
Abstract
Introduction
Carotid endarterectomy (CEA) is a well-standardized intervention for stroke prevention in patients with significant carotid artery stenosis, with an evident improvement of the surgical outcome in the last decades. The rate of postoperative strokes, either ischemic or hemorrhagic, dropped from 7.8% in the early experience to less than 1% in the latest series.1,2 Reasons for such a reduction can be attributed to progresses in anesthesiological technique, cerebral monitoring, surgical experience, technical refinement, 2 and better medical management.
Despite this reported improvement in CEA outcomes, a detailed analysis of the possible causes of intra- and perioperative stroke if often lacking, probably because of the low number of such events.
Possible causes of perioperative stroke include embolization during dissection, residual intimal flaps, acute thrombosis, hyperfusion syndrome, and intracranial hemorrhage. 3 The type of surgical technique—patch endarterectomy or eversion—as well as the use of shunt have not been identified as risk factors for stroke.4,5 Current guidelines suggest that the surgeon adopt the individualized preferred technique for CEAs, in order to achieve the most favorable outcome. 6
While a number of studies describe surgical technique, only a minority evaluates the timing of carotid clamping during dissection. Some surgeons prefer to sharply dissect only a short portion of the common or internal carotid artery while appropriately heparinized, in order to clamp the artery before exposing the entire bifurcation; this allows to minimize the risk of distal embolization, at the price of an increase in clamping time.7,8 Other surgeons prefer to clamp common, external, and internal carotid arteries only after they completely expose all arteries and complete the entire dissection, in order to reduce the ischemic time.
The aim of the present study was to analyze the different causes of stroke after CEAs and to evaluate the outcome according to the surgical technique, specifically with regard to the sequence of carotid clamping/dissection maneuvers (clamped-dissection (CD) vs preclamping-dissection (PCD).
Methods
Patients
All CEAs performed from 2006 to 2019 in a single academic center were prospectively collected in a dedicated database, reporting the clinical characteristics, cardiovascular risk factors, and technical surgical aspects. The patients treated in the study had a symptomatic or an asymptomatic carotid artery stenosis >50% or >80%, respectively, in accordance with the current guidelines for CEAs. 6 CEAs performed for restenosis or postradiation stenosis or in association with coronary artery bypass grafting were not considered.
The study was performed following the rules of our Institutional Ethical Review Board (comitato etico area vasta Emilia centro-n. 3686), and all patients gave their informed consent. All patients were registered prospectively into a dedicated database for subsequent retrospective analysis. The database was de-identified according to the European General Data Protection Regulation (EU 2016/679). No preregistration exists for the studies reported in this article.
Definition of Post-CEA Stroke
Postoperative strokes were classified according to the time of identification: “intraoperative” if disclosed; immediately postoperatively, upon awaking from general anesthesia; or “postoperative” if onset within the first 30 days. Major strokes were defined in accordance with the modified Rankin scale (mRS)9,10 values ≥3; if the mRS was ≤2 the strokes were classified as minor.
Stroke Etiology Classification.
