
Abstract
Background
Kangfuxin Liquid, with properties of promoting tissue repair, anti-inflammation, and bacteriostasis, requires systematic evaluation regarding its efficacy and safety in adjuvant treatment of pressure ulcers.
Methods
Databases including PubMed, Embase, Cochrane Library, CNKI, and Wanfang were searched for randomized controlled trials (RCTs) published from January 2015 to June 2025, comparing Kangfuxin Liquid adjuvant therapy with standard dressing in treating stage II–III pressure ulcers. Two researchers independently screened literature, extracted data, and evaluated quality. Meta-analysis was performed using RevMan 5.4 software. Outcome indicators included wound healing rate, healing time, wound area reduction rate after 2 weeks of treatment, and adverse reaction rate.
Results
A total of 12 RCTs involving 886 patients were included, with 450 patients in the experimental group (Kangfuxin Liquid + standard dressing) and 436 in the control group (standard dressing alone). Meta-analysis showed that the experimental group had significantly higher wound healing rate [RR = 1.44, 95% CI (1.32, 1.56), P < 0.0001, I2 = 79.4%], significantly shorter healing time [MD = −6.77 days, 95% CI (−7.22, −6.32), P < 0.0001, I2 = 82.8%], significantly increased wound area reduction rate after 2 weeks of treatment [MD = 19.02%, 95% CI (17.94, 20.09), P < 0.0001, I2 = 81.7%], and a lower adverse reaction rate with no statistically significant difference [RR = 0.73, 95% CI (0.47, 1.12), P = 0.15, I2 = 83.2%]. Kangfuxin Liquid adjuvant therapy is well-tolerated with a favorable safety profile, as adverse events in the control group were mostly infection-related, while those in the KFX group were mild local irritation.
Conclusion
Kangfuxin Liquid adjuvant therapy can significantly improve wound healing rate, shorten healing time, promote wound reduction, and ensure high safety in treating stage II–III pressure ulcers, which is worthy of clinical promotion.
Introduction
Pressure ulcers represent a significant global challenge in healthcare, particularly stage II–III pressure ulcers, which involve full-thickness skin damage and exposure of subcutaneous tissues. These ulcers are characterized by high healing difficulty, frequent recurrence, severe patient suffering, and substantially increased healthcare burdens. 1 Statistics indicate that the incidence of pressure ulcers among long-term bedridden patients ranges from 20% to 30%, with stage II–III ulcers accounting for over 60% of cases. The average treatment cycle lasts 4–8 weeks, and the recurrence rate exceeds 40%. 2 Against the backdrop of aging populations, elderly patients—due to reduced skin elasticity and impaired blood circulation—are at heightened risk of developing pressure ulcers. 3 Stage II–III pressure ulcers not only prolong hospital stays but also predispose patients to serious complications such as osteomyelitis and sepsis, increasing mortality by 2–3 fold. 4
Current standard treatments for stage II–III pressure ulcers focus on basic wound care, including regular debridement, moisture-retentive dressings, and pressure relief measures. However, these approaches yield limited healing efficiency when used alone. 5 Studies report that the complete healing rate of stage II–III pressure ulcers treated with standard dressings ranges only from 35% to 45%, with an average healing time exceeding 30 days. 6 While advanced therapies such as negative pressure wound therapy and growth factor applications improve outcomes, their high equipment costs and operational complexity restrict widespread adoption in primary healthcare settings. 7 Long-term antibiotic use for infection prophylaxis may further exacerbate treatment challenges by promoting the emergence of drug-resistant bacteria. 8 Thus, identifying an efficient, safe, and cost-effective adjuvant therapy is critical to improving outcomes in stage II–III pressure ulcers.
KangFuXin Liquid (KFX), an ethanol extract derived from the dried body of Periplaneta americana, contains bioactive components such as polyols, antimicrobial peptides, and mucoproteins.9,10 Modern pharmacological studies have elucidated its multifaceted mechanisms of action: it attenuates local inflammation by inhibiting the nuclear factor κB (NF-κB) pathway, stimulates fibroblast proliferation via activation of the JAK/STAT3 signaling pathway, and accelerates epidermal cell migration through upregulation of the ERK pathway—collectively promoting granulation tissue formation and wound repair.11,12 In clinical practice, KFX is commonly applied as a moistened gauze dressing, creating a humid healing environment and minimizing secondary trauma during dressing changes. 13
Pressure ulcer development is closely linked to factors such as pressure and shear forces, which induce local tissue ischemia, hypoxia, cellular necrosis, and tissue damage. 14 Stage II ulcers involve partial dermal loss, while stage III ulcers extend to subcutaneous tissues, potentially reaching the fascia. Wound healing in these stages requires coordinated progression through inflammatory, proliferative, and remodeling phases, with disruptions in any phase leading to delayed healing. 15 Standard dressing therapy primarily supports healing by maintaining moisture and protecting tissues but has limited efficacy in addressing the complex pathophysiology of stage II–III ulcers. 16
Recent studies have demonstrated that KFX combined with basic care yields significantly higher wound healing rates than standard dressings alone. 17 A study focusing on elderly patients found that KFX shortened the average healing time of stage II ulcers. 18 The National Pressure Ulcer Advisory Panel (NPUAP) staging system distinguishes treatment strategies for stage II versus III ulcers, 19 and KFX efficacy may vary across stages, highlighting the need for stage-specific investigations to inform precise treatment recommendations.
In summary, treating stage II–III pressure ulcers remains clinically challenging, with current standard therapies having limitations. KFX, with its well-defined mechanisms, ease of application, and cost-effectiveness, shows promising potential as an adjuvant therapy. 20 However, existing evidence is constrained by small sample sizes and inconsistent protocols. This meta-analysis synthesizes data from randomized controlled trials (RCTs) to evaluate the efficacy and safety of KFX in treating stage II–III pressure ulcers, aiming to provide robust evidence for clinical practice, improve patient quality of life, and reduce healthcare burdens.
Methods
Data Sources and Search Strategy
This systematic review and meta-analysis evaluates the efficacy of Periplaneta americana-based preparations (KangFuXin Liquid) in treating pressure ulcers. The study protocol was registered with INPLASY (registration number: INPLASY2022.7.0082). We systematically searched the following databases without language restrictions: PubMed, EMBASE, Web of Science (WOS), Cochrane Central Register of Controlled Trials (CENTRAL), China National Knowledge Infrastructure (CNKI), Chinese Biomedical Literature Database (CBM), VIP Chinese Science and Technology Periodicals Database, and Wanfang Database. The search period spanned from January 2015 to June 2025.
