
Abstract
Objective:
The global burden of surgical vascular disease is increasing and with it, the need for cost-effective, accessible prognostic biomarkers to aid optimization of peri-operative outcomes. The neutrophil-lymphocyte ratio (NLR) is emerging as a potential candidate biomarker for perioperative risk stratification. We therefore performed this systematic review and meta-analysis on the prognostic value of elevated preoperative NLR in vascular surgery.
Methods:
We searched Embase (Ovid), Medline (Ovid), and the Cochrane Library database from inception to June 2019. Screening was performed, and included all peer-reviewed original research studies reporting preoperative NLR in adult emergent and elective vascular surgical patients. Studies were assessed for bias and quality of evidence using a standardized tool. Meta-analysis was performed by general linear (mixed-effects) modelling where possible, and otherwise a narrative review was conducted. Between-study heterogeneity was estimated using the Chi-squared statistic and explored qualitatively.
Results:
Fourteen studies involving 5,652 patients were included. The overall methodological quality was good. Elevated preoperative NLR was associated with increased risk of long-term mortality (HR 1.40 [95%CI: 1.13-1.74], Chi-squared 60.3%, 7 studies, 3,637 people) and short-term mortality (OR: 3.08; 95%CI: 1.91-4.95), Chi-squared 66.59%, 4 studies, 945 people). Outcome measures used by fewer studies such as graft patency and amputation free survival were assessed via narrative review.
Conclusions:
NLR is a promising, readily obtainable, prognostic biomarker for mortality outcomes following vascular surgery. Heterogeneity in patient factors, severity of vascular disease, and type of vascular surgery performed renders direct comparison of outcomes from the current literature challenging. This systematic review supports further investigation for NLR measurement in pre-vascular surgical risk stratification. In particular, the establishment of a universally accepted NLR cut-off value is of importance in real-world implementation of this biomarker.
Introduction
Vascular surgery is associated with a high risk of perioperative adverse events, in part due to the heavy burden of comorbidities in surgical candidates. 1 -3 The incidence of surgical disease is increasing with growing life expectancy and cardiovascular disease globally. 4 Inexpensive and accessible perioperative biomarkers are crucial in improving the risk-stratification of these patients in order to optimize perioperative care.
Neutrophils and lymphocytes are known to play an active role in the pathogenesis and aggressiveness of atherosclerotic plaque formation and stability. 5,6 The neutrophil-lymphocyte ratio (NLR) is a ratio of the absolute count of neutrophils to the absolute count of lymphocytes, and provides an indication of systemic inflammatory burden, as well as important information about the complex inflammatory milieu of a patient’s vasculature.
Two reviews conducted in recent years by Tan et al. (2015) and Bhat et al. (2013), raised the notion that the NLR may be superior to white cell count or subtypes, as a prognostic biomarker, because it alludes to a complex interplay between 2 complementary immune pathways that culminate in neutrophilia and lymphopenia respectively. 7,8 NLR values are also more resilient to modulation by physiological stressors such as dehydration and exercise than individual white cell subtypes. 7 Furthermore, Horne et al. (2005) were able to show that an elevated NLR, even within normal white cell subtype count references, is associated with atherosclerotic events and mortality. 9
A growing body of evidence supports NLR as a prognostic marker for morbidity and mortality following cardiac surgery and percutaneous coronary intervention. 10 -12 Studies over the last 10 years have since begun to investigate NLR as a prognostic biomarker in vascular surgery. 8
We therefore conducted this systematic review and meta-analysis on the prognostic value of preoperatively measured NLR in predicting mortality and other vascular complications in patients undergoing both open and endovascular surgery in elective and emergent patient contexts.
Methods
Study Design
This systematic review and meta-analysis of prognostic test accuracy evaluated study-level data and was reported in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) Statement. Study design was consistent with current methodological guidance. 13 -15 There were no major protocol deviations.
Eligibility Criteria
We included original research studies evaluating the prognostic value of elevated preoperative NLR in predicting short or long-term postoperative complications following vascular surgery in adult patients. We excluded studies measuring perioperative neutrophil or lymphocyte counts alone, studies measuring NLR postoperatively only, studies where angiogram was performed without vascular intervention, studies involving cardiac or intracranial surgery, non-human studies, paediatric studies, studies with incomplete or insufficient data for our statistical analyses, and conference abstracts.
