
Abstract
Introduction
Published evidence of venous thrombotic complications of COVID-19 is lacking from India. This case series consists of twenty-nine adult patients who were COVID -19 positive and treated for Deep Vein Thrombosis (DVT) during the second wave of the COVID-19 pandemic, in India. The study was aimed at analyzing patient demographics of patients with DVT and the outcome of Catheter-Directed Thrombolysis (CDT) in COVID positive patients.
Keywords
Introduction
As on the 20th of July 2021, there were a total of 191 million cases of Coronavirus with 4.1 million deaths worldwide, of these, 31.2 million and 414,000, respectively, are from India. 1 The exact mechanism of thrombosis due to SARS-CoV-2 infection whilst being less understood, one aspect is clear, and that is the association with a prothrombotic phenotype and probably endothelial inflammation. 2 Coagulopathy is associated with the COVID-19 infection and has led to a high incidence of both arterial and venous thrombosis with its associated complications whilst the mortality was lesser than the first wave.
General observation has been that sub-segmental pulmonary embolism (PE) is reportedly commoner in the second wave despite a higher number patients being on prophylactic anticoagulation.3,4 The increase in numbers of critically ill patients due to the more virulent delta variant could be the reason for this.
We analyzed data of twenty-nine patients who presented with DVT during a 3-month period who were managed with either CDT plus anticoagulation or with anticoagulation alone. The experience and observations in this case series is shared while stressing on the need for compiling a larger series before drawing definitive conclusions about the management of COVID associated DVT.
Material and Methods
Patient Characteristics on Presentation.
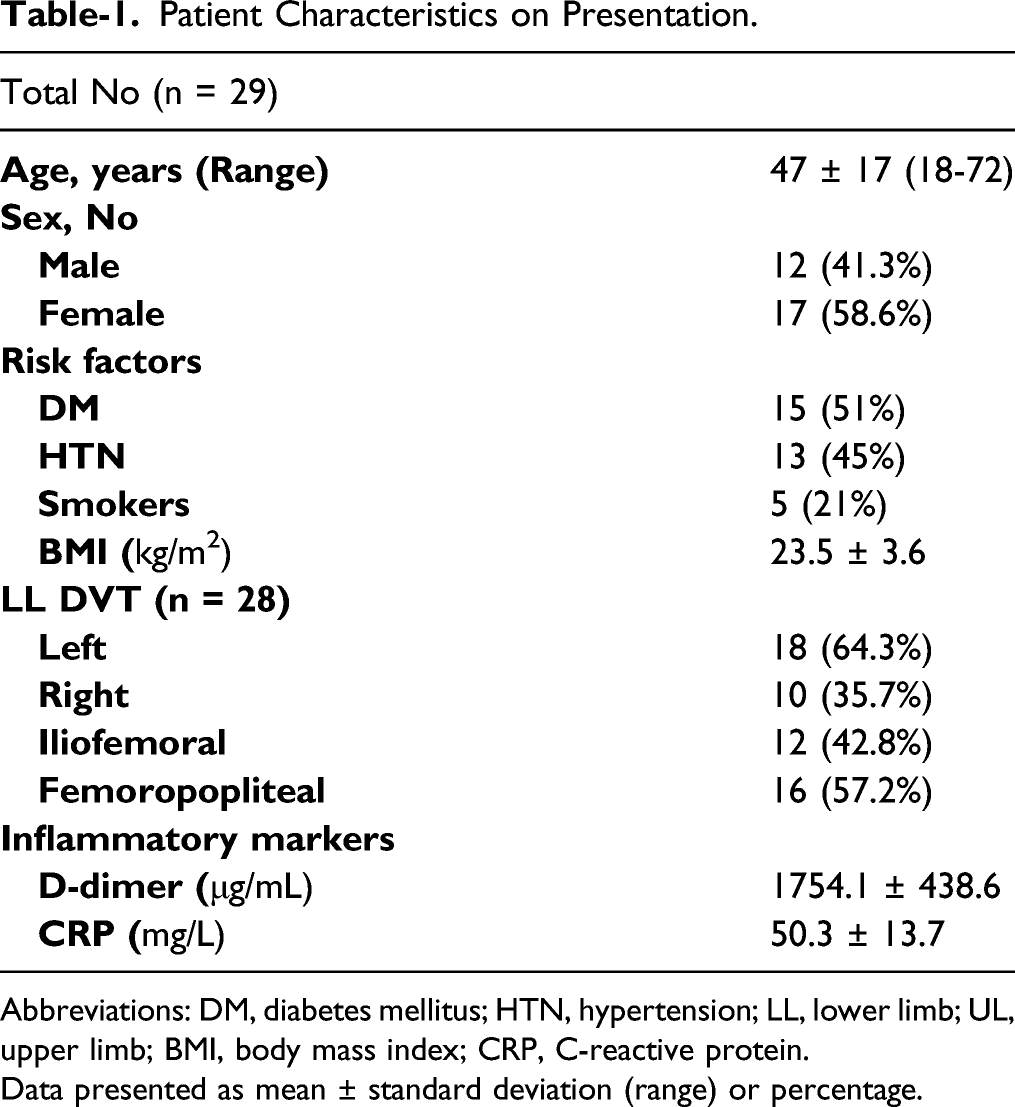
Abbreviations: DM, diabetes mellitus; HTN, hypertension; LL, lower limb; UL, upper limb; BMI, body mass index; CRP, C-reactive protein.
Data presented as mean ± standard deviation (range) or percentage.