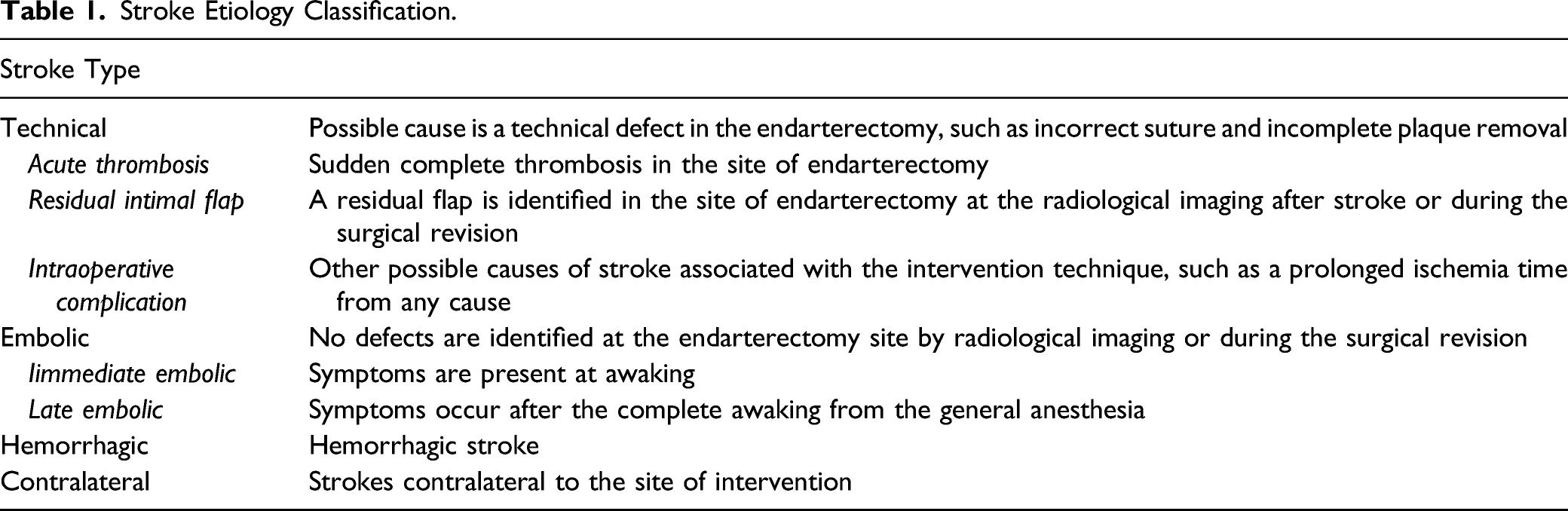
Technical:
the causes were likely associated with a technical defect of the endarterectomy or other intraoperative complications. Specifically, (i) acute thrombosis: stroke was associated with a sudden complete thrombosis localized to the endarterectomy site. (ii) Residual flap: a residual flap was identified at the site of endarterectomy by radiological assessment after stroke onset or during surgical revision. (iii) Intraoperative complications: other possible causes of stroke associated with the intervention.
Embolic:
no defects were identified at the site of endarterectomy by radiological imaging or during the surgical revision, and were further divided into (i) immediate embolic stroke: possible embolization during the dissection, and late embolic stroke: embolization from other possible sources occurring subsequent to the index procedure.
Hemorrhagic: h
emorrhagic stroke.
Contralateral:
strokes occurring contralateral to the site of intervention for any cause.
In case of a stroke identified immediately after CEA, the patient was re-anesthetized and the surgical wound was reexposed. A direct carotid digital subtraction angiography was performed to identify possible causes of stroke, and a surgical revision of the endarterectomy was performed if necessary. In case of a stroke occurring outside the operating room, a cerebral computed tomography angiography of the supra-aortic and intracerebral vessels was performed in order to establish the necessity of a surgical revision.
Surgical Technique
CEA was routinely performed under general anesthesia, with longitudinal arteriotomy, routine shunting and patching (Dacron), and cerebral near-infrared spectroscopy monitoring (NIRS). Eversion endarterectomy was also performed when anatomically indicated. Shunting (Bard, 8195 Industrial Blvd Covington, GA 30014 USA) was used routinely after plaque removal. 11 NIRS monitoring was employed in all cases despite routine shunting, in order to ascertain efficacy of brain perfusion. Intraoperative duplex ultrasonography was performed for quality control.
The surgical techniques for carotid dissection were classified as follows:
Clamped dissection (CD)
Only a short segment of the common or the distal internal carotid artery—according to the patient anatomy and the surgeon preference—was exposed and clamped, after systemic heparinization (aimed at achieving an activated clotting time >200 sec); the residual carotid bifurcation was then dissected out and a complete clamping of the common-internal-external carotid arteries was obtained in order to proceed with the endarterectomy.
Preclamping dissection (PCD)
Complete exposure of the carotid bifurcation was performed before carotid clamping.
The surgical technique was adopted at the discretion of the operating surgeon; 7 senior vascular surgeons are effective members of the vascular team.
Statistical Analysis
Continuous variables were described with mean and standard deviation (SD) for normal distribution and were compared by unpaired Student’s t test. The differences between percentages were assessed using Fisher’s test or the chi-square test, when appropriate. Multivariate analysis was performed to investigate the influence of different risk factors (significant at the univariate analysis) on post-CEA stroke by binary logistic regression. Risk factors were reported as odds ratio (OR) and 95% of confidence interval (CI). A value of P ≤ .05 (two-tailed) was considered to be significant. The statistical tests were performed using SPSS® 21.0 for Windows® (SPSS, Chicago, Il, USA).
