
Abstract
Objective:
The aim of our study was to assess the prevalence of renal masses suspected of malignancy and adrenal incidentalomas in patients with abdominal aortic aneurysm based on the computed tomography angiography (CTA).
Methods:
In the retrospective cross-sectional study, the CTA scans of patients with abdominal aortic aneurysms and thoraco-abdominal aortic aneurysms type II-IV were assessed. Patients with thoraco-abdominal aortic aneurysms type I and V and history of abdominal aortic surgery were excluded from the study.
Results:
Study group comprised 937 patients with a median age of 73.0 years, 83.8% of whom were male. CTA revealed renal tumors in 11 patients (1.2% of the study population) with a median size of 26 mm (interquartile range 20-50). Adrenal incidentalomas were found in 61 patients (6.5% of the study population). In 20 patients (2.1%) adrenal lesions were found bilaterally.
Conclusion:
In the described cohort, the renal and adrenal tumors were relatively common findings among patients with abdominal aortic aneurysm and thoraco-abdominal aortic aneurysms type II-IV. Both anaesthesiologists and surgeons should be vigilant about the possibility of such coexistence in order to provide the patients with the best possible perioperative care and an optimal surgical modality.
Keywords
Introduction
The abdominal aortic aneurysm (AAA) is 1 of the most common vascular diseases in the elderly population and is associated with significant mortality. 1 According to the recent guidelines, computed tomography angiography (CTA) is the recommended imaging modality for therapeutic decision making and treatment planning, as well as for the confirmation of aneurysmal rupture. 2
Nowadays, both adrenal and renal masses are usually diagnosed accidentally on abdominal ultrasound or computed tomography (CT) performed for other medical indications. Most of the identified renal lesions are eventually diagnosed as benign cysts, which are detected in up to 40 percent of adults who undergo abdominal CT. 3 However, aside from benign findings, masses suspected of malignancy are occasionally revealed thus warranting an urgent investigation. 4 With increasing utilization of cross-sectional imaging, the number of incidentally detected cases of renal cancer is increasing up to approximately 74,000 new cases annually in the United States and 84,000 in the European Union.5,6 The treatment of choice for small renal masses, defined as smaller than 40 mm, is partial nephrectomy, however active surveillance and ablative therapies are viable alternatives in elderly and/or comorbid patients. Surgical approach (partial or radical nephrectomy) is recommended for lesions greater than 40 mm.4,7,8
The reported incidence of adrenal incidentalomas revealed in the thoracic and abdominal computed tomography varies from 0.8 to 5% in the general population.9-11 Most of them are non-secreting adenomas.12,13 However, it is estimated that 10 to 15% of adrenal incidentalomas produce excessive amounts of hormones, in most cases leading to development of subclinical Cushing’s syndrome.12,13 Approximately 3% of them prove to be catecholamine-secreting tumors. 12 Although the majority of these adrenal masses are benign, the likelihood of them being diagnosed as adrenocortical carcinoma strongly depends on the size of the lesion.14-16 Therefore, current guidelines recommend surgery for all adrenal incidentalomas greater than 40 mm, even if imaging characteristics (like homogeneity and high concentration of lipids) suggest a benign nature of the mass.14-16
Incidental renal and adrenal findings in CTA performed in patients with AAA may warrant some additional and urgent testing, and therefore, delay elective AAA repair.4,11
The current data are scarce and the actual incidence of coexisting renal and adrenal lesions in patients with AAA detected on CTA remains unknown. Thus, we performed this study to establish the prevalence of coexisting renal masses suspected of malignancy and adrenal incidentalomas in patients with AAA based on the CTA.
Material and Methods
Study Design
The presented study was performed at the Vascular Center at St. John Grande Hospital in Kraków between October 2010 and July 2017. In each enrolled patient we retrospectively analyzed CTAs of abdominal aorta performed using the 32-slice spiral CT scanner—Aquilion 32, Toshiba.
Eligible patients were identified in a database containing imaging studies of patients treated in our center. We included the most recent scans of the patients with a diagnosis of AAA or thoraco-abdominal aortic aneurysm (TAAA) type II-IV (according to the Safi modification of Crawford TAAA classification 17 ) without any history of abdominal aortic surgery. Patients diagnosed with TAAA type I and V (without the involvement of the infrarenal aorta) were excluded. All CTA scans were evaluated by a certified radiologist.
