
Abstract
Pacinian corpuscles (PCs) remain insufficiently investigated in diabetes mellitus, diabetic neuropathy and associated alterations in plantar soft-tissue integrity, despite their role as fast-adapting mechanoreceptors essential for proprioception and locomotor stability. The extent to which PCs contribute to sensory impairment and foot dysfunction in these conditions remains unclear. This scoping review aimed to evaluate research on the distribution, density, and morphology of plantar PCs in the adult human foot among healthy populations and individuals with diabetes. Studies published from 1 January 2015 to 28 February 2026 were identified from 6 electronic sources. Reporting followed PRISMA guidelines, and methodological quality was assessed using the Joanna Briggs Institute (JBI) critical appraisal tools. Four studies met the inclusion criteria. These included a case report, an experimental study, a morphometric analysis, and a combined retrospective–prospective study, each involving relatively small sample sizes. Both histological quantification and magnetic resonance imaging (MRI) can detect PCs and may support early identification of peripheral neuropathy-related sensory changes, but the evidence remains sparse. Accordingly, further research in larger, well-characterised cohorts is needed to establish reliable reference standards and to clarify changes in PC density associated with diabetic neuropathy.
Pacinian corpuscles (PCs) are one of four specialised cutaneous mechanoreceptors within the somatosensory system.1,2 Also referred to as Vater–Pacini or lamellar corpuscles,3,4 they are the largest mechanoreceptors.5,6 Plantar PCs play a fundamental role in providing sensory feedback that contributes to postural stability, gait coordination, and protective responses during weight-bearing activities.7,8 Accurate sensory input from these receptors is essential for the development and maintenance of optimal movement patterns. PCs detect mechanical stimuli including deep pressure, vibration, and skin deformation. 9 They are sensitive to high-frequency vibration (up to approximately 1000 Hz) and transient pressure changes,10,11 and so they respond effectively to stimuli generated during locomotion. 12 By transmitting vibratory sensory input to the central nervous system, PCs also contribute to tactile processing involved in perceiving object shape, texture, and size during contact with surfaces. 10 Despite their important role in plantar sensation and locomotor function, the distribution, density, and morphology of PCs in the adult plantar foot, and their alterations with healthy ageing and diabetes, remain comparatively underexplored across evolutionary biology, anatomy, physiology, biomechanics, and clinical research. Moreover, available evidence on their distribution, density, and morphology in the adult human foot is limited.
Diabetic neuropathy has been associated with alterations in plantar soft tissue structure, including thinning of the plantar fat pad. 13 Given the critical role of PCs in vibration detection and proprioceptive feedback, neuropathic changes affecting PCs may contribute to impaired vibration sensitivity, reduced proprioceptive input during weight-bearing activities, and compromised plantar tissue integrity. These perturbations may impair mobility, gait, and postural control.12,14
Therefore, the aim of this scoping review was to evaluate the evidence on distribution, density, and morphology of PCs in the plantar foot of adults, including both healthy individuals and those with diabetes.
Methods
Protocol
The review protocol was initially registered with PROSPERO (Number: CRD420261288111). 15 However, preliminary screening revealed a small, heterogeneous body of evidence that did not support meaningful systematic synthesis. The study was therefore reframed as a scoping review.
Literature Search
In accordance with PRISMA-ScR reporting guidelines for scoping reviews, 16 a comprehensive literature search was conducted across four bibliographic databases (MEDLINE Ovid, CINAHL, PubMed, and the Cochrane Library). These databases were selected to capture the breadth of the interdisciplinary literature relevant to plantar PCs, with supplementary searches conducted in Google Scholar and the PROSPERO registry. Searches were limited to studies published from 1 January 2015 to 28 February 2026 to reflect contemporary anatomical mapping techniques and current understanding of plantar mechanoreceptor distribution and density. Advances in imaging and histological analysis during this period support the relevance of recent literature to the aims of this study. Search terms were established using the PICO framework (Population, Intervention/Interest, Comparison, and Outcome) as recommended by Eriksen & Frandsen, 17 incorporating both free-text keywords and Medical Subject Headings (MeSH) to ensure a comprehensive and systematic search. Only studies involving human participants and published in English were included, with no additional restrictions applied beyond the predefined inclusion and exclusion criteria. Reference lists and citation tracking were also used to identify additional eligible studies.