Search Strategy
The following electronic bibliographic databases were searched from inception to June 2019: Medline (Ovid), Embase (Ovid) and the Cochrane Library. Our search strategy included a comprehensive set of keywords and MESH terms for NLR prognostication in vascular surgery 15,16 (Online Appendix—Search Strategy). In these searches, we placed no restriction on language or publication period, and reference lists of included studies were searched for further potentially relevant citations.
Study Selection
Two review authors (SMJ and JP-D) comprehensively screened the titles and abstracts yielded by our search for studies potentially eligible for inclusion in our review based upon the pre-defined selection criteria. Following this, potentially relevant studies were assessed by both authors independently via full-text review for eligibility, with a third author passing final judgement on any disagreements (CBC). Studies failing to meet inclusion criteria after full-text review were excluded.
Data Extraction and Management
Two review authors (SMJ and JP-D) independently extracted data from each included study using standardized forms. We extracted the following information: study timeframe, design and setting, relevant study population demographics and co-morbidities, operative details, preoperative NLR measurement, selection of threshold for NLR elevation, prognostic performance in relation to outcomes observed (including true positive (TP), true negative (TN), false positive (FP), and false negative (FN) rates, hazard ratios (HR) and odds ratios (OR) reported), and follow-up duration of patients. Where fewer than 3 studies reported an outcome, we restricted the outcome to qualitative analysis.
Assessment of Methodological Quality
Two review authors (SMJ and JP-D) independently assessed the risk of bias in incorporated studies using the Prediction model Risk Of Bias ASsessment Tool (PROBAST), 17 with discrepancies again resolved via a third author’s adjudication (CBC) (Online Appendix—Methodological Quality Scale).
Outcome Measurements
The primary outcome of interest was the relationship between the preoperative NLR and long-term mortality of patients who underwent vascular surgery. A secondary outcome analyzed was the association of preoperatively measured NLR with 30-day mortality in this setting. Other outcomes related to post-surgical vascular complications were analyzed qualitatively in a narrative review.
Statistical Analysis and Data Synthesis
We tabulated the maximally adjusted reported HRs and log-transformed ORs with associated 95% confidence intervals (CIs) from each included study and generated summary estimates using mixed effects modeling. Statistical heterogeneity was estimated using the Chi-square statistic. Where fewer than 10 studies reported an outcome, we were unable to perform a meta-regression to explore between-study heterogeneity and instead sources of clinical heterogeneity were assessed qualitatively. All analyses were performed using the R statistical package “metafor,” and figures were generated using “ggplot2”. 18,19 Where fewer than 10 studies were included, publication bias was not formally assessed. We performed a post-hoc sensitivity analyses to determine whether outlier NLR thresholds contributed to statistical heterogeneity.
Results
Search Results
A total of 1,329 studies were identified through a comprehensive search of three databases, and an additional 150 studies were found through other sources. Exclusion of duplicates and irrelevant references resulted in 1,397 articles which underwent title and abstract screening. Finally, 29 potentially relevant studies were identified for full-text review, from which 14 articles were selected for inclusion in this systematic review (Figure 1—PRISMA Flow Chart). Of these, 5 studies were not included in the meta-analysis as their data did not include survival outcomes, but did report incidence of other important complications following non-cardiac, non-cerebral vascular surgery. The characteristics of these 14 eligible studies are detailed in Table 1.
