
Abstract
Keywords
Manuscript
Case Report
A 65-year-old woman presented to the emergency department with a 2-day history of worsening epigastric pain, nausea, and episodes of pre-syncope without evidence of gastrointestinal bleeding. She was previously well, with a history of depression, anxiety, and an open cholecystectomy. Initial physical examination revealed that she was hemodynamically unstable with hypotension (90/60 mmHg) and tachycardia (110 bpm). Her abdomen was mildly distended with epigastric tenderness. Her blood tests showed a falling hemoglobin level over 4 hours (127 g/L to 82 g/L).
After resuscitation including intravenous fluid and blood transfusion and vasopressor infusion, the source of her hemorrhage was investigated with an urgent computed tomography angiogram (CTA). This showed hemoperitoneum and a large hematoma filling the lesser sac, with contrast extravasation from a 9-mm left gastric artery aneurysm. This prompted an attempt at endovascular embolization of the left gastric artery. Selective cannulation of the celiac artery via a right femoral approach was successful and the aneurysm was visualized (Figure 1A). However, vessel spasm prevented wire and catheter advancement. Ongoing hemodynamic instability despite fluid and blood product resuscitation precluded further embolization attempts; therefore, the procedure was abandoned and the decision was made to proceed to operative control of the hemorrhage. Selective catheter angiogram showing (A) the left gastric artery aneurysm (large arrow) and vasospasm of the coeliac trunk (small arrows). (B) Selective catheter angiogram of the celiac trunk showing successful left gastric artery aneurysm coil embolization and resolution of the coeliac trunk vasospasm, with persistent irregularities to the hepatic artery proper (small arrows).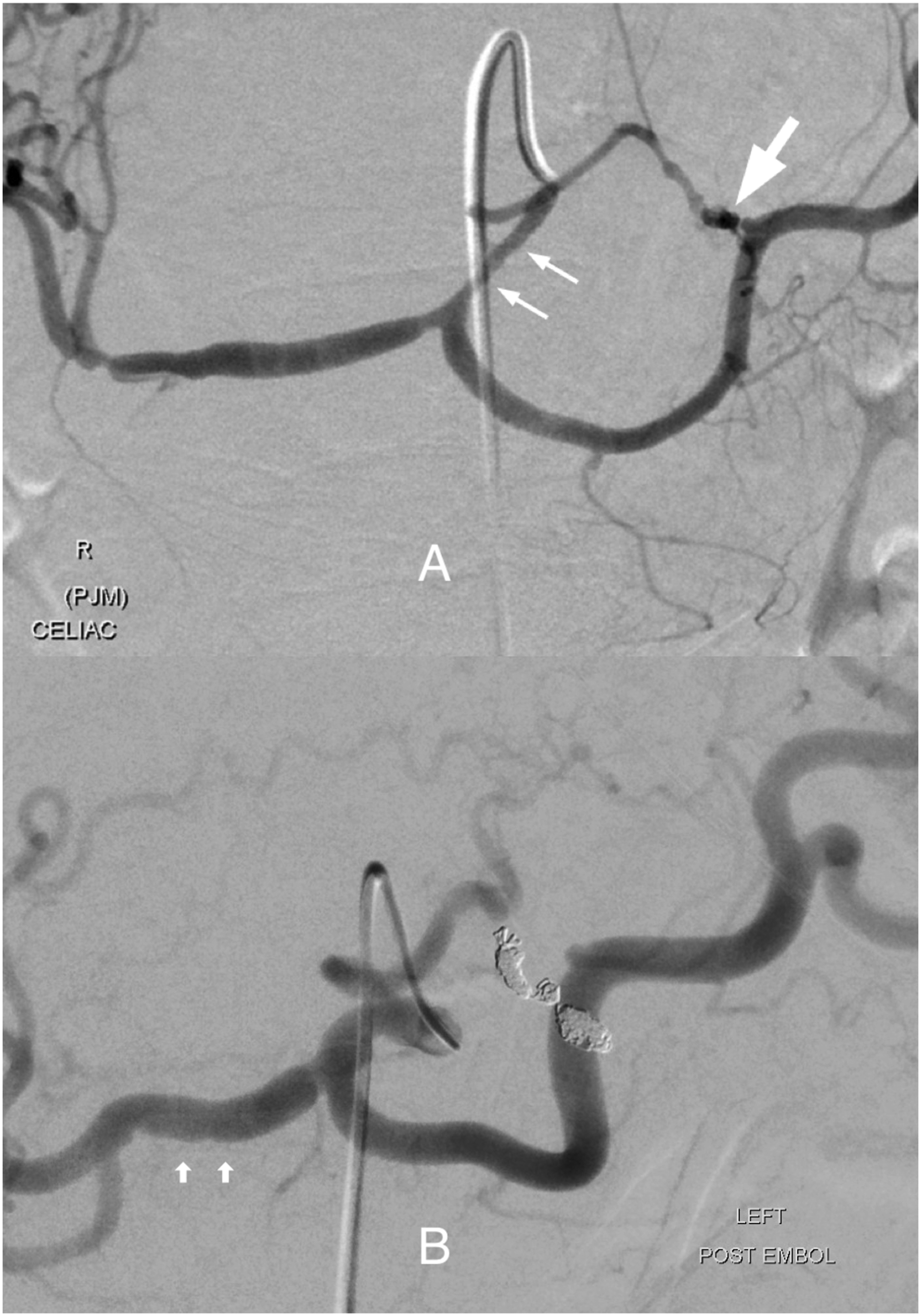
Intraoperatively, the bleeding point was identified in the vicinity of the left gastric artery pedicle which was controlled with polypropylene sutures. However, the extensive hematoma and hemodynamic instability precluded further detailed exploration needed to achieve ligation or excision of the aneurysm
The post-operative CTA demonstrated a persistent 5-mm aneurysm of the left gastric artery without contrast extravasation. Given the risk of further spontaneous rupture, endovascular embolization was re-attempted 2 days later. The aneurysm was successfully occluded with a series of Target® (Stryker, Fremont, CA) detachable platinum coils (Figure 1B). This delayed attempt at embolization benefitted from further resuscitation and resolution of the vasospasm seen in the initial angiogram.
