
Abstract
Carotid blowout syndrome (CBS) is defined as a rupture of common carotid artery or its branches. Endovascular intervention has been advocated as first line of treatment for CBS. This Case Report describes 5 patients with prior history of head and neck cancer who presented with CBS. Two patients presented as acute, 2 as impending, and one as threatened CBS. The lesions found were pseudoaneurysm and focal vascular irregularities involving the common carotid artery, cervical internal carotid artery and lingual artery. Embolization and occlusion with detachable coils of the artery was used in all patients. Technical success and immediate hemostasis were achieved in all patients. One patient presented transient cranial nerve palsy. No recurrent CBS was reported during the follow-up. In our experience, coil embolization, if possible, is a safe and efficient technique in treatment of CBS secondary to head and neck cancers.
Introduction
Carotid blowout syndrome (CBS) is defined as a rupture of common carotid artery or its branches. CBS is a rare but life-threatening complication that occurs in up to 4% of patients after major oncological surgery for advanced head and neck cancer, especially in previously irradiated necks.1,2 CBS develops when a damaged arterial wall cannot sustain its integrity, mainly in patients who have undergone surgical procedures and/or radiotherapy (RT) due head and neck tumors. 2
Chaloupka et al 3 classified CBS into 3 types as grade 1 or “threatened blowout,” in which there is a clinically exposed vessel through soft tissue breakdown; grade 2 or “impending blowout,” in which a sentinel bleed occurred at or near the time of presentation but resolved spontaneously or with conservative measures; and grade 3 or “acute CBS”, with acute or ongoing bleeding usually requiring resuscitation or emergent intervention.