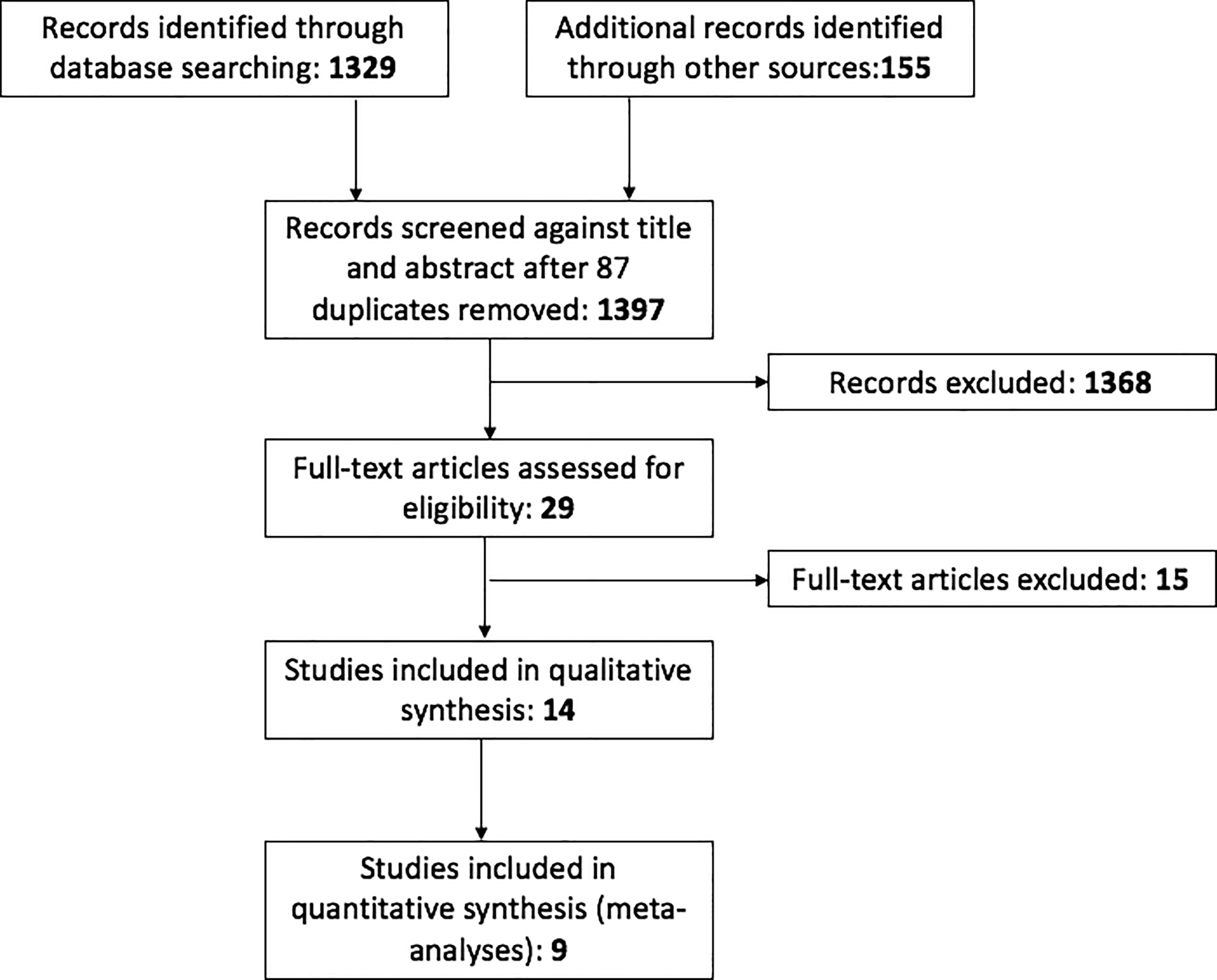
PRISMA flow diagram.
Characteristics of Included Studies.
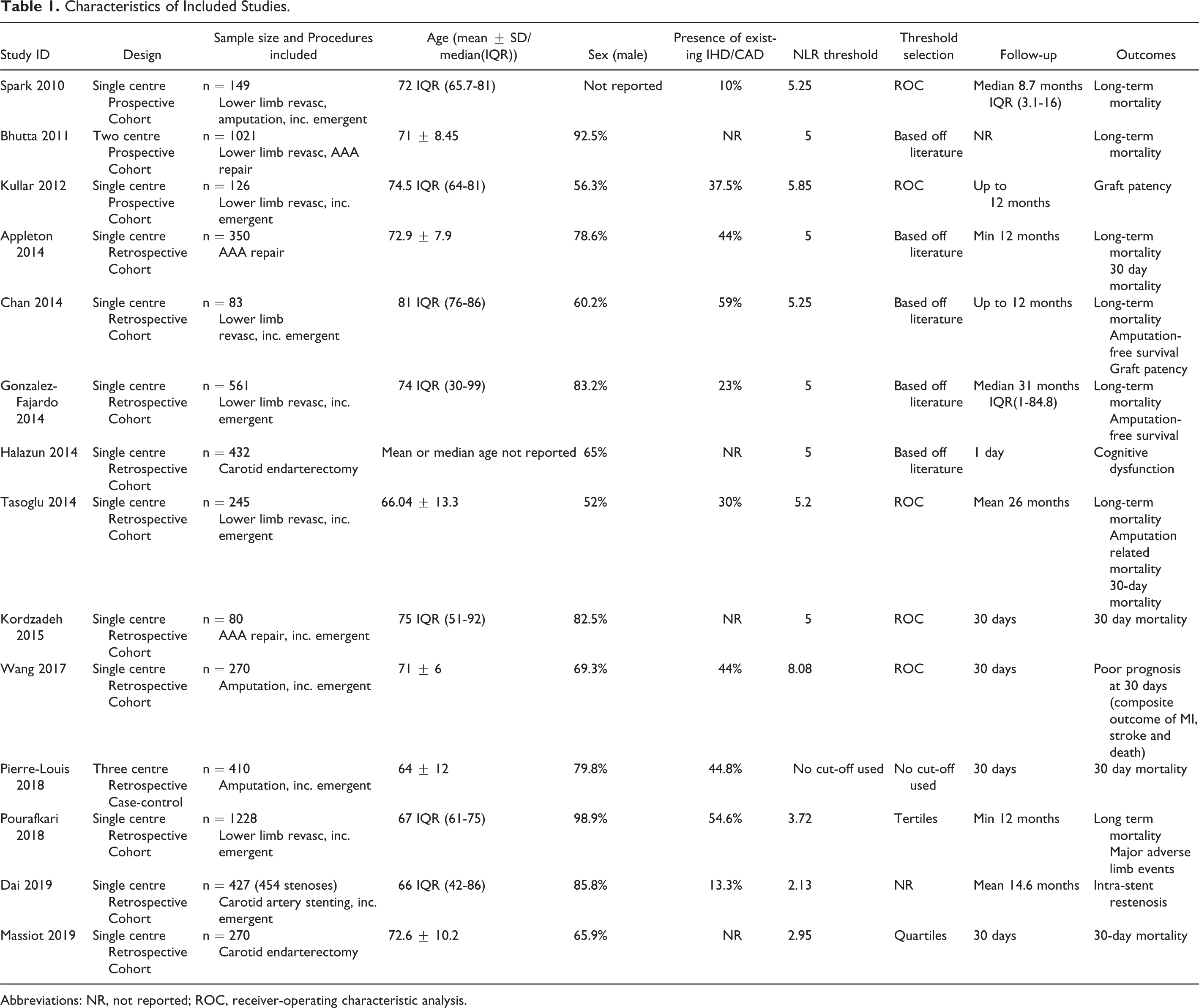
Abbreviations: NR, not reported; ROC, receiver-operating characteristic analysis.
Description of Included Studies
The 14 studies included were published between 2010 and 2019 and together involved 5,652 participants, 20- 33 from a wide variety of ethnic backgrounds and healthcare contexts. The majority (10 out of 14) of included studies were retrospective observational cohort studies using prospectively maintained hospital databases to select and analyze data from patients meeting their study criteria over the course of pre-defined years. Three studies incorporated in this review were prospective observational cohort studies, reporting data relevant to our review, 20,26,30 and one study was a case-control design reporting relevant data. 28 All studies analyzed preoperatively measured NLR in patients who had undergone vascular surgery (not involving cardiac or neurosurgical operations). All studies had 80 patients or more, 2 of which had over 1,000 participants. 20,29
Information on patient follow-up time, patient sex, presence of ischemic heart disease (IHD)/coronary artery disease (CAD), and NLR measurements and cut-offs used were available for meta-regression. Other pre-defined covariates were either not reported or reported heterogeneously and were therefore not included in the meta-regression. Between studies there was some discrepancy in the methods used to stratify patients based on pre-procedural NLR. Ten studies used a pre-defined NLR cut-off informed by prior research or ROC curve analysis to stratify the study populations into groups above and below this level. Two studies used NLR quantiles based upon the distribution NLR values measured preoperatively in their study population. Of these, one used tertiles and one used quartiles. 27,29 One study looked at the mean preoperative NLR of those in the study who had died, and those who had not. 28
