
Abstract
Introduction
Carotid endarterectomy (CEA) is the treatment of choice for revascularization of appropriate symptomatic and asymptomatic carotid stenosis. While newer treatment modalities such as transcarotid artery revascularization (TCAR) (Silk Road Medical, Sunnyvale, CA) have emerged as a promising alternative, CEA remains the gold standard for stroke prevention in the setting of critical carotid stenosis. However, the absolute risk reduction for neurologic events is modest, particularly for asymptomatic patients, so surgeons must be mindful of implementing strategies to minimize perioperative complications.
The technique of CEA and use of intraoperative completion studies at the time of surgery has been proposed to identify early technical factors that may be immediately corrected and thereby prevent neurologic events by our group and others.1-6 The choice of study (Doppler, duplex ultrasound (DU), and completion arteriography (CA)) remains controversial and individual practice patterns vary.7-10 Herein, we review the potential impact of routine CA following CEA.
Methods
A retrospective review of our prospectively maintained database was performed in a de-identified manner. All patients undergoing isolated CEA between 1992 and 2019 were included in the analysis. CA was routinely performed during this time. Informed consent and formal institutional review board review was waived in accordance with the University’s policy given the de-identified nature of this study.
Patient Variables
De-identified data were collected on patient demographics, relevant co-morbidities, operative details, and perioperative variables.
Procedural Details
All CEAs were performed by an attending vascular surgeon assisted by a vascular surgery fellow at Pennsylvania Hospital. CEA was performed with cervical block, local anesthesia, and intravenous sedation. Neurologic checks were performed throughout the procedure. During the study period, all patients who underwent CEA also underwent CA of the repair site and intra-cranial vasculature. Indications for