CDT was performed after ultrasound guided access of the popliteal vein in prone position under local anesthesia via a 6Fr sheath (RadiofocusR,Terumo) which was upgraded after a venogram through this sheath, to a 8Fr sheath (Avanti+R,Cordis) whilst systemic heparinization with unfractionated heparin [UFH] at 1 mg/kg was given. An 8 Fr guide catheter (Vista BriteR,Cordis) was then introduced over the wire in to the vein and then a 50 mL Luer-lock syringe was connected to the catheter. A thromboaspiration performed with rapid to and fro movements of the guiding catheter in the thrombus. Inferior Venacava (IVC) filters were not used in any of the patients prior to CDT. A check venogram was performed assess thrombus reduction and clearance. Thereafter, a 4Fr multi-hole valved infusion catheter (Cragg-McNamaraR, Medtronic) was introduced over a .35 angled glide wire (RadiofocusR, Terumo) and the catheter was placed about 5 cm into the (IVC). A bolus dose of 10 mg of Tissue Plasminogen Activator (TPA) was infused over a period of 1-2 minutes. This was followed by an infusion of 10 mg of TPA via the catheter for 2 hours and a completion venogram performed and the hardware removed (Figures 1A-1D). If there was evidence of a May-Thurner lesion then dilatation of the lesion was done with 14 or 16 mm × 40 mm non-complaint balloon (AtlasR,Becton-Dickinson and Company). All patients were discharged on Rivaroxaban 15 mg twice daily for 3 weeks, followed by 20 mg once daily for 3 months. (A) Iliofemoral deep vein thrombosis; (B) Post-catheter-directed thrombolysis of iliofemoral deep vein thrombosis; (C) Femoropopliteal deep vein thrombosis; (D) Post-catheter-directed thrombolysis of femoropopliteal deep vein thrombosis.
Those group of patients who were managed medically were also put on the above regimen of Rivaroxaban. Both groups received Aspirin 75 mg for similar duration and were also advised to wear class II below knee compression stockings. All patients were advised clinical review at 1, 4, and 8 weeks. A venous duplex study and Villalta scoring was also done at 3 months.
