
Abstract
Acute kidney injury, a sudden decline in renal filtration, is a surprisingly common pathology resulting from ischemic events, local or systemic infection, or drug-induced toxicity in the kidney. Unchecked, acute kidney injury can progress to renal failure and even recovered acute kidney injury patients are at an increased risk for developing future chronic kidney disease. The initial extent of inflammation, the specific immune response, and how well inflammation resolves are likely determinants in acute kidney injury-to-chronic kidney disease progression. Lymphatic vessels and their roles in fluid, solute, antigen, and immune cell transport make them likely to have a role in the acute kidney injury response. Lymphatics have proven to be an attractive target in regulating inflammation and immunomodulation in other pathologies: might these strategies be employed in acute kidney injury? Acute kidney injury studies have identified elevated levels of lymphangiogenic ligands following acute kidney injury, with an expansion of the lymphatics in several models post-injury. Manipulating the lymphatics in acute kidney injury, by augmenting or inhibiting their growth or through targeting lymphatic-immune interactions, has met with a range of positive, negative, and sometimes inconclusive results. This minireview briefly summarizes the findings of lymphatic changes and lymphatic roles in the inflammatory response in the kidney following acute kidney injury to discuss whether renal lymphatics are a beneficial, maleficent, or a passive contributor to acute kidney injury recovery.
Impact statement
Acute kidney injury (AKI) occurs frequently during ischemia, infection, or drug-induced toxicity. Despite an initial recovery, AKI increases future chronic kidney disease (CKD) risk. This may be, in part, due to how well the initial renal inflammation was managed. The lymphatic vasculature could be important in this process through the regulation of fluid balance, macromolecule and immune cell transport, and immunomodulatory roles. AKI and CKD studies have identified increased lymphatic growth factors and inflammation-associated lymphangiogenesis in the kidney post-injury and suggest these processes as potential targets for therapeutic intervention. This minireview summarizes these findings and attempts to answer the question of whether renal lymphatics are good or bad following AKI.
Introduction
AKI is an inflammatory disease that is associated with increased mortality, adverse cardiovascular events, and rising hospitalization costs.1–3 Acute kidney injury (AKI), as defined by Kidney Disease: Improving Global Outcomes (KDIGO), is characterized by a ≥0.3 mg/dL increase in serum creatinine within 48 h or an increase of 1.5× from baseline serum creatinine occurring within the previous seven days or a <0.5 mL/kg/h decrease in urine output over a 6-h period. 4 In the United States, common causes of AKI include nephrotoxic injury, fluid volume deficit, and ischemia, with studies estimating that 50% of patients admitted to the ICU will exhibit an AKI.5,6 Other underlying health concerns such as heart disease, aging, diabetes, and hypertension increase the risk of developing AKI. 1 While many patients successfully recover from AKI, clinical research has demonstrated a strong correlation of AKI incidence to the future development of chronic kidney disease (CKD).6–8 CKD is associated with a progressive loss in renal function, which increases cardiovascular diseases risk and can result in eventual kidney failure. Changes to renal blood flow and the biology of the blood endothelium in AKI have been well-studied—understandably as blood flow and filtration are clinical determinants of renal function—while the roles of the lymphatic vasculature have been largely unappreciated. Lymphatic vessels control tissue homeostasis through fluid and electrolyte balance, immune regulation and trafficking, and antigen and chemokine transport. These roles make lymphatics a potentially critical part of the kidney’s functional and inflammatory response to AKI. Increasing evidence from basic research indicates that lymphatics and lymphangiogenesis, an expansion of the lymphatic network, are part of the AKI response.9–11 This minireview thus aims to summarize the current research on the beneficial or maleficent roles of lymphatics in AKI and how renal lymphangiogenesis may be a potential target to alter the inflammatory environment following AKI to prevent CKD progression.