The study protocol complied with the Helsinki Declaration and was approved by The Bioethics Committee of The Regional Chambers of Physicians in Kraków (No. OIL/KBL/13/2016). Patient`s written consent was not required.
Definitions
The transverse planes diameter of ≥ 30 mm for the infrarenal aorta was used to define the aortic aneurysm. 2
Incidental adrenal lesions and renal masses were identified on contrast-enhanced abdominal aortic CTA, typically assessed before and after the intravenous administration of 1 mL/kg of low-osmolar contrast material (Optiray 300, Guerbet, France). The number and size of the adrenal and renal masses for each patient were recorded.
Renal masses were suspected of malignancy if they were characterized by presence of 4,8: solid renal mass especially heterogeneous, with interspersed fat and calcification or homogeneous mass with enhancement greater than 15 Hounsfield unit (HU) after contrast administration renal cyst classified as III or IV according to Bosniak renal cyst classification system
Renal lesions suspected of malignancy, originating from the renal pelvis or ureter, were excluded from the analysis.
An adrenal incidentaloma was defined as a mass lesion greater than 1 cm in diameter, discovered incidentally by radiologic examination performed for other reasons. 16
Comorbidities
Patients` baseline characteristics and comorbidities were gathered based on a comprehensive analysis of medical records obtained by physicians during the hospitalization or consult in an outpatient clinic. Comorbidities (hypertension, diabetes mellitus, peripheral artery disease, coronary artery disease, congestive heart failure, chronic obstructive pulmonary disease and history of cerebrovascular events, severe chronic kidney disease and smoking) were identified on the basis of medical records, use of medications typical for given condition and symptoms confirmed by physical examination or tests appropriate for each disease i.e. blood pressure measurement, fasting plasma glucose or oral glucose tolerance test, ankle-brachial index, CTA, electrocardiogram, echocardiography, chest x-ray image, lung function tests, computed tomography and glomerular filtration rate < 30 mL/minute/1.73 m2 calculated according to the Modification of Diet in Renal Disease formula). Definitions of comorbidities used in this study were described in detail in a previous report. 18
Statistical Analysis
We presented categorical variables were as counts (percentages), and continuous variables as medians (25-75 quartile range) unless otherwise specified. The continuous variables were compared using the Mann-Whitney U test. A 2-sided P value < 0.05 was considered statistically significant. We performed the statistical analysis with the Statistica 13.1 software (StatStoft®, Tulsa, OK, U.S.A.).
Data Availability
The data associated with the paper are not publicly available but are available from the corresponding author on reasonable request.
Results
Study Population
We identified 1281 patients, who underwent CTA of abdominal aorta between October 2010 and July 2017, of whom 937 were diagnosed with AAA or TAAA type II-IV with no history of abdominal aortic surgery and had a complete CTA imaging. The study sample comprised 746 males (83.8%) and the median age was 73 years (67-79). The most common comorbidities were hypertension (85.6%), coronary artery disease (45.9%) and peripheral artery disease (30.1%). Detailed demographic and clinical characteristics of the study group are shown in Table 1. Data concerning comorbidities were missing for 19 (2.0%) of patients in the study group.
The Study Group Characteristics.