Methodological Quality
The overall methodological quality of the included studies was generally good (Online Appendix). Three studies did not adjust for potential confounders using multivariate regression modelling, 25,27,34 and one study adjusted for <5 covariates, 32 thus likely had residual confounding. These studies were assessed as having a high risk of potential bias. Otherwise there was only a small amount of uncertainty regarding outcomes, time-to-outcome, data analysis, and attrition rate in some studies; and these were deemed at an unclear risk of bias. 24,26,28,30
Long-Term Mortality
Meta-analysis of 7 studies involving 3,637 patients found a moderate association between elevated preoperative NLR and long-term mortality after vascular surgery, which reached statistical significance (HR 1.40[95%CI: 1.13-1.74]) (Figure 2—Long-term Mortality). 21,22,23,29,31,34 There was moderate between-study heterogeneity (chi-squared 60.8%). Potential sources of between-study heterogeneity included: differences in the type of vascular surgery performed, number of potential confounders adjusted for in multivariate analysis, the basis on which NLR threshold was selected, time of publication of study (ranged from 2010-2018), differences in the presence of cardiovascular risk factors (presence of reported IHD/CAD ranged from 10-60%), and male sex (ranging from 52-99%). In the post-hoc sensitivity analysis, the inclusion of Pourafkari 2018, which use an NLR cutoff of 3.7, did not contribute to statistical heterogeneity as evidenced by overlapping 95% confidence intervals (sensitivity HR 1.51 [95% CI 1.18-1.94]).