The cumulative mortality and morbidity of untreated CBS are 40% and 60%, respectively.3,4 For these reasons, identification at the early stages and prevention of grade 3 CBS are crucial. 5 Emergency surgical ligation has been traditionally the only therapeutic maneuver available for CBS. 3 However, surgical management of CBS is usually difficult because the procedures must often be performed in previously irradiated or infected fields; in these circumstances, emergency open surgery is usually complicated by local wound infection, tissue fibrosis and/or necrosis, hemodynamic instability, profound hypotension, global cerebral ischemia and consumptive coagulopathy secondary to extreme blood loss. 2 Recently, endovascular intervention by means of balloon occlusion, coil embolization or covered stent-graft placement has been advocated as first line of treatment for CBS.6,7
Case Reports
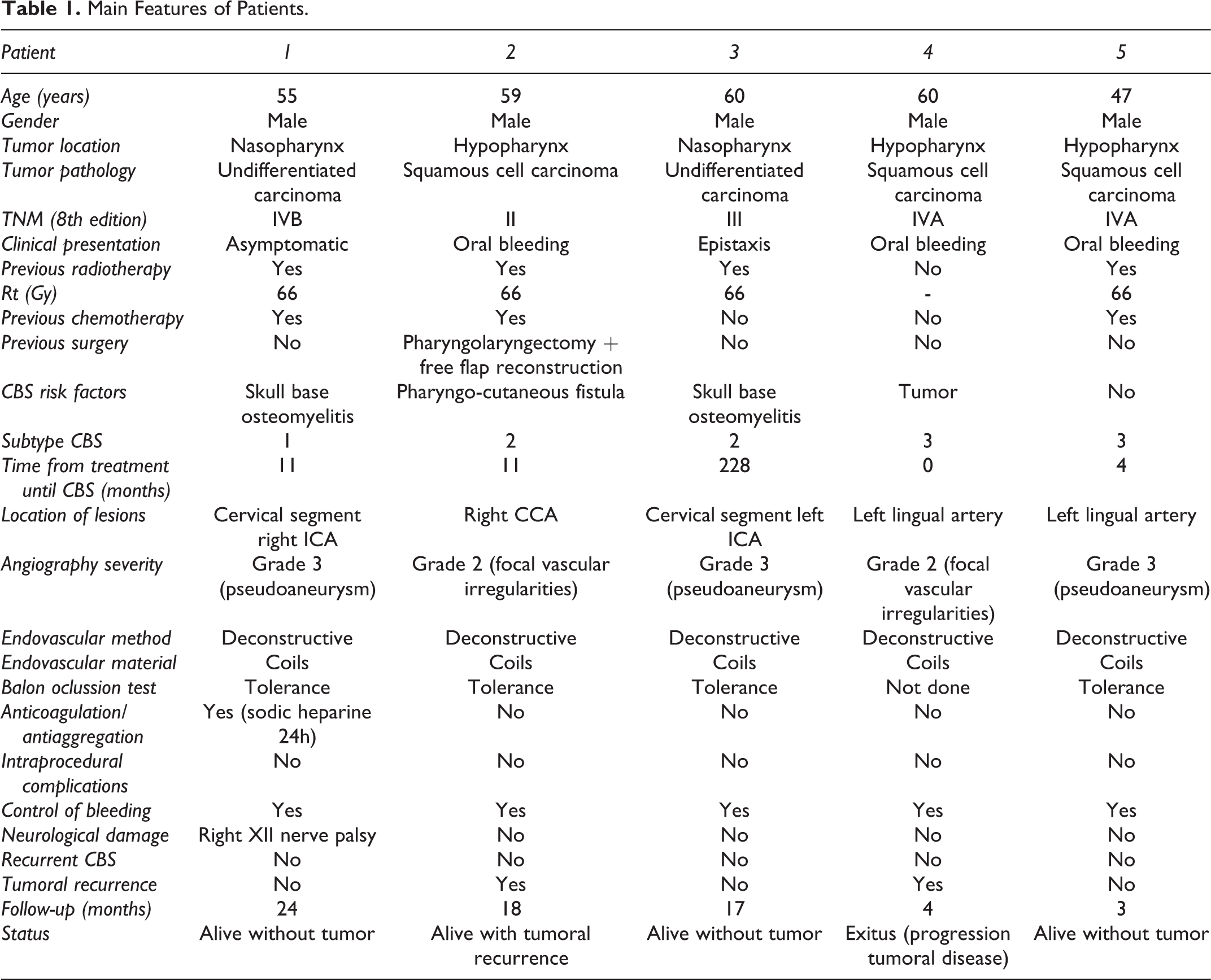
This single-institution retrospective report was approved by Regional Ethical Committee and written consent was obtained from each patient. The features of these 5 patients with CBS treated by endovascular embolization in our department between 2015 and 2020 are summarized in the Table 1.
Main Features of Patients.
All patients but one presented in our emergency department with severe oral bleeding or epistaxis. A patient with nasopharyngeal carcinoma (patient 1) was diagnosed with CBS while performing a CT scan to follow up on a skull base osteomyelitis. In 1 patient the oral bleeding was the presenting symptom of the tumor, and in the remaining 3 CBS was suspected due to a prior history of surgery or radiation for a head and neck tumor.
