
Abstract
Background
Weekend effect characterized by worse perioperative outcomes has been demonstrated in some surgery patients admitted on weekends, as opposed to weekdays. This study aimed to examine weekend effect on open surgical repair or thoracic endovascular aneurysm repair (TEVAR) for Stanford Type B Aortic Dissection (TBAD).
Methods
Patients who underwent TBAD repair were identified in National/Nationwisde Inpatient Sample from Q4 2015-2020. Open surgery and TEVAR were examined separately. Multivariable analyses were performed comparing in-hospital perioperative outcomes of patients under weekday and weekend admission. Adjusted preoperative variables included sex, age, race, socioeconomic status, hospital characteristics, clinical symptoms, comorbidities, and elective/non-elective admission. Also, length of stay, days from admission to operation, and total hospital charge were compared.
Results
Among patients who underwent open TBAD repair, 1321 were admitted on weekdays and 340 on weekends. Among patients who underwent TEVAR for TBAD, 2018 were admitted on weekdays and 440 wereadmitted on weekends. There was no difference in open repair outcomes between those admitted on weekdays vs weekends. In TEVAR, weekend admission was associated with higher post-procedural kidney failure (1.14% vs .20%, aOR = 4.11, P = .04) and superficial wound complications (2.73% vs 1.49%, aOR = 2.2, P = .03) but lower respiratory complications (5.80% vs 3.64%, aOR = .47, P = .01). Also, in TEVAR, weekend admission was associated with longer time from admission to operation (3.92 ± .27 vs 2.35 ± .09 days, P < .01).
Conclusions
Renal malperfusion was a common indication for TBAD repair. TBAD patients admitted over the weekend and underwent TEVAR had higher post-procedural kidney failure, which may be due to delayed diagnosis and treatment.
Introduction
Aortic dissection is broadly classified into Stanford Type A (TAAD) or Type B (TBAD) based on the relationship of the dissection to the origin of the brachiocephalic artery. TAAD involves the ascending aorta or aortic arch including the brachiocephalic artery. 1 TAAD often necessitates immediate open surgical intervention due to the risk of complications and is generally associated with a worse prognosis due to the proximity to the coronary and cerebral arteries.2,3 In contrast, TBAD involves the descending aorta distal to the origin of the brachiocephalic artery. 4 Historically, the initial management of TBAD was non-operative, medical treatment unless complications developed, such as rapid aortic expansion, rupture, or malperfusion syndrome. In TBAD, two surgical approaches can be considered: open repair and thoracic endovascular aortic repair (TEVAR). Open surgical repair performed through a left thoracoabdominal incision is highly morbid, while TEVAR has gained favor as a less invasive procedure indicated for acute TBAD with rupture or malperfusion,5,6 as well as uncomplicated TBAD.7,8 The choice of open repair vs TEVAR is determined based on surgeon and center expertise, as well as individual patient characteristics and the extent of the dissection. 9
The weekend effect in surgery refers to the observed elevated risk of worse perioperative outcomes among patients who are admitted on weekends, as opposed to weekdays, underscoring the potential for suboptimal treatment outcomes during weekend surgeries.10-13 The weekend effect may be caused by a reduction in staffing, less experienced personnel, and limited availability of certain procedures during off-peak hours. 14 Worse outcomes with weekend admission may also be attributable to delay of surgery until the following week. Numerous studies investigating the weekend effect on acute aortic dissection have demonstrated a significant association between cases admitted during weekends and a higher mortality rate.15-17 However, TAAD and TBAD are distinct conditions with distinct clinical courses and varying management strategies. Only a few studies have taken these differences into account when examining the weekend effect. While many studies have investigated the weekend effect on mortality rates for TAAD, the impact of this phenomenon on TBAD remains less studied.18-20 In one study that examined the weekend effect in TBAD, it was discovered that weekend admission of TBAD patients is linked to increased mortality rates. 19 As TBAD treatment modalities, such as open repair and TEVAR, involve different patient selection criteria and management strategies, it is critical to consider these surgical approaches separately when analyzing the impact of weekend admission on outcomes after TBAD repair.