A draft MEDLINE (Ovid) search strategy is provided below and was adapted to reflect the syntax, subheadings, and indexing terms of the other databases:
Pacinian corpuscle*.af. Vater Pacini*.af. lamellar corpuscle*.af. morphology*.af. density.af. distribution.af. count.af. pathological.af. disease.af. degeneration.af. diabetes.af. diabetes mellitus.af. diabetic f??t.af. peripheral nerve injury.af. plantar*.af. plantar fat pad.af. (1 or 2 or 3) and (4 or 5 or 6 or 7) and (8 or 9 or 10) and (11 or 12 or 13 or 14) and (15 or 16)
Study Eligibility Criteria
The PICO framework 17 was used to structure the research question and guide the development of the search strategy in accordance with the PRISMA-ScR guidelines. This scoping review aimed to address the following research question: What evidence exists regarding differences in the distribution, density, and morphology of Pacinian corpuscles in the plantar aspect of the foot between healthy adults and individuals with diabetes mellitus?
Inclusion and Exclusion Criteria
Inclusion criteria comprised quantitative peer-reviewed cadaveric or in vivo research investigating plantar PCs of the adult human foot in healthy and/or individuals with diabetes of both sexes. Studies reporting PC distribution, and/or density, and/or morphology were considered. Acceptable study designs included randomised controlled trials, non-randomised and quasi-experimental studies, observational studies (cohort, case–control, cross-sectional), and anatomical investigations. Studies examining PCs alongside other mechanoreceptors were also considered where relevant plantar-specific data could be extracted. Exclusion criteria included studies involving individuals aged <18 years, non-human models, non-peer-reviewed literature, qualitative or retrospective-only studies, and publications that did not specifically examine plantar PCs. This approach ensured the review synthesised high-quality, clinically relevant, quantitative human data while minimising methodological bias and supporting reliable comparison of morphometric outcomes.
Study Outcomes
Primary outcomes of interest included studies reporting the distribution, density, and morphology of PCs in the plantar aspect of the human foot, particularly within the anterior region, in healthy adults and/or individuals with diabetes. Evidence derived from both cadaveric specimens and in vivo imaging modalities was included to enable comparison between anatomical and radiological approaches to PC identification and measurement.
Secondary outcome data included regional variation within the anterior plantar foot (metatarsal heads compared with the toes), age-related variation in PC distribution, density, and morphology, sex-based differences, and foot laterality (left vs right or dominant vs non-dominant foot). In addition, differences in measurement approaches across studies, including assessments of absolute distribution, density, and morphological characteristics, were examined to support comparison between methodologies.
Study Selection Process
All identified records were uploaded to Rayyan, a web-based systematic review screening tool, 18 for duplicate removal and title and abstract screening. Titles and abstracts were independently screened by two reviewers (S.A. and J.L.M.) with expertise in podiatric research and cardiac nursing, against predefined inclusion and exclusion criteria. Full-text articles that met the initial screening requirements were retrieved and assessed for eligibility using the same criteria, and reasons for exclusion were documented. Reference lists of included studies were also manually screened against the predefined inclusion and exclusion criteria to identify any additional eligible studies. Disagreements between reviewers were resolved at all stages through discussion until consensus was reached.
Data Extraction and Analysis
Data extraction was performed independently by two reviewers (S.A. and J.L.M.), using a predefined data extraction form developed specifically for this review. Extracted information included study characteristics (author, year, country, study design, and sample size); participant characteristics (age, sex, health status, and presence of diabetes, where available); methodological approach (cadaveric or in vivo imaging); and outcomes relating to the distribution, density, and morphology of PCs in the plantar aspect of the foot. Additional variables extracted included regional variation within the anterior plantar foot, age-related and sex-based differences, foot laterality, and measurement approaches used across studies, where applicable. Extracted data were synthesised descriptively and presented in tabular and narrative form.
Risk of Bias
Given the variation in study methodologies, study quality was assessed using design-specific Joanna Briggs Institute (JBI) critical appraisal tools appropriate to each study design to support interpretation of methodological strengths, limitations, and potential sources of bias across the included studies.19,20
Results
The literature search identified 64 records from six electronic sources, with one additional record identified through manual searching. After removing 7 duplicates in Rayyan, 58 records remained for title and abstract screening. Of these, 45 records were excluded for being irrelevant to the review objectives, including studies assessing vibration perception thresholds, palmar anatomical sites, ineligible aetiologies, anatomical locations outside the scope of the review, and unrelated outcome measures, leaving 13 articles for full-text assessment. Following full-text review, nine studies were excluded for failing to meet the inclusion criteria, leaving four included in the final review (Figure 1). These studies were full-text publications from 2021 to 2025 and originated in three countries: Switzerland (n = 2), Spain (n = 1), and India (n = 1). The final set comprised one case report, one experimental quantitative study, one morphometric anatomical study, and one combined retrospective–prospective study (Table 1).