Results
Stroke Rate and Etiology
Clinical and Technical Characteristics of the Population Examined.
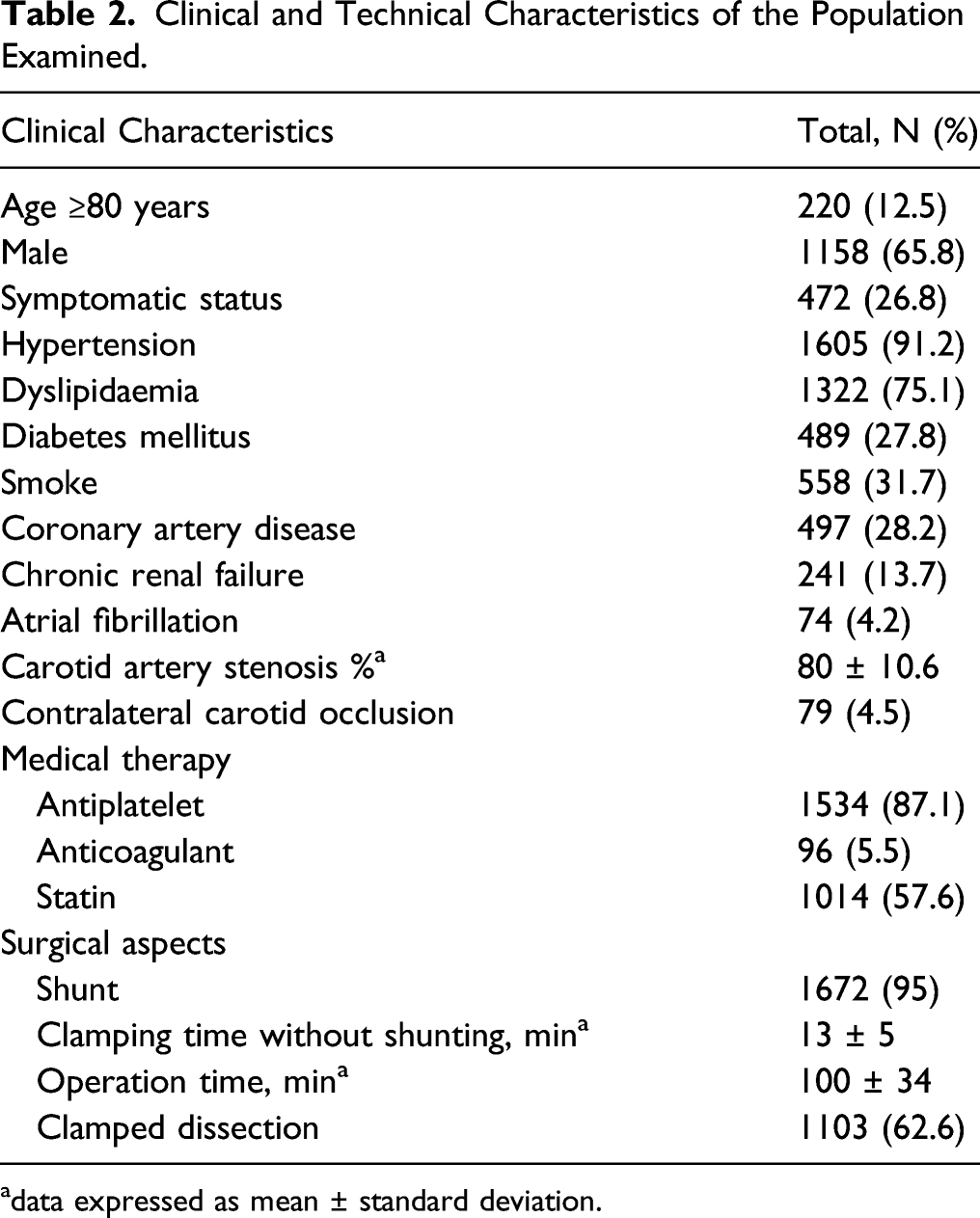
adata expressed as mean ± standard deviation.
