
Abstract
Antiphospholipid syndrome is an autoimmune condition characterized by arteriovenous thromboembolic events. Thrombocytopenia is a common finding among these patients and is typically of mild severity not requiring any treatment. However, severe cases of thrombocytopenia should be treated. Steroids, intravenous immune globulin (IVIG), and immunomodulatory agents are the first-line treatment options, and surgical splenectomy is usually reserved for more severe and refractory cases of thrombocytopenia. Herein, we report the case of a 30-year-old man with primary antiphospholipid syndrome and severe thrombocytopenia. The patient’s thrombocytopenia had been refractory to almost all the medical managements, and surgical splenectomy could not be an option due to the patient’s high-risk condition for surgery. The patient was successfully managed by partial splenic embolization (PSE) which was a unique application of this technique.
Keywords
Introduction
Thrombocytopenia has a reported incidence rate of 16–44% among patients with antiphospholipid syndrome (APS) 1 and is usually of mild to moderate severity. Severe thrombocytopenia (platelet count < 50 000 /microL), however, is relatively rare among these patients with a reported incidence rate of 3%. 2
It has been proposed platelet counts above 50 000 /microL usually do not require treatment in patients with APS; however, platelet counts below 20 000 /microL should receive treatment. 3 Glucocorticoids with or without intravenous immune globulin (IVIG) are the first-line, and mycophenolate mofetil, cyclophosphamide, and azathioprine are the second-line treatment options. 3 Surgical splenectomy is also proposed as a treatment option; though, it should only be reserved for patients with severe and refractory thrombocytopenias due to increased risks associated with surgery in this population. 3
Partial splenic embolization (PSE) has been proven as a safe and effective treatment option for thrombocytopenia and portal hypertension in various disease conditions.4,5 However, to the best of our knowledge, there is no report on application of this technique for treatment of thrombocytopenia in patients with APS.
Herein, we report a 30-year-old man with medical history of APS who presented with an episode of epistaxis in the setting of severe refractory thrombocytopenia. The patient was successfully managed using PSE.
Case Presentation
A 30-year-old man with a medical history of primary APS presented to the emergency department because of spontaneous epistaxis. The patient was first diagnosed with APS 13 years ago, following an episode of unprovoked concurrent deep vein thrombosis (DVT) and pulmonary thromboembolism (PTE). The patient also had a history of left renal vein thrombosis and a second PTE occurring 1 year following the initial diagnosis.
The patient’s medication history included warfarin (5 mg tablet daily), aspirin (80 mg tablet daily), atorvastatin (20 mg tablet daily), and hydroxychloroquine (200 mg tablet twice daily). On examination, the vital signs were within normal limits. Two ecchymoses of 10 x 15 cm and 15 x 20 cm were noted on the posterior surface of the thorax. Laboratory findings were remarkable for severe thrombocytopenia (platelet count = 13 000 /microL), mild anemia (Hb=12.4 g/dL), and elevated INR of 2.0, and the peripheral blood smear was only remarkable for severe thrombocytopenia. Moreover, there was no splenomegaly or hepatomegaly on ultrasound examination.
Epistaxis was controlled with nasal packing, then, the patient was hospitalized for the management of severe thrombocytopenia. During hospitalization, intravenous corticosteroid and 2 courses of IVIG were administered, but only a minimal response was observed (platelet count increased to 35 000 /microL). A dose of rituximab was also administered, and the patient was discharged with oral corticosteroid. The platelet count was consistently low (30 000-40 000 /microL) on the two- and four weeks outpatient follow-up visits. Second dose of rituximab was also administered; however, on the six- and eight weeks outpatient follow-up visits, the platelet count plummeted to 9000 /microL. Therefore, the patient was readmitted for the inpatient management of severe thrombocytopenia.
Since the medical managements had been unsuccessful, surgical splenectomy was planned for the patient. However, on the third day of admission, the patient developed acute intermediate-risk PTE with resultant severe pulmonary hypertension making the patient a high-risk candidate for surgery. Following a multidisciplinary discussion, PSE was proposed as a possibly effective and safe treatment for the patient. All the possible risks and benefits and also the fact that enough evidence did not exist in the literature were explained for the patient, and PSE was planned after obtaining informed written consent.