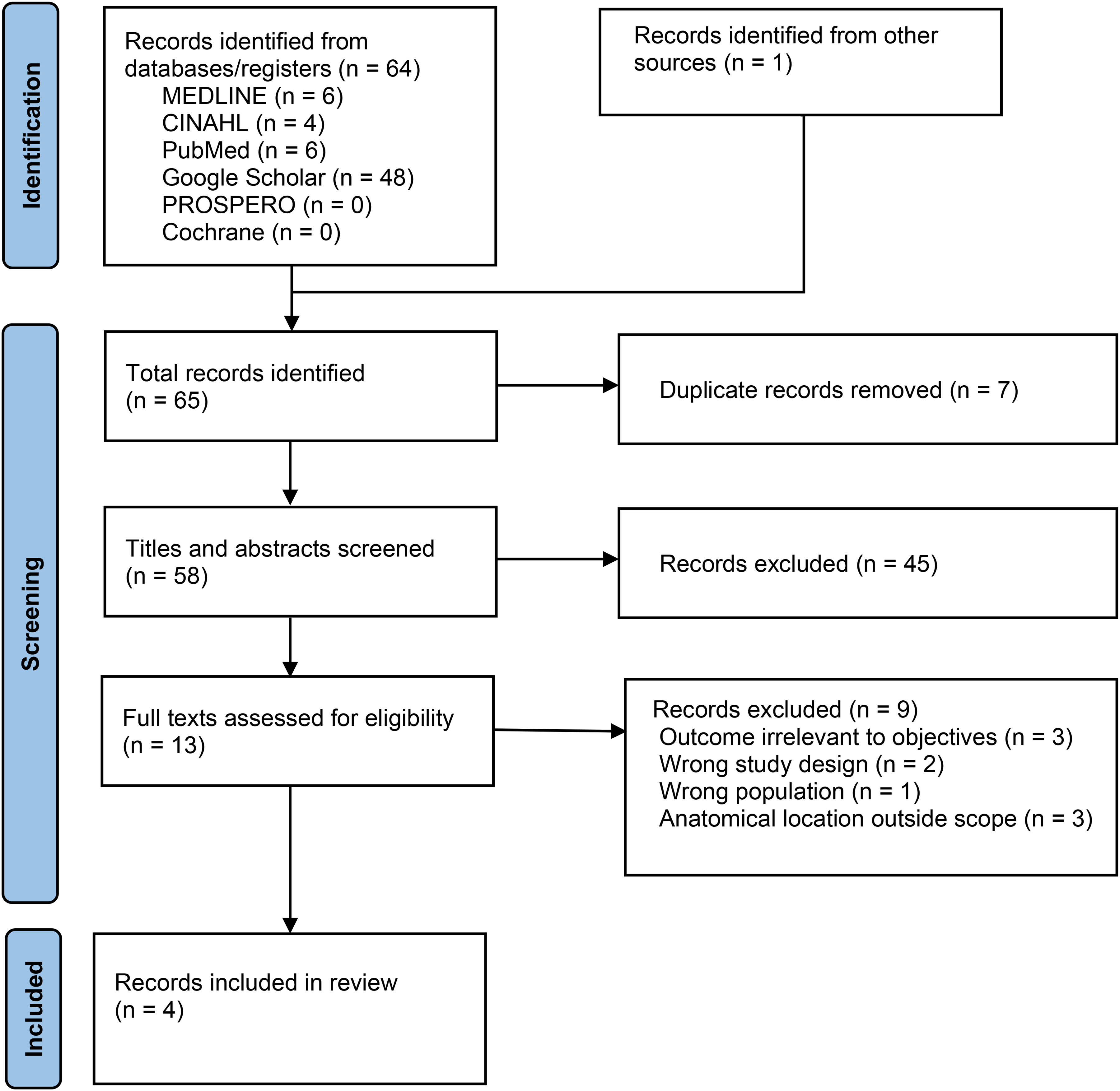
Prisma flow chart.
