
Abstract
Objective
The clinical outcomes of this first-in-human (FIH) study provide safety and performance results 1 year after implantation of the VenoValve.
Background
Chronic venous insufficiency (CVI) is most often caused by valve failure in the venous system, which circulates blood from the lower limbs back to the heart and lungs. Severe diseases significantly influence quality of life, and current treatment options are limited. This study provides 1-year patient outcomes from 11 patients implanted with the VenoValve for treatment of severe deep venous CVI in C5 and C6 patients. Earlier results from 6-month follow-ups were previously published.
Methods
This prospective FIH study assessed the safety and performance of the VenoValve surgically implanted in 11 patients with C5 and C6 disease. All patients were followed up for at least 1 year. Assessments for adverse events, reflux time, disease severity, pain scores, and quality of life were reported.
Results
Implantation of VenoValve into the deep femoral vein was successful in all patients. Adverse events included 1 hematoma, 3 superficial wound infections, and 1 bleeding complication due to over-anticoagulation. One VenoValve became occluded due to patient non-compliance with anticoagulation medication. One-year clinical outcomes included significant decreases in mean reflux times (54%), and significant improvements in mean disease severity revised venous clinical severity score (56%), mean visual analog scale pain scores (76%), and Venous Insufficiency Epidemiologic and Economic Study QOL/sym scores.
Conclusions
The promising results from this FIH study demonstrate sustained safety and effectiveness of the VenoValve at 1 year post-implantation, and support further study for its use as a novel treatment for severe, deep venous CVI caused by valvular incompetence. A pivotal, prospective, non-blinded, single-arm, multi-center study in the United States with seventy-five (75) patients is in progress to assess the safety and effectiveness of VenoValve in these patients through 30 days and 6 months. The clinical trial is registered on ClinicalTrials.gov under identifier: NCT04943172 (https://clinicaltrials.gov/ct2/show/NCT04943172?term=hancock+jaffe&draw=2&rank=1).
Keywords
Introduction
Chronic venous disease (CVD) is one of the most prevalent chronic diseases worldwide. Global data from the International Vein Consult Program on CVD from 2012 reported that the worldwide prevalence of CVD was 83.6%, with 63.9% of subjects ranging from C1 to C6. These results included data from over 91 000 subjects across 20 countries. 1 In 2004, the National Venous Screening Program conducted the largest US study for detecting venous disease which included 2200 adults across 40 states. The study found that 71% of the subjects had some form of venous disease and that 40% had superficial or deep reflux in at least one vein segment. Of those with reflux, 53% had deep venous reflux and 47% had superficial reflux. 2 Based on today’s US population of approximately 210 million people aged 17 and older, an estimated 84 million people have chronic venous insufficiency (CVI) (40%). The prevalence of severe, deep venous reflux defined as C4 to C6 disease on the Clinical-Etiological-Anatomical-Pathophysiological (CEAP) classification in the US population is approximately 9.5 million people.
Chronic venous insufficiency is a large subset of CVD that afflicts millions of patients worldwide, and is caused by elevated pressure in the veins of the lower extremity (venous hypertension). Lower extremity edema, trophic skin changes, and severe discomfort are secondary to venous hypertension and can lead to diminished quality of life for patients with CVI and loss of work productivity. Chronic venous insufficiency is a progressive disease, and if left untreated, can lead to venous ulcers and a higher risk of deep vein thrombosis. Incompetent valves in the deep venous system of the lower limbs cause venous reflux, where blood flows in the wrong direction. Instead of blood returning to the heart and lungs, it pools in the lower leg and ankle, leading to increased venous pressure or venous hypertension within the venous system. Each year, approximately 150, 000 new patients are diagnosed with CVI. 3
Chronic venous insufficiency pathophysiology is generally attributed to 3 main causes: venous obstruction, poor pump function of the calf muscle, and valvular incompetency. Sufficient technologies exist for aid in revascularization of obstruction, which occurs in about 20% of CVI patients. Structured exercise regimens have been shown to improve calf muscle pump function and ejection fraction; however, calf dysfunction is rare in occurrence. 4 The treatment for severe, deep venous CVI due to valvular incompetency remains a challenging impediment for providing relief to these patients.