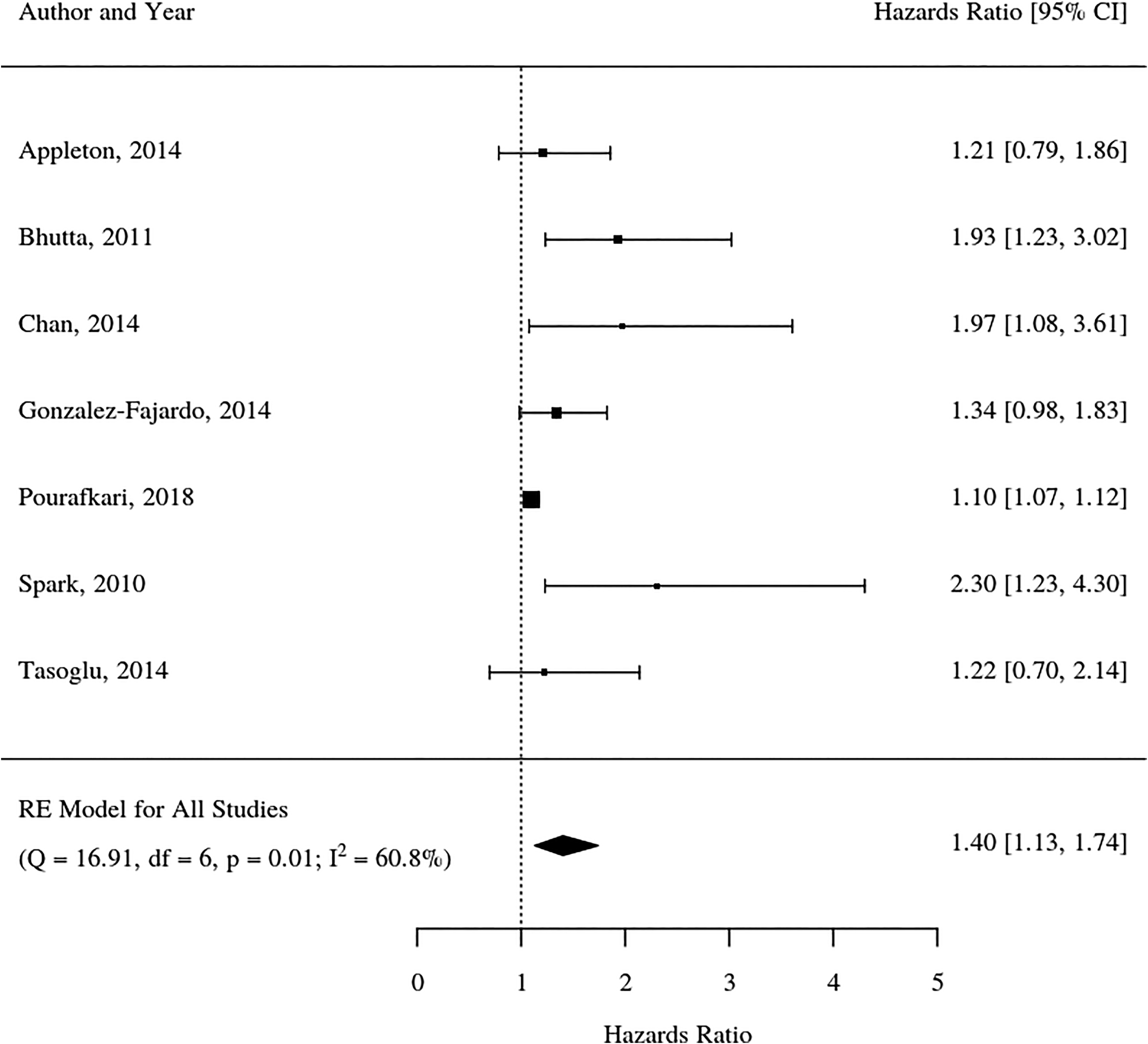
Forest plot for long-term mortality.