Roles of lymphatics and lymphatic renal physiology
Broadly, the lymphatic vasculature is a key regulator within the body responsible for facilitating dietary lipid absorption and the clearance of interstitial macromolecules and for maintaining tissue fluid homeostasis, electrolyte balance, and immune surveillance. Lymph transports immune cells and antigens to the lymph nodes, wherein lymphocytes can then be programmed for adaptive immune responses.12,13 Based on the critical roles that have been identified for lymphatics in other pathologies, such as cancer, autoimmune disease, wound healing, and transplant rejection, it is likely that lymphatics would play a part in the AKI inflammatory response. 14
Under normal physiological conditions, renal lymphatics are found in the cortex and follow the renal arteries inward toward larger collecting lymphatics at the hilum or flow outward to join a capsular lymphatic network. Renal lymphatic anatomy and physiology has been recently and elegantly reviewed by Russell 15 and Jafree. 16 Initial lymph is approximately equal to the composition of interstitial fluid. In the renal cortex, this is composed of fluid reabsorbed from both capillary filtrate and the tubules. Most renal lymph is subsequently drained through the hilar lymphatics to the renal lymph nodes for immune surveillance before being returned to the blood circulation via the thoracic duct.16,17 During the pathogenesis of disease, inflammatory conditions alter vascular perfusion and permeability, changing the hydrostatic and osmotic pressures that govern interstitial fluid generation and lymphatic uptake and flow; dysregulation of these balances results in tissue edema. 13 Renal lymphatic function, or dysfunction, is therefore critically involved in tissue homeostasis under pathophysiological conditions.15,18
Expansion of the lymphatic vessel network, lymphangiogenesis, is commonly associated with tissue inflammation. 19 Lymphangiogenesis is driven predominantly through Vascular Endothelial Growth Factor (VEGF)-C and VEGF-D growth factor signaling through VEGF receptor (VEGFR)-3. VEGFR-3 is expressed primarily on lymphatic endothelial cells in the adult, but is also found on some macrophage and other endothelial cell populations in inflammation and development.8,20 VEGFR-3 signaling promotes vascular patterning in the kidney during development and, during renal inflammation, elevated VEGF-C/D expression promotes inflammation-associated lymphangiogenesis.21,22
AKI and lymphatics
While lymphatic changes in AKI have garnered increased attention in recent years, the current research findings are divided as to whether renal lymphatics and lymphangiogenesis are beneficial in remediating inflammation or if they propagate a malicious immune response. Under normal physiological conditions, VEGF-D and VEGF-C are present in the renal tubules at low levels. 23 Upon injury to the kidney, both the tubular epithelium and infiltrating macrophages secrete VEGF-C and VEGF-D and promote lymphangiogenesis.23–27 Some studies have found promotion of renal lymphangiogenesis to be beneficial by promoting increased immune cell trafficking, clearance of debris, and clearance of excess fluid from the interstitium (Figure 1)9,17,18,20 Other published findings have indicated lymphatics may be negatively regulating renal inflammation.28–30 Further research must be conducted to determine if conflicting findings are indicative of different lymphatic responses to specific injuries or if this is a passive response to an inflamed renal environment. It is clear the lymphatic vasculature potentially fulfills many roles in the renal environment that regulates homeostasis. For example, our lab has demonstrated that augmenting renal lymphatics through a murine genetic model reduced blood pressure, increased sodium excretion, and decreased renal proinflammatory immune cells in models of hypertension associated with kidney inflammation.31,32 Whether similar mechanisms are at play in the pathogenesis of AKI remains to be fully elucidated.