Superficial CVI and venous ulcers that result solely from superficial reflux may be treated with endovenous ablation therapies in combination with compression garments and wound care with varying degrees of success. However, the absence of a viable treatment for deep venous reflux has confounded clinicians for decades and has severely hampered treatment success for patients with deep venous reflux or those with a combination of superficial and deep venous reflux. 5 There are no effective or widely available devices to replace malfunctioning venous valves. To fill this void in treatment therapy, Hancock Jaffe Laboratories (now EnVVEno Medical Corporation) (Irvine, California) has developed VenoValve, a bioprosthetic porcine valve implant intended for use in patients with deep venous valvular insufficiency. The VenoValve is surgically implanted into the native femoral vein and provides a functional venous valve that reduces the reflux of blood in the lower extremity veins, thereby reducing venous pressure.
VenoValve is a porcine aortic monocuspid valve sewn onto a stainless-steel frame. The monocusp design allows the valve to open and close under the unique hemodynamic conditions that exist in the deep venous system. The combination of the unique monocusp design, together with properties of the native porcine non-aortic cusp tissue, the natural shape of the aortic root, and the stainless-steel frame, which mirrors the natural shape of the porcine aortic root, all contribute to the anti-thrombogenic properties of VenoValve (Figure 1). Hancock Jaffe VenoValve.
The VenoValve is designed to prevent or reduce reflux (the backflow or regurgitative volume of blood) into the lower extremity deep venous system, thereby reducing elevated venous pressure that is seen in the diseased lower extremity. A first-in-human clinical trial with the VenoValve was conducted, and 1-year clinical outcomes from this trial are reported. By providing a relative decrease in venous hypertension, the VenoValve results in marked improvements for patients with severe CVI. A prior manuscript presenting 6-month data from this trial has been published in the Journal of Vascular Surgery. 6
Methods
This FIH trial was a non-randomized, single-center, prospective study. The study enrolled 11 patients with severe deep venous CVI (C5 and C6 disease patients). Concomitant disease of deep venous CVI with superficial reflux was noted in 9 of these patients. In these cases, ablation of the superficial system and injection therapy of perforators was performed at least 6 weeks prior to the procedure. If symptoms persisted or there was no improvement in their ulceration, these patients were enrolled into the study.
The study was conducted at the University Hospital, Cirulaser Andes S.A. in Colombia, South America, with the principal investigator, Dr Jorge Ulloa, under the approval of the local ethics committee and Colombia National Food and Drug Surveillance Institute (INVIMA) (see INVIMA file number 20152610 for approval). Written informed consent was obtained from all study participants before any study-specific procedures or assessments were performed and prior to the patients being treated with the device.
In total, 11 patients were implanted with VenoValve and followed up for at least 1 year. The study endpoints included assessments for reflux time, revised venous clinical severity score (rVCSS) (clinical assessment of the leg for venous disease), Venous Insufficiency Epidemiologic and Economic Study (VEINES) QOL score (a questionnaire comprising 25 items that quantify disease effect on quality of life in patients with venous disorders), a symptoms questionnaire (VEINES Sym), and visual analog scale (VAS) score for assessment of pain levels. The first implant occurred on February 6, 2019, and the last implant occurred on December 11, 2019. Data for the study were collected in December 2020.
Reflux in the deep system in all patients was noted throughout the common femoral vein, femoral vein, and popliteal vein. Reflux values were noted at all levels and recorded preoperatively as well as post-operatively at defined intervals of 24-h, 14-day, 30-day, 90-day, 160-day, and 6-month intervals post-implantation. Planar x-ray imaging was conducted at 1 year to evaluate valve positioning.
Implant of the device was performed with an open surgical procedure, with the device being placed in the femoral vein in the upper thigh region. Ten patients had placement of the device under regional anesthesia and 1 under local anesthesia. The device was tacked to the native femoral vein with a monofilament suture to prevent any migration of the device. Patients were heparinized during surgery with 5000 units, and during 2 weeks of the postoperative period, patients were treated with low molecular weight heparin at 1 mg/kg/bid. Eight patients were switched to Coumadin anticoagulation, and 3 patients were switched to a direct oral anticoagulant. Patients were anticoagulated for the duration of this study with an oral agent. No antiplatelet medications were prescribed. After the implantation procedure, half of the patients were discharged shortly after ambulating and the other half were admitted for a 23-hour stay. All patients were discharged with compression stockings.