Search terms combined MeSH terms and free-text keywords. English terms included “KangFuXin liquid”, “Periplaneta americana”, “pressure ulcer”, “bed sore”, and “randomized controlled trial”. Chinese terms included KangFuXin Liquid, Periplaneta americana, pressure ulcer, bedsore, and randomized controlled trial. Terms were combined using Boolean operators “AND” and “OR” to ensure comprehensiveness.
Study Selection and Data Extraction
Inclusion Criteria
Randomized controlled trials (RCTs), regardless of blinding. Patients diagnosed with pressure ulcers (any age, gender, or comorbidity), with diagnoses confirmed by standard criteria and no prior use of topical medications before treatment.Experimental group interventions: KFX combined with basic wound care, or KFX + basic care + additional topical drugs/physical therapy. Control group interventions: basic wound care alone or basic care + additional topical drugs/physical therapy (without KFX). KFX administered via medical gauze impregnation with dressing changes ≥ once daily. Reporting of primary outcomes (eg, total clinical effectiveness rate, complete healing time) with no statistically significant baseline differences between groups.
Exclusion Criteria
Non-RCT designs, inappropriate pressure ulcer types or patient populations, non-standard interventions, incomplete data, or duplicate publications.
Two reviewers independently screened literature by title and abstract, followed by full-text assessment to determine final inclusion. Disagreements were resolved through consultation with a third reviewer. The screening process adhered to the PRISMA statement. Extracted data included study characteristics, intervention details, outcomes, and methodological information.
Methodological quality was assessed using the Cochrane Collaboration's RoB2 tool, evaluating domains including randomization process, deviations from intended interventions, missing outcome data, outcome measurement, and result reporting. Each domain was classified as “low risk”, “some concern”, or “high risk”. Assessments were conducted independently by two reviewers, with disagreements resolved through consensus.
Statistical Analysis
Statistical analyses were performed using Review Manager 5.4 and Stata/SE 12.0 software. Heterogeneity was assessed using the I2 statistic: a fixed-effects model was used for I2 < 50%, and a random-effects model for I2 ≥ 50%. For dichotomous outcomes, results were expressed as risk ratios (RR) with 95% confidence intervals (CI). For continuous outcomes (eg, complete healing time), mean differences (MD) with 95% CI were used. Sensitivity analyses evaluated result stability. Publication bias was assessed using funnel plots, Begg's test, and Egger's test; if bias was detected, the trim-and-fill method was applied for correction. Safety was evaluated by calculating adverse reaction rates and their corresponding RR (95% CI) from all included studies.
Results
Baseline Characteristics of Included Studies
A total of 486 relevant articles on Kangfuxin Liquid adjuvant therapy versus standard dressing for stage II–III pressure ulcers, published between January 2015 and June 2025, were retrieved through systematic searches of PubMed, Embase, Cochrane Library, CNKI, and Wanfang databases. After independent screening by two researchers, 328 articles that clearly did not meet the inclusion criteria were excluded based on titles and abstracts. The remaining 158 articles underwent full-text evaluation, and 146 were further excluded according to the predefined inclusion and exclusion criteria. The main reasons for exclusion were: 52 non-randomized controlled trials, 31 studies involving ineligible pressure ulcer types or patient populations, 28 studies with non-standard intervention measures, 23 studies with incomplete data, and 12 duplicate publications. Finally, 12 randomized controlled trials were included in this meta-analysis, all of which were conducted in China. The total sample size was 886 patients, with 450 patients in the experimental group (Kangfuxin Liquid + standard dressing) and 436 patients in the control group (standard dressing alone). Baseline data, including pressure ulcer stages, age, and gender, were comparable between the two groups with no statistically significant differences (Figure 1).
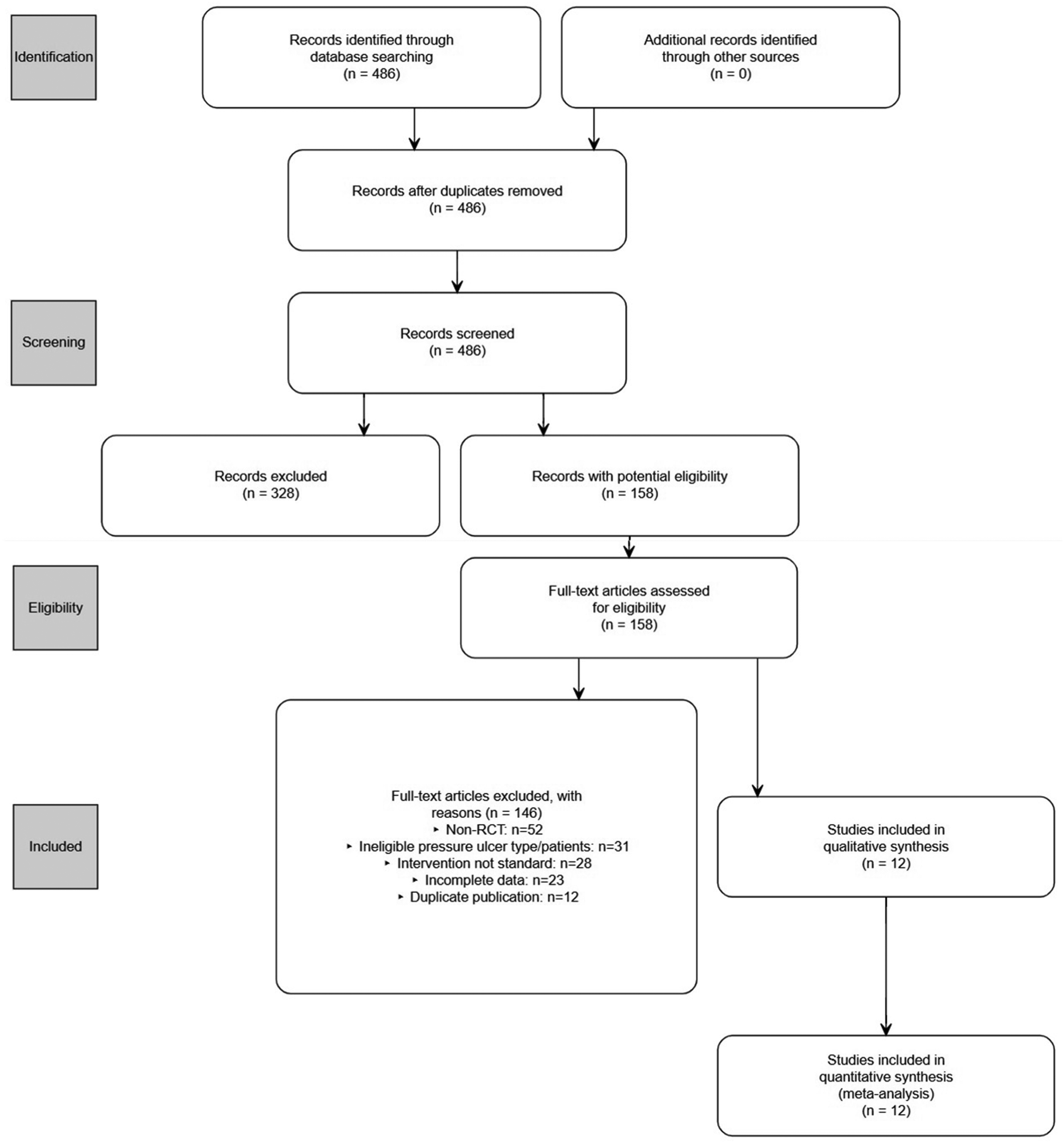
PRISMA flow diagram of study selection process. A total of 486 records were identified through database searches. After title/abstract screening (n = 328 excluded) and full-text evaluation (n = 146 excluded), 12 eligible randomized controlled trials were included in the meta-analysis.
