
Abstract
Purpose
This study aims to determine the clinical effectiveness of a stent with radioactive seed strand (RSS) inserted in patients with superior vena cava (SVC) obstruction (SVCO) secondary to non-small-cell lung cancer (NSCLC).
Methods
Between January 2013 and December 2019, 63 patients with SVCO related to NSCLC received stent implantation with (n = 30) or without (n = 33) RSS insertion at our center. The clinical efficacy, stent patency duration, and overall survival (OS) were compared between these two groups.
Results
Both groups achieved 100% clinical and technical success rates. There were no obstacles associated with the procedure performed for the patients. Two patients in the RSS group and 7 patients in the stent-alone group experienced stent re-stenosis. The rate of re-stenosis between the two groups was not significantly different (P = .099). Patients in the RSS group had significantly longer median patency than those in the stent-alone group (381 vs 309 days, P = .045). All patients died because of the development of tumors during the follow-up. Patients in the RSS group had a significantly longer median OS than those in the stent-alone group (229 vs 178 days, P = .026). During the follow-up, no patient in the RSS group suffered RSS migration or brachytherapy-related complications.
Conclusion
For patients with SVCO secondary to NSCLC, a stent with RSS insertion is efficacious and safe, and it may improve stent patency and OS.
Introduction
Superior vena cava (SVC) obstruction (SVCO) can be secondary to lung cancer and other mediastinal tumors.1-4 Lung tumors are responsible for more than 90% of the cases of malignant SVCO in patients.5-7 Patients with malignant SVCO, in general, cannot be treated surgically since their tumors highly advanced. 1 Only palliative therapies have been appropriate for these patients.
Many research studies have concluded that stent insertion might be used as a first-line treatment for most SVCO patients because the stent gave a rapid relief from SVC syndrome.5-7 Though, after an initial successful endovascular stent placement, re-stenosis of the SVC stent occurred in up to 41% of patients. 7 The re-stenosis of the SVC stent was mainly caused by tumor growth. 8