intervention were >70% asymptomatic internal carotid artery (ICA) stenosis and >50% symptomatic ICA stenosis. Pre-operative antiplatelet regimen included at least aspirin, but additional agents were added at the discretion of the operator. Patients were systemically heparinized during the procedure with a weight-based dose (80 units/kilogram). Patients are fully reversed with protamine sulfate at the discretion of the operator. Patch angioplasty or eversion endarterectomy was performed at the discretion of the attending surgeon. CA was performed by inserting a 21-gauge butterfly needle in the common carotid artery 1–2 cm proximal to the repair and hand-injecting contrast in 2 views. Injections were performed with half strength contrast using a power injector. The butterfly needle tubing is back bled and the injector tubing de-aired before injection.
Statistical Analysis
De-identified data points were analyzed in Excel (Microsoft Corporation, Redmond, WA). Chi square tests were performed to determine the statistical significance of categorical variables, while continuous variables were compared using Student’s t-test.
Results
Baseline Patient Characteristics and Intra-operative Details.
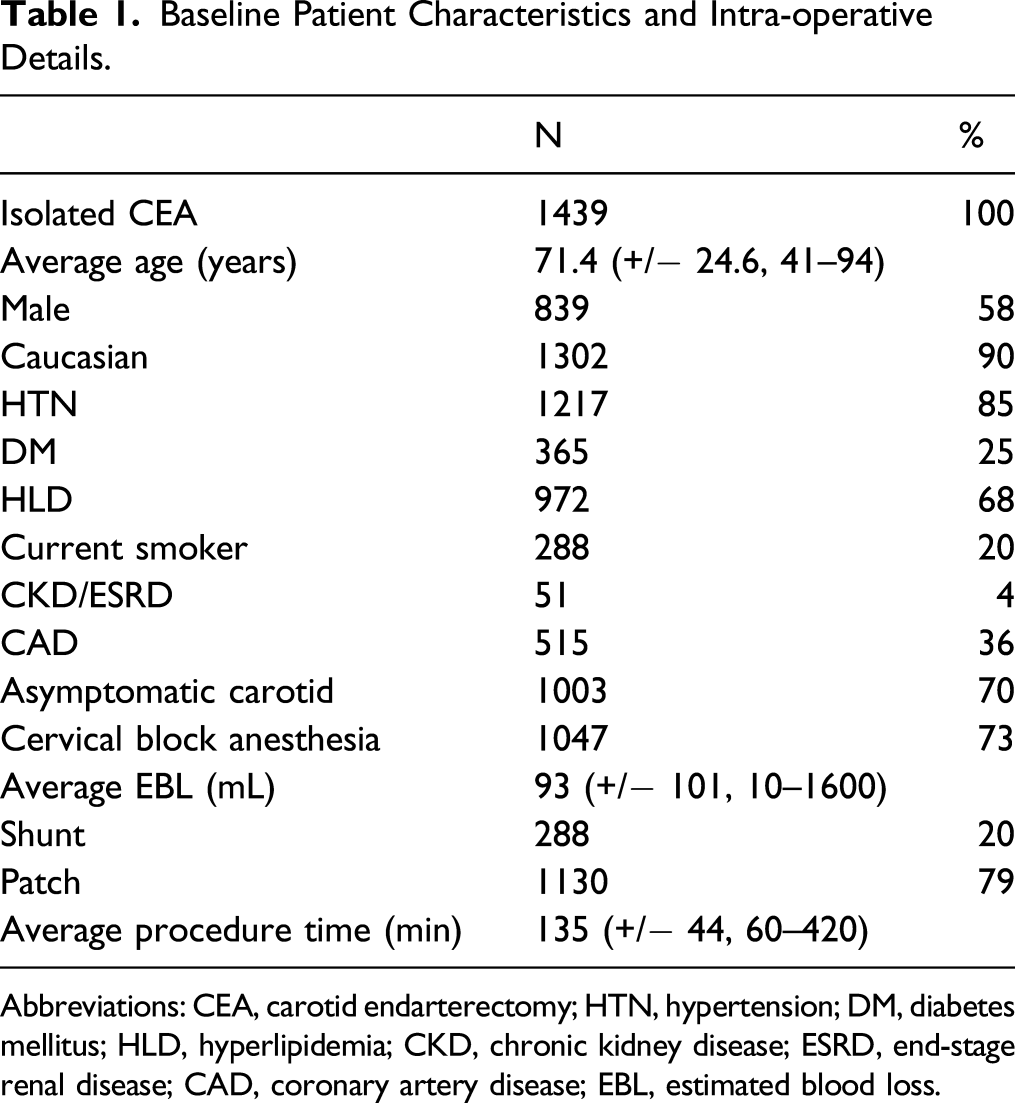
Abbreviations: CEA, carotid endarterectomy; HTN, hypertension; DM, diabetes mellitus; HLD, hyperlipidemia; CKD, chronic kidney disease; ESRD, end-stage renal disease; CAD, coronary artery disease; EBL, estimated blood loss.
Abnormal Completion Angiogram Findings.
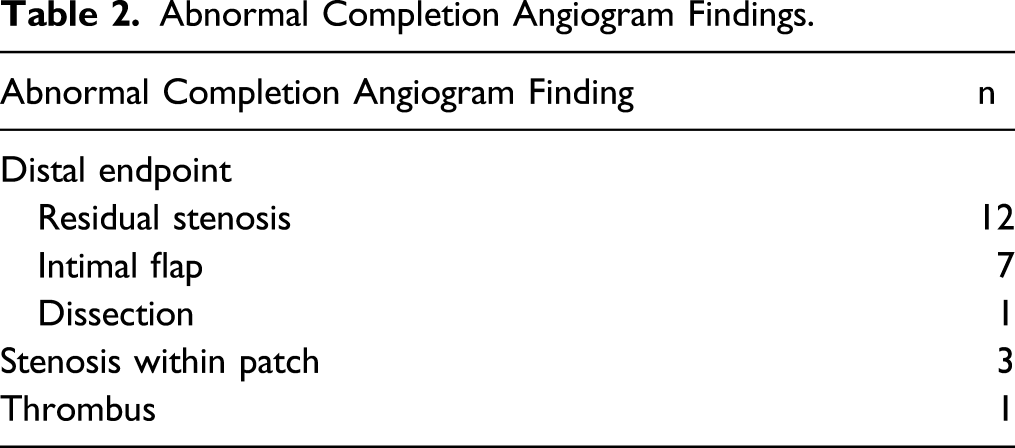
Seventeen of the 20 distal endpoint lesions were treated with stent placement. 11 Patch revision was performed for the remaining 3 distal lesions and for the 3 lesions within the body of the graft. The thrombus was treated with open thrombectomy, but no underlying lesion was identified. There were no perioperative strokes in the 24 (1.7%) patients with an abnormal CA that underwent immediate intraoperative revision.
Perioperative Strokes.
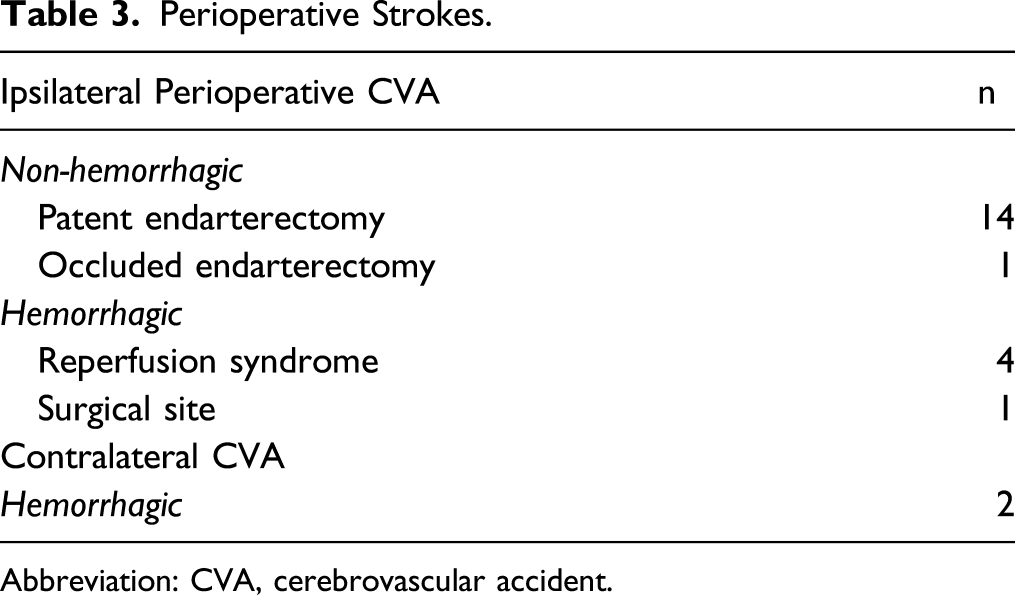
Abbreviation: CVA, cerebrovascular accident.