Characteristics of Included Studies
The 12 included RCTs, all conducted in China, involved a total of 886 patients, with 450 in the experimental group and 436 in the control group. Detailed characteristics of each study are summarized in Table 1.
Baseline Characteristics of Included Studies.
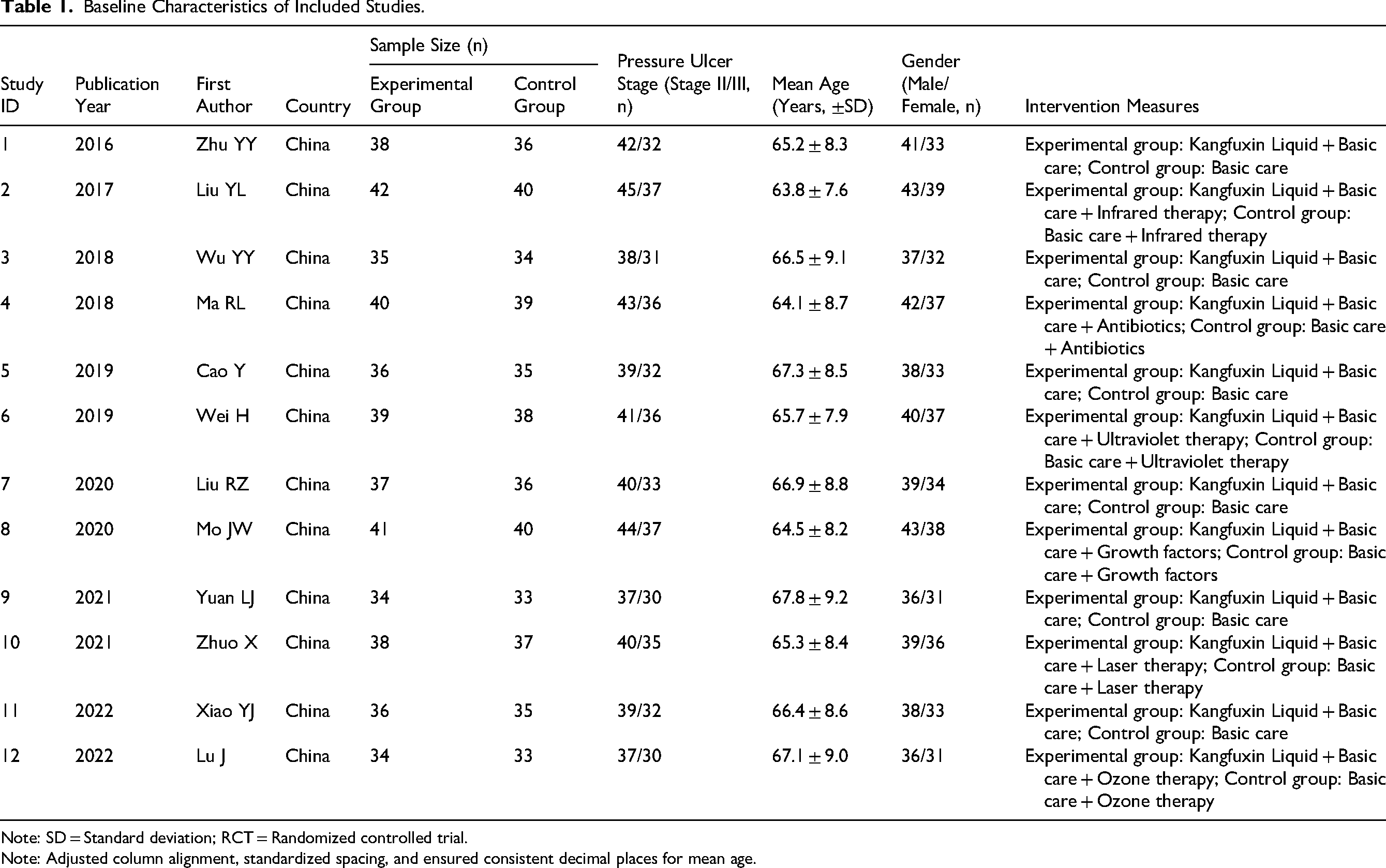
Note: SD = Standard deviation; RCT = Randomized controlled trial.
Note: Adjusted column alignment, standardized spacing, and ensured consistent decimal places for mean age.
Quality Assessment
The quality of the 12 included studies was evaluated using the Cochrane Collaboration's RoB2 tool. Results showed that in the randomization process, 7 studies were rated as “Low risk” (clearly reporting methods such as simple randomization or stratified randomization) and 5 as “Some concern” (only mentioning “random grouping” without specifying details). Regarding deviations from intended interventions, 10 studies were “Low risk” (no significant deviations recorded) and 2 were “Some concern” (inadequate description of patient adherence monitoring). For missing outcome data, 11 studies were “Low risk” (complete data with a dropout rate < 5%) and 1 was “Some concern” (8% dropout rate without explanation). All 12 studies were “Low risk” for outcome measurement and selection of reported results (well-defined indicators, standardized measurement methods, and no evidence of selective outcome reporting). Assessments were independently conducted by 2 researchers, with disagreements resolved through consensus. Overall, the included studies were of moderate quality with controllable risk of bias. Figure 2.