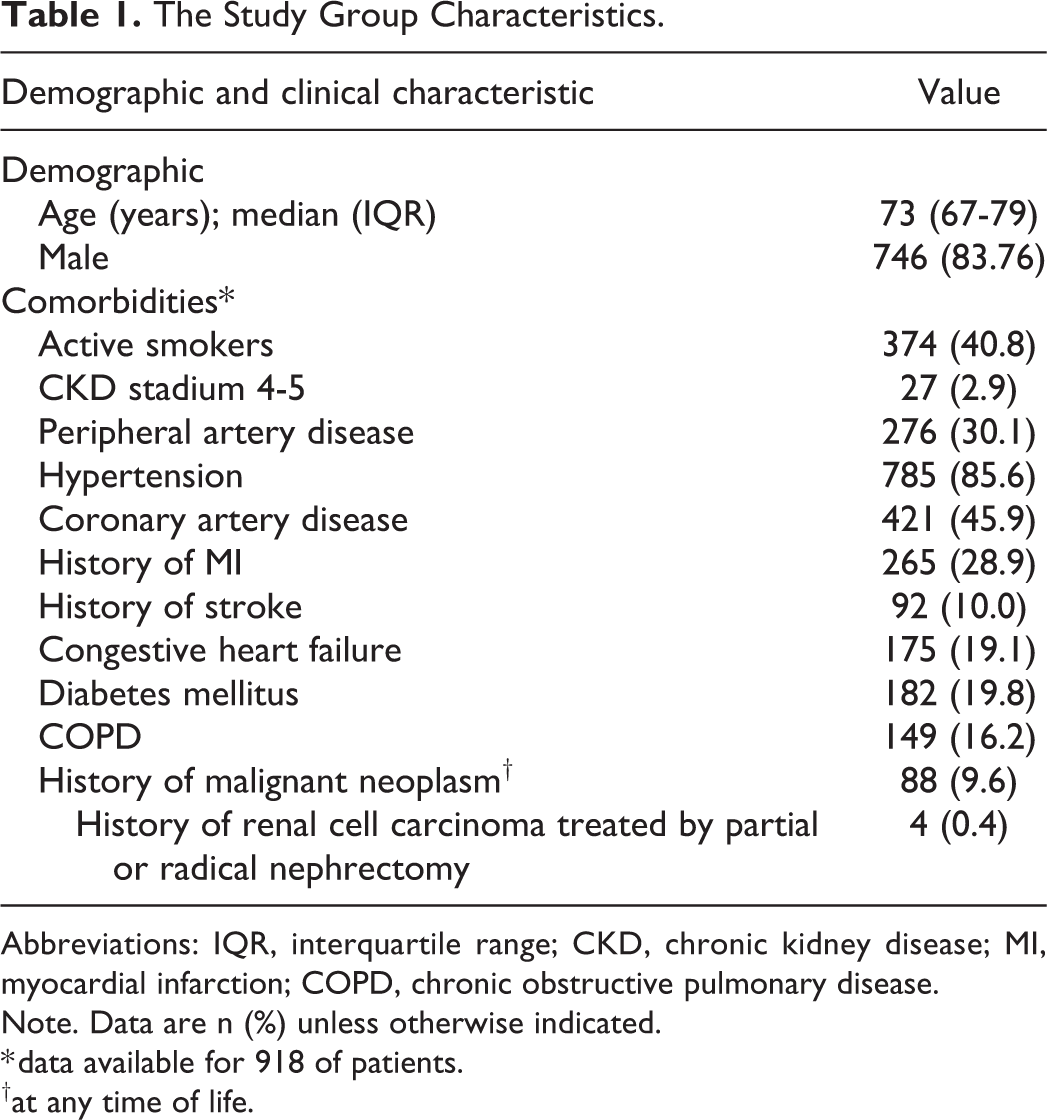
Abbreviations: IQR, interquartile range; CKD, chronic kidney disease; MI, myocardial infarction; COPD, chronic obstructive pulmonary disease.
Note. Data are n (%) unless otherwise indicated.
* data available for 918 of patients.
†at any time of life.
Concomitant Renal Masses
Overall, concomitant renal tumors were found in 11 patients (1.2% of the study population) with median size 26 mm (IQR 20-50). Among them 10 (90.9%) masses were solid and 1 (9.1%) was classified as renal cyst IV according to Bosniak renal cyst classification system. In 4 cases (36.4%) lesions were greater than 40 mm. Three patients (27.3%) had simultaneous focal lesions in the adrenal glands. The prevalence and distribution of renal masses suspected of malignancy are shown in Table 2.
Prevalence and Diameters of Renal Masses Suspected of Malignancy and Adrenal Incidentalomas.
