
Abstract
Introduction
Renal arteriovenous fistula (RAVF) is a rare malformation of the kidney. Approximately 70% of cases are acquired or iatrogenic, whereas 20% are congenital, and 3–5% are idiopathic. 1 The majority of cases are iatrogenic and occur as a complication of renal biopsy, nephrostomy, blunt or penetrating trauma, inflammation, malignancy, and renal surgery. 2
Renal vein aneurysms (RVAs) are extremely rare vascular lesions. Most RVAs are idiopathic and associated with medial layer pathology but may also develop secondary to thrombosis, venous hypertension, and RAVF. 3 RVAs are usually asymptomatic and detected incidentally or may present with abdominal pain and hematuria. 4 There is limited information in the literature about RVAs. Here, we present a case of successful endovascular treatment of an RVA secondary to RAVF, which was thought to have been developed as a result of penetrating knife injury 11 years ago. Informed consent was obtained from the patient for the publication of this case and relevant pictures.
Case Report
A 40-year-old man presented with a severe headache lasting for 1 day to the emergency department. He had no additional history except for penetrating stabbing from the left flank 11 years ago. At that time, no treatment was planned for the patient due to stabbing. On physical examination, there were no additional features except minimal tenderness in the left upper quadrant. His blood pressure was 190/120 mm/Hg. Blood count and renal function tests were within normal limits. The urinary system ultrasound examination revealed a large anechoic lesion in the left renal sinus that indicating aneurysmal dilatation of the left renal vein. The computed tomography (CT) angiography demonstrated an 18 cm diameter venous aneurysm due to an arteriovenous fistula filled with contrast that filling the retroperitoneal area along the middle and lower pole anterior section of the kidney, a 7.5 cm aneurysmal enlargement at the level of the middle and upper pole segmental branch, and expansion of the left renal artery up to 2.5 cm from the proximal level due to the increased flow caused by aneurysm and fistula (Figure 1). Considering the size of the RVA, accompanying