Preprocedural, the patient was transfused with platelets to increase the platelet count to a level above 50 000 /microL and broad-spectrum antibiotics were administered in preparation for the embolization procedure. Under moderate sedation, femoral artery access was obtained using 18-G needle and 6-F sheath. Afterwards, celiac trunk was selected using a 5-F Cobra catheter (Cook Medical, USA) (Figure 1(a)), and the catheter was parked to the proximal segment of the splenic artery (Figure 1(b)). Subsequently, a microcatheter (EmboCathPlus, 2.9 to 3.0-French, Merit Medical, USA) was directed inside the inferior primary branch of the splenic artery and then inside the distal segmental branch supplying splenic lower pole (Figure 1(c)). Finally, subselective embolization of the splenic lower pole was performed by infusing 355- to 500-μm polyvinyl alcohol (PVA) particles to achieve near-stasis of flow in the target branches (Figure 1(d)) preserving perfusion to the upper pole (Figure 1(e) and (f)). Patrial splenic artery embolization in a 30-year-old man with primary antiphospholipid syndrome presenting with refractory thrombocytopenia and bleed. (a) Using a 5-F Cobra catheter, celiac trunk was selected and celiac trunk angiography was performed. Note the catheter tip (arrow). (b) The catheter was parked in the proximal segment of the splenic artery and splenic artery angiography was performed. Note the catheter tip (arrow), superior primary branch (arrowhead), and inferior primary branch (asterisk) of the splenic artery. (c) A microcatheter was advanced into the lower pole primary branch of the splenic artery and then into the more distal branch supplying a portion of the lower pole. (d) Subselective embolization of the splenic lower pole was performed using 355- to 500-μm polyvinyl alcohol (PVA) particles. Note the microcatheter tip (arrows). (e and f) Post-embolization angiography shows preserved vascular perfusion to the upper pole and complete embolization of lower polar branches.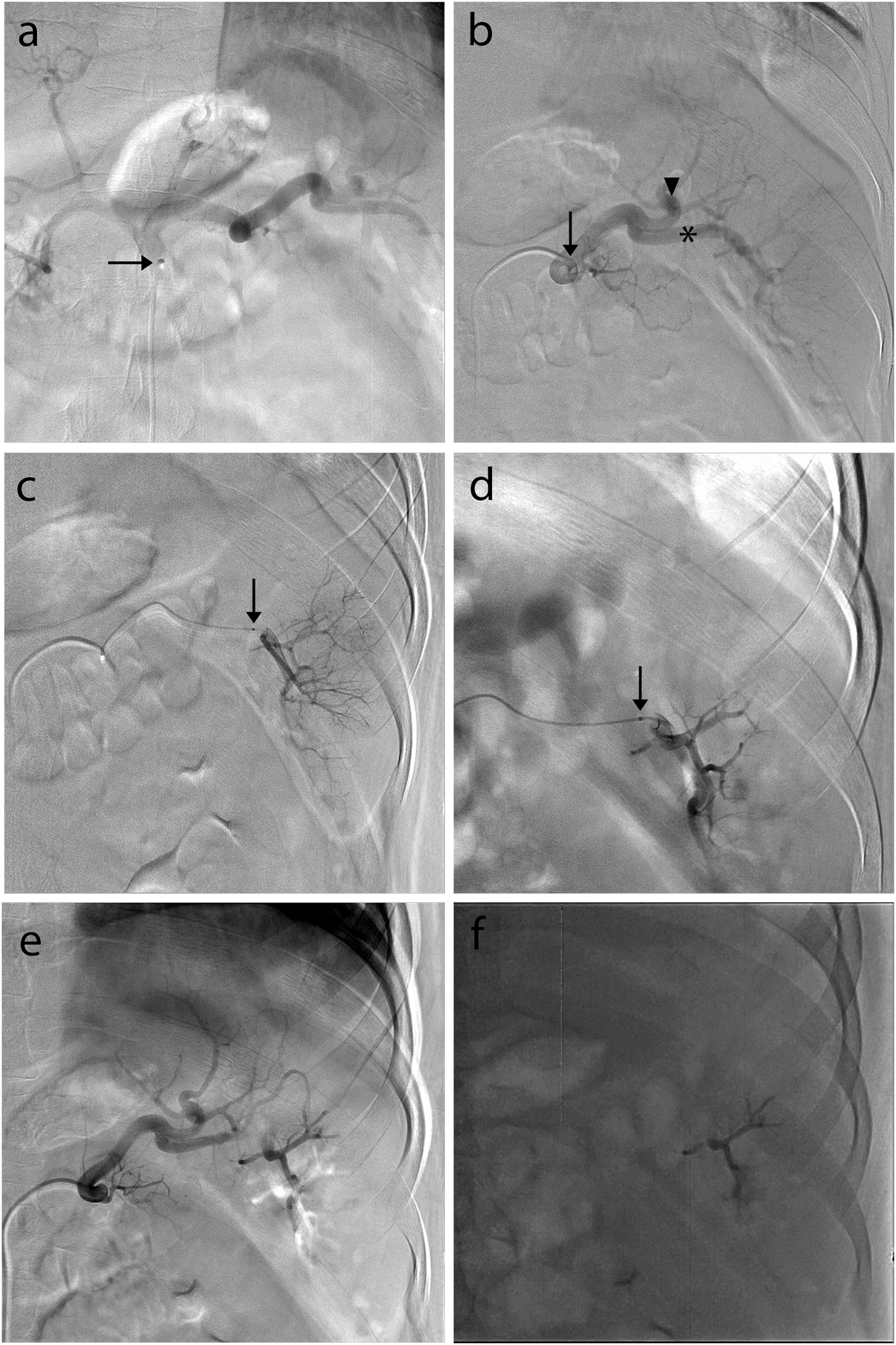
The platelet count started to rise within 24 hours following the procedure. Figure 2 shows the trend of platelet counts from the day of intervention to 2 months later. The post-embolization CT scan of abdomen performed 7 days following the procedure demonstrated the infarction of approximately 60% of splenic volume (Figure 3). A splenic lower pole abscess was also identified as a post-procedural complication which was successfully treated with systemic