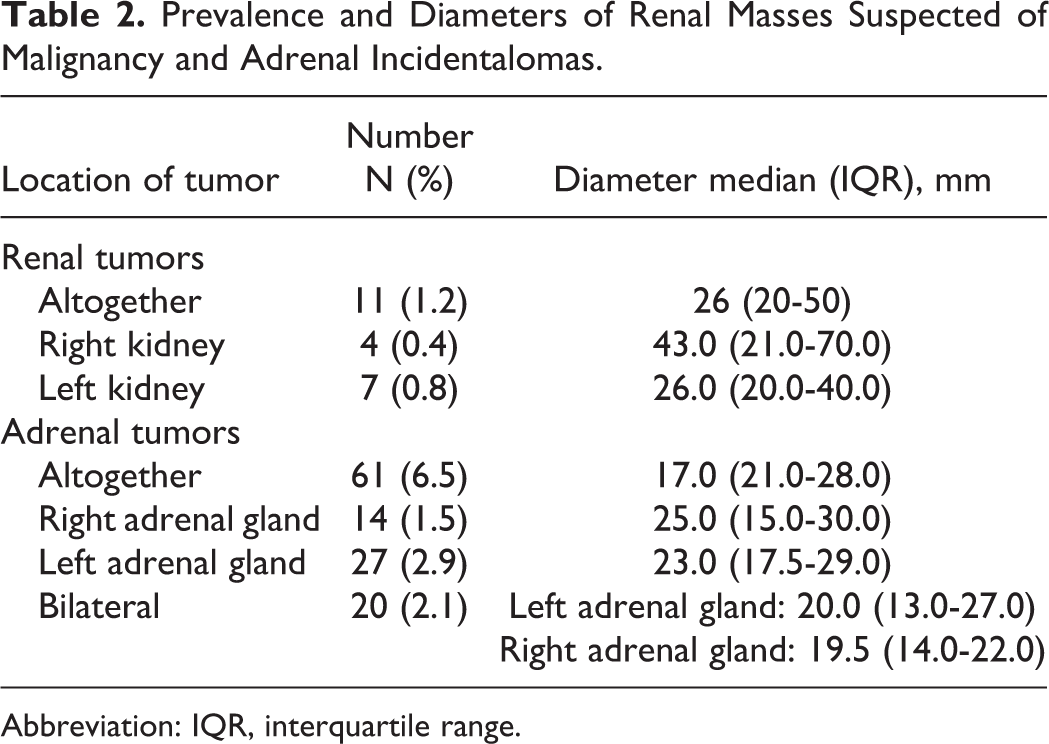
Abbreviation: IQR, interquartile range.
We analyzed the surgical approach taken in patients with concomitant renal tumors: 1 patient underwent simultaneous open aortic surgery and radical nephrectomy endovascular aortic repair was performed in 3 patients. open aortic surgery was performed in 3 patients (1 of them died shortly after surgery because of postoperative complication) 4 patients were qualified for endovascular aortic repair, however, 1 of them died before surgery because of reason unrelated to abdominal aortic aneurysm nor renal tumor and 3 patients did not consent to the proposed treatment.
In 2 patients renal cell carcinoma was diagnosed after radical nephrectomy (in 1 case, as mentioned above, performed simultaneous with AAA repair and in 1 case performed few months after endovascular aortic repair). Unfortunately, data regarding results of postoperative urology consultation and the type of proposed treatment (radical or partial nephrectomy or active surveillance) in other patients are not available.
Concomitant Adrenal Incidentalomas
Concomitant adrenal incidentalomas were found in 61 patients (6.5% of the study population). However, only in 3 cases (4.9%) lesions were greater than 40 mm. The prevalence and distribution of adrenal incidentalomas are shown in Table 2.
In a subgroup of 61 patients with adrenal incidentalomas, 36 patients underwent aortic repair (open repair in 24 cases and endovascular repair in 12 cases). In this subgroup 31 patients underwent an elective procedure, however, only 11/31 (35.5%) had endocrinology work-up before the aortic repair. In all cases, non-secreting adenomas were diagnosed and none of the patients were qualified for adrenalectomy.
Importantly, median interval between the AAA diagnosis and the procedure was significantly longer in patients who had endocrinology consultation (12.5 vs. 4.5 weeks, p = 0.033) compared to those who did not have such work-up prior to the surgery.