After patients were found to be hemodynamically stable, an emergency digital subtraction angiography (DSA) of the carotid arteries was performed in all cases for the diagnosis of the source of bleeding. According to the patients’ clinical presentation, 2 patients were classified as acute, 2 patients as impending, and one as threatened CBS.
The lesions found were pseudoaneurysms (n = 3) and focal vascular irregularities (n = 2) involving the common carotid artery (CCA, n = 1), internal carotid artery (ICA, n = 2), and lingual artery (n = 2) (Figures 1 and 2).
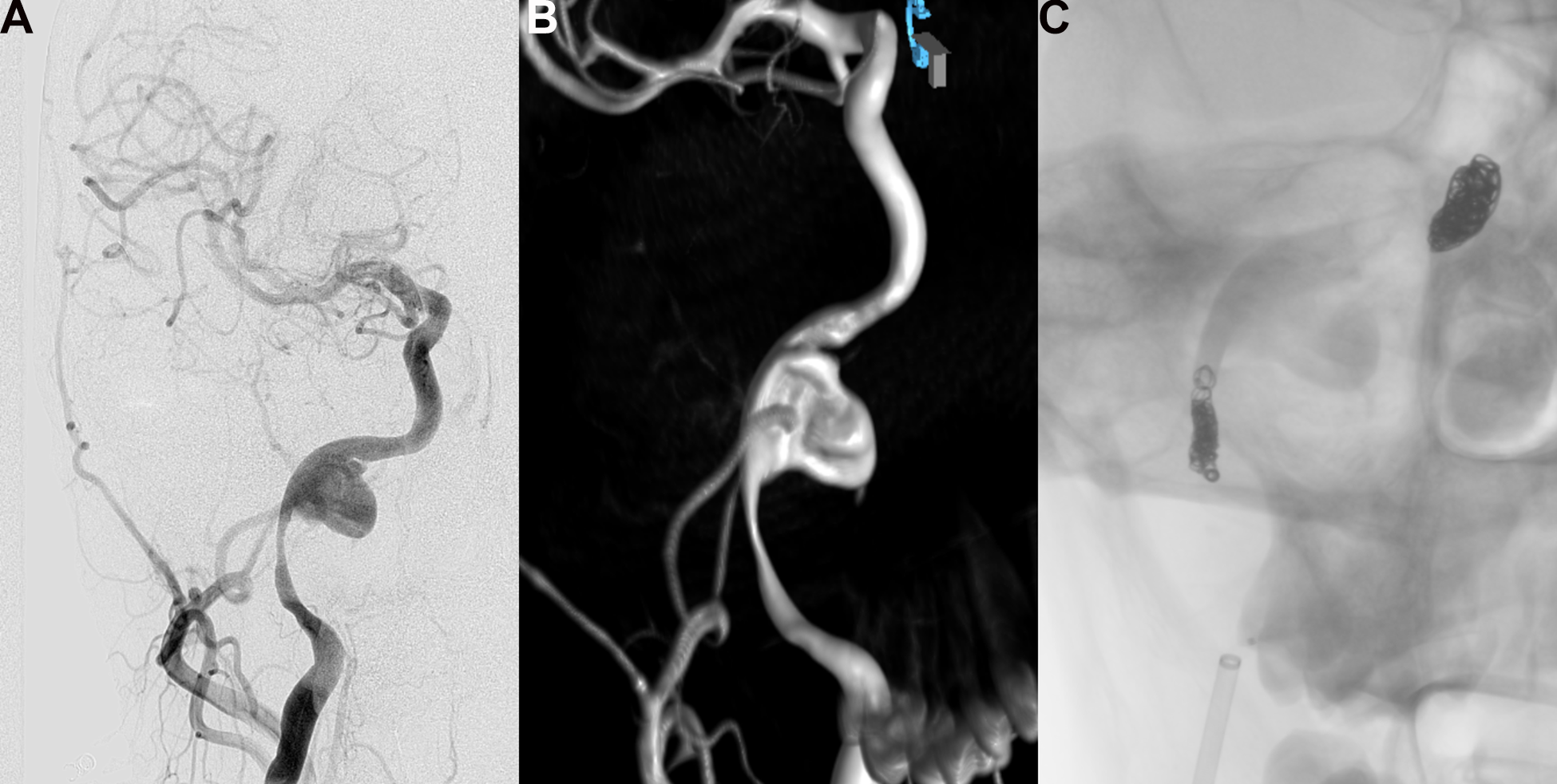
A, Digital subtraction angiography of pseudoaneurysm in cervical segment of right common carotid artery. B, Three-dimensional reconstruction. C, Proximal and distal occlusion with coils.
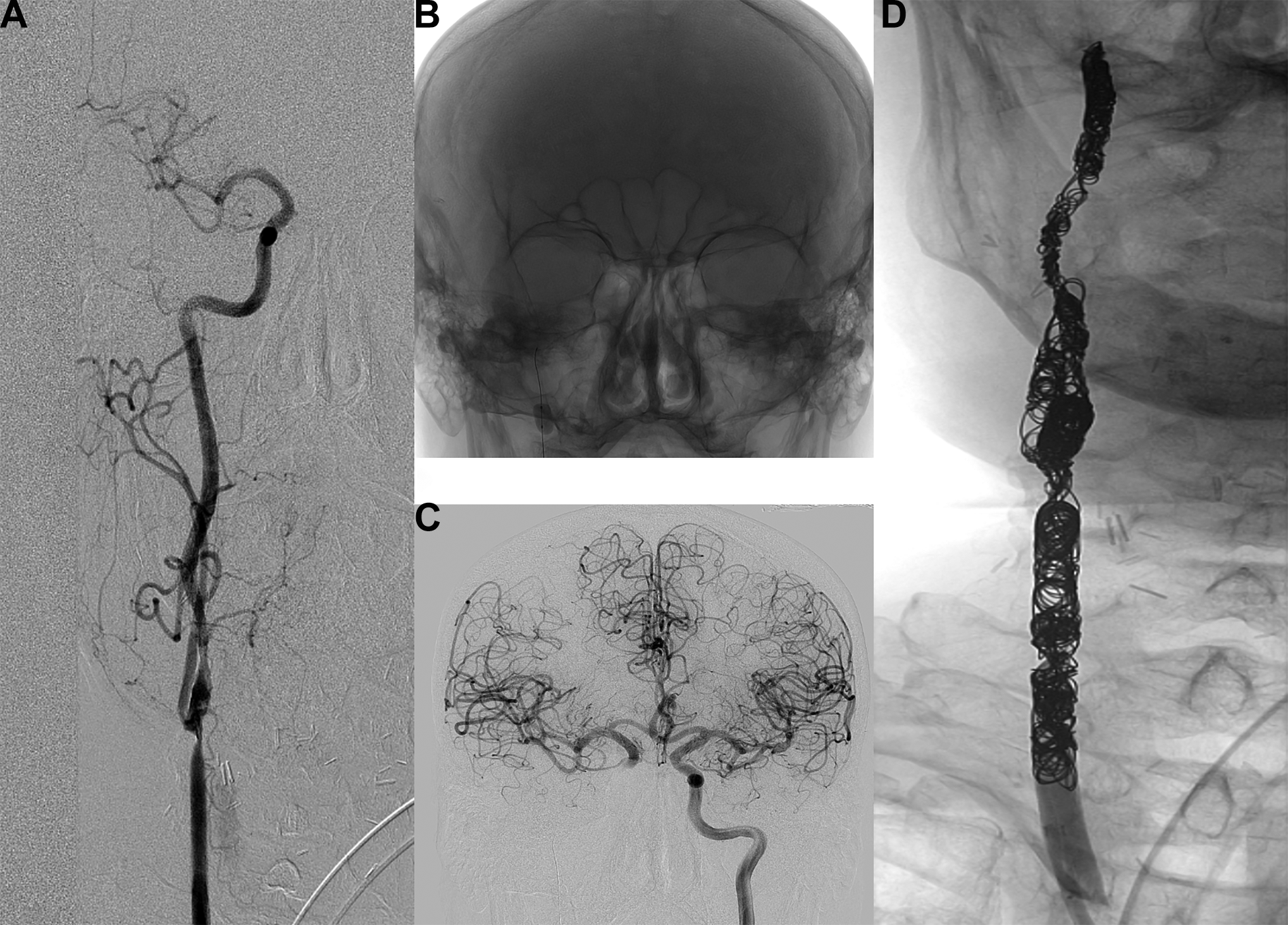
A, Focal endoluminal irregularity and stenosis of right common carotid artery. B, Remodeling balloon in distal segment. C, Tolerated balloon occlusion test. D, Definitive occlusion with coils.
Balloon occlusion test (BOT) indicated no risk of ischemia in any patient. This occlusion test was certificated by clinical examination and angiographic analysis of the collaterals. The occlusion test protocol used is the one described by Abud et al in 2005, 8 performed with a high compliance balloon over the injured carotid area. In case the patient is awake, we combine it with 10 minutes of arterial occlusion associated with a neurological examination. Those patients who could not tolerate this would have been considered for carotid stenting. Embolization and occlusion with Micrusphere cerecyte coils® with a platinum spherical 3-dimensional spherical structure (Cardiva, Sunnyvale, U.S.A.) of the artery was used in all patients to manage CBS. Technical success and immediate hemostasis were achieved in all patients without acute complications. One patient developed transient hypoglossal nerve palsy in the periprocedural period.