Many researchers inserted a radioactive seed strand (RSS) beside the stent to provide brachytherapy effectiveness and prevent stent re-stenosis in patients with malignant luminal obstructions.9-11 However, this technique has not been used for patients with malignant SVCO. In addition, previous research studies also did not focus on patients with SVCO caused by a specific cancer type.5-7
Here, we aim to assess the clinical effectiveness of patients with SVCO secondary to non-small-cell lung cancer (NSCLC) following stent with RSS insertion.
Materials and Methods
Ethics committee of Xuzhou Central Hospital approved this single-center retrospective study (No. XZXY-LJ-20210115-014). Written informed consent was not required due to the retrospective nature of the investigation.
Patients
Our analysis comprised 63 patients with SVCO secondary to NSCLC who were treated with stent insertion between January 2013 and December 2019. The criteria for the inclusion of these patients were as follows: (a) a confirmed malignant SVCO diagnosis, (b) SVCO caused by NSCLC, and (c) inoperable cases. Exclusion criteria for these patients were as follows: (a) Eastern Cooperative Oncology Group performance status (ECOG PS) ≥ 4; (b) patients who underwent post-operative external radiotherapy; and (c) patients who experienced severe renal, lung, cardiac, or coagulatory dysfunctions.
Baseline Data of the Included Patients.
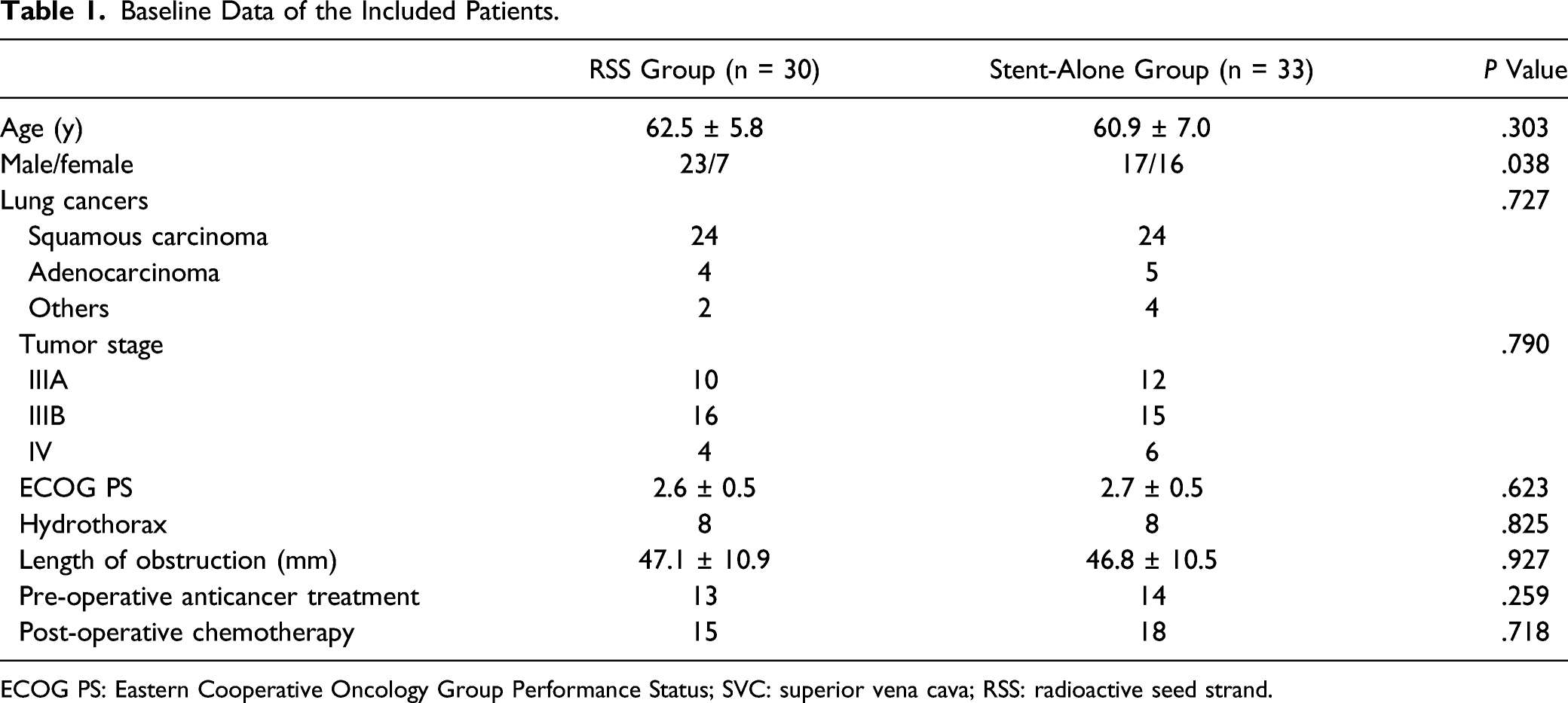
ECOG PS: Eastern Cooperative Oncology Group Performance Status; SVC: superior vena cava; RSS: radioactive seed strand.
Diagnosis
Patients with malignant SVCO were diagnosed using a combination of symptoms and the findings of a thoracic contrast-enhanced computed tomography (CT) scan (Fig. 1(a)). The length and degree of SVCO were assessed by CT. The pathological diagnoses of NSCLC were made by the bronchoscopy or CT-guided biopsy results. A 58-year-old man with SVCO secondary to NSCLC underwent stent with RSS insertion. (A) Pre-operative CT demonstrated the SVC (arrow) was compressed by the NSCLC. (B) The length and degree of obstruction were confirmed via SVC venography. (C) The stent was being released from the stent delivery system (long arrow), and a guide catheter (short arrow) which was used to deliver the RSS was placed beside the stent. (D) The RSS (short arrow) and stent (long arrow) were adjusted to be placed in parallel in the vascular lesion segment. (E) The SVC venography confirmed the patency of stent. (F) The follow-up CT obtained 3 months after stent (long arrow) and RSS (short arrow) insertion showed the patency of stent.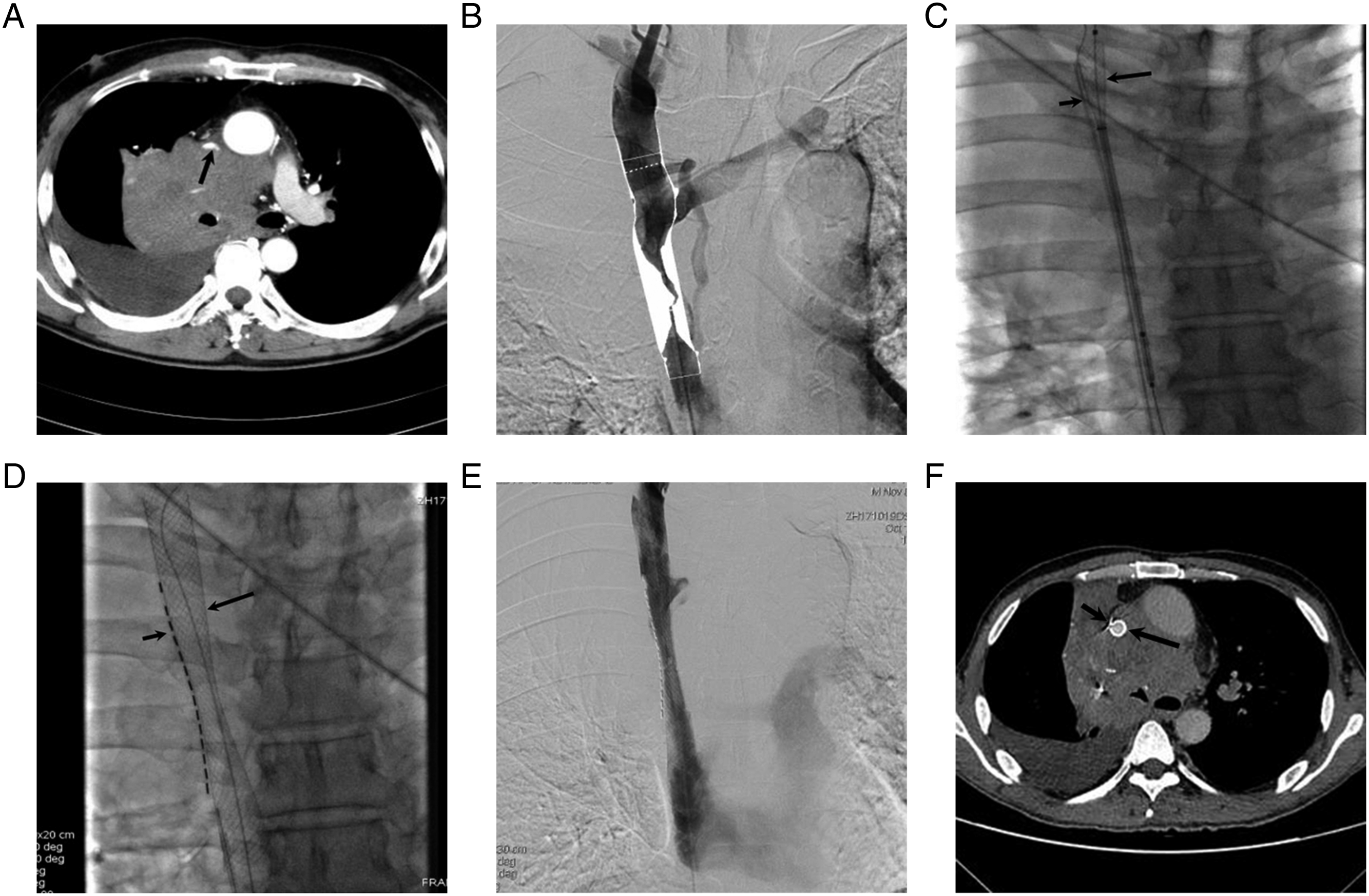