The object of this study was to explore the weekend effect in patients who undergo either open surgical repair or TEVAR for TBAD, comparing those admitted on weekends with those admitted on weekdays. This study aimed to examine postoperative outcomes, as well as the hospital stays and related costs that are associated with weekend admission. This investigation may yield significant insights into how weekend hospital admissions might influence the management and outcomes of TBAD patients undergoing surgical interventions.
Materials and Methods
Data Source
Patients who underwent TBAD repair were identified in the National/Nationwide Inpatient Sample (NIS) from the last quarter of 2015-2020. Patients who were diagnosed with aortic dissection were identified using International Classification of Diseases, 10th Revision, Clinical Modification (ICD10-CM) of I71.01, I71.03. Then, patients who underwent open surgery and TEVAR for TBAD were further identified by International Classification of Diseases, 10th Revision, Procedure Coding System (ICD-10-PCS) (open repair: 02QW0ZZ, 02RW07Z, 02RW08Z, 02RW0JZ, 02RW0KZ, 02UW08Z, 02UW0JZ, 02UW07Z,02UW0KZ, 02BW0ZZ; TEVAR: 02QW3ZZ, 02QW4ZZ, 02HW3DZ, 02UW3JZ, 02VW3DZ, 02VW3EZ, 02VW3FZ, 02VW3ZZ, 02VW4CZ, 02VW4DZ, 02VW4EZ, 02VW4FZ, 02VW4ZZ). Patients under the age of 18 were excluded. Patients were stratified into 2 cohorts based on weekday or weekend admission as documented in the NIS database.
Preoperative Variables
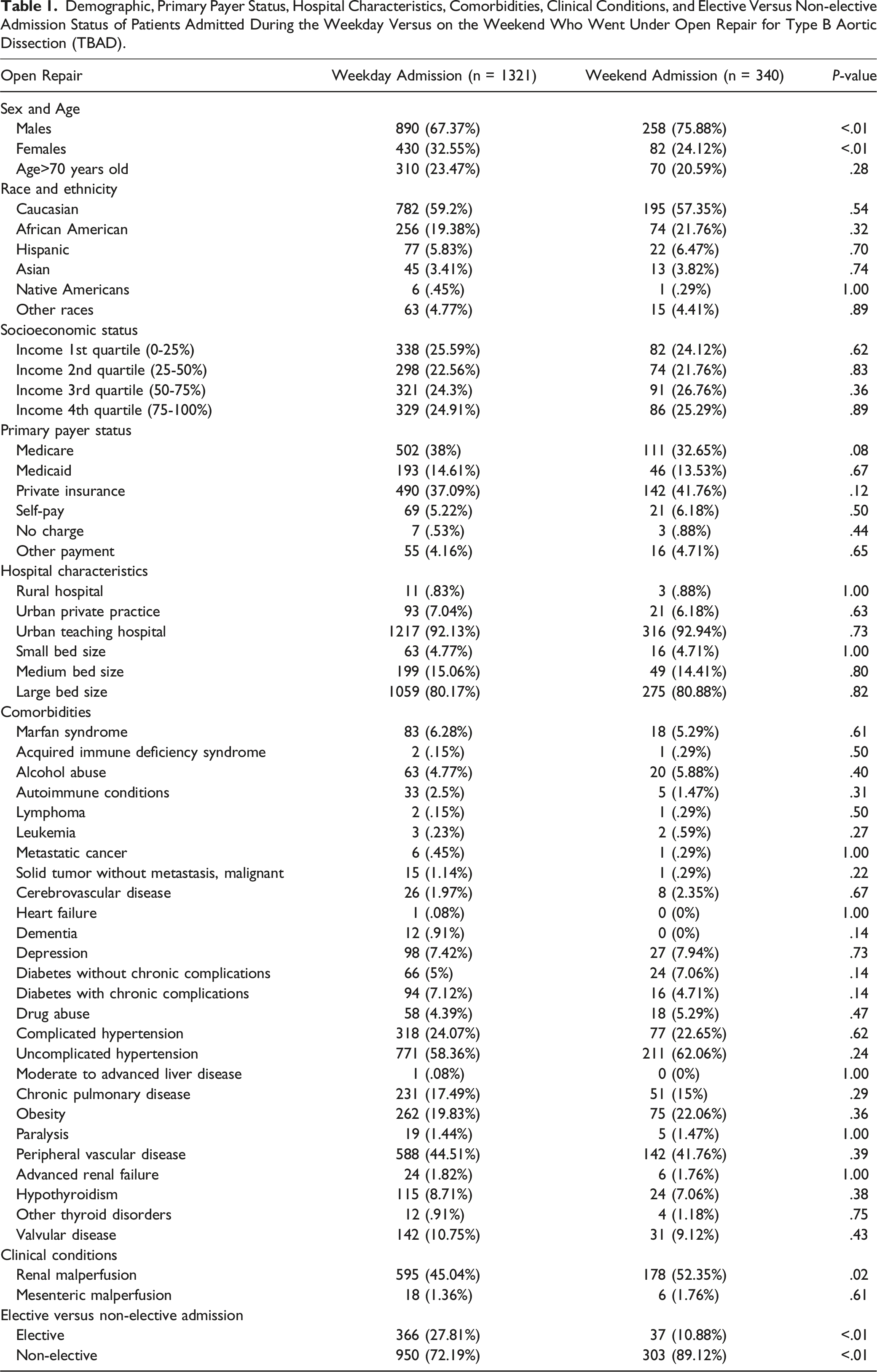
Demographic, Primary Payer Status, Hospital Characteristics, Comorbidities, Clinical Conditions, and Elective Versus Non-elective Admission Status of Patients Admitted During the Weekday Versus on the Weekend Who Went Under Open Repair for Type B Aortic Dissection (TBAD).