Results
Patient Demographics.
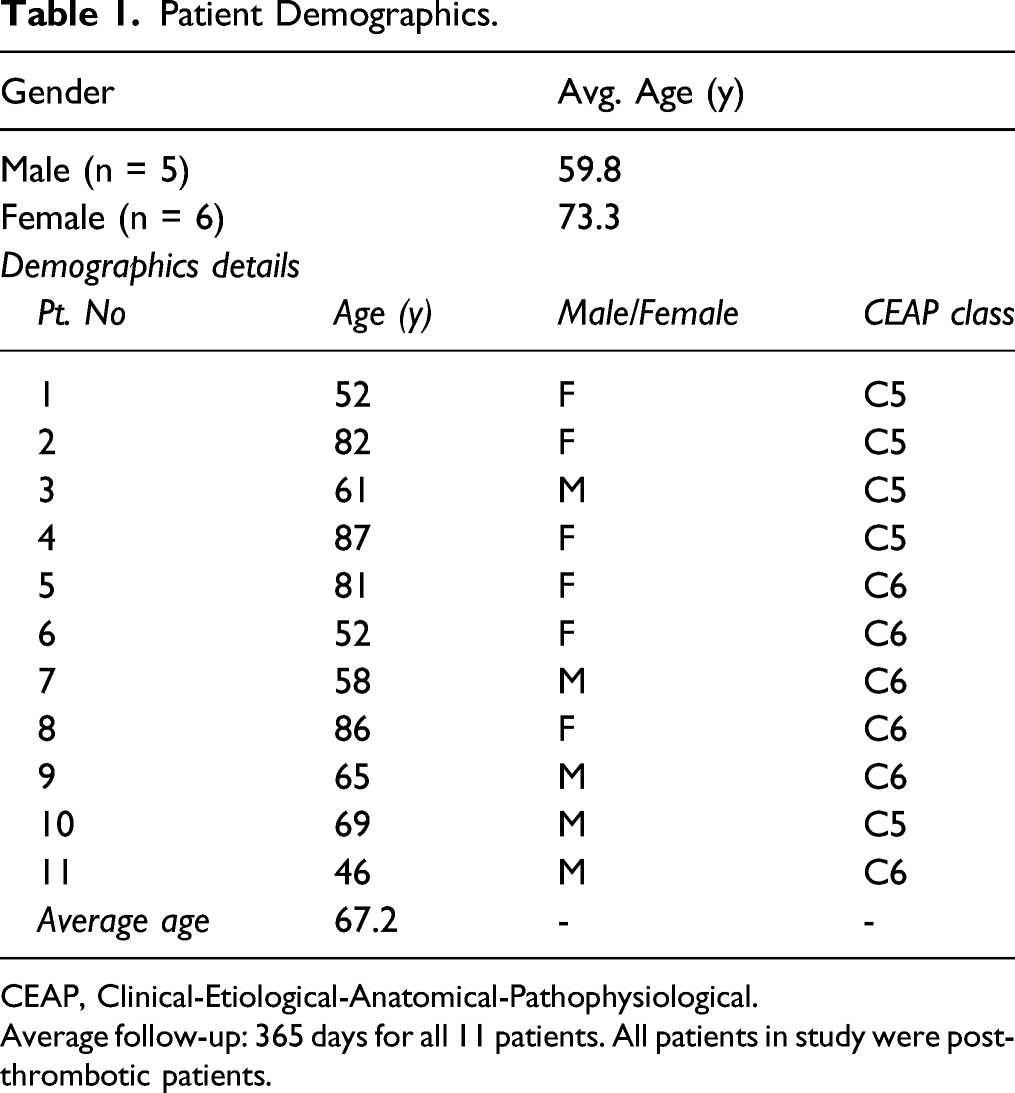
CEAP, Clinical-Etiological-Anatomical-Pathophysiological.
Average follow-up: 365 days for all 11 patients. All patients in study were post-thrombotic patients.