Stents
All stents used in this study were uncovered self-expanded metal stents (Wallstent, Boston, Marlborough, MA, USA). The stent diameter was 10%–15% larger than that of the SVC, and the stent length extended at least 10 mm beyond both sides of the SVCO.
Radioactive Seed Strand
An RSS was produced using a 4F medical plastic tube (Boston) that was combined with several I-125 seeds (Chinese Atomic Energy Science Institution, Beijing, China). To obtain the RSS, the tube was sealed at the distal end and I-125 seeds were placed linearly along the catheter. The remaining proximal segments of the tube that did not contain seeds were removed, and the proximal end was then sealed.
Each I-125 seed (dimensions: 4.5-mm long, .8-mm diameter) emitted a low-energy of 35.5-keV γ-rays with a half-life of 59.6-day. The SVCO length was used to estimate the number of I-125 seeds to be inserted in the medical plastic tube.
Stent Insertion Alone
All processes were carried out under fluoroscopic guidance, and the right femoral vein was pierced. A 5F VER catheter (Cordis, Miami, Florida, USA) and .035-inch guide-wire (Terumo, Tokyo, Japan) were sent to the SVCO distal site. Once this was accomplished, the catheter was pushed proximally along the guide-wire to the obstruction. SVC venography was used to confirm the length and degree of obstruction, and a rigid guide-wire (Cook, Bloomington, Indiana, USA) was implanted in place of the original guide-wire. The SVCO was then dilated using a balloon with a diameter of 10–12 mm (Cordis), and a stent was delivered to the obstructed area via the rigid guide-wire, with the stent positioned to cover the SVCO.
Stent With Radioactive Seed Strand Insertion
All procedures were performed under fluoroscopic guidance, and bilateral femoral veins were pierced. The stent was inserted via the right femoral approach, and the RSS was inserted via the left femoral approach. The procedures of stent insertion were the same as those mentioned above. The stent delivery system was placed at the SVCO’s lesion segment via the rigid guide-wire (Cook), and the RSS was also administered to the SVCO’s lesion segment via guide catheter (Fig. 1(b)-(c)). The RSS and stent were adjusted to be parallel (Fig. 1(d)-(e)). The stent was released first, and then the guiding catheter was smoothly removed to release the RSS.