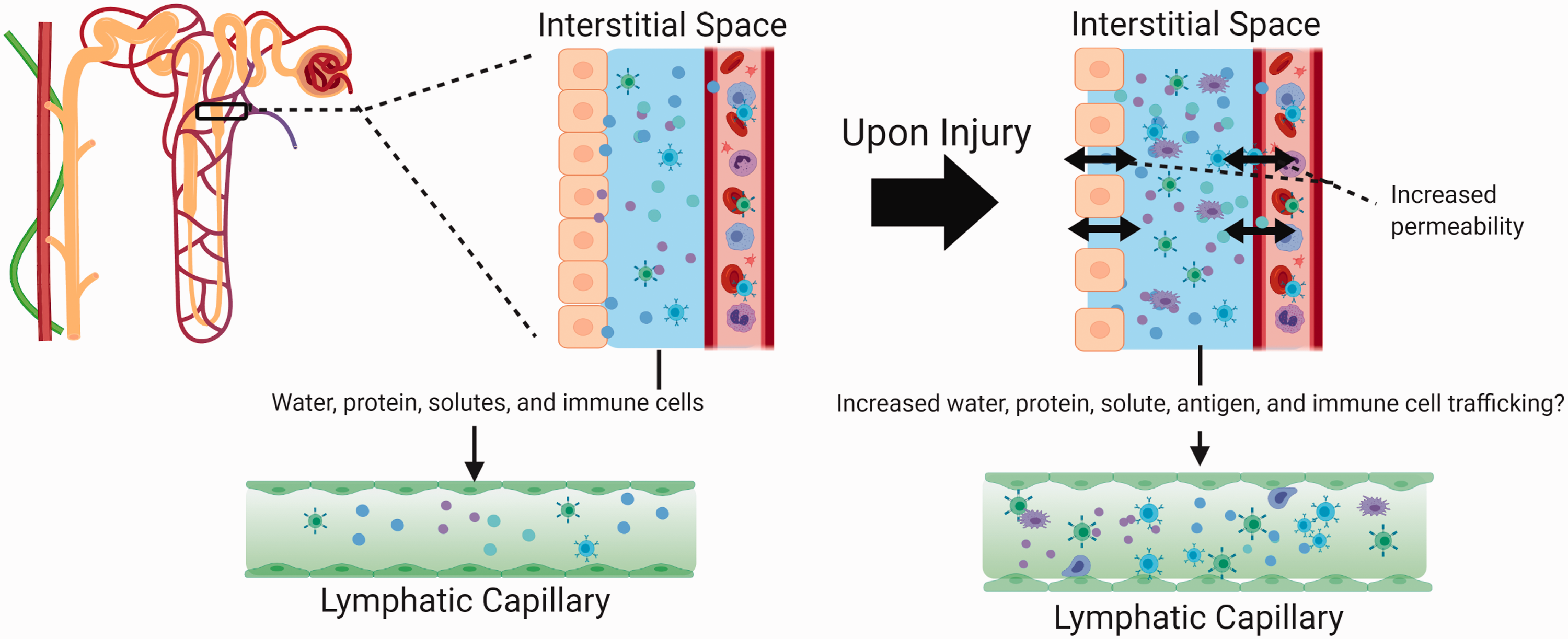
Lymphatic capillary modulation of the interstitial space in AKI. Interlobular artery with associated lymphatic depicted near nephron. Normal lymphatic capillary transport of macromolecules, water, and immune cells from the interstitial space (left). After AKI damage or activation of the renal epithelium and blood endothelium increases the interstitial contents and inflammation (right). Activated immune cells, antigens, and cytokines interact with and are transported by the lymphatic capillary (to the lymph node) resulting in either a dampening or propagation of the immune response. Created with BioRender.com.
Renal lymphangiogenesis: Beneficial or detrimental?
The pathophysiological etiologies of human AKI are diverse and a range of pre-clinical models exist to study the tissue injury response. 33 The endogenous lymphatic response in AKI models has been characterized through research published by Zarjou et al. and Pei et al.23,28 in several of the pre-clinical AKI models commonly including: ischemia reperfusion (I/R), cisplatin-induced nephrotoxicity, folic acid-induced nephropathy, and diphtheria toxin selective tubular injury. Our own model of isolated glomerular injury through podocyte apoptosis also demonstrates a marked increase in cortical lymphatics (Figure 2). 34 The models nearly universally demonstrated increased VEGF-C/D expression in the kidney following injury and vigorous lymphangiogenesis compared to controls. Increased lymphatic vessel labeling and/or elevated VEGF-C/D was also confirmed in human renal biopsy tissue. 28 AKI thus elicits an inflammation-associated lymphangiogenic response similar to other tissue injuries.