Performance Results
One-Year Post-Implantation Results.
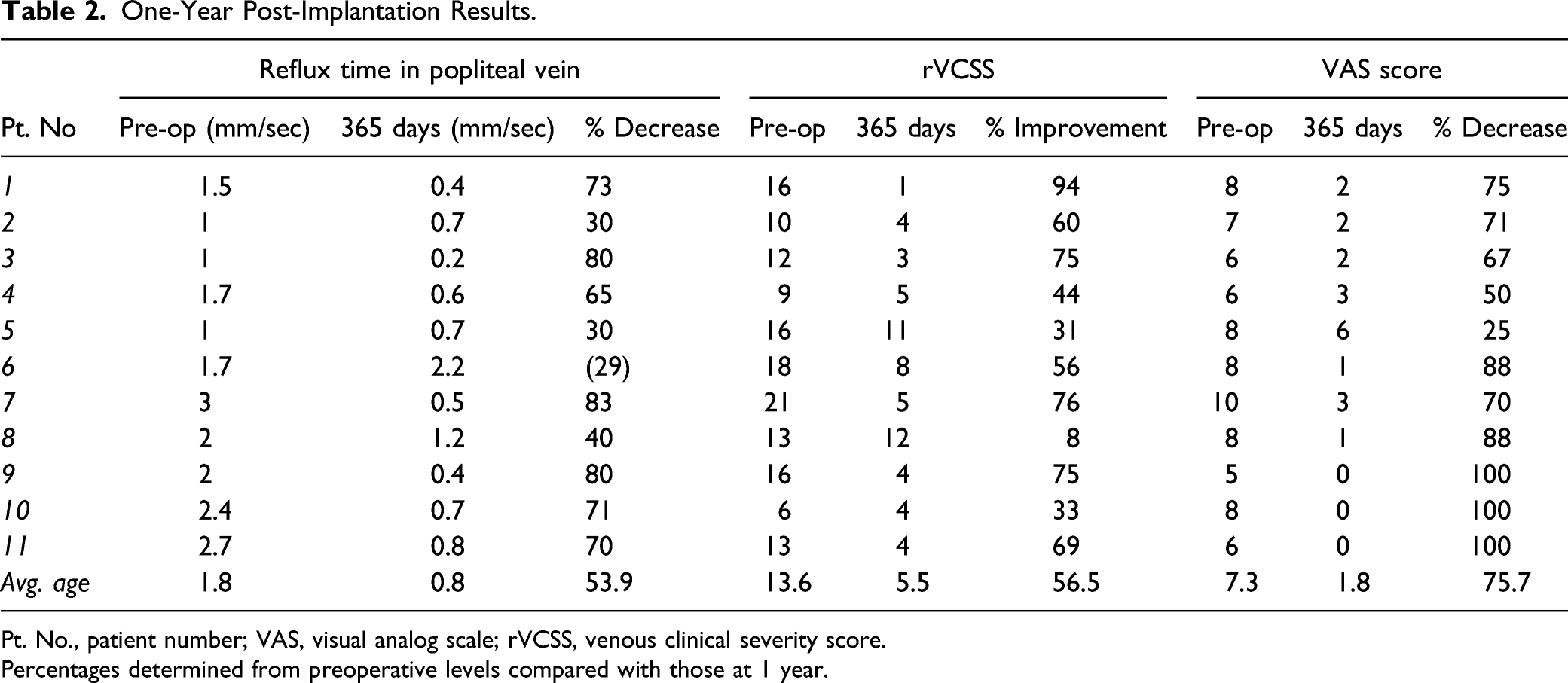
Pt. No., patient number; VAS, visual analog scale; rVCSS, venous clinical severity score.
Percentages determined from preoperative levels compared with those at 1 year.