Post-Stenting Treatment
Patients were given subcutaneous low-molecular-weight heparin (6000 IU/12 h) for 3 days before oral administration of warfarin sodium to keep their international normalized ratio between 2 and 3.
Assessment
Elimination of the SVCO was used to define the technical success of stent implantation.5-8 The elimination of the SVCO was confirmed by the post-stenting SVC venography. The successful positioning of RSS between the stent and the SVC wall was classified as the technical success of RSS insertion. The clinical success was considered only when the stent’s two-sided pressure gradient was less than 10 mmHg following stenting.5-8
Patients were followed up every 6 months till death after a regular checkup at 1, 3, and 6 months. Patients had a thoracic contrast-enhanced CT scan and clinical assessments during follow-up. The return of SVCO symptoms was thought to indicate stent re-stenosis.
Stent patency was the primary endpoint in this study, with secondary endpoints including technical success, clinical success, and overall survival (OS)
Statistical Analysis
SPSS v16.0 (SPSS, Chicago, IL, USA) was utilized for all statistical analyses. To compare the continuous and categorical data, we employed t-test and χ2 test, with paired t-test used to compare the changes before and after stent implantation. The survival-related data were calculated and compared by Kaplan–Meier curves and log-rank test. Any patient who died without stent re-stenosis was censored from the study for patency calculations. A multivariate Cox regression analysis was used to look for factors that were linked to patient survival. In this multivariate model, any variable with a P < 0.1 value in univariate analysis was included. The significance level was set at P < .05.
Results
Technical Success
In the stent-alone group, all patients had technical success with stent implantation. Furthermore, all patients in the RSS group had technical success with the insertion of the stent. Table 1 shows the baseline information for the 63 patients. The proportion of males was significantly higher in RSS group than that in stent-alone group (P = .038). The other baseline data were comparable between the 2 groups. Each patient received 1 stent with 12–14 mm of diameter and 60–90 mm length. In the RSS group, each patient received 1 RSS and each RSS contained 12–16 I-125 seeds. No patient experienced procedure-related complications.