The follow-up period ranged from 3 to 24 months (mean 13.2 months). During the follow-up no recurrent CBS was reported. One patient died 4 months after the procedure because of a progression of the cancer. The remaining patients were alive at the last follow-up.
Discussion
CBS is a rare event that commonly occurs in patients with previous aggressive surgical management or radiotherapy of head and neck cancer. This dreadful complication requires acute intervention owing to high mortality and morbidity rates. Stratification and management of CBS is complex and require a multidisciplinary team.2,9
We found that 4 of 5 patients had been irradiated (more than 65 Gy) before presenting CBS. In addition, 3 of 5 patients suffered an active infection at the time of CBS. Both factors, radiation and infection, add up to their effects on the vasa vasorum in the adventitious layer. 10 Nevertheless, advanced stage status has also been associated with the occurrence of this complication and thus, one of the patients in our series (patient 4) with a stage IVA hypopharyngeal cancer presented with a CBS prior to the treatment.
CBS often manifests as bleeding through the mouth or through the neck. Nevertheless, one case (patient 1) had no manifestation of acute hemorrhage. This case was detected incidentally on CT scan. It can be sometimes difficult to diagnose CBS because it may not cause any symptoms, or it may manifest itself as a harmless neck swelling. It is important to consider the possibility of dangerous vascular injury in patients treated for a head and neck cancer with rapidly growing masses.