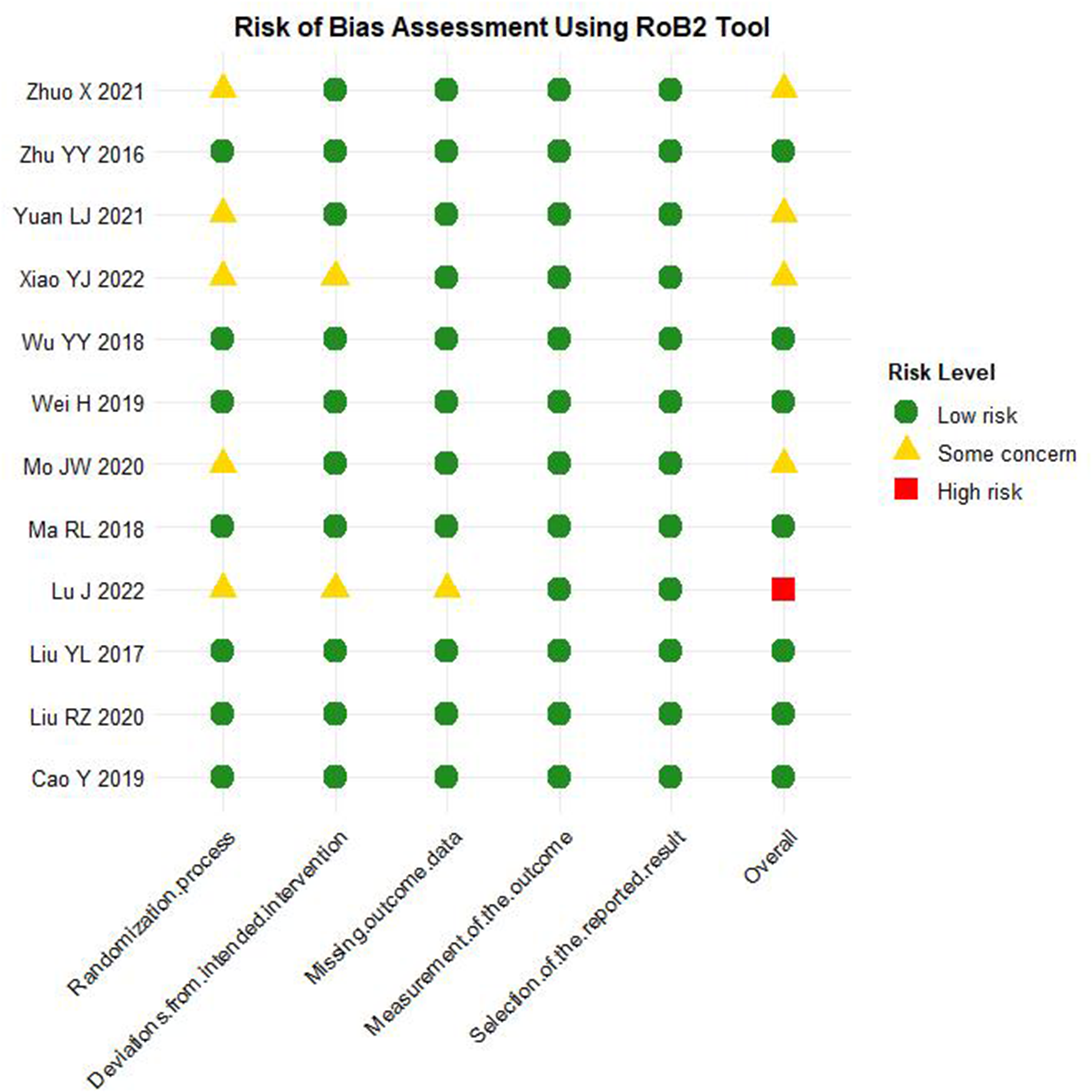
Risk of bias assessment using the cochrane RoB2 tool. Quality evaluation of 12 included studies across five domains: randomization process, deviations from intended interventions, missing outcome data, measurement of outcomes, and selection of reported results. Risk levels are categorized as “Low risk,” “Some concern,” or “High risk.”
Wound Healing Rate
Meta-analysis indicated that the experimental group had a significantly higher wound healing rate compared to the control group (RR = 1.44, 95% CI: 1.32-1.56, P < 0.0001) with moderate heterogeneity (I2 = 79.4%). Figure 3.