Discussion
Presented retrospective cross-sectional study reports the prevalence of renal masses suspected of malignancy and adrenal incidentalomas in patients with AAA. The results were partially consistent with previously published data. Veraldi et al showed that among 913 AAA patients who underwent open or endovascular aneurysm repair (EVAR), renal cell carcinomas (RCCs) were found in 1.3% of individuals. 19 Similar results were presented by Habets et al (1.3% rates of RCC among 385 patients who were qualified to EVAR). 20 However, Maeda et el. identified RCC in only 0.43% of 1175 patients with AAA who underwent EVAR. 21 The presented study is the first cross-sectional study describing the incidence of renal masses suspected of malignancy based on CTA in patients diagnosed with AAA, while the above mentioned studies included exclusively patients undergoing surgical AAA repair.
To our knowledge this is the first study reporting the prevalence of adrenal incidentalomas based on CTA in patients suffering from AAA. Previous studies on the general population showed the incidence of adrenal incidentalomas diagnosed by thoracic or abdominal CT to range from 0.5% to 5.0%.9-11,22 Compared to other available studies, the prevalence of incidentalomas in our cohort is relatively high, however further studies are warranted to evaluate the association between aortic aneurysm and the presence of adrenal incidentalomas.
Aside from its descriptive value, our findings might potentially have important clinical implications. Presence of AAA and concomitant malignancy represent a challenging issue in terms of treatment priority, timing, and expected outcome. Elective AAA repair is a prophylactic procedure performed if the lifetime risk of rupture exceeds the risk of treatment. Therefore, the prognosis of concomitant neoplasm is crucial in the decision making process together with other comorbidities and patient’s preference. 2 Nowadays, EVAR with its low short-term morbidity and mortality offers improved treatment of patients with AAA and concomitant renal tumor. According to the current guidelines EVAR is the intervention of choice for these patients.2,20,23 However, if the patient is not suitable for endovascular repair, a synchronous open approach may be considered. 2
Unlike renal tumors, adrenal incidentalomas are mostly benign lesions and the risk of adrenocortical carcinoma is relatively low. 15 However, the presence of adrenal lesion might become an important clinical issue. Even though the majority of adrenal incidentalomas are non-functional, according to the current guidelines all patients with adrenal lesions should undergo tests for Cushing’s syndrome and pheochromocytoma.16,24 In addition, in all patients with hypertension and/or hypokalemia the exclusion of aldosteronoma is warranted. 24 Functional adrenal mass could be a serious comorbidity, especially in the described clinical setting as the excess of catecholamines produced by pheochromocytoma can cause sustained or paroxysmal hypertension which increases the risk of aneurysm rupture and probability of cardiovascular complications during the surgical procedure.2,25,26 Clinical manifestation of hypercortisolism in the midst of others includes hypertension and elevated cardiovascular risk. 27 The relatively high prevalence of adrenal incidentalomas among patients with AAA showed in the study may imply, that adrenal lesions might become significant clinical issue in this population.
Our study discovered renal cell carcinoma was eventually confirmed in both patients with known histopathological tumor status. Unfortunately, this observation is based on a very small sample and therefore should be treated with caution and warrants further investigation. Our study also revealed an alarming observation that majority of patients with adrenal incidentalomas did not undergo endocrinology consult before surgery. We believe that there is a room for improvement in this aspect of care and that more attention should be paid by clinicians to appropriate preoperative management of patients with AAA according to the current endocrinological guidelines. In general, patients with concomitant renal or adrenal masses should be referred to an appropriate specialist before AAA repair. Later, an optimal surgical approach should be selected by a clinical team including vascular surgeon and urologist or endocrinologist depending on the characteristics of AAA and renal or adrenal mass as well as patient condition and comorbidities.
The study has several limitations. The patients with ruptured AAA were excluded, as they were initially diagnosed outside of the Vascular Center and the CTAs were not available for evaluation. Moreover, the sequential CTA analysis as well was not done, despite in some cases more than 1 CTAs were available. Finally, the authors had no access to all histopathological findings so the actual nature of some discovered tumors remains unknown.
Conclusion
Coexistence of renal and adrenal tumors with abdominal aortic aneurysm and thoraco-abdominal aortic aneurysms type II-IV was described in approximately 7.4% of enrolled patients. In the light of high perioperative risk immanently associated with aortic repairs, it is crucial for both surgeon and an anesthesiologist to have as much knowledge as possible about patient`s diseases potentially altering surgical modality and perioperative management.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.