Characteristics of Included Studies.

Summary of Included Studies
Four studies investigated the distribution, density, and morphology of PCs using complementary imaging and histological approaches across healthy and diabetic populations (Table 1). Two studies employed MRI to characterise the in vivo distribution and clustering patterns of PCs in the plantar forefoot,21,22 whereas two others used histological and immunohistochemical analyses to examine corpuscle morphology and density in clinical and cadaveric plantar toe samples.23,24 In the study by García-Mesa et al, 24 mean HbA1c values increased progressively from controls (<5.7%) to individuals with non-painful distal diabetic sensorimotor polyneuropathy (NP-DDSP) (6.5 ± 0.5%) and painful distal diabetic sensorimotor polyneuropathy (P-DDSP) (7.6 ± 5.2%). Two of the nine study groups reported by Mahato et al 23 were excluded from this review because participants were aged <18 years.
Distribution and Density of Pacinian Corpuscles
In the imaging study by Germann et al, 22 high-resolution 7-T MRI identified a network of PCs in the plantar aspect of the left foot of two asymptomatic male volunteers aged 34 and 56 years. These receptors formed “chain-like” clusters in regions where they were most densely grouped, particularly within the proximal phalanges, metatarsophalangeal (MTP) joints, and toes. A combined retrospective and prospective single-centre study using 3-T MRI evaluated the number and distribution of PCs in the forefoot. 21 Results from the healthy cohort (15 male volunteers) were extracted for analysis, including scans of both the left and right feet. The overall mean number of PCs identified across the phalanges, MTP joints, and metatarsals was 265.3 ± 49.3, demonstrating homogeneous clustering consistent with previous studies.22,25 In the retrospective cohort with distal sensorimotor polyneuropathy (DSP), a lower mean PC number at the forefoot (82.7 ± 46.1) was reported.
Using histological and immunohistochemical methods, García-Mesa et al 24 analysed plantar skin samples obtained from the distal phalanx of the toes across three mixed-gender groups: cadaveric controls (n = 10), individuals with NP-DDSP (n = 10), and individuals with P-DDSP (n = 10). A total of 58 PCs were identified based on their characteristic lamellated morphology on histology and the immunohistochemical presence of S100P in Schwann-like cells within the lamellar structure. Compared with controls, the number of PCs was reduced by approximately 50% in the NP-DDSP group and was nearly absent in the P-DDSP group. This was reflected in the mean number of PCs per skin sample, which progressively decreased across groups from 5.8 ± 1.02 in controls to 3.1 ± 1.0 in the NP-DDSP group and to 0.2 in the P-DDSP group, indicating marked PC rarefaction associated with increasing neuropathic severity.
A morphometric analysis of cadaveric plantar skin specimens from the great toe was conducted in 52 mixed-gender cadavers aged 21–90 years, 23 although it was not specified whether samples were obtained from the left or right side. PCs were observed both as solitary structures and arranged in small clusters, typically comprising three to five corpuscles.
Morphology of Pacinian Corpuscles
On high-resolution 7-T MRI, PCs were structurally differentiated from the surrounding vasculature based on morphology and signal characteristics. 22 Unlike the tubular, branching networks of blood vessels that extend through multiple image slices, PCs appeared as ovoid nodules. Their diameters ranged from 1 to 5 mm. On cross-sectional images, vessels diplayed a dark central core with a bright peripheral rim, whereas PCs appeared as homogenous, hyperintense, spots.22 Similarly, Goller et al 21 reported maximum PC diameters ranging from 1 to 5 mm, consistent with the findings of Germann et al 22 However, in the retrospective cohort with DSP, smaller PC diameters (1-3 mm) were identified.
García-Mesa et al 24 identified PCs histologically by their characteristic lamellated morphology and immunohistochemical staining profile, specifically the presence of S100P in Schwann-like cells within the lamellar structure. Mahato et al 23 reported age-related increases in PC size, with statistically significant increases observed in horizontal and vertical diameters, outer perimeter, and capsule thickness across age groups. In addition to these morphometric changes, PCs exhibited considerable variability in shape, appearing triangular, oval, fusiform, quadrilateral, dumbbell-shaped, cylindrical, or circular.
Quality Assessment
The methodological quality of the included studies was assessed using the JBI critical appraisal tools tailored to each study design. Overall, the studies demonstrated variable methodological quality, with strengths primarily related to advanced imaging techniques and detailed histological analyses, and limitations including small sample sizes, lack of histological confirmation in imaging-based studies, and potential confounding in clinical cohorts.