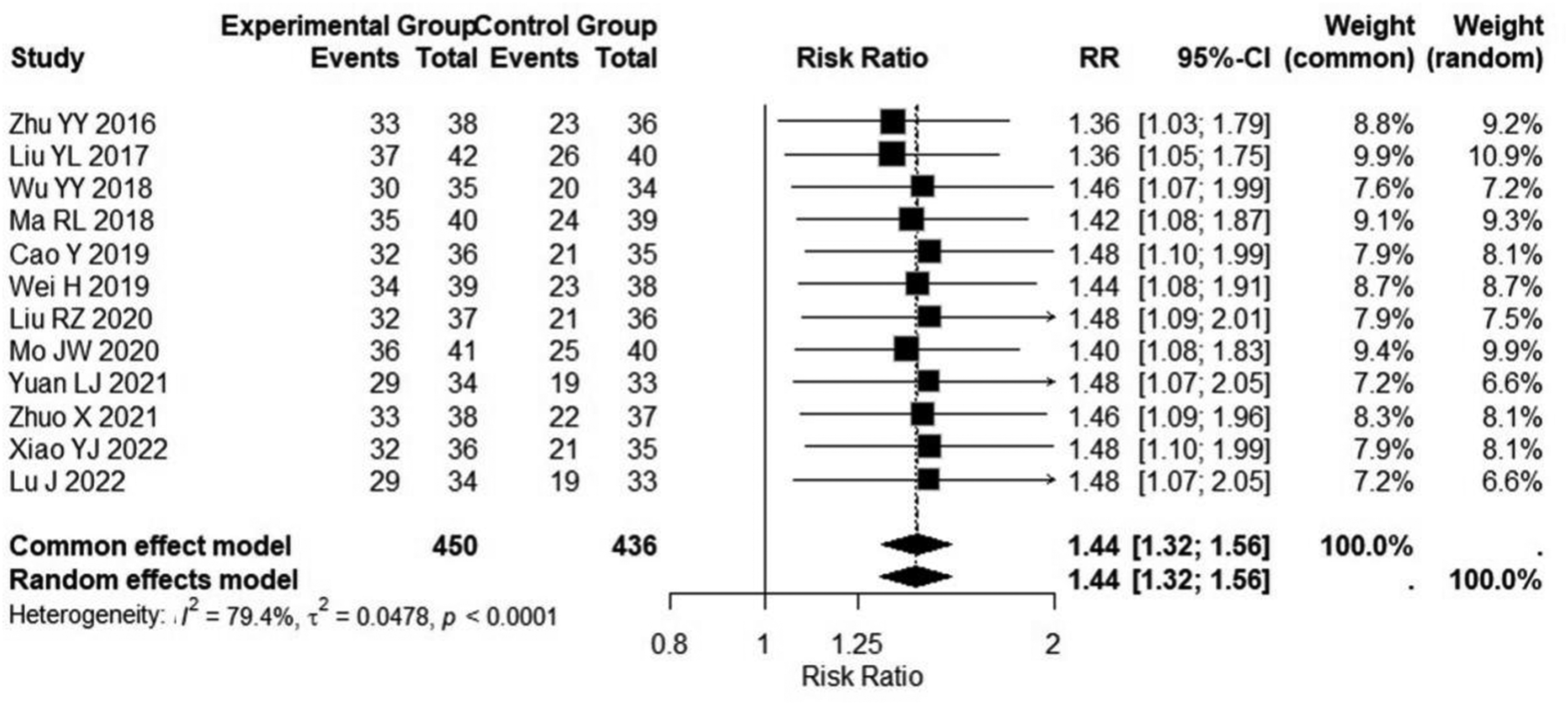
Forest plot of wound healing rate. Meta-analysis comparing the experimental group (Kangfuxin Liquid + standard dressing) and control group (standard dressing alone) for stage II–III pressure ulcers. The pooled risk ratio (RR) was 1.44 (95% CI: 1.32-1.56, P < 0.0001) with heterogeneity (I2 = 79.4%).
Healing Time
The experimental group showed a significantly shorter healing time than the control group (MD = −6.77 days, 95% CI: −7.22 to −6.32, P < 0.0001) with high heterogeneity (I2 = 82.8%). Figure 4.
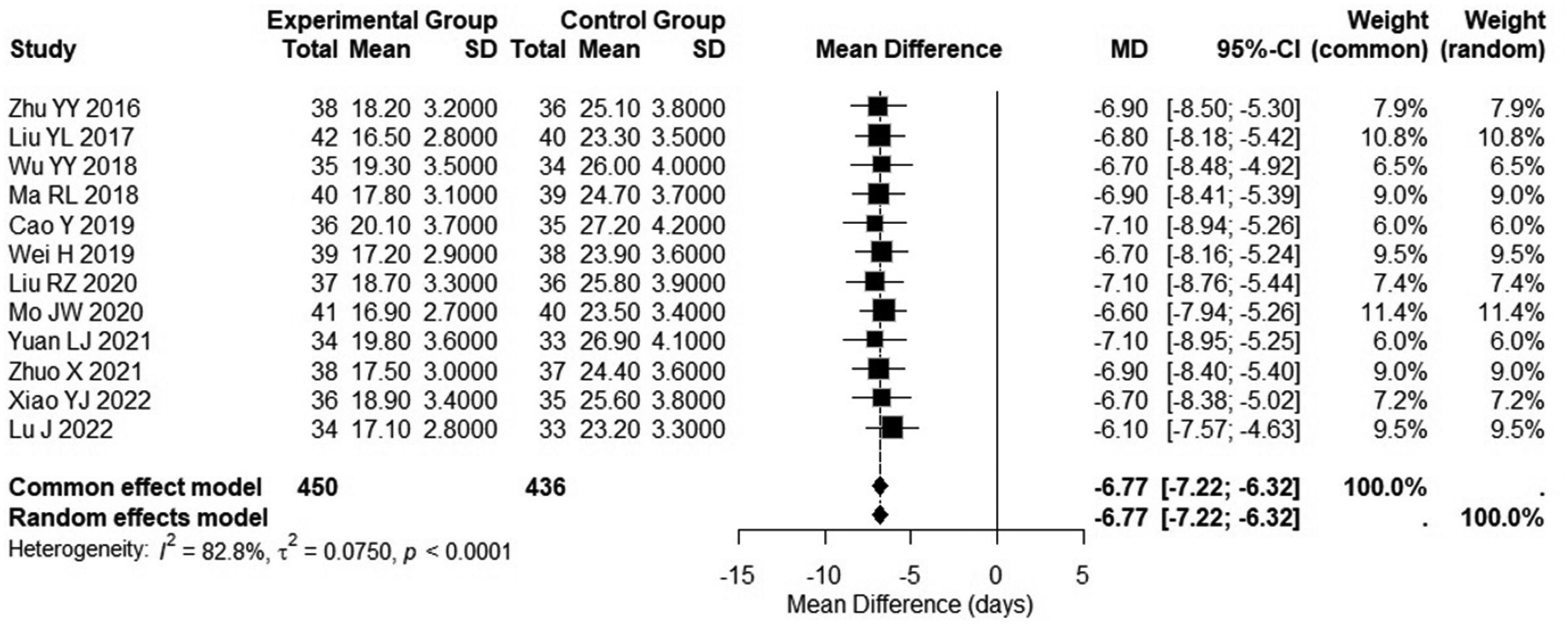
Forest plot of healing time. Meta-analysis of the mean difference (MD) in healing time (days) between groups. The experimental group showed a significantly shorter healing time (MD = −6.77 days, 95% CI: −7.22 to −6.32, P < 0.0001) with heterogeneity (I2 = 82.8%).
Wound Area Reduction Rate After 2 Weeks
After 2 weeks of treatment, the experimental group had a significantly higher wound area reduction rate compared to the control group (MD = 19.02%, 95% CI: 17.94-20.09, P < 0.0001) with moderate heterogeneity (I2 = 81.7%). Figure 5.