Demographic, Primary Payer Status, Hospital Characteristics, Comorbidities, Clinical Symptoms, and Elective Versus Non-elective Admission Status of Patients Admitted During the Weekday Versus on the Weekend Who Went Under Thoracic Endovascular Aortic Repair (TEVAR) for Type B Aortic Dissection (TBAD).
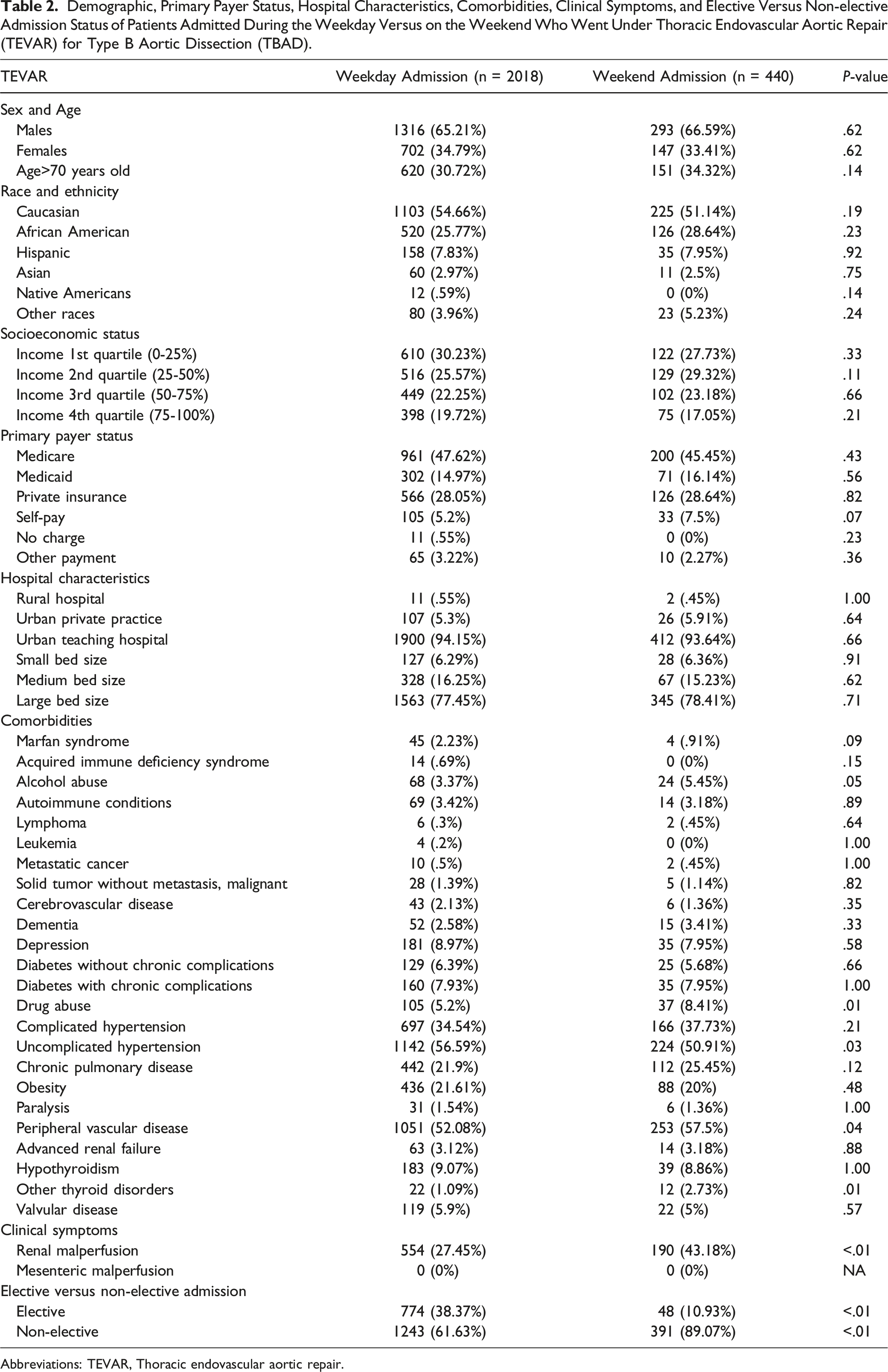
Abbreviations: TEVAR, Thoracic endovascular aortic repair.
Perioperative Values
Perioperative outcomes included mortality, myocardial infarction (MI), stroke, respiratory complications, post-procedural renal failure, superficial wound complication, deep wound complication, shock, bleeding, pulmonary embolism (PE), venous thromboembolism (VTE), and transfer out to other hospital facilities. The ICD10-CM codes for the outcomes are summarized in Table S1. The perioperative outcomes were compared between patients admitted on weekdays and weekends. In addition, time from admission to operation, hospital length of stay (LOS), and total hospital charge were compared. It is important to note that the NIS database does not include data regarding patient follow-up after discharge. As a result, all observed perioperative outcomes are entirely based on in-hospital documentation.
Statistical Analysis
Fisher's exact test was used to compare categorical preoperative variables for patients who were admitted on weekdays and weekends. Post-operative outcomes were also compared between these 2 groups. For the binary post-operative outcomes, multivariable logistic regression was employed for comparison, adjusting for preoperative variables that showed adequate differences (P < .1) by Fisher's exact test. Adjusted odds ratios (aORs) and 95% confidence intervals (CI) were calculated. Continuous