Short-Term Mortality
Four studies involving 945 patients were meta-analyzed, and an increased odds of 30-day mortality was associated with elevated preoperative NLR (OR: 3.08; 95%CI: 1.91-4.95) (Figure 3—30-day Mortality). 25,27,31,34 There was a moderate degree of between-study heterogeneity (chi squared 66.59%) and potential sources of between-study heterogeneity were similar to what was found in the long-term mortality analysis; particularly differences in operative cohort, with each study population undergoing different vascular surgical procedures (open AAA repair, carotid endarterectomy and lower-limb revascularization). A study by Pierre-Louis et al. (2018) was excluded from the analysis because no HR or OR was reported.
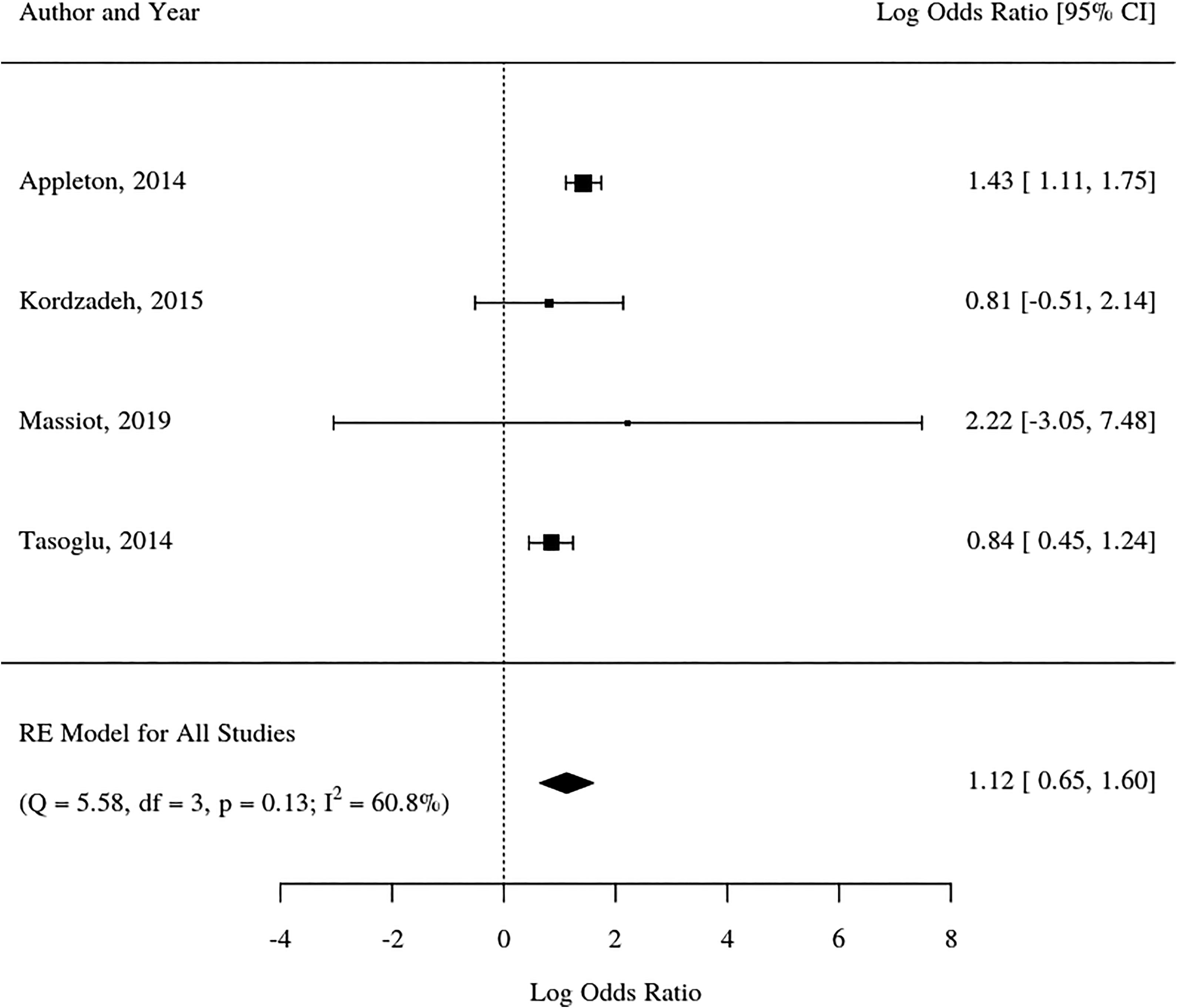
Forest plot for 30-day mortality. Log-transformed odds ratios are displayed. The line of statistical significance is 0.