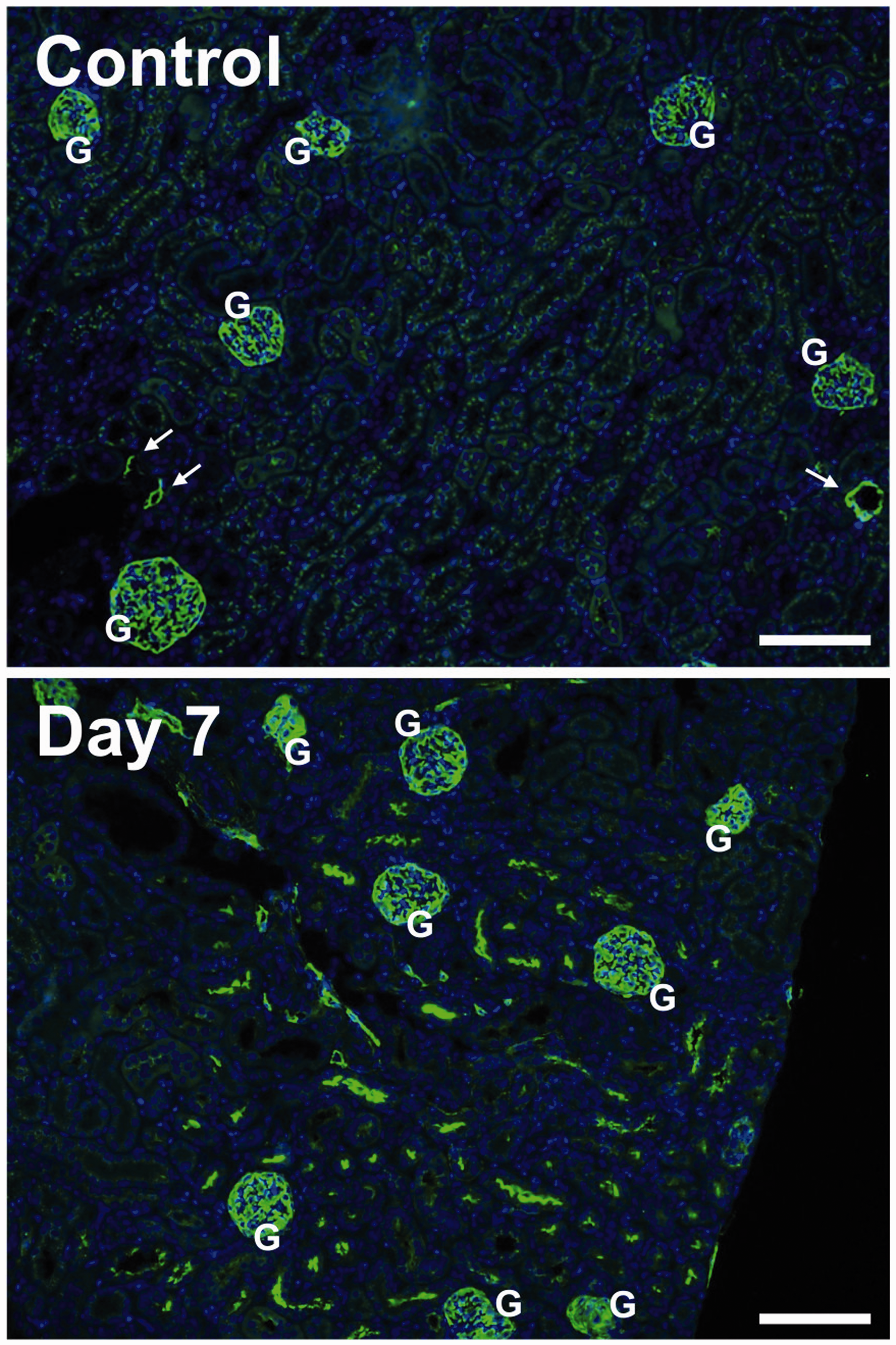
Renal lymphatics following AKI. In a healthy, control kidney, lymphatics (arrows) are sparse in the cortex, associated with large blood vessels. Seven days after a proteinuric injury, podoplanin-positive lymphatic cells and structures are found throughout the cortex. Green: podoplanin; Blue = DAPI; “G” indicates glomeruli. Bars = 100 µm.
Beneficial findings?
Renal lymphangiogenesis has been targeted in a number of studies identifying a potential beneficial role in regulating AKI. In a loss of function experiment, Zhang et al. demonstrated increased renal fibrosis following renal lymphatic ligation and bilateral lymphatic renal duct ligation. 35 Disrupting the lymphatic circulation promoted further renal fibrosis, through increasing TGF-β1/Smad signaling, and progression to chronic renal failure. Severing the lymphatic circulation could potentially prevent proper immune cell clearance from the site of injury. 36 Renal lymphangiogenesis was also found to be beneficial in a unilateral ureteral obstruction (UUO) AKI model. 25 This study demonstrated that augmenting lymphangiogenesis by treating with VEGF-C following UUO injury not only improved the fibrotic response post injury, but also decreased inflammatory cytokines, TGF-β levels, and total macrophage numbers when compared to vehicle-treated mice. These studies demonstrate that renal lymphatics play a positive role in regulating the fibrotic and immune response in AKI, but other studies suggest the opposite.