RAVF, and the age of the patient, a nephron sparing approach was planned, and therefore, an endovascular intervention was planned for the management of the patient. Axial computed tomography (CT) image (A) shows an 18 cm left renal vein aneurysm. Axial CT image (B) shows an arteriovenous fistula (white arrow) between the renal artery segmental branch and the left renal vein. A 3D multi-slice CT-scan reconstruction (C) shows an excellent demonstration of left renal vein aneurysm.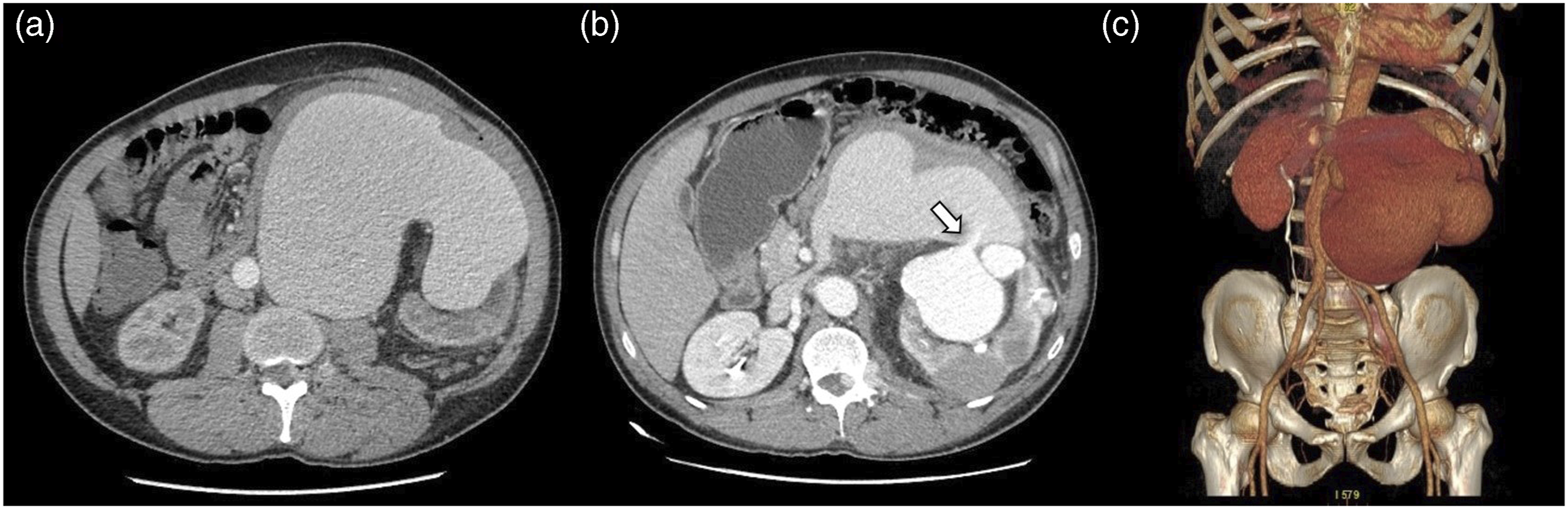
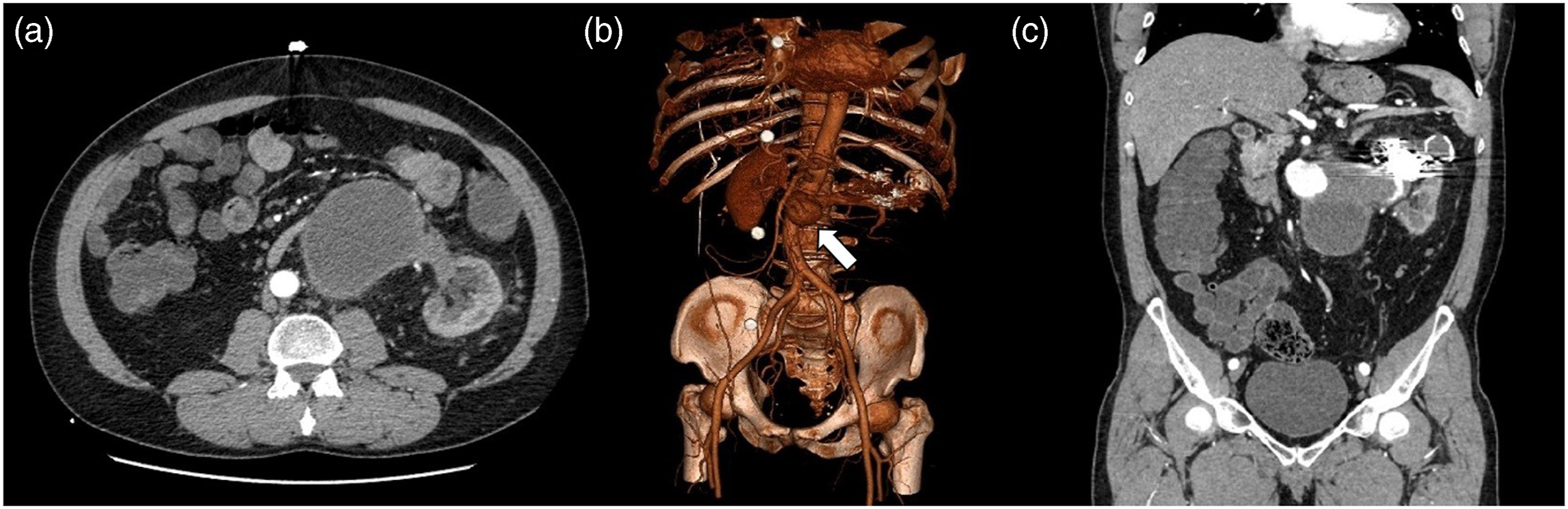
Bilateral femoral access was performed since the patient’s renal artery diameter is large (>30 mm) and 2 vascular plugs must be placed at the same time for proper occlusion. After bilateral femoral artery was punctured using a modified Seldinger technique under general anesthesia, a 7-Fr long sheath (Destination Guiding Sheath, Terumo Corporation, Tokyo, Japan) was placed into the femoral artery and selective catheterization of the renal artery was performed with a 5-Fr C2 (ImagerTM II, Boston Scientific, Massachusetts, USA) catheter. Selective renal angiograms were performed to demonstrate the vascular lesions (Figure 2). Aneurysmal dilatation up to 7 cm in the left renal artery, a high-flow RAVF in the upper pole branch of the left renal artery, and venous aneurysm in the renal vein with a craniocaudal length of 18 cm were observed in the angiography. Due to the large diameter of the left renal artery, the vascular plugs with a diameter of 20 and 18 mm (Amplatzer Vascular Plug (AVP) II, AGA Medical Corp., Golden Valley, Minnesota, USA) were opened side by side and a temporary barrier was created within the renal artery (Figure 2). At this stage, the space between plugs was filled with .018’’ and .035’’ detachable coils (Interlock Fibered IDC Occlusion System, Boston Scientific, Massachusetts, USA) to prevent the risk of migration. In addition, during angiography a second high-flow fistula was seen in another segmental artery, this area was catheterized via a microcatheter and embolized with a 6 mm vascular plug (AVP IV, AGA Medical Corp., Golden Valley, Minnesota, USA). In control angiography, it was seen that total occlusion