Overall, 30 (1.7%) perioperative strokes occurred; 14 (47%) were identified immediately postoperatively, upon awakening from general anesthesia, and 16 (53%) in the period between the first and 30th days after surgery.
Etiology of Stroke in Accordance with the Symptomatic Status.

The composition of the surgical team was evaluated as a parameter associated with the incidence of strokes; the overall rate of postoperative strokes ranged from 0% to 3.1%, with no statistical differences in the interoperator analysis (P = .18).
Outcomes Based on the Dissection Approach Adopted
Distribution of Etiology of Strokes in Accordance with the Symptomatic Status and the Carotid Dissection Approach Adopted During Carotid Endarterectomy.
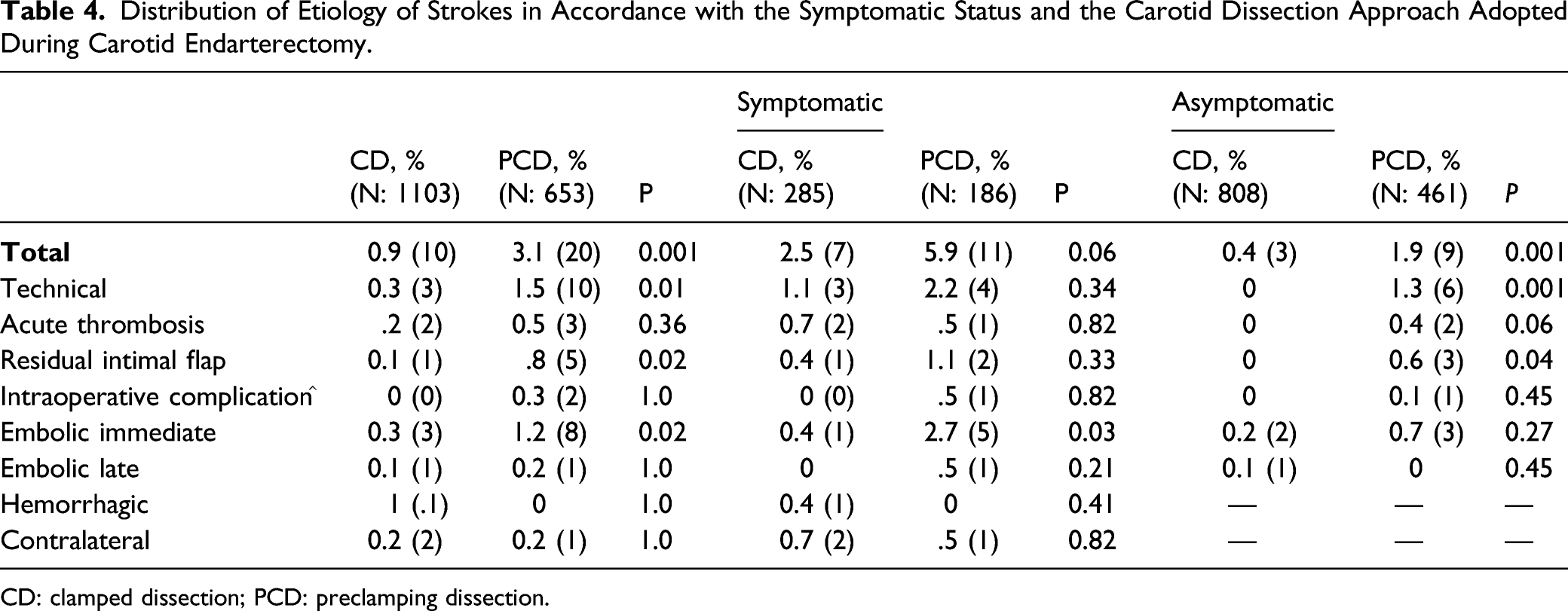
CD: clamped dissection; PCD: preclamping dissection.
Discussion
In the current series on 1760 CEAs, the postoperative stroke rate was 1.7% (n = 30), with a significant difference between symptomatic and asymptomatic patients (3.8% vs 0.9%).