Clinical Success
Clinical Effectiveness in Two Groups.

RSS: radioactive seed strand.
Patency
No patient was lost in the follow-up process. Two patients in the RSS group and 7 patients in the stent-alone group experienced stent re-stenosis. The rate of re-stenosis in the 2 groups was not significantly different (7/33 vs 2/30, P = .099). Eighteen and fifteen patients in stent-alone and RSS groups received chemotherapy after stent insertion, respectively, (P = .718). In the RSS group, no patient experienced RSS migration or brachytherapy-related complications during the follow-up.
Stent re-stenosis was induced by tumor ingrowth (n = 6) or thrombi development (n = 1) in the patients in the stent-alone group. Five of the 7 patients had their stents replaced again, 1 was treated with catheter-directed thrombolysis, and 1 refused further therapy.
All stent re-stenosis in the RSS group was caused by tumor ingrowth, and they were treated with repeat stent implantation.
Patients in the RSS group had considerably longer median patency than those in the stent-alone group (381 vs 309 days, P = .045, Fig. 2). Kaplan–Meier curve demonstrated a longer stent patency period was found in stent with RSS group.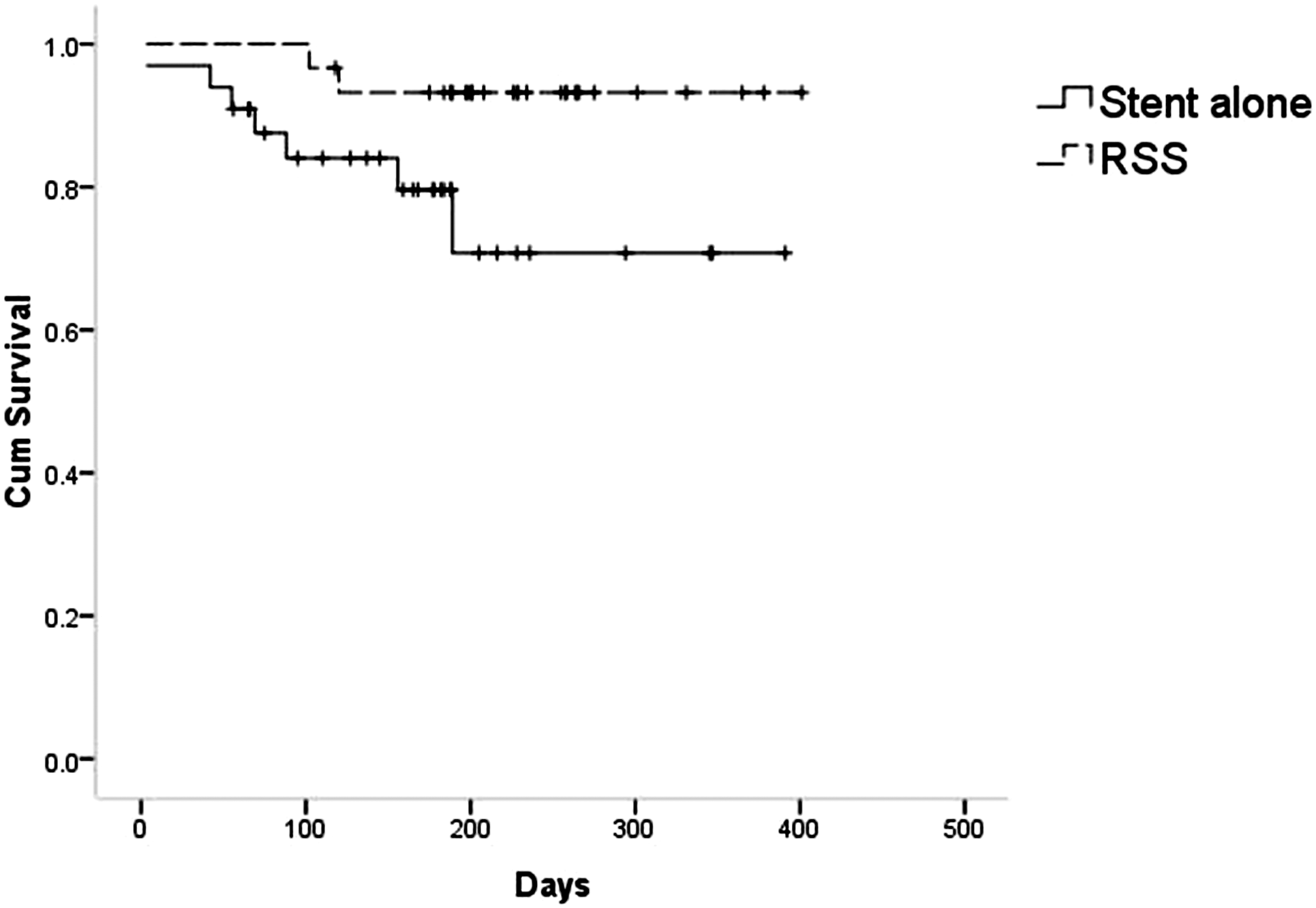
Predictors of Stent Re-stenosis.
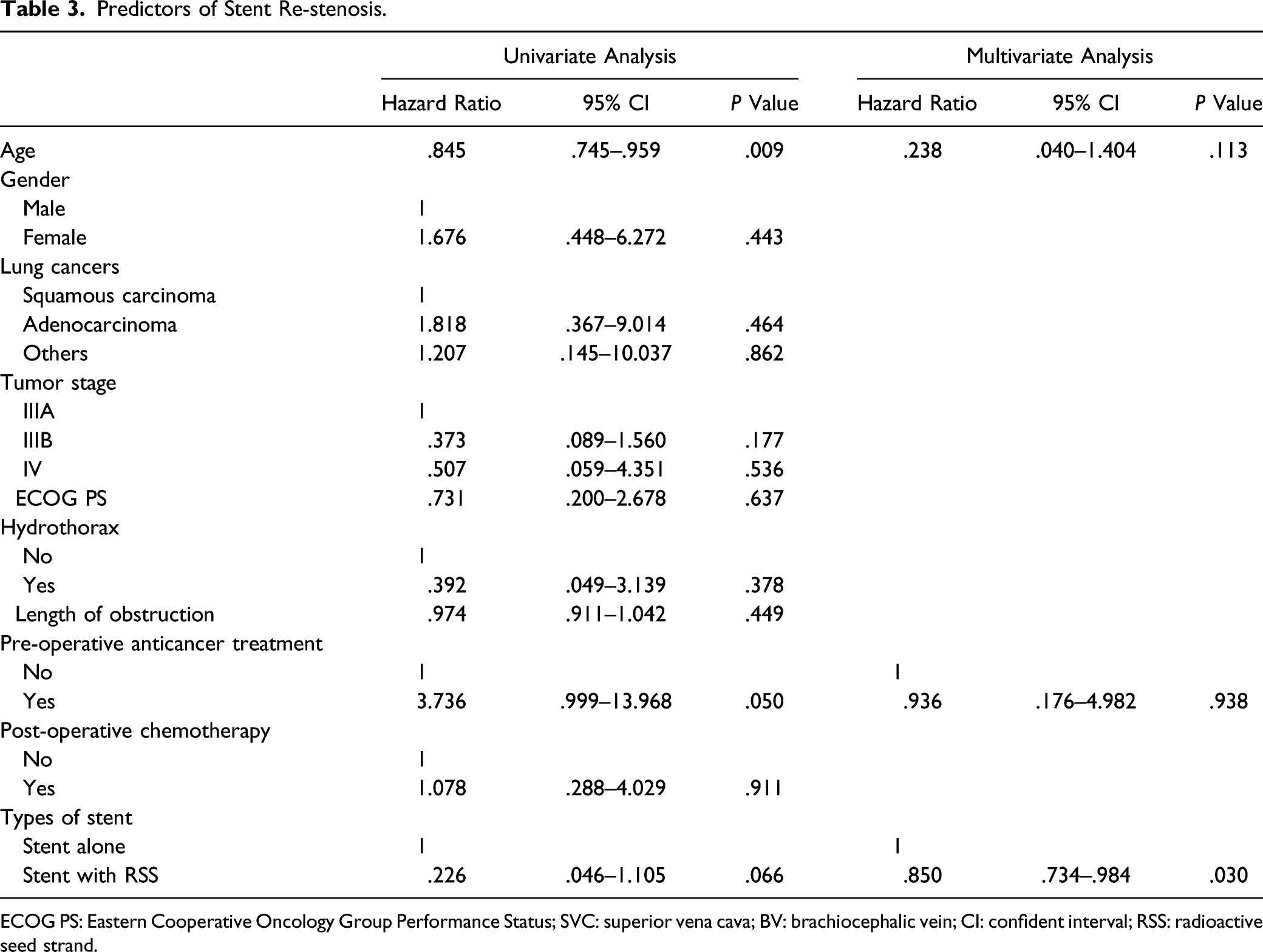
ECOG PS: Eastern Cooperative Oncology Group Performance Status; SVC: superior vena cava; BV: brachiocephalic vein; CI: confident interval; RSS: radioactive seed strand.
Overall Survival
All patients died as a consequence of tumor development during the follow-up. Patients in the RSS group had a considerably longer median OS than those in the stent-alone group (229 vs 178 days, P = .026, Fig. 3). Kaplan–Meier curve demonstrated a longer OS was found in stent with RSS group.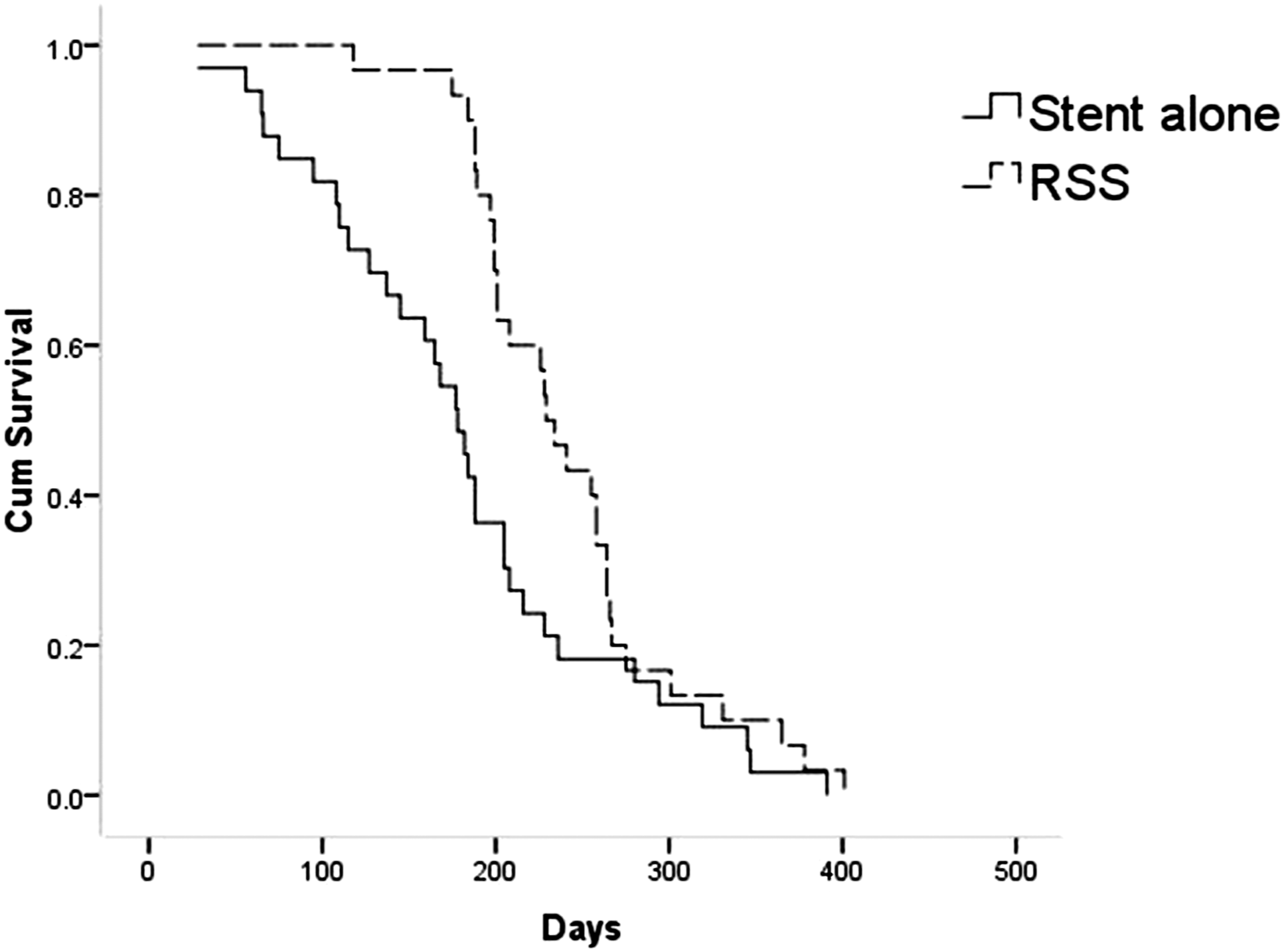
Predictors of Overall Survival After Stent Insertion.
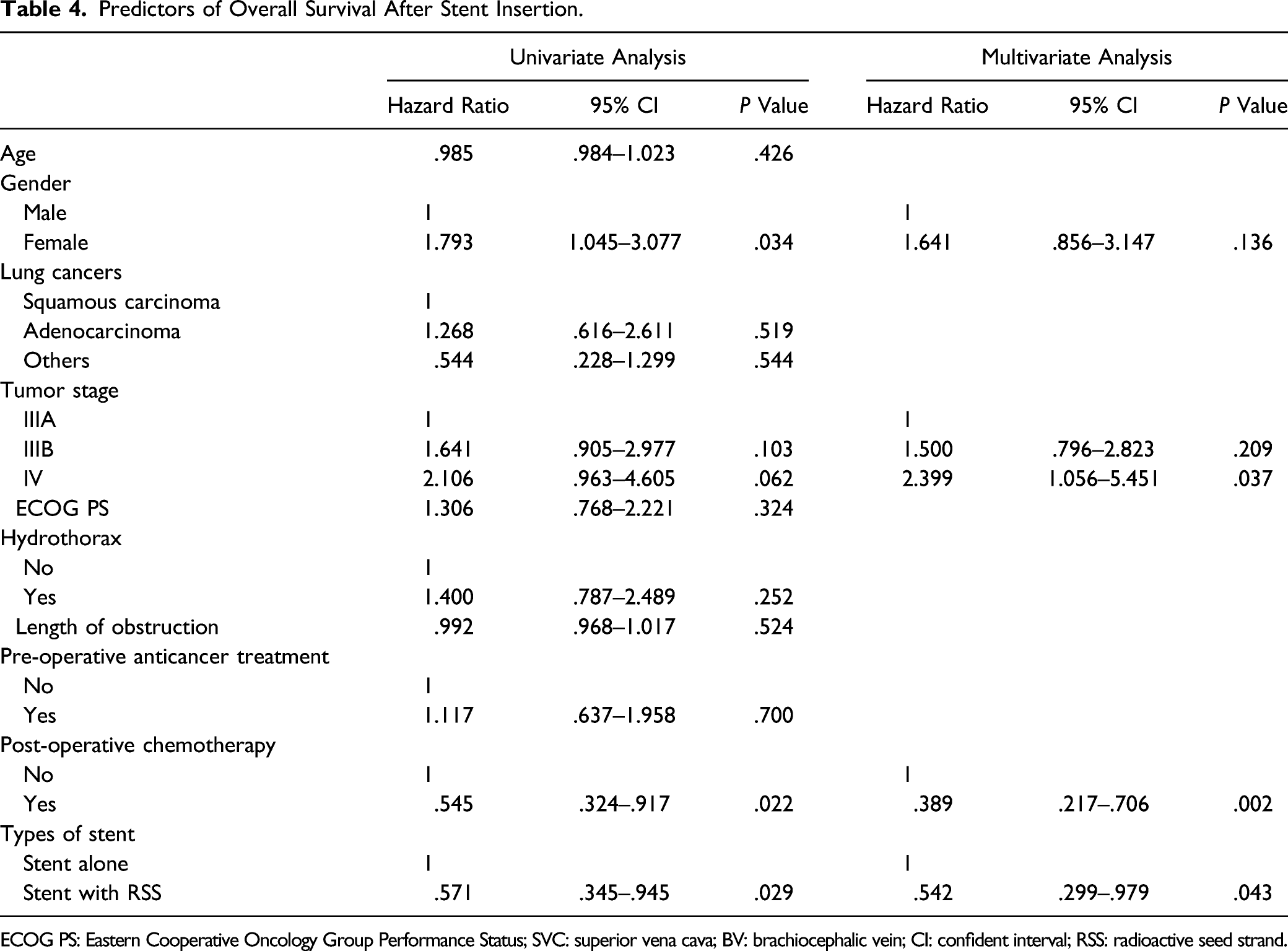
ECOG PS: Eastern Cooperative Oncology Group Performance Status; SVC: superior vena cava; BV: brachiocephalic vein; CI: confident interval; RSS: radioactive seed strand.