Germann et al 22 used high-resolution 7-T MRI to visualise plantar PCs. Interpretation of these findings should consider several methodological limitations. These include the absence of histological confirmation, lack of inter-observer reliability assessment, and substantial sampling bias due to the very small cohort (n = 2). Consequently, the findings should be interpreted as preliminary and primarily represent a methodological demonstration of the capability of 7-T MRI and the 3D-DESS sequence to visualise mechanoreceptor networks rather than definitive anatomical evidence.
Goller et al 21 provided further support for MRI-based assessment of PC distribution and rarefaction. Nevertheless, a number of methodological limitations were identified. Different MRI scanners were used for the healthy and DSP cohorts, which may have influenced size measurements and introduced measurement variability. In addition, the retrospective design of the study and hardware heterogeneity limit the immediate generalisability of the findings to broader clinical settings.
García-Mesa et al 24 demonstrated several methodological strengths, including the use of high-resolution confocal microscopy and double immunofluorescence, which enhanced the internal validity of the histological findings in PCs. Quantification was further strengthened by using two blinded observers and standardised section intervals (50 μm), thereby reducing the potential for measurement error. However, the relatively small sample size (n = 10 per group) may limit statistical power, particularly given the variability associated with diabetes progression and participant age. Furthermore, the lack of statistical adjustment for potential confounders, including age differences between groups and variation in diabetes duration, suggests caution when attributing the observed PC degeneration solely to pain status.
Mahato et al 23 provided detailed morphometric data on PCs in cadaveric plantar skin across the lifespan. Methodological limitations were identified that may affect the interpretation and generalisability of these findings. The older adults (>81 years) cohort was underpowered (n = 4), thereby increasing susceptibility to outliers. In addition, although fixation in 10% buffered formalin represents standard histological practice, chemical fixation is known to induce tissue shrinkage,26,27 which may affect absolute morphometric measurements. The lack of adjustment for potential confounders such as body mass index (BMI) and sex further limits the interpretation of absolute size comparisons. Nevertheless, relative differences between age groups are likely to remain valid, and the findings provide a useful reference for the morphometry of PCs in the great toe, although they cannot be confidently extrapolated to the entire plantar foot without further investigation.
Discussion
This scoping review addresses an important gap in podiatric and neurological research by providing the first comprehensive synthesis of evidence relating to the distribution, density, and morphology of PCs in the plantar foot across both histological and MRI-based studies. By integrating findings from four heterogeneous studies involving healthy adults and individuals with diabetes, the review identified key patterns in PC distribution, density, and morphology, highlighted methodological inconsistencies, and revealed important gaps in the current evidence base. Nonetheless, the literature remains sparse and heterogeneous, underscoring the need for further research to clarify the role of PCs in plantar sensory function, diabetes mellitus, and peripheral neuropathy.
MRI-based investigations to date have included only male participants, limiting the generalisability of imaging-derived findings. Although both histological and MRI studies consistently report the greatest clustering of PCs in the forefoot, baseline reference data on PC counts, distributions, and densities across both sexes are lacking. Furthermore, no studies examined the potential influence of age-related changes in foot-shape, limb dominance, or left–right laterality on PC distribution or associated pathology. These gaps highlight priority areas for further investigation and provide direction for subsequent research exploring the functional significance of PCs in plantar biomechanics and disease processes.
Notably, MRI findings in both studies21,22 are consistent with those reported in histological investigations. Goller et al 21 provide initial evidence supporting MRI-based detection of PC rarefaction. Nevertheless, these findings require further validation due to technical heterogeneity between studies and the limited availability of normative data. Replication in larger and more diverse cohorts with comprehensive neurological and metabolic screening is required before MRI-derived estimates of PC distribution and density can be considered representative of normal anatomy. Although clustering patterns were similarly described, PCs were also characterised as having a rod- or column-like arrangement 25 or belt-like configuration. 28 Furthermore, despite their relative sparsity in the heel, PCs possess large receptive fields, suggesting a role more closely aligned with plantar sensory feedback than with fine spatial discrimination.
Histological and immunohistochemical analyses of PCs in plantar tissue specimens from individuals with NP-DDSP and P-DDSP showed morphological differences compared with cadaveric control specimens, 24 indicating a marked reduction in PCs associated with increasing neuropathic severity. Similar degenerative changes observed in other cutaneous mechanoreceptors within the same study suggest that PC degeneration may form part of a broader disruption of the peripheral mechanosensory system as diabetic neuropathy progresses from non-painful to painful stages.