The angiographic findings in patients with CBS are heterogeneous. The most common finding described in the literature is extravasation at the CCA bulb in up to 40% of cases. 3 However, in our group, pseudoaneurysms are more frequent (3 out of 5 cases).
Endovascular occlusion and endovascular repair with covered stents are currently the 2 mainstays of treatment in CBS.2,11 However, the indication of one or other technique must be personalized and tailored in each case. Occlusion can always be performed on the external carotid artery (ECA) trunk. CCA and ICA can also be occluded if BOT indicates no risk of ischemia. 2 In our study, coil embolization was chosen in all cases, including those that involved CCA and ICA due to a BOT with adequate tolerance. Carotid occlusion was chosen over other treatments such as covered stents, due to the lower complexity of the technique and to avoid the risks of stent infection and hemorrhagic recurrence. Despite new advances with covered stents in a patient with acute bleeding, carotid occlusion makes possible to avoid antiplatelet drugs. On the other hand, covered stents with a diameter suitable for the common carotid artery or the internal carotid artery require high-profile inserters, 8F or greater and less than 90 centimeters in length, which, although their use is possible, are technically longer and more complicated to use than carotid occlusion. Endovascular repair with covered stents would be preferable for patients at risk of permanent carotid occlusion indicated by intolerance to a BOT, such as in cases of incomplete circle of Willis, contralateral carotid severe stenosis or total occlusion, or in cases of emergency status of the patient precluding an occlusion test. 2
Vascular plugs (like Amplatzer Vascular Plug) can be used for fast occlusion of extracranial carotids, especially in hemodynamically unstable patients. 12 These devices are more effective and faster than coils in these cases, but they are not of routine use at our center. In our patients the entire artery was occluded instead of using proximal plugs to avoid reentry by collaterals, ensure distal and proximal obstruction, and vascular re-permeabilizing that could cause new bleeding.
One of the most commonly complications of endovascular occlusion is the delayed cerebral ischemia. In our study none of the patients developed this complication; 4 patients had tolerance to BOT and a complete circle of Willis, and in the remaining patient BOT was not performed because of the lingual artery was the affected segment. The incidence of delayed ischemic events in patients who passed the BOT has been reported to be as high as 20%.13,14 However, this incidence of delayed ischemia occurs under ideal conditions of elective carotid sacrifice, not the unstable conditions of a grade 3 CBS patient.
In our study, 1 patient (patient 1) developed transient hypoglossal nerve palsy in the periprocedural period. This can be explained by mechanical damage to the nerve at the junction level over the ICA at the cervical level. No other complications were reported during the follow-up.
Although infection is a frequent risk factor for CBS, infectious complications directly related to endovascular coil embolization are not really common. However, it is likely to increase in the setting of increased used of neuroendovascular techniques in the future. In a review published in 2007 7 case reports of patients who experienced infection related to coils used for embolization of arteries were discovered and abscess formation in the area of coil placement was the most common infectious complication directly related to endovascular coil embolization. 15 Our patients with skull base osteomyelitis received a 3-month course of culture-directed antimicrobial therapy and the patient with infected pharyngo-cutaneous fistula was treated with piperacillin-tazobactam for 10 days, and none of them experienced subsequent infection in the area of coil placement.
In cases of extensive tissue necrosis and carotid artery exposure (either to the skin or the aerodigestive tract), coverage of the exposed area with well vascularized myocutaneous or free flaps to prevent recurrent bleeding is indicated (except in the palliative setting). None of our patients presented with this situation and required these additional procedures; in the patient with pharyngo-cutaneous fistula the previous free flap allowed for closure of the fistula and the carotid was no longer exposed to saliva.
The literature has reported that the average time from CBS to death varies from 4 to 12 months and endovascular treatment is able to offer 10 extra months of survival.5,16 Patients treated with coil embolization survive longer than patients treated with stent grafts. This is partly caused by the higher effectiveness of the occlusion and partly by the less severity of the hemorrhages of the ECA compared to ICA/CCA. 14 In our study, although most of the patients suffering from the acute CBS of the CCA/ICA, they were treated with occlusion, the average follow-up time of our patients was 10.6 months (maximum of 16 months in 2 patients). Only 1 patient died due to the tumor, and no recurrent CBS was reported.
Conclusion
In our experience, coil embolization, if possible, is a safe and efficient technique in treatment of CBS secondary to head and neck cancers. Stratification and management require a multidisciplinary team.
Footnotes
Authors’ Note
Informed consent has been obtained from the patients (or patient’s family/guardian) for publication of the case report and accompanying images.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.