Reflux times were measured at baseline (pre-valve implantation), and at 30, 60, 90, 180, and 365 days post-valve implantation for all 11 patients (Figure 2). One-year outcomes for reflux times.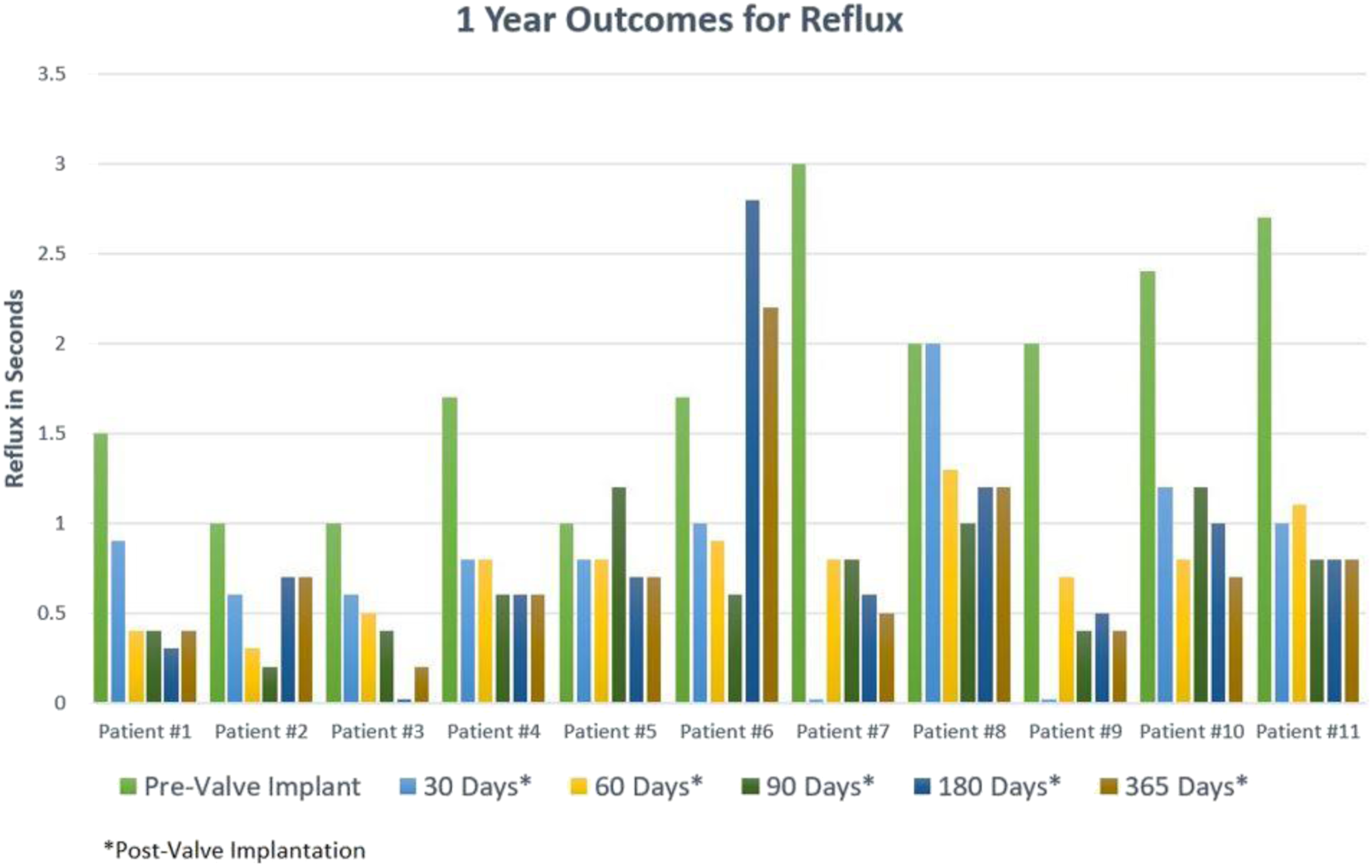
Disease severity was measured at baseline and at 30, 60, 90, 180, and 365 days post-valve implantation for all 11 patients. Improvement in rVCSS was recorded for all 11 