antibiotics and ultrasound-guided drainage. The culture of drained specimen was positive for staphylococcus aureus. At discharge, the patient’s final platelet count and INR were 100 000 /microL and 2.3, respectively. Platelet count trend after the intervention. This diagram shows the course of the patient’s platelet counts following the intervention. The post-embolization non-contrast CT scan of abdomen was performed 7 days following the procedure demonstrating the infarction of approximately 60% of splenic volume. Foci of air was also observed within the infarction area (arrow heads).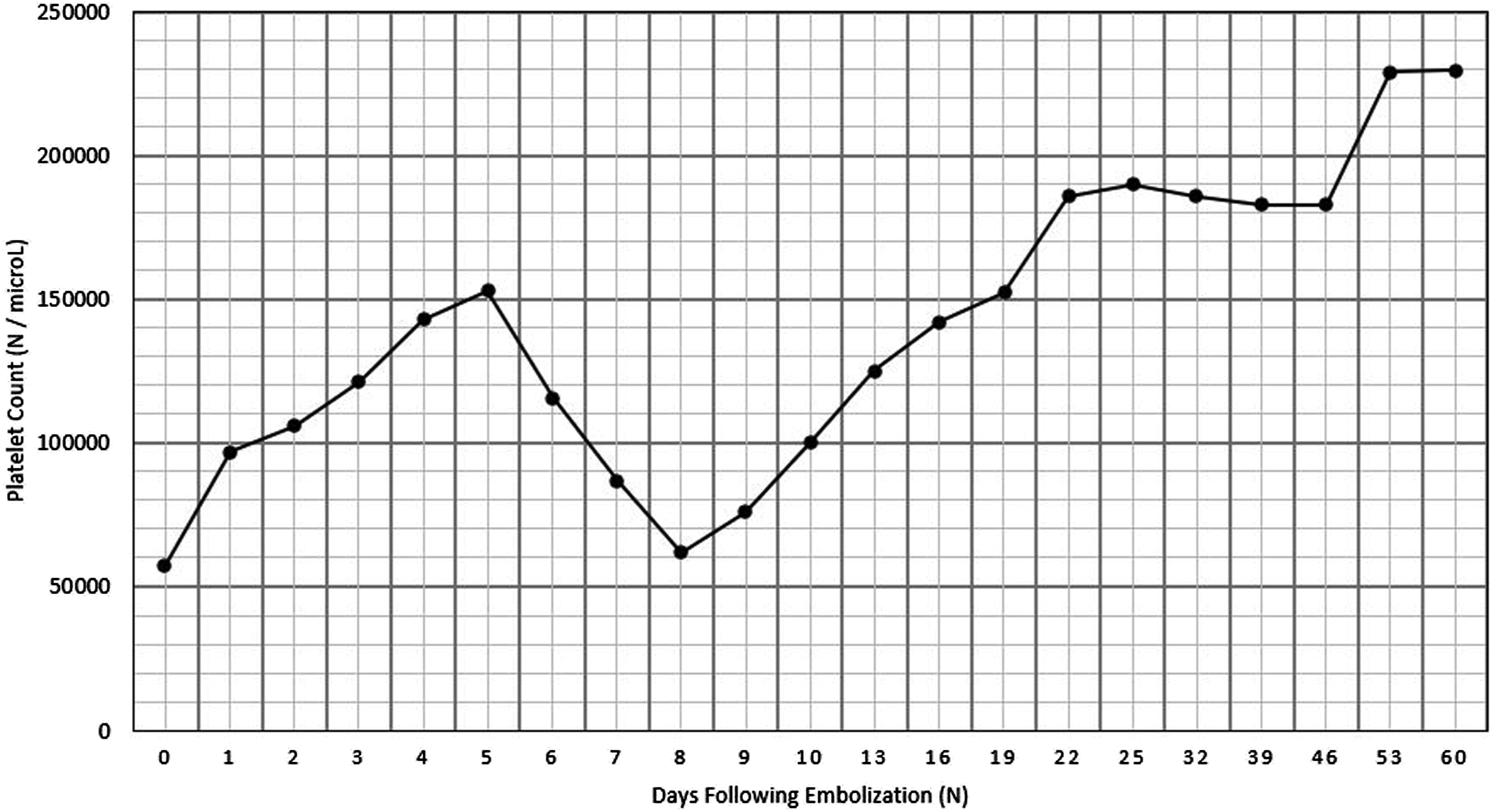

Discussion
PSE is a less invasive alternative to the surgical splenectomy that involves milder injuries and fewer complications. 6 Commonly used embolic agents in PSE include permanent agents such as polyvinyl alcohol (PVA) particles and steel coils and temporary agents such as absorbable gelatin sponge.6,7 The optimal choice between these embolic agents has not been defined and the decision has to be individualized for each patient. 7 As PVA particles are smaller, they can occlude the more distal branches of splenic circulation eliminating the possibility of collateral reperfusion to the targeted territory of splenic parenchyma causing a more complete infarction. Gelatin sponge is mainly criticized because of its temporary nature. 6 In addition, the more proximal occlusion of splenic artery with steel coil is shown to have a short-lasting effect on splenic parenchyma that is mainly attributed to collateral perfusion development to the targeted territory. 6 We chose to use 355- to 500-μm PVA particles for our patient since a significant and permanent improvement in the platelet count was desired.
The targeted amount of infarcted splenic volume has to be neither low nor high. Too small amount of volume reduction will not exert the desired effect on splenic function and too high amount of volume reduction will increase the risk for post-embolization complications, most notably, abscess formation.4,8 Although the optimal amount of volume reduction has yet to be defined, experience suggests that embolization of 50% to 70% of splenic volume has a balanced efficacy and complications risks. 4 In the present case, we attempted to embolized about 60% of the splenic volume, which resulted in a good response in platelet count.