When assessing postoperative strokes by etiology, technical defects were found to be the most frequent cause, followed by immediate embolic events. These types of postoperative strokes were more frequent in symptomatic patients than in asymptomatic ones. A possible explanation of the influence of the neurological status on the occurrence of technical defects can be due to a higher complexity of the plaque in symptomatic patients, with a greater distal extension or a more fragile structure leading to a challenging endarterectomy. Similarly, the higher rate of immediate embolic strokes in symptomatic patients can be explained by the higher risk of embolic potential associated with the carotid dissection prior to the endarterectomy.
The other 6/30 (20%) strokes were neither technical nor immediate embolic, and the exact mechanism is unclear. 3 strokes were contralateral, 1 was hemorrhagic and the other 2 were late embolic strokes that occurred in the second and fourth weeks after surgery. Therefore, other causes should be considered; embolic events from other sources can be associated with atrial fibrillation or from aortic plaques or intracerebral vascular thrombosis.
There is some evidence in the literature describing various etiologies for strokes following CEAs. De Borst et al. 3 analyzed 599 CEAs, reporting 1.5% carotid occlusion, .5% embolization, .5% unknown, .2% hemorrhage, and .6% other causes. In the evaluation of the types of stroke from the ICSS trial, Huibers at al. 13 considered 27 strokes after 819 (3.3%) CEAs for symptomatic carotid artery stenosis; mechanisms of stroke were carotid-embolic in 4 cases, another 4 were due to thrombosis or occlusion of the carotid artery, 5 cases were hemodynamically related, 6 cases were caused by hyperfusion, 3 were cardioembolic, and 5 cases remained undetermined. The authors defined the cause as hemodynamic when a severe perioperative hypotension episode occurred for a bradycardia/asystole. The data from ICSS confirm that a minority of post-CEA strokes occurred intraoperatively (10/27; 37%). Despite the rigorous and precise neurological evaluation in the ICSS trial, 5/27 (19%) strokes remained undetermined.
In our study, we evaluated the effect of the surgical technique in dissection and exposure of the carotid bifurcation on the incidence of stroke. Our analysis shows that the exposure performed after carotid clamping is associated with a significant reduction of postoperative stroke, irrespective of etiology. In particular, CD significantly reduced the rate of immediate embolic strokes in symptomatic patients. Other studies also demonstrate better outcomes with the CD technique. Pratesi et al. 7 and Bourke et al. 14 reported good results with early internal carotid clamping prior to dissection/exposure of the carotid bulb. Similarly, Yoshida et al. 8 demonstrated successful outcomes when clamping the common-external and internal carotid artery before the dissection of the carotid bifurcation.
Despite prolonged cerebral ischemia time associated with the CD technique, no hemodynamic strokes occurred. This may be explained by our use of intraoperative cerebral monitoring as well as routine use of a carotid shunt. The neuromonitoring with NIRS is not widely employed; however, its efficacy is comparable with that of EEG.15,16 An NIRS reduction greater than 15% from basal levels is considered significant15,16 and warrants more expeditious endarterectomy in an effort to minimize cerebral hypoperfusion time; otherwise, the CEA is performed, and the shunt is inserted only after complete plaque removal; this is not the standard approach, as many surgeons shunt the carotid prior of plaque removal, but shunting after plaque removal was demonstrated to be similarly effective, and it is our routinely approach. 12
The present retrospective analysis underlines that CD can reduce the incidence of early postoperative strokes, especially in symptomatic patients. In this context, it is interesting to note that with the CD technique, the incidence of perioperative stroke in asymptomatic patients is as low as 4%.
Nevertheless, there is still a percentage of strokes that are unrelated to the surgical technique. Contralateral strokes, and hemorrhagic and late embolic strokes were uncommon (.3%); however, they are difficult to be predicted.
Limitations to our study include those inherent to the retrospective analysis of prospectively collected data; lack of technique selection, which was by discretion of the surgeon; and the low rate of events (small sample size) precluding more robust statistical analysis. The high number of asymptomatic patients is likely due to the fact that our database was initiated in 2006, much earlier than the 2018 publication of the current European recommendations for CEAs for asymptomatic patients. In conclusion, strokes after CEAs are typically associated with technical defects in both symptomatic and asymptomatic patients. The CD technique may help reduce the rate of immediate embolic strokes, in particular in symptomatic patients. However, a small fraction of postoperative strokes are likely multifactorial and may be more difficult to be prevented.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.