patients from preoperative levels through 1-year follow-up, with an improvement of 8.09 points, 56.5% at 1 year (Figure 3). One-year outcomes for disease severity (rVCSS). (3A) rVCSS scores for patients over 1 year and (3B) rVCSS percent improvement over time with VenoValve (VV). rVCSS, revised venous clinical severity score.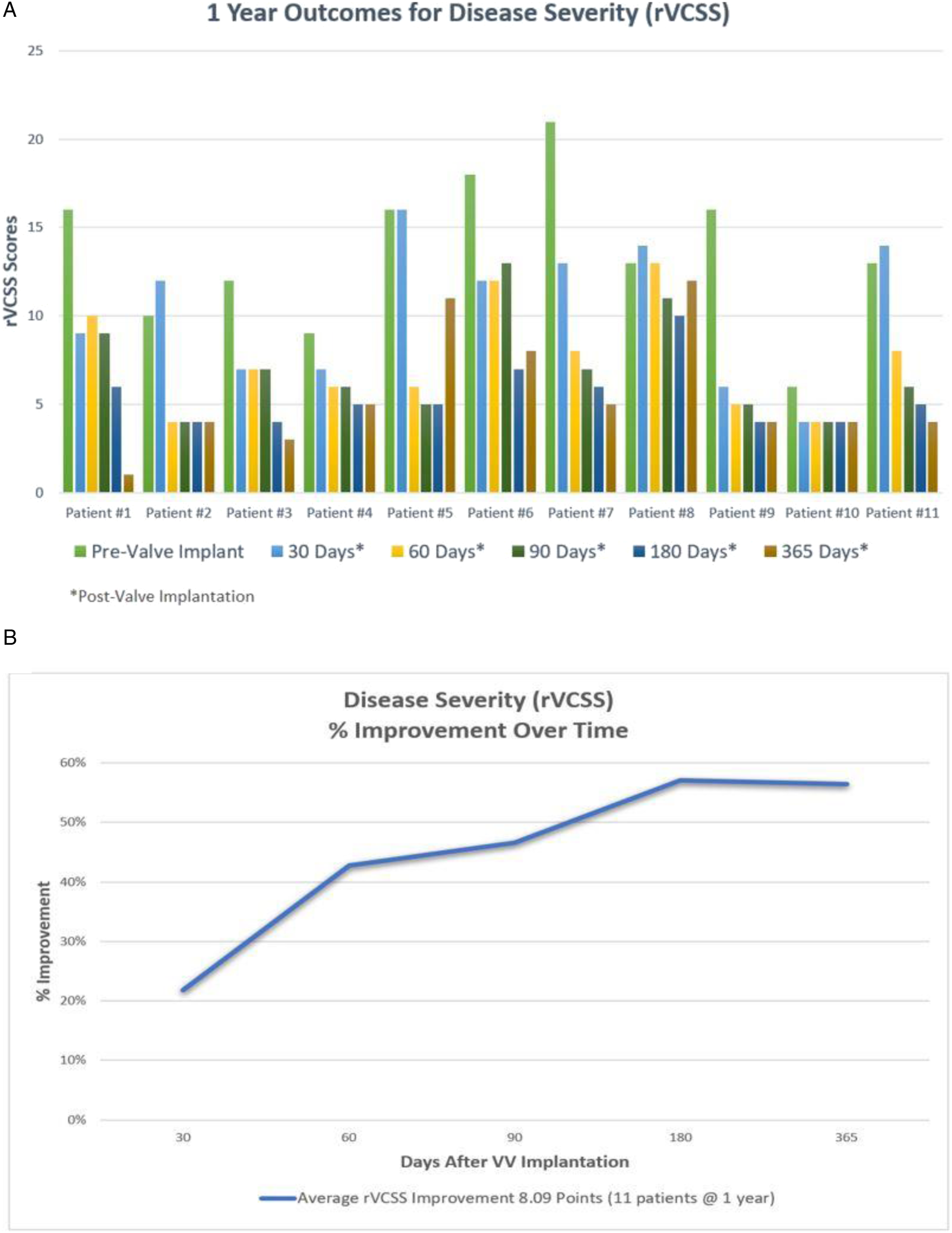