Age-related changes in PC morphology and function were evident across the included studies. Detailed morphometric analysis of PCs in the thick plantar skin of the human great toe demonstrated a significant association between increasing age and corpuscle size, with horizontal and vertical diameters, outer perimeter, outer area, and capsule thickness exhibiting progressive enlargement across the lifespan. 23 These findings suggest that PCs undergo continuous structural remodelling throughout development and ageing. Morphological changes may occur alongside age-related decline in vibrotactile sensitivity, 29 although the relationship between these phenomena remains unclear. Despite being restricted to the great toe, the study provides valuable reference data on age-related morphological variation in plantar PCs. However, these observations cannot be confidently generalised to other mechanoreceptor-rich regions of the foot without further investigation. Evidence from developmental and adult studies also suggests that PC density may vary across the lifespan, although direct comparisons remain challenging because of differences in study populations and methodological approaches. The progressive enlargement of PCs may therefore represent a dynamic or compensatory response to age-related alterations in sensory function, although this relationship remains speculative and warrants further investigation.
This review has some limitations. The first relates to the small number of studies investigating plantar PCs (n = 4), with much of the available literature focusing on other anatomical regions. Considerable heterogeneity between studies, including differences in MRI hardware, histological protocols, and measurement approaches, limited direct comparison of findings. Anatomical investigations relied primarily on cadaveric specimens, which may not fully reflect the structural and functional characteristics of PCs in living tissue. Imaging-based identification of PCs remains technically challenging, and variation in image resolution and acquisition parameters may influence reported estimates of corpuscle size and distribution. Included studies lacked detailed demographic reporting, limiting assessment of potential differences related to age, sex, or limb dominance. Although PCs are known to contribute to vibration detection and proprioceptive feedback, direct evidence linking their plantar distribution to locomotor function remains limited.
Our findings have implications for understanding the structural and functional importance of plantar PCs in healthy ageing and in neuropathic disease processes. Future research should prioritise larger and more diverse cohorts and consider anatomical variables such as foot size and shape, which differ significantly between men and women and change with age.30,31 Given that both histological and MRI studies consistently report the highest concentration of PCs in the forefoot, sex- and age-related differences in forefoot morphology may contribute to variation in corpuscle distribution and density. In addition, limb dominance has been proposed as a factor influencing the laterality of foot disorders. Indeed, it has been reported that approximately two-thirds to three-quarters of patients with diabetes undergo ulceration or amputation on the dominant side.32–34 These observations suggest that dominance-related loading patterns may represent an important variable for future investigations of plantar PC distribution. Furthermore, because the relationship between PCs, plantar fat pad and locomotion remains poorly understood, comparative animal models with locomotor loading patterns and metabolic characteristics comparable to those of humans may provide additional insight into the functional role of clustered corpuscle distributions in impact attenuation during gait, plantar soft-tissue alterations, and PC degeneration in neuropathic conditions.
In conclusion, evidence suggests that PCs in the plantar foot exhibit consistent clustering patterns across the phalanges, MTP joints, and metatarsals, with reported diameters typically ranging from 1 to 5 mm across both MRI and histological studies. Histological investigations further indicate age-related increases in PC size, whereas studies in diabetic peripheral neuropathy demonstrate progressive reduction and structural degeneration that form part of a broader disruption of the peripheral mechanosensory system. Although peripheral neuropathy appears to be associated with reduced PC density, the degree of this reduction and how it evolves across different stages of diabetes have yet to be established. Moreover, interpretation of these findings is limited by small sample sizes, methodological heterogeneity, population variability, and incomplete adjustment for confounding variables. Finally, the literature remains insufficient to establish definitive normative reference values for PC density or to fully characterise their significance in health and diabetes.
Footnotes
ORCID iDs
Author Contributions
Conceptualisation: S.A., Methodology: S.A., C.F. and F.Z., Formal analysis: S.A. and J.L.M., Investigation: S.A. and J.L.M., Data curation: S.A., Writing – original draft: S.A., Writing – review & editing: C.F., F.Z., C.A., S.G.S., R.M.B., J.A., and N.P, Visualisation: S.A., Supervision: C.F. and F.Z., Project administration: S.A.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.