of the high-flow RAVF in the renal artery was achieved. There were no complications during the procedure. After the procedure, anticoagulation at therapeutic dosing (enoxaparin) was prescribed in addition to prophylactic acetylsalicylic acid 80 mg daily. The patient had a fever for 2 days after the procedure and was treated with intravenous antibiotics. No other complications were observed in the follow-up except fever. The patient was discharged with oral antibiotics on the 10th day after the procedure. During the follow-up period, the CT angiography examinations of the patient demonstrated RAVF was closed and the RVA size reduced (Figure 3) and the patient’s arterial blood pressure came up to normal levels. Pre-embolized angiogram image of AVF. (A) Angiogram image of temporary amplatzer vascular plug (AVP) deployment (B) Angiogram image (C) shows the placement of the AVP II and multiple coils. Angiogram image (D) shows successful occlusion of the renal arteriovenous fistula. CT scan after twenty-one months. Axial CT image (A) and 3D multi-slice CT-scan reconstruction (B) show that size of the renal vein aneurysm has decreased. Coronal CT image (C) shows occluded arteriovenous fistula. CT, computed tomography.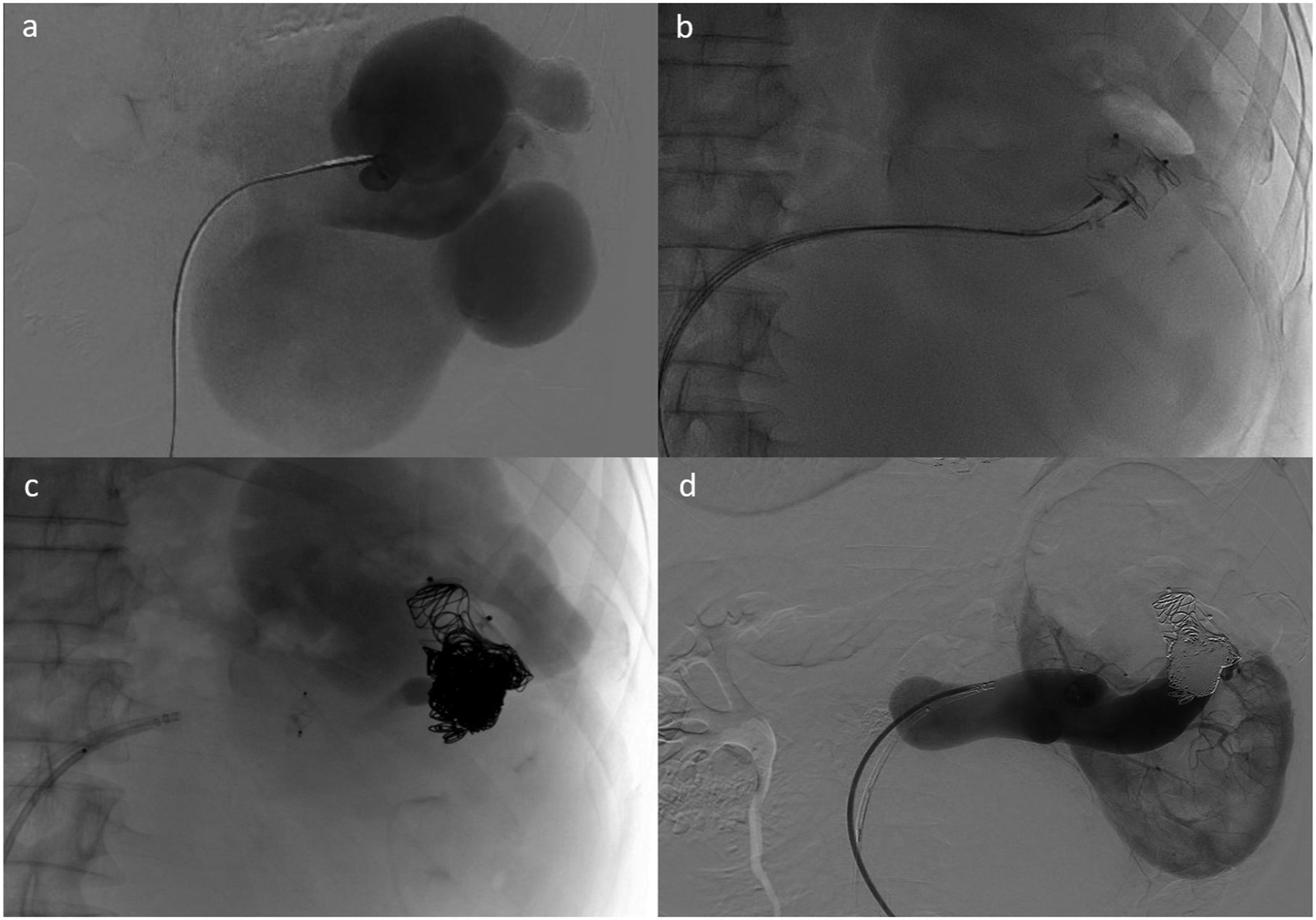
Discussion
Visceral venous aneurysms are uncommon conditions. RVAs are very rare and constitute < 3% of visceral vein aneurysms. 4 True RVA is characterized by a thin vessel wall due to medial atrophy with loss of elastic fiber, 5 and they can also occur secondary to RAVF, thrombosis, and venous hypertension. 3
Renal arteriovenous fistula is a related entity in which injury occurred in a renal artery branch and proximate vein, resulting in blood passing from a higher pressure system directly into contiguous veins. RVAs secondary to RAVF are rare. RAVFs usually resolve spontaneously. RAVFs become symptomatic as a result of complications due to high blood flow and cardiac failure, venous hypertension. 6 RVAs may be symptomatic due to rupture, thrombosis, or embolism and life-threatening situations usually emerge in these cases.