Visual analog scale scores for pain levels were measured at baseline and at 30, 60, 90, 180, and 365 days post-valve implantation for all 11 patients. Overall improvement in pain scores was recorded for all 11 patients, with an average improvement of 75.7% from preoperative levels to 1 year (Figure 4). One-year outcomes for visual analog scale.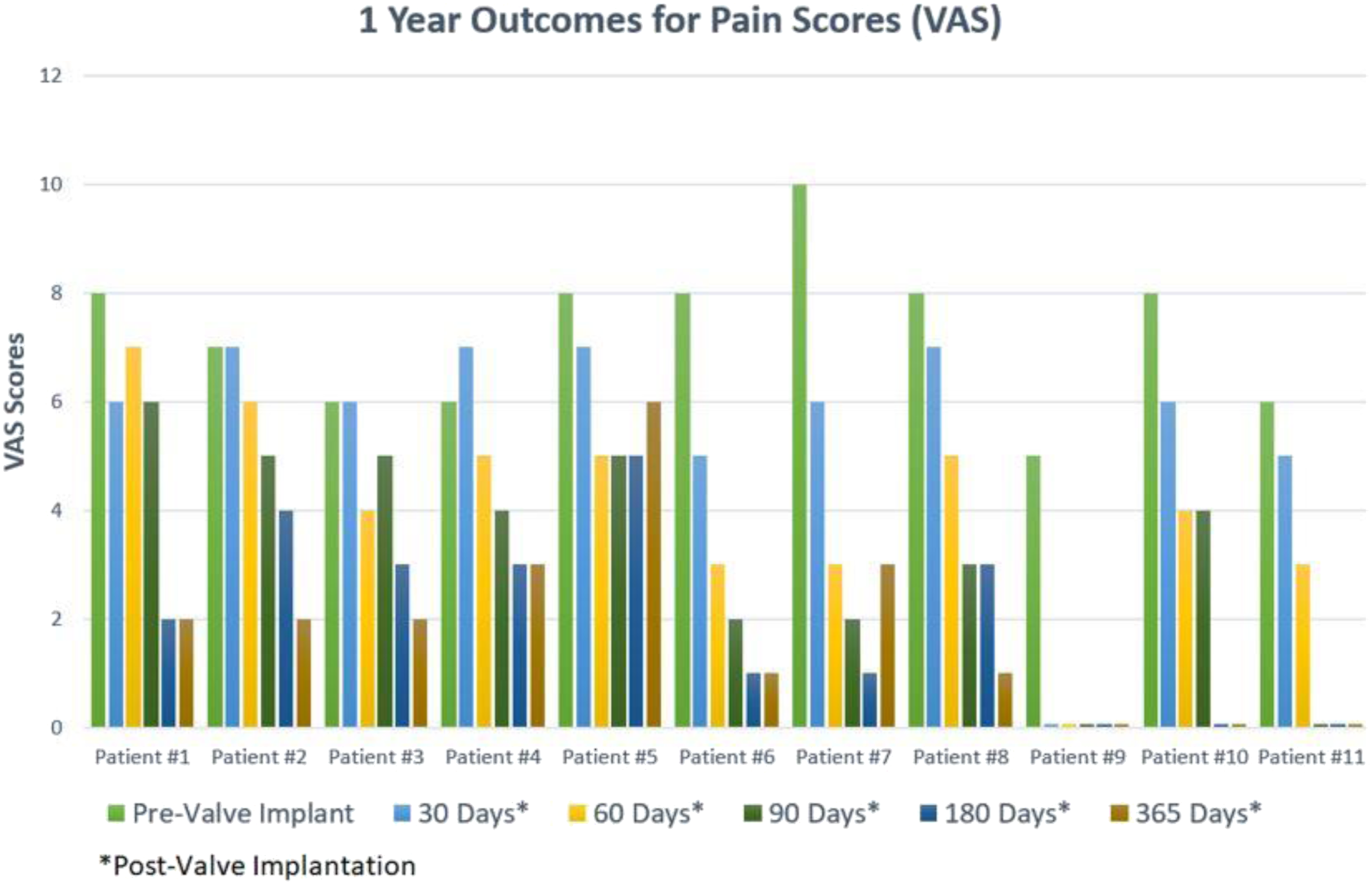
VEINES Quality of Life/Symptom Scores at 1 Year.