A series of investigations were performed to identify the cause of this unusual aneurysm. “String of beads” changes involving the renal arteries, typical for fibromuscular dysplasia (FMD), were shown on the initial CTA and selective angiography (Figure 2). Further cerebrovascular imaging with CTA revealed similar changes of the right internal carotid and right vertebral arteries (Figure 3), without any intracranial aneurysms. The screening tests performed for vasculitides, including autoantibodies, complement levels, HIV, and hepatitis screen, were negative. Selective catheter angiogram of the (A) right and (B) left renal arteries showing the “string of beads” appearance of multifocal fibromuscular dysplasia of the mid-renal arteries. Computed tomography angiogram of the extracranial right internal carotid artery showing the “string of beads” appearance of multifocal fibromuscular dysplasia (arrows).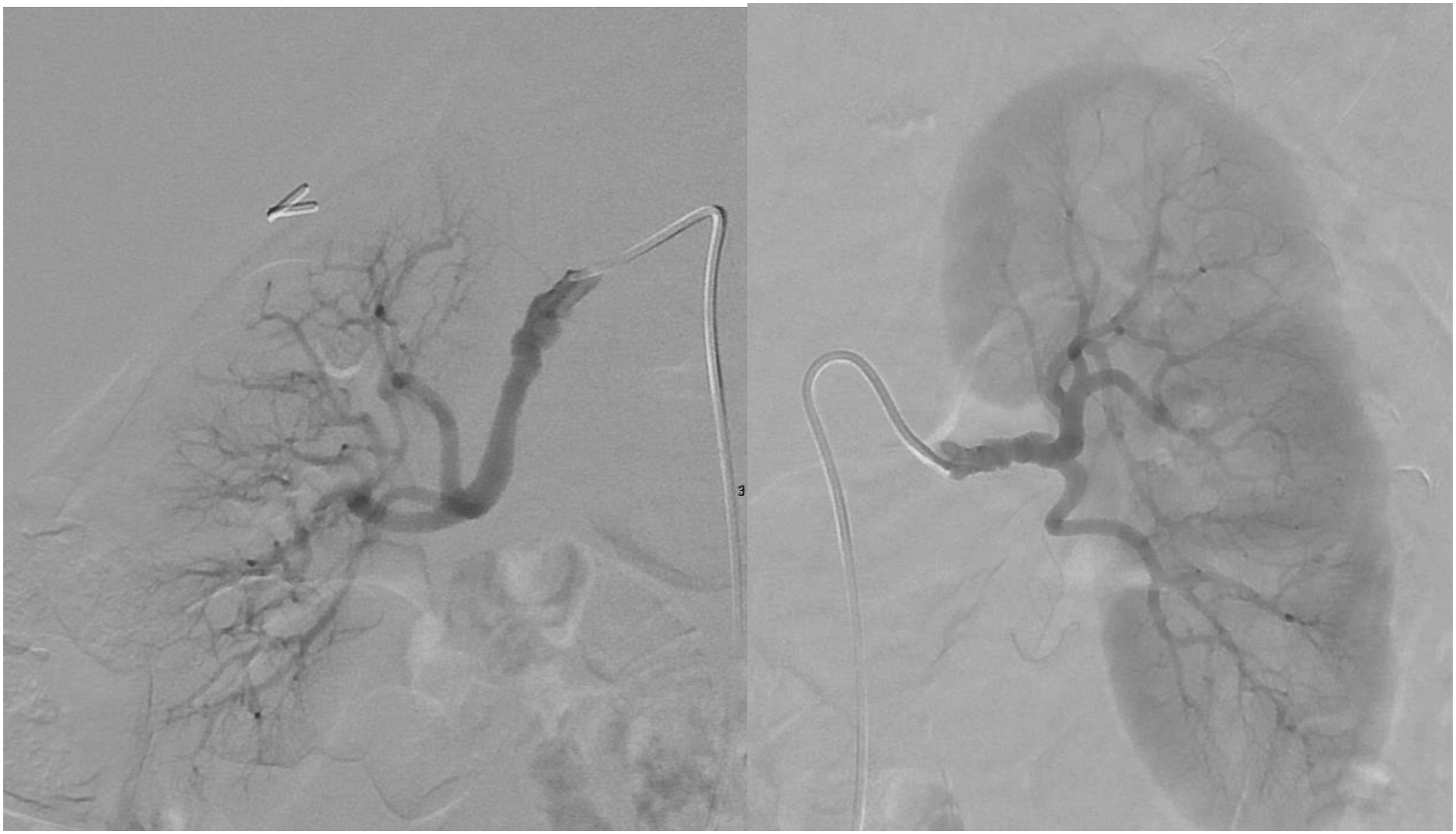

The post-operative recovery was uncomplicated, and she was discharged home after 9 days. At 6-month follow-up, she returned to work and her follow-up CTA confirmed occlusion of the left gastric artery aneurysm without any new aneurysm formation.
