and non-significant in this cohort.
Diagnostic Performance.
Multivariable Logistic Regression Analysis
Logistic Regression Analysis for Intensive Care Unit Admission.
Discussion
In this retrospective cohort of patients admitted with diabetic foot infection, we demonstrated that the lactate-to-albumin ratio is an independent predictor of ICU admission. Although both serum lactate and albumin individually showed significant associations with disease severity, their combined ratio provided superior discriminative ability compared with albumin alone and comparable performance to lactate. Importantly, LAR remained independently associated with ICU admission even after adjustment for age, mean arterial pressure, and ankle–brachial index.
An important observation from our data is that differences between ICU and non-ICU patients were predominantly driven by systemic physiological parameters — blood pressure, heart rate, respiratory rate, oxygen saturation, and lactate — rather than by local DFI severity indicators such as Wagner grade, inflammatory markers (CRP, systemic immune-inflammation index), or surgical intervention rates. This finding suggests that LAR, as a composite of systemic metabolic and nutritional markers, functions primarily as a marker of global physiological instability rather than a DFI-specific severity index. Clinicians should therefore interpret LAR in this context: it reflects the host's systemic response to infection and physiological reserve, rather than the direct severity of the foot wound itself. This is consistent with the known pathophysiology of LAR in sepsis and other systemic conditions, where it captures the interplay between acute metabolic decompensation and impaired host defense capacity.6,19,20 Indeed, LAR has been shown to correlate strongly with SOFA score and to serve as an independent predictor of ICU admission across heterogeneous critically ill populations. 21
Previous research has consistently shown that elevated serum lactate reflects tissue hypoperfusion, anaerobic metabolism, and compromised mitochondrial function.22,23 Albumin, beyond its nutritional role, is a negative acute-phase reactant capturing a complex interplay of systemic inflammation, capillary leak, dilutional effects, and decreased hepatic synthesis. When combined into the LAR, the resulting metric incorporates both rapid-onset metabolic derangement and the patient's baseline inflammatory/nutritional reserve.
Several large studies support this concept. Yoon et al in a systematic review and meta-analysis of 4723 patients with sepsis or septic shock reported pooled sensitivity ∼0.71 and specificity ∼0.68 for mortality, with an overall AUC of ∼0.74. 19 In another study of sepsis patients admitted to ICU (n≈1136), LAR (cut-off >0.71) showed stronger discriminative power for mortality (AUC ∼0.869) compared to albumin or lactate alone. 20 In the setting of community-acquired pneumonia, Hancı et al demonstrated that LAR was comparable to established severity scores (PSI, CURB-65, qSOFA) in predicting both ICU admission and mortality. 10 Furthermore, in a prospective study of patients with sepsis and acute respiratory failure, LAR was non-inferior to SOFA and APACHE-II in predicting in-hospital outcomes and mechanical ventilation requirement. 24 Moreover, in patients with sepsis-associated acute kidney injury, elevated LAR was associated with significantly increased 30-day and 90-day mortality risks. 25
Regarding the incremental value of LAR over lactate alone: in our study, the AUC of LAR (0.717) was numerically higher but not statistically significantly different from lactate alone (0.702; DeLong p = .134). This finding should be acknowledged as a key limitation. The clinical rationale for LAR rests on its ability to contextualize acute metabolic stress within the patient's inflammatory and nutritional reserve — particularly relevant in DFI patients who may have chronic hypoalbuminemia from prolonged infection or malnutrition. Nonetheless, statistical superiority over lactate alone was not demonstrated in this cohort, and future adequately powered studies will be needed to establish meaningful additive predictive value. Of note, serum albumin has been shown to improve 30-day mortality prediction beyond the SOFA score alone in ED patients with infections, 26 providing indirect support for the conceptual basis of LAR as a composite marker.
Our results also highlight the role of ankle–brachial index as an independent predictor of ICU admission. Peripheral arterial disease is a key contributor to the pathogenesis and severity of diabetic foot infection, and lower ABI values reflect impaired limb perfusion and higher risk of tissue necrosis, potentially necessitating more intensive monitoring.27,28 Conversely, higher mean arterial pressure was protective, consistent with previous data linking hypotension to worse outcomes in DFI and sepsis.
This study has several limitations. First, its retrospective design may introduce selection bias and limit causal inference. Second, lactate and albumin measurements were obtained at a single time point; dynamic changes during hospitalization were not evaluated. Third, our findings are derived from a single center. Fourth, the multivariable model was not internally validated (eg, by bootstrapping or cross-validation), and the high model AUC (0.973) likely reflects overfitting given the limited outcome events relative to model complexity 18 ; external prospective validation is therefore essential before clinical implementation. Fifth, the study did not capture subsequent ICU transfers from the general ward. Sixth, DFI-specific severity markers (Wagner grade, inflammatory indices) did not differ significantly between groups, limiting conclusions about LAR as a DFI-specific prognostic tool. Despite these limitations, the large sample size and standardized data collection strengthen the validity of our descriptive findings.
Conclusion
The LAR is an easily obtainable and inexpensive biomarker that demonstrates good discriminative performance for predicting ICU admission in patients with diabetic foot infection. Although its discriminative ability was not statistically superior to lactate alone, LAR integrates systemic metabolic stress with the host's inflammatory and nutritional reserve, offering a composite measure of physiological vulnerability. Incorporating this ratio into routine assessment may facilitate early risk stratification and guide timely interventions. Prospective multicenter studies with internal and external validation are warranted to confirm these findings and explore whether LAR-guided management strategies can improve outcomes in this high-risk population.
Footnotes
Acknowledgments
The authors thank the emergency department staff for their contribution to patient management and data recording.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the institutional ethics committee (Approval No: 2025/153). The requirement for informed consent was waived due to the retrospective and anonymized design.
Consent for Publication
Not applicable.
Author Contributions
K.Y.: Conceptualization, methodology, formal analysis, data curation, writing—original draft.
O.Y.: Investigation, validation, writing—review and editing.
All authors have read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.