Results
There were 29 patients in this cohort, 12 male and 17 female. The mean age was 47 ± 17 years, with range being 18 –72 years. 15 (51%) had diabetes mellitus, 13 (45%) were hypertensive, and 6 (17%) were smokers. Mean body mass index was 23.5 ± 3.6 kg/m2 [Range 19.2–33.5]. None of the female patients were on oral contraceptive pills or hormone replacement therapy. Eight-six percent had not received any COVID vaccine and the remaining 14% had received only one dose. Average time of presentation from being COVID positive was 17.8 ± 3.6 days and all but one patient developed DVT after becoming Covid negative. None of the patients were prophylactic anticoagulation at presentation. 28 patients had lower limb involvement, with 12 (42.8%) having IF and 16 (57.2%) FP DVT. 10 of 16 patients having involvement of FP segment and 8 of 12 having IL DVT had symptoms on the left side. One patient had upper limb DVT involving the brachial and axillary vein. This patient was diagnosed as a case of Paget-Schrotter and at follow-up is doing well with minimal swelling and discomfort. She refused to undergo any surgical procedure and hence was put on an extended regimen of anticoagulation for 6 months with Rivaroxaban and grade-2 custom made compression garment. Average D-dimer and CRP levels on first consultation were 1754.1 ± 438.6 μg/mL and CRP 50.3 ± 13.7 mg/L, respectively.
Treatment and Outcome of Lower Limb DVT Cohort.
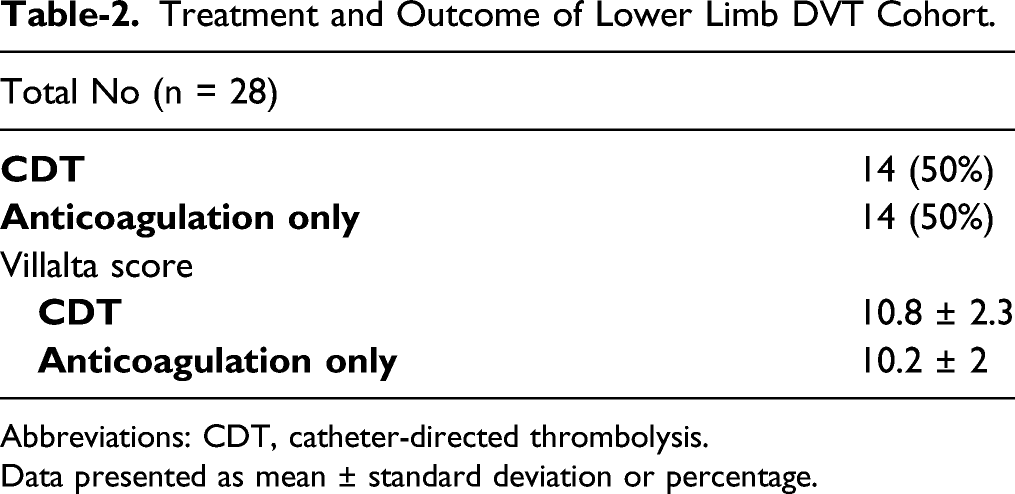
Abbreviations: CDT, catheter-directed thrombolysis.
Data presented as mean ± standard deviation or percentage.