Maleficent findings?
Renal lymphangiogenesis may be merely indicative of inflammation or may worsen the tissue’s immune response. After identifying marked renal lymphangiogenesis in a model of adriamycin nephrosis, 37 Yazdani et al. tested whether inhibiting lymphangiogenesis by blocking VEGFR-3 impacted interstitial inflammation and fibrosis. 38 They found that proteinuria-induced tubulointerstitial inflammation, immune cell populations, and tissue fibrosis all occurred independently of whether lymphangiogenesis occurred or not, thus suggesting that lymphatics hold a passive role in the process. 38 In chronic renal inflammation models of diabetic nephropathy and lipotoxicity, a similar conclusion could be made: when the underlying pathology was targeted and tubulointerstitial fibrosis and inflammation were reduced, so too were lymphatic vessel proliferation and density. 30 A recent study utilizing several AKI models demonstrated that inflammation-associated lymphangiogenesis in the kidney may, however, be potentially detrimental to the healing process and that blocking it could be helpful. 28 With increased renal lymphangiogenesis, the renal draining lymph node (RDLN) experienced more dendritic cell recruitment with increased expression of the lymphatic endothelium-secreted chemokine CCL21. Neutralizing CCR7 (the receptor for CCL21) reduced trafficking into the RDLN and improved the inflammatory response, making the case that renal lymphatics play a potentially negative role in AKI. This finding is similar to the immunologic phenomenon associated with lymphatics during renal transplant or autoimmune responses in which severing the connection to the RDLN has proven beneficial.29,39 (An excellent review of this topic has been previously published. 40 ) Severing the lymphatic vasculature has been demonstrated to exacerbate inflammatory conditions in other pathologies through increased interstitial edema, CCL21 expression, and fibrotic signaling that may promote an allogenic immune response.16,17,41 These studies demonstrate that renal lymphatics may potentially play a detrimental role in regulating the fibrotic and immune response in AKI or may be merely indicative of the overall inflammatory response.
The etiologies of AKI are various and may ultimately determine if lymphangiogenesis is beneficial, maleficent, or simply a passive response to an inflamed renal environment. How lymphatics regulate the immune response may provide a key to understanding why lymphangiogenesis elicits different outcomes across various kidney pathologies and models.
Lymphatic regulation of the renal immune environment
Following AKI, diverse immune cell types are involved in the pathogenesis and propagation of the inflammatory response.42,43 Two functions of the kidneys in regulating systemic fluid and cytokine homeostasis are altered in AKI, but could also be impacted by changes to the renal lymphatic vasculature. 44 Blind-ended lymphatic capillaries act as access points for immune cells to enter the lymphatic network and travel to draining lymph nodes. Lymphatic endothelial cells (LECs) have also demonstrated local immunomodulatory roles in cancer models through cross presentation of antigens and expression of MHC I, MHC II, and PD-L145, 46 For example, IFNγ released from CD8+ T cells drives increased expression of PD-L1 on LECs and disrupting IFNγ leads to local CD8+ T-cell accumulation within the skin during melanoma. 47 While this immunomodulatory function of LECs has not been specifically investigated in AKI, PD-1 signaling has demonstrated protection against I/R-induced AKI. 48 In AKI, the initiation, maintenance, and resolution phases are mediated by inflammation and immune cell responses which include inflammatory monocytes, neutrophils, lymphocytes, and natural killer (NK) T cells.49–51 Many of these cell types are potentially signaling to and being regulated by LECs.9,50 In the renal inflammatory environment, lymphangiogenesis has been identified ahead of fibrotic remodeling, suggesting lymphatics may play an early immunomodulatory role. 37