Vascular Complications
Chan et al. (2014) and Gonzalez-Fajardo et al. (2014) both measured amputation free survival (AFS) as a primary outcome following limb revascularization in patients with critical limb ischemia (CLI). Chan et al. found that over 12 months, the NLR >5.25 patient group had no significant decrease in AFS compared with the NLR <5.25 patient group (HR: 1.86; 95%CI: 0.83-4.4). 21 Gonzalez-Fajardo et al. found that over 5 years, patients with NLR >5 had a significant decrease in AFS compared to the NLR <5 patient group (HR: 2.33; 95%CI: 1.73-3.12). 23
Tasoglu et al. (2018) measured amputation as an outcome following lower-limb revascularization and found that over a mean follow up time of 26 months, patients who had a raised NLR (>5) had more amputation events (P-value = 0.001). 31
Graft-patency at 12 months was reported in 2 studies where lower limb bypass grafting was performed on patients with CLI or peripheral arterial disease (PAD). 21,26 Chan et al. (2014) found that an NLR >5.25 was not significantly associated with reduced graft patency at 12 months compared with the NLR <5.25 patient group (HR: 1.03; 95%CI: 0.74-1.43). 21 Kullar et al. (2012) had similar findings, showing that at 12 months postoperatively, raised preoperative NLR (>5.85) was not significantly associated with reduced graft-patency compared with the NLR <5.85 patient group (OR: 0.87; 95%CI: 0.74-1.03). 26 Dai et al. (2019) also investigated the effect of NLR on vascular patency, reporting on intra-stent restenosis (ISR) in their patient population undergoing carotid artery stenting (CAS). They found that over a mean follow up time of 14.6 months, patients with a raised NLR (>2.13) were almost three times as likely to develop ISR (defined as stenosis over 50%) (HR: 2.74; 95%CI: 1.46-5.14). 22
Pourafkari et al. (2018) investigated the predictive role of pre-procedural NLR in the development of major adverse limb events (MALE) after elective lower-limb revascularization for PAD. MALE included limb amputations, open revision and bypass procedures, or thrombolysis procedures on the same leg. Results showed that over patient follow up (minimum 12 months) raised NLR (>3.72) was associated with greater incidence of MALE than in the NLR <3.72 patient group (HR: 1.09; 95%CI: 1.07-1.12). 29
Wang et al. (2017) reported on the relationship between elevated NLR and poor prognosis after amputation for severe CLI. This was a compound outcome that included death, myocardial infarction (MI) and stroke. They showed a strong association between preoperative NLR >8.08 and poor prognosis at 30 days post-amputation, with those in the raised NLR group having an almost 26-fold greater odds of outcome compared to patients with NLR <8.08 (OR: 26.23; 95%CI: 5.8-118.58). 32
Discussion
In this systematic review and meta-analysis, we found elevated preoperative NLR to be a promising prognostic biomarker for both long- and short-term mortality following vascular surgery. These results support the hypothesis that increased preoperative systemic inflammation is prognostically significant in both emergent and elective vascular surgery. NLR is routinely available from the full blood count and may present an accessible and cost-effective risk stratification tool. Definitions of elevated NLR within included studies was varied, and establishing a universal NLR cut-off remains a priority for research.
Pooled analysis of data from 3,637 patients in 7 separate studies showed that raised preoperative NLR increased the risk of long-term all-cause mortality following vascular surgery by 40% (HR 1.40 [95%CI: 1.13-1.74]). Raised preoperative NLR was associated with a statistically significant increased odds of 30-day mortality in patients undergoing vascular surgery, as observed in pooled analysis of data from 945 patients over 4 separate studies (OR: 3.08; 95%CI: 1.91-4.95).
Interestingly, some of the excluded studies, as well as a small number of the included studies also evaluated postoperative NLR, which can indicate an inflammatory response to surgery. While those results were not incorporated into our analyses, postoperative NLR as well as the change in NLR value between the pre and postoperative time points could represent important prognostic biomarkers warranting future research.