Discussion
The choice of completion intraoperative imaging modality following CEA remains largely discretionary and its impact is poorly defined. While the use of Doppler and DU have frequently been described,7-10 our practice has included routine use of CA following CEA. Our overall perioperative stroke, death, and combined stroke–death rate in this cohort was comparable or even favorable compared to NSQIP results, and CA in this series may have played a role in reducing our perioperative stroke rate even further.12–18 Of note, we do not revise defects identified in the external carotid artery.
While the use of CA as the completion imaging modality of choice has previously been studied, the results have been inconsistent. In our study, we found there were no perioperative strokes in the 24 (1.7%) patients with an abnormal CA that underwent immediate intraoperative revision, and thereby, we potentially avoided strokes in these 1.7% of patients. We demonstrated that CA can be performed safely and potentially halved the perioperative stroke rate from 3.2% (1.5% actual + 1.7% potential strokes prevented by repairing defects found on CA) to 1.5% (actual). Roon and colleagues in 1992 reported similar findings and demonstrated a statistically significant reduction in perioperative stroke rate with the adoption of routine CA (4.5% pre-CA vs 1.3% with CA). 19 Other early reports of CA echoed these results and further suggested a decreased re-intervention rate in those patients who underwent CA.20,21
Despite these data, the utility of CA has been questioned.14,22,23 Some surgeons have opined that careful visual inspection of the artery after endarterectomy and closure is adequate to ensure a satisfactory result. Another argument has been made that re-exploring the endarterectomy site has the potential to increase the stroke risk by re-clamping and extending ischemic times. One of the largest series to assess completion imaging modalities was the EVEREST (Eversion Versus Standard Carotid Endarterectomy) study group where 1004 patients (77%) underwent CA. Although 28 patients (4%) underwent revision based on CA findings, the authors suggested that revision was not protective of unfavorable outcomes. 22 A more recent study by Malas et al has demonstrated that completion imaging yields higher rates of early re-exploration and revision. 24 However, routine completion imaging was not associated with significant decrease in adverse event rates compared with selective completion imaging.
While during the first portion of this study we performed CEA and routine CA using a portable C-arm, we and many other vascular surgeons currently perform vascular procedures in a hybrid fixed-imaging endovascular operating room. Avoiding the need to summon a radiology technician to manipulate a C-arm, and instead being able to move the ceiling-mounted C-arm over the operative site as soon as the operation is completed, saves time and provides superior imaging. In our hands, performing CA usually adds 5 minutes to the operation. Our findings are consistent with those of Malas et al with no significant complications from performing CA. 24
With the advent of TCAR, vascular surgeons have witnessed an increase number of carotid stents being placed. CA is an essential component of both TCAR and transfemoral carotid artery stenting (TF-CAS) to ensure excellent technical results. This begs the question as to why CA should not be used for CEA? Some might argue that CA after stenting is necessary because technical abnormalities will be found more commonly after stenting than after surgery. However, the higher stroke rate associated with stenting compared to surgery is related to passage of catheters and wires across the diseased aortic arch and ICA and not necessarily due to technical problems identified on completion CA.
There are limitations to our study. First, intraoperative findings of CA are somewhat subjective and surgeons may differ as to whether revision may be necessary. We recognize that minor defects should be left alone. However, all 24 defects noted in this series appeared significant, and we would argue that all needed repair. Second, we cannot be certain that all patients who underwent intraoperative revision based on CA would have suffered a neurologic event if we had not revised the endarterectomy site. We feel that even a 1–2% yield in identifying technical deficiencies might substantially impact the efficacy of CEA for stroke prevention. Finally, our series used CA alone as a completion imaging modality, and we therefore cannot make a direct comparison to other completion imagining modalities.
Conclusion
Our experience demonstrated that routine use of CA following CEA can be performed safely and quickly. This completion imaging modality may have approximately halved our perioperative stroke rate.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical board/IRB approval deferred in accordance with our institution’s policy on de-identified registry studies.