Multiple studies have demonstrated activated macrophages, dendritic cells (DCs), lymphocytes, and neutrophils can promote lymphangiogenesis.42,51,52 For example, macrophages accumulate immediately after onset of AKI and are a source of increased VEGF-C that may drive lymphangiogenesis.24,52,53 Research in UUO models has demonstrated VEGF-C released from macrophages drives lymphangiogenesis in part through a CCR2-mediated activation of the PI3K-AKT-mTOR signaling pathway.24,27,28 Specifically, anti-inflammatory M2 macrophages have been demonstrated to release higher levels of VEGF-C in UUO models when compared to pro-inflammatory M1 macrophages. 27 Macrophage VEGF-C secretion and lymphangiogenesis were increased in a UUO model through both hyaluronan and toll-like receptor 4-dependent signaling. 26 Some T-cell populations have also demonstrated an ability to inhibit lymphatic growth.54,55 During inflammation, cytokines released from Th2 cells were found to inhibit lymphangiogenesis, while regulatory T cells promoted lymphangiogenesis by increasing lymphotoxin-β receptor signaling in lymphatic endothelial cells. 56 Recently, a cell profiling study in an I/R injury model found increased TGF-β and lymphotoxin-β expression possibly tying these inflammatory pathways to a lymphangiogenic response in AKI. 57
Upon lipopolysaccharide or ischemic insult to the kidney, renal DCs increase trafficking to the RDLN where antigen-specific CD4+ cells promote further T-cell proliferation. 58 DC mobilization is promoted by the lymphatic vasculature through increased lymphatic expression of the chemokine CCL21. 59 Together, these studies indicate the DC response in AKI may be regulated through lymphatic expression of CCL21, which promotes homing of immune cells to the lymph node and T cell survival.60,61 LECs have demonstrated expression of MHC I, MHC II, and cross presentation of environmentally derived antigens which in turn prime CD8+ T cells. 45 Furthermore, sphingosine-1-phosphate receptor (S1PR1) signaling regulates CD8+ cell egress from the draining lymph node 62 ; targeting S1P signaling appears to be beneficial in several models of AKI and transplantation.63,64 In AKI, T regulatory cells derived from the lymph node appear to be protective against ischemia reperfusion injuries dependent on IL-10 expression. 65 Interestingly, T regulatory cells also rely on both IL-10 and TGF-β signaling to promote antibody production. Increased TGF-β levels in obstructive nephropathy models promote both fibrosis and lymphangiogenesis through increased connective tissue growth factor (CTFG) and VEGF-C production. 30 Furthermore, TGF-β signaling in chronic kidney disease activates a noncanonical pathway through increased Sonic hedgehog which has been demonstrated to promote LEC proliferation. 66 LEC interactions with T-cells and their cytokines define a role for LECs as antigen-presenting cells and provide a potential mechanism through which T cell systemic peripheral tolerance is mediated. 45 It is clear lymphatics communicate directly to the renal immune environment and systemically through interactions with antigens and immune cells. These studies present a host of potential mechanisms through which lymphatics in the kidney may impact immune homeostasis of the kidney before, during, and after AKI.
Conclusions
Increasing research focusing on lymphatics in AKI has identified that the lymphatic system plays a key role in regulating the pathophysiological outcomes post injury. Based on the current body of literature, whether these roles are beneficial or mostly detrimental remains inconclusive. It is possible that lymphatic changes in AKI are simply a response to inflammation, rather than a contributor. Nephrotoxic, immunological, and hydrostatic renal injuries are initiated by different insults and drive different mechanistic responses. Therefore, timing and type of injury may elicit unique lymphatic responses that determine the conflicting roles observed in the reviewed studies. For example, a glomerular injury does not elicit the same tubulointerstitial injury, lymphatic remodeling, and inflammatory response as an I/R or UUO-induced AKI. The timing of injury onset, in relation to the degree of lymphangiogenesis, may also alter how beneficial the lymphatic vasculature is within the renal tissue. Promoting lymphangiogenesis at stages earlier in the inflammatory response may assist in immune cell clearance, while increased lymphangiogenesis in an established chronic inflammatory environment may further promote fibrotic remodeling. The lymphatic vasculature has various roles in maintaining tissue fluid homeostasis, actively regulating solute flux, and transporting antigen and immune cells throughout the body making it an intriguing system to study in the context of tissue injury. Understanding how lymphatic functions and lymphangiogenesis impact AKI will determine whether renal lymphatics may be a diagnostic or therapeutic target managing AKI in the future.
Footnotes
Authors’ contributions
The authors made substantial contributions to the literature research, writing, and editing of the manuscript.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: HAC and JMR were supported in part by the National Institute of Diabetes And Digestive And Kidney Diseases of the National Institutes of Health [R01DK119497].