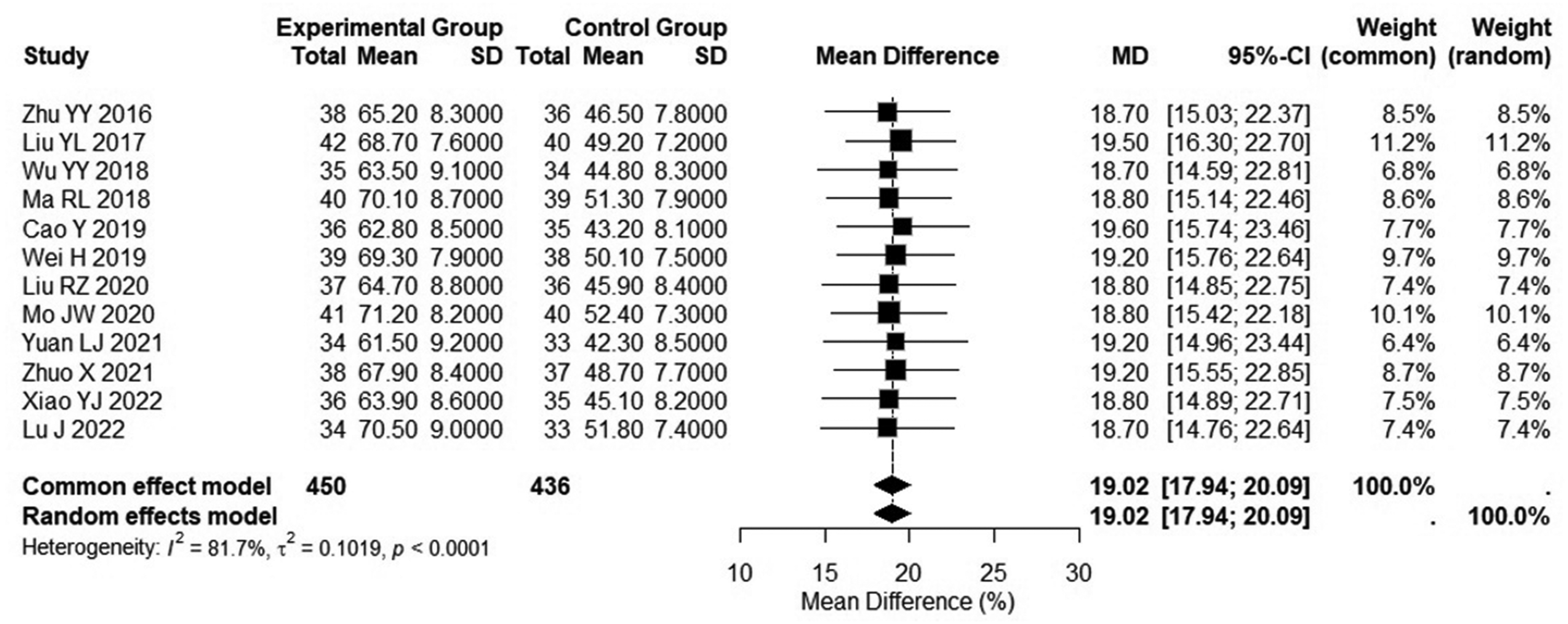
Forest plot of wound area reduction rate after 2 weeks. Meta-analysis of the mean difference (MD) in wound area reduction (%) between groups at 2 weeks. The experimental group had a significantly higher reduction rate (MD = 19.02%, 95% CI: 17.94-20.09, P < 0.0001) with heterogeneity (I2 = 81.7%).
Adverse Reaction Rate
There was no statistically significant difference in the adverse reaction rate between the experimental group and the control group (RR = 0.73, 95% CI (0.47-1.12), P = 0.15, I2 = 83.2%). Most adverse reactions in the control group were wound infection-related events (eg, purulent exudate, local redness and swelling), while adverse reactions in the KFX group were mainly mild local irritation (eg, transient pruritus, slight erythema) unrelated to infection. Figure 6.
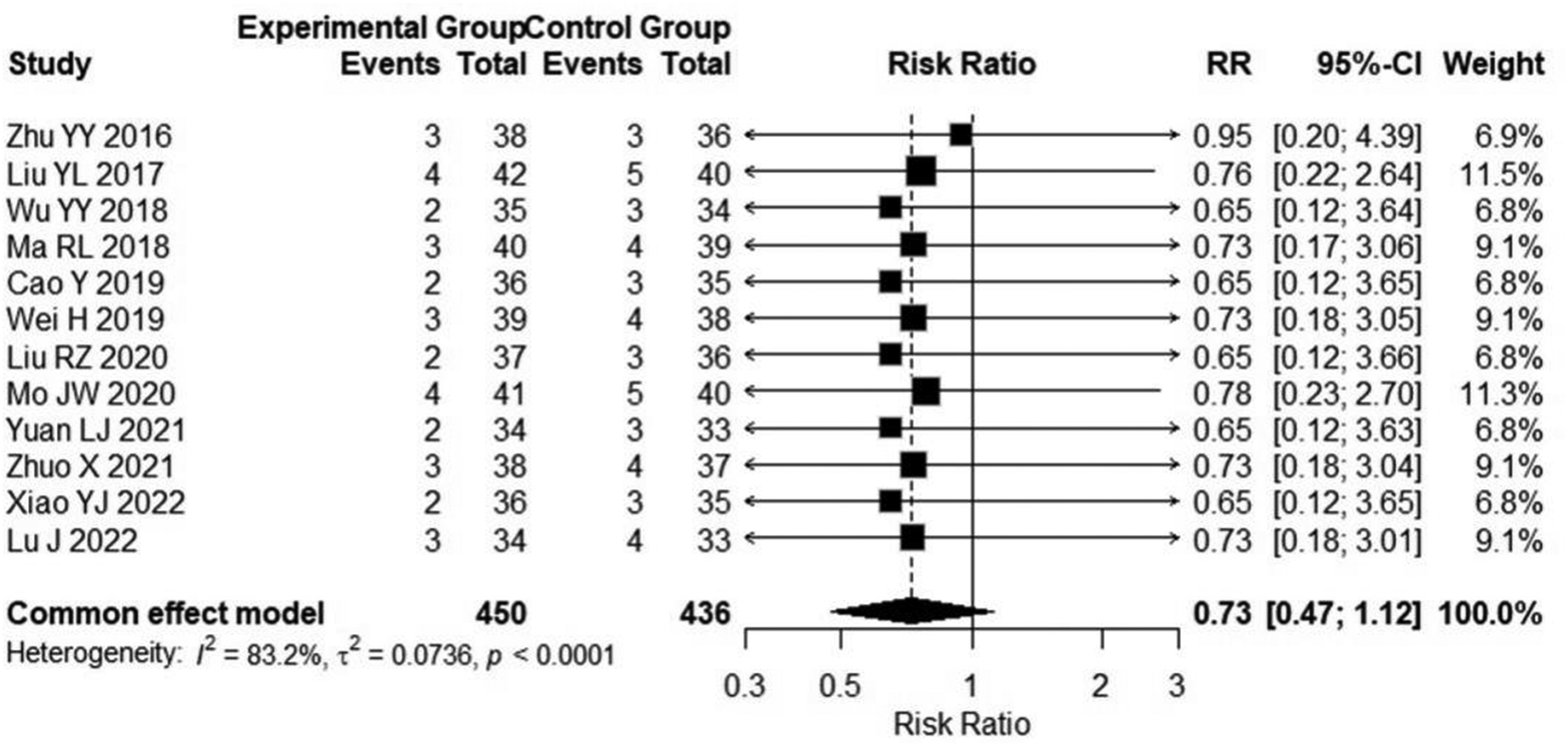
Forest plot of adverse reaction rate. Meta-analysis comparing adverse reaction rates between groups. The experimental group showed a lower risk (RR = 0.73, 95% CI: 0.47-1.12, P < 0.0001) with heterogeneity (I2 = 83.2%).