Discussion
Fibromuscular dysplasia is an idiopathic non-atherosclerotic vascular disease that affects medium-sized arteries. 1 It is an uncommon disease, and 90% of cases occur in female patients. 2 It can manifest as stenosis, dissection, or aneurysm formation. Traditionally, FMD is diagnosed histologically by identifying fibroplasia of the arterial wall. Likewise, the classification is based on the layer of the arterial wall affected by fibroplasia. Medial fibroplasia is the most common subtype of FMD, which is characterized by multifocal stenoses alternating with areas of dilation—producing the so-called “string of beads” appearance on angiography. 1 With the trend toward endovascular treatment, tissue sampling is increasingly uncommon in clinical practice. In a recent international consensus, angiographic finding of typical stenotic arterial lesions is thought to be sufficient to establish the diagnosis of FMD. 3
Fibromuscular dysplasia typically affects renal and carotid arteries but virtually any arterial territory can be involved in this condition. Within the United States and European registries, renal FMD accounts for 66–91% and cerebrovascular FMD accounts for 58–80% of cases. Multivessel involvement is found in 31–66% of cases. Visceral artery FMD occurs in approximately 18% of cases and generally occur in patients with multivessel FMD. 3 To our knowledge, this is the first report of gastric artery aneurysm in the setting of FMD.
There are several conditions that can mimic FMD and should be considered as differential diagnoses. Similar stenotic lesions can occur in segmental arterial mediolysis (SAM) and large-vessel vasculitides. Aneurysms and dissections can occur in similar distributions in some connective tissue diseases such as Loeys–Dietz syndrome and Ehlers–Danlos syndrome. 3 Specially, SAM has been increasingly recognized as a cause of visceral artery aneurysms, and it is particularly difficult to differentiate from FMD. 5 SAM is a rare non-atherosclerotic vascular disease characterized by vacuolar degeneration of the medial layer of the vessel wall.6,7 Over time, reparative fibrosis can result in lesions that may be histologically and radiologically indistinguishable from FMD.6,8 In addition, although SAM most commonly affects the celiac trunk and its branches with aneurysms or dissection, it can affect any arterial territory. Given these shared features between FMD and SAM, some authors proposed that SAM may be a precursor or variant of FMD.9,10 Nonetheless, some differentiating clinical features between the 2 conditions have been suggested.6,8 FMD tends to affect young to middle-aged females, with involvements of the renal and extracranial carotid artery occurring most frequently. SAM shows no gender predilection and typically affects visceral mesenteric arteries with dissection, aneurysms and spontaneous hemorrhage. In our presented case, given the patient’s female gender, classical “beads-on-string” appearance, and the involvement of the renal and intracranial distribution, FMD appears to be the most likely diagnosis. In our presented case, given the patient’s female gender, classical “string of beads” appearance, and the involvement of the renal and intracranial distribution, FMD appears to be the most likely diagnosis.
There is currently no cure for FMD. The management strategy is focused on ongoing surveillance and tailored treatment toward the affected arterial bed and its manifestations. 2 Our patient presented with a ruptured gastric aneurysm which mandated urgent operative management. Although there are no prior reports of FMD-related gastric artery aneurysms, gastric artery aneurysms in general are known to rupture even at small sizes. Unlike most of the other visceral artery aneurysms, there does not appear to be a safe threshold for conservative management of these aneurysms. Hence, the recent guidelines from the Society for Vascular Surgery recommend treatment of all gastric artery aneurysms regardless of size. 4 All unruptured FMD-related gastric artery aneurysm of any size should similarly warrant treatment.
The presented case demonstrated that FMD is an important differential diagnosis to consider in cases of visceral aneurysms and thorough investigation of other arterial beds can be revealing in these patients. Additionally, this case also shows the impact of visceral artery vasospasm on endovascular access should not be underestimated and subsequent attempts can be successful after a period of resuscitation.
Footnotes
Declaration of Conflicting Interests
The authors declare that there is no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent has been given by the patient for the publication of the case details and images.