Although angiography is the gold standard in the diagnosis of RAVF, currently computerized tomography and magnetic resonance angiography are the most common diagnostic method and their 3D reconstructions are also used for planning surgical or endovascular intervention in many cases. Angiography still maintains its important place in diagnosis and treatment as it offers definitive treatment options.
Indications for treatment of RAVF are the progressive increase in the size of the fistula or concomitant aneurysm, hematuria, hypertension, and high-output heart failure. 1 Symptomatic RAVFs can be treated by an endovascular or surgical approach. In our case, there was a risk of rupture of the giant RVA and the patient had persistent hypertension. Following a risk-benefit assessment of different treatment options, an endovascular approach to occlude the RAVF was considered as the best option, with a lower risk of bleeding and morbidity compared with the surgical options.
Recently, endovascular techniques are used even for RVA with RAVFs. 7 The use of vascular plugs in high-flow RAVF was first described in 2007 by Idowu et al. 8 AVP is frequently used as an embolic tool in the treatment of RAVF and it can be used with or without coil, and effective in high-flow RAVFs in which the renal artery is ectatic or aneurysmal since it is possible to reposition it prior to final placement. 9 High-flow RAVF is still considered difficult to manage by endovascular embolization because the embolic agent may pass into the draining vein and this may lead to life-threatening complications such as pulmonary embolism. Also, the embolizing agent may migrate to the vessels feeding the renal parenchyma or the systemic circulation. In our case, migration of plugs was prevented by filling the space between vascular plugs with coils, and no complication was observed after the procedure.
In conclusion, a giant RVA secondary to RAVF is an unusual entity and enigma. We present a case of symptomatic giant RVA with a high risk of rupture secondary to iatrogenic RAVF presenting with hypertension and to our knowledge this is the largest RVA in the current literature. AVP combined with coils can be used safely and effectively to preserve kidney function in patients with large RAVF.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.