Discussion
In a recent study, comparison was made of thrombotic complications and survival in hospitalized patients who had COVID-19 infection between the first and second wave of the pandemic. They found that in the second wave the overall mortality risk was reduced by 47%, but the cumulative incidence of thrombotic complications was still high, more so in the ward patients, despite advances in the management of the infection and higher use of LMWH. 3 PE was being diagnosed a median of 2 days prior to transfer to ICU due low threshold for diagnostic tests and imaging.3-6
The mechanism of coagulopathy in the above subset of patients is not fully understood. An association with a prothrombotic phenotype has been found. 2 Interestingly in the second wave, the majority of the patients had no sign or symptom of VTE at admission, but, were found to have sub-segmental PE on imaging done to assess their respiratory status. This could be because patients were getting a lower dose of LMWH than needed, higher dose of steroids that could have contributed to thrombosis or as a direct SARS-CoV-2-specific procoagulant effects.4,5,7 Screening tests to identify patients at risk of COVID-associated VTE remains elusive. The sensitivity and specificity of D-dimer ranges between 91–96% and 10–24%, respectively. Global coagulation assays like thrombin generation (TG) and rotational thromboelastometry (ROTEM) can be alternative tests to estimate COVID-19 associated coagulopathy and thrombosis risk. 2 Clinicians need to have a high index of suspicion and a low threshold for diagnostic imaging, especially when the quality of CTPA has improved.4,6
Unlike in the first wave of COVID-19 where high prevalence of VTE was noted in the aged (>65 years) and critical population, in the second wave, younger (47 ± 17 years) and less sicker patients were affected. 8 In our study, none of the patients were on any prophylactic anticoagulation. This probably does not support the view for the need for higher doses of thromboprophylaxis to prevent VTE in COVID positive patients.9,10 We observed in our series a higher incidence of DVT in female patients when compared to males. In a meta-analysis from Italy, male sex did not impact outcomes of VTE. 11 In this series, all except one patient developed symptomatic DVT, after being tested negative for COVID-19, suggesting a need for an extended duration of prophylactic anticoagulation in this subset of patients. However, there is conflicting evidence regarding use of post-discharge thromboprophylaxis in COVID-19. Though societal guidelines do not support use of extended thromboprophylaxis, some recent studies support their use in select situations.12-14 All the patients had elevated D-dimer and CRP but these alone cannot be used as an indicator toward a higher propensity for coagulopathy. 15
Literature is sparse on use of CDT for COVID-associated proximal DVT and current guidelines favor use of medical management over advanced therapies for IF DVT.16,17 In this study, 14 patients underwent successful CDT, with good radiological and clinical improvement. There were no procedure-related complications and results were similar to non-COVID patients with similar involvement. The authors recommend considering the use of CDT for all with COVID-associated IF DVT and those with FP DVT who have significant edema and or impending venous gangrene if the bleeding risk is within acceptable limits. The presence of co-morbidities like diabetes, hypertension, or smoking did not seem affect outcome of treatment.
The Villalta score is a useful tool to follow-up outcomes of DVT and there seems to be no published literature, which had looked at long-term outcome in this patient population. 18 We found no significant difference in outcome between COVID and Non-COVID patients with VTE at 3 months follow up. Finally, patients in our study treated with CDT did not re-thrombose, unlike the experience of the authors with CDT for acute limb ischemia in COVID patients.
Limitations
Our study is retrospective and being multi-centric can have variations in management protocols at presentation, admission, and ICU care of COVID-19 infected patients. Pre-intervention Villalta score assessment was not possible in any of the patients as both the centers where the study was carried out were converted to “COVID centers” by the government for in-patient care. The case load was very high and the members of staff were thin on the ground. All the patients with IF DVT underwent CDT with anticoagulation and there was no comparison group in the same subset where anticoagulation alone was used. The numbers are small, and a larger cohort is needed to draw definitive conclusions or formulate guidelines. Having said that, literature about DVT in the second wave from India is non-existent as of now. Future studies should involve centers that manage VTE patients with CDT and agree on a common management protocol. There is need to assess the diagnostic and prognostic accuracy of tests like TG and ROTEM whilst continually attempting to understand coagulopathy in COVID-19 patients.
Conclusion
Coagulopathy associated with the COVID-19 pandemic remains an enigma. We suggest that CDT could be offered to COVID positive patients with symptomatic Iliofemoral DVT with good outcomes and an acceptable post-intervention Villalta score. The overall treatment of COVID-associated DVT and its outcomes do not appear to be different from non-COVID patients. A Randomized controlled trial looking at full anticoagulation vs CDT in high-risk patients and its outcome in reducing thrombotic complications with reduced risk of bleeding is needed which would also help to formulate guidelines for recommending catheter-directed thrombolysis vs anticoagulation alone in COVID-associated DVT.
Footnotes
Acknowledgments
Ms. Kinari Shah for helping with data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.