PSE has been proved to be a safe and effective treatment to improve platelet counts in various disease conditions.4,5,9 In a retrospective analysis of 39 patients with chronic idiopathic thrombocytopenic purpura, authors have concluded that initial and repeated PSE can be an efficient alternative to splenectomy. 10 In their study, one year after the initial embolization, a complete response (platelet count > 100 000 /microL), a partial response (platelet count between 50 000 and 100 000 /microL), and no response were seen in 11 (28%), 9 (23%), and 19 (49%) of the patients, respectively. Peak platelet response had occurred between 3 and 30 days following the embolization procedure and platelet counts had started to decreased gradually after reaching the peak, in all of the patients. In another retrospective analysis of 13 patients, authors have shown that proximal splenic artery embolization can be an effective and safe treatment option for chemotherapy-induced thrombocytopenia, allowing systemic chemotherapy to be continued in these patients. 11 In their study, the peak platelet response had occurred between 7 and 91 days following the embolization procedure. Furthermore, PSE has long been proven to be an effective treatment option for improvement of thrombocytopenia in patients with liver cirrhosis.12,13 However, a thorough literature review did not reveal any report on the application of PSE for thrombocytopenia in a patient with APS. PSE appeared to be an ideal treatment for the present patient as it provided a rapid and sustained rise in platelet count and allowed resumption of the anticoagulation therapy.
For follow-up, we performed ultrasonographic examination of the spleen one day following the procedure that confirmed the successful embolization of about 60% percent of the splenic volume without any evident complication. Platelet count was also checked on a daily basis for 10 days. Regular platelet count checking was also recommended to be performed every 1 to 2 weeks for 2 months, and thereafter, every 1 to 2 months. The recurrence of thrombocytopenia during the follow-up period could warrant repeating the PSE. 14
Footnotes
Acknowledgments
The authors would like to thank you Dr. Nariman Nezami for his help writing and reviewing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved by our institutional review board (IRB) (IR.TBZMED.REC.1400.341).
Informed Consent
Informed written consent was obtained from the patient to publish the case, medical images, and the laboratory data. This study was approved by ethics committee of Tabriz University of Medical Sciences (Approval No. IR.TBZMED.REC.1400.341).