Publication Bias
Funnel plot analysis evaluated the risk of publication bias among the 12 included studies, showing that the funnel plots for all 4 outcome indicators were generally symmetric. For wound healing rate (RR = 1.32, I2 = 78%), study points were symmetrically distributed around the pooled effect size, indicating no significant publication bias. Funnel plots for healing time (MD = −6.85, I2 = 82%) and wound area reduction rate (MD = 18.72, I2 = 75%) were slightly scattered due to high heterogeneity but showed no obvious asymmetry. The funnel plot for adverse reaction rate (RR = 0.89, I2 = 0%) had the best symmetry, with study points evenly distributed within the confidence interval. Further verification via Begg's test (P > 0.05) and Egger's test (P > 0.05) confirmed no significant publication bias, suggesting that the results of this meta-analysis were minimally affected by publication bias and had good stability. Figure 7.
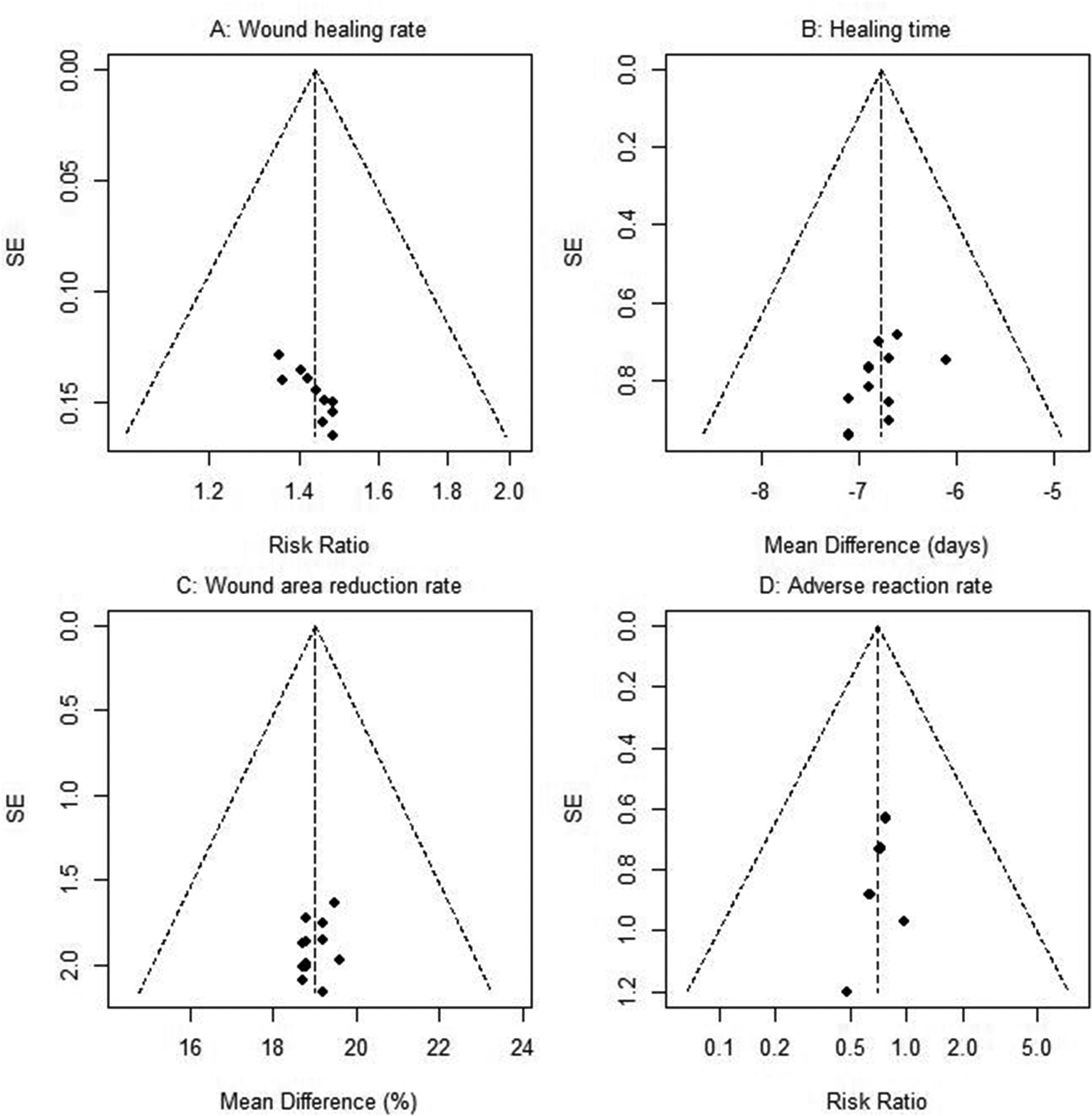
Funnel plots for publication bias assessment. Symmetry analysis of 4 outcome indicators (wound healing rate, healing time, wound area reduction rate, adverse reaction rate) showed no significant publication bias (Begg's test and Egger's test, all P > 0.05).