NLR has been shown to be a marker of inflammation closely related to cardiovascular events for over 10 years, 34,35 and it is well known that perioperative cardiovascular events make up a large component of perioperative morbidity and mortality. 36 Evidence from cardiovascular surgery studies repeatedly demonstrate that an elevated NLR is a good prognosticator of adverse patient outcome in such inflammation-centric diseases. One literature review, 37 2 systematic reviews with meta-analysis, 8,38 and 2 reviews 7,39 have been conducted thus far, analyzing the role of NLR in prognostication of occlusive vascular disease, and vascular surgery including cardiovascular surgery. NLR has emerged in each of these studies to have a prognostic utility independent of already recognized risk factors.
NLR has been shown to be influenced by medications in frequent use in the vascular surgery population. Fici et al. (2013) showed a significant decrease in NLR in patients beginning antihypertensive therapy, while Akin et al. (2013) showed that therapeutic treatment with statins resulted in a significant reduction in NLR. 40,41 Only a minority of included studies controlled for statin use in their statistical analyses. Future research should evaluate whether pre-operative statin and anti-hypertensive use modulate the prognostic significance of NLR. Additionally, whether active NLR-lowering strategies are safe and effective in vascular surgery should be evaluated.
Novascular surgery guidelines currently recommend routine NLR measurement pre- or postoperatively. This may be because there is no universally accepted threshold marker of increased risk. Heterogeneity in the thresholds for this review, limits its guidance for defining what constitutes raised NLR. It would make sense that a higher NLR threshold would be more sensitive in identifying patients at greatest risk of post-surgical complications or morbidity, and one study involved in this systematic review did in fact report 26-fold greater odds of outcome (poor-prognosis at 30 days after surgery) when NLR threshold was set at 8.08, where other studies tended to use a value around 5, and had more conservative findings. 32 Further research is needed to create a generalizable NLR elevation threshold from high quality, multicenter, prospective ROC studies. Although the evidence is preliminary, once an acceptable threshold has been defined, NLR measurement should be considered during pre-vascular-surgical work-up, to aid perioperative decision making and risk stratification.
The present study should be interpreted with consideration to the following limitations. For both meta-analyses, heterogeneity was moderate, and could be partially explained by variables such as type of surgery performed and threshold of NLR used. We were unable to explore this heterogeneity further by conducting a full and rigorous meta-regression due to under-reporting of relevant covariates and the number of included studies. Selection bias of papers to be included in this review cannot be definitively excluded, however this was minimized by having independent researchers screening the title/abstract and full-text phases. Additionally, risk of publication bias is also unable to be excluded, however the search strategy was designed to be expansive and encompassing of studies with all kinds of results reported. Limitations that were more difficult to mitigate in this study were that most of the involved papers were retrospective in nature. This introduces bias into these individual studies by way of participant selection, and a lack of control for exposure or outcome assessment by the researchers, who rely on databases for record keeping.
This systematic review and meta-analysis found that elevated preoperative NLR was associated with worse short- and long-term survival in vascular surgery. Differences between prognostic value of preoperative and postoperative NLR must be elucidated, as well as any significance of the change in NLR from preoperative to postoperative measurement. Furthermore, standardized thresholds to demarcate “elevated” NLR should be ascertained. More robust, randomized, prospective trials investigating this trend with adjustment for relevant covariates would help in finding a place for routine NLR measurements in risk stratification for perioperative care. Early identification of at-risk patients may allow for mitigation of vascular surgical complications, medication optimization, and enhanced perioperative care. As a preoperative biomarker, NLR shows prognostic promise and should be a consideration in current clinical practice once acceptable thresholds for interpretation can be determined.
Supplemental Material
Supplemental Material, ONLINE_SUPPLEMENT - Prognostic Significance of Preoperative Neutrophil-Lymphocyte Ratio in Vascular Surgery: Systematic Review and Meta-Analysis
Supplemental Material, ONLINE_SUPPLEMENT for Prognostic Significance of Preoperative Neutrophil-Lymphocyte Ratio in Vascular Surgery: Systematic Review and Meta-Analysis by Sarah M. Jackson, Luke A. Perry, Carla Borg, Dhruvesh M. Ramson, Ryan Campbell, Zhengyang Liu, Jacqueline Nguyen, Ned Douglas, Juliana Kok and Jahan Penny-Dimri in Vascular and Endovascular Surgery
Footnotes
Acknowledgments
We would like to thank Cochrane Australia and Covidence for their support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.