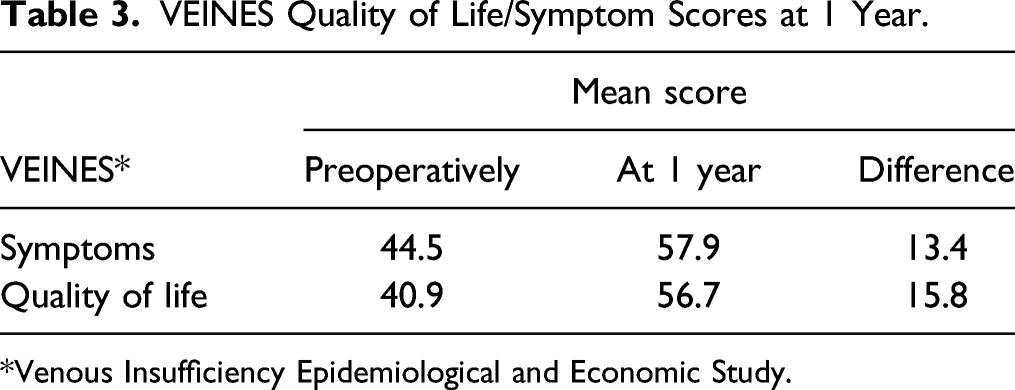
*Venous Insufficiency Epidemiological and Economic Study.
Safety Results
Adverse events included 1 patient who experienced occlusion of the VenoValve due to non-compliance with anticoagulation medication after 90 days. The reflux time for this patient returned to the pre-operative levels at 6 months. However, decreases in both disease manifestation and pain were reported as this patient experienced significant venous ulcer healing prior to the event. Other adverse events included 1 hematoma at the incision site that was aspirated, 1 bleeding complication in a patient who developed Coumadin incompatibility, and 3 superficial wound infections in C6 patients that were treated with antibiotics. These ulcer infections were already present prior to implantation and were not caused by the procedure or device. Two of these patients required hospitalization due to underlying comorbid medical conditions.
Discussion
The prevalence of patients with venous disease is high, and currently available medical treatment options for patients with severe deep venous CVI are very limited. The VenoValve is the first prosthetic valve for treating CVI and has shown clinical success at the 1-year follow-up. The 1-year results from this study demonstrated significant improvement in the care of patients with severe CVI. A few safety issues were noted in this study. All adverse events were nondevice-related and occurred within 4 months of the implantation procedure. There was no recurrence of ulcers in this study during the 1-year follow-up. Although this was not a wound assessment study, marked improvement and wound healing were noted in all patients.
This publication is a follow-up to the previous report published in the Journal of Vascular Surgery providing the 6-month results for these patients. 6 One-year follow-up of these patients presented in this publication demonstrates continued improvement. At 1 year, the objective clinical outcomes included measured improvements in reflux times and disease severity. These measured clinical outcomes include an 8-point improvement, which reclassifies patient diagnosis from severe disease to mild disease. In addition, subjective improvements noted by the patients included significant improvements in their quality of life, as well as a marked reduction in their perceived pain. The results from this FIH trial provide sustained evidence of clinical safety and device performance for use of the VenoValve as a possible novel treatment for patients with CVI.
As the small sample size is a limitation of the study, more studies with a larger number of patients are needed to further support the implantation of the VenoValve as a standard surgical treatment for deep venous system reflux. Hancock Jaffe Laboratories is currently conducting a larger pivotal clinical study, the Hancock Jaffe Surgical Anti-Reflux Venous Valve Endoprosthesis Study, with 75 patients enrolled at up to 20 investigational sites in the US under an investigational device exemption approval by the US Food and Drug Administration (clinical trial identifier: NCT04943172). The VenoValve may be a significant milestone for patients with CVI, as this device provides a possible solution to this complex group of patients.
Footnotes
Acknowledgments
We would like to thank Carolyn McCuan of CTM Medical Consulting for her contribution to the writing and technical assistance of this manuscript, and for the development of the tables and figures.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Ulloa is the principal investigator of this study and a vascular surgeon with Fundacion Santa Fe de Bogota (Bogota, Colombia). Dr Glickman is an executive at Hancock Jaffe Laboratories. Dr Ulloa and Dr Glickman are working under a grant from Hancock Jaffe. Funding was not received from any other source.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Hancock Jaffe Laboratories.