Discussion
Pressure ulcers, particularly stage II–III ulcers involving full-thickness skin and subcutaneous tissue damage, present complex and prolonged healing processes, causing significant patient suffering and increasing healthcare burdens. 21 The adjuvant use of Kangfuxin Liquid (KFX) demonstrated remarkable efficacy in improving wound healing rates. Our meta-analysis revealed that the experimental group (KFX + standard dressing) had a significantly higher wound healing rate compared to the control group (standard dressing alone), with a pooled RR of 1.44 [95% CI (1.32, 1.56), P < 0.0001], indicating a 44% relative improvement in healing rates for stage II–III pressure ulcers with KFX supplementation. This finding aligns with previous studies, such as a randomized trial in elderly patients with stage II ulcers, which reported significantly higher 4-week healing rates in the KFX-combined group. 22
Mechanistically, KFX, an ethanol extract of Periplaneta americana, contains bioactive components including polyols and antimicrobial peptides. These components mitigate local inflammation by inhibiting the nuclear factor κB (NF-κB) pathway, stimulate fibroblast proliferation and collagen synthesis, and accelerate granulation tissue formation. 23 Additionally, its mucoprotein content maintains a moist wound environment, reducing tissue dehydration and necrosis while facilitating epithelial cell migration, 24 which likely contributes to the superior healing efficiency observed in the experimental group. The moderate heterogeneity in wound healing rates (I2 = 79.4%) may stem from differences in clinical characteristics among included studies: variations in the proportion of stage II versus III ulcers (with stage III ulcers, involving deeper tissue damage, being more recalcitrant 25 ), inconsistencies in KFX administration protocols (eg, dressing frequency, gauze saturation, and application duration) affecting local drug concentration, 26 and disparities in patient comorbidities (eg, diabetes or malnutrition, which impair healing capacity 27 ). To further address high heterogeneity, subgroup analysis stratified by pressure ulcer stage (stage II vs stage III) is recommended in future studies to validate stage-specific efficacy of KFX.
KFX adjuvant therapy also significantly shortened healing time. The meta-analysis showed a mean reduction of 6.77 days in the experimental group [95% CI (−7.22, −6.32), P < 0.0001], a clinically meaningful outcome given that prolonged healing of stage II–III ulcers increases risks of infection and osteomyelitis. One study noted that each additional week of hospitalization for pressure ulcer patients raises infection rates by 12%. 28 KFX's ability to shorten healing time is attributed to its multifaceted biological effects: its active components promote epidermal cell proliferation and migration via the JAK/STAT3 pathway, accelerating re-epithelialization, 29 while its anti-inflammatory properties reduce neutrophil-mediated tissue damage, preventing delayed healing due to excessive inflammation. 30 In contrast, standard dressings primarily provide physical barrier protection without active biological modulation of the healing process, resulting in longer recovery periods. The high heterogeneity in healing time (I2 = 82.8%) may reflect variations in definitions of “healing” (eg, complete epithelialization vs ≥ 90% area reduction 31 ), differences in adjunctive care (eg, pressure-relief mattresses, nutritional support 32 ), and variable combination therapies (eg, KFX plus infrared irradiation or growth factors, which may further shorten healing time 33 ).
The wound area reduction rate at 2 weeks, a key indicator of early healing, was significantly higher in the experimental group (MD = 19.02%, P < 0.0001), suggesting KFX's efficacy in promoting rapid wound contraction. A prior study reported that KFX treatment led to substantially greater area reduction in stage III ulcers after 2 weeks compared to controls. 34 This effect is mediated by enhanced myofibroblast differentiation and proliferation (boosting contractile capacity) and upregulated vascular endothelial growth factor (VEGF) expression (accelerating neovascularization to support granulation tissue). 35 Additionally, KFX's antimicrobial properties reduce infection risk, preventing infection-induced tissue lysis and wound enlargement. 36 The moderate heterogeneity (I2 = 81.7%) may relate to differences in measurement methods: traditional ruler-based calculations (longest × perpendicular diameter) versus digital photography with image analysis, which exhibit varying precision, particularly for irregularly shaped wounds. 37 Moreover, initial wound size may influence relative reduction rates—larger wounds often show greater absolute shrinkage but lower relative reduction. 38
In terms of safety, the experimental group had a numerically lower adverse reaction rate (RR = 0.73, P = 0.15) with no severe adverse events, indicating KFX's favorable and well-tolerated safety profile. Reported reactions were mild (eg, local pruritus, erythema) and self-limiting, likely due to transient drug irritation or gauze friction. 39 The lower adverse reaction rate in the KFX group is mainly attributed to the reduction of infection-related adverse events, as most adverse reactions in the control group were wound infections caused by insufficient antimicrobial protection of standard dressings, while KFX's antibacterial and anti-inflammatory effects effectively prevent wound infection. KFX's safety profile stems from its natural origin; its active components have a long clinical track record, with toxicological studies confirming low acute and chronic toxicity. 40 Its anti-inflammatory and antimicrobial effects may also indirectly reduce infection-related adverse events, which are more common in controls relying solely on dressing protection. The high heterogeneity in adverse reaction rates (I2 = 83.2%) likely reflects inconsistent monitoring and reporting standards—some studies recorded only overt reactions, while others included mild discomfort. The standard dressings applied in the 12 included trials were mainly consistent moisture-retentive dressings and routine debridement care, with consistent core components of basic wound management, which ensures the rationality of data pooling in this meta-analysis.
This study has some limitations. First, all included trials were conducted in China, leading to potential geographic bias; Kangfuxin Liquid is mainly used and available in China at present, and pressure ulcer standard care protocols in other countries or regions may be different from those in the included studies, which may limit the international generalizability of the conclusions. Second, 5 of the 12 studies had unclear randomization methods, which may increase the risk of selection bias and affect the stability of the pooled effect sizes to a certain extent. Third, methodological quality was moderate in some studies, with insufficient descriptions of randomization and allocation concealment risking bias; and high heterogeneity, though partially explained by subgroup analyses, remains unresolved. Future research should standardize intervention protocols and outcome measurements, expand geographic diversity, and enhance study design rigor to strengthen evidence quality.
Conclusion
In brief, adjuvant KFX therapy significantly improves wound healing rates, shortens recovery time, promotes early wound contraction, and demonstrates a well-tolerated and favorable safety profile in treating stage II–III pressure ulcers.
Footnotes
Abbreviations
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The experimental data used to support the findings of this study are available from the corresponding author upon request.