Discussion
In this study, we compared the relative long-term outcomes and clinical efficacy between patients with SVCO secondary to NSCLC who underwent stent alone and stent with RSS insertion. For both treatment modalities, we achieved 100% technical and clinical success. This demonstrates that RSS implantation had no influence on the initial therapeutic efficacy of stent implantation for SVCO symptoms. The RSS took up a little space in the SVC lumen and did not affect blood flow.
All of the participants in this research had uncovered stents. In patients with SVCO, tumor ingrowth is the most common cause of stent re-stenosis. 7 Therefore, many researchers used the covered stents to prevent tumor ingrowth.5,7,8 Indeed, no patients with SVCO experienced tumor ingrowth after covered stent insertion, and covered stents may reduce the rate of stent re-stenosis.7,8 Wang et al 8 discovered that when malignant SVCO patients were treated with covered stents rather than bare stents, the stent patency duration was longer (374 days vs 317 days, P = .049). However, more than half of the patients received anticancer treatments after stent insertion in Wang’s study. 8 Anticancer treatments might also play an important role in improving stent patency.
Brachytherapy has been widely used for anticancer treatment.12,13 I-125 seeds have been widely used during brachytherapy procedures because they have a long half-life, a narrow irradiation range, and a high radiobiological effect.9-11 Stent with RSS insertion has been used for patients with malignant biliary obstruction, portal venous tumor thrombus, and cancer-associated venous obstruction.9,10,14 The RSSs were effective in suppressing tumor growth and ensuring long-term patency.
In this study, the RSS group had significantly longer stent patency than the stent-alone group (381 days vs 309 days; P = .045). However, the rates of stent re-stenosis were not significantly different between the 2 groups (7/33 vs 2/30, P = .099). That is to say, RSS may not prevent tumor growth because: (a) brachytherapy was not consistently effective in all patients, and (b) RSS only affected a small part of tumor near the stent, and thus, the entire tumor could not be only treated by the RSS. Nevertheless, RSS did prolong the stent patency duration by prolonging the time to tumor progression. Multivariate analysis also showed that the use of RSS was the independent factor of longer stent patency. This could be due to the RSS’s ability to suppress tumor cell multiplication, induce tumor cell death, and diminish vascular intimal hyperplasia, all of which help to reduce the risk of re-stenosis following stent implantation. 10
The median OS in the stent with RSS group in this study was 229 days, which was significantly longer than the 178 days in the stent-alone group (P = .026). However, multivariate analysis showed many other factors (including use of post-operative chemotherapy and lower tumor stage) were also associated with the longer OS. Therefore, a stent with RSS insertion combined with post-operative chemotherapy might be recommended for the patients with SVCO secondary to NSCLC. We did not compare the OS of patients with stage IV NSCLC who received a stent alone versus a stent plus RSS since each group only comprised 6 and 4 patients, respectively. Further analysis still requires more sample size.
In this study, we did not observe any patient who experienced RSS migration. This finding might be attributed to that the diameter of the stents was 10%–15% larger than that of the SVC. Even if the tumor shrinks, the bigger stent can precisely hold the RSS in the blood channel, preventing migration.
This study had various limitations. To begin with, the current study’s sample size is small, and the retrospective clinical study brings various biases into the data analysis. Though the study’s unique cancer type may reduce the possibility of bias, more prospective studies are needed to confirm our findings. Second, because these patients originated from a single center which exhibited insufficient validations from a variety of characteristics that are underplayed in various clinical settings. Third, because of the smaller sample size, the clinical efficacy of 2 procedures in stage IV patients could not be determined.
In conclusion, stent implantation with RSS is safe and effective for patients with SVCO secondary to NSCLC, it may improve stent patency and OS. However, more prospective, multicenter clinical trials are needed to confirm the findings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.