variables, including time from admission to operation, LOS, and total hospital charge, were examined using a generalized linear model (GLM), adjusting for all preoperative variables. All statistical analyses were conducted using SAS (version 9.4). A P-value <.05 was defined as statistically significant. The authors were given full access to the data and bore the responsibility of preserving the accuracy of the analysis. As the study involved a review of retrospective and anonymized data from the NIS, it received an exemption from the requirement for approval from the Institutional Review Board (IRB) at The George Washington University.
Results
Among patients who underwent open TBAD repair, 1321 were admitted on weekdays and 340 on weekends. Among patients who underwent TEVAR after TBAD, there were 2018 admitted on weekdays and 440 admitted on weekends.
Demographics, primary payer status, hospital characteristics, comorbidities, clinical symptoms, and elective vs non-elective admission status of patients admitted during the weekday vs on the weekend who went under open repair for TBAD are summarized in Table 1. Compared to weekday patients, weekend patients were more likely to be male (75.88% vs 67.37%, P < .01), have renal malperfusion (52.35% vs 45.04%, P = .02), and under non-elective admission (89.12% vs 72.19%, P < .01). There was no difference in all other variables in open surgery.
For patients with TBAD who went under TEVAR, demographics, primary payer status, and hospital characteristics of patients admitted during the weekday vs on the weekend are summarized in Table 2. There was no difference in these variables between the 2 cohorts. Comorbidities and clinical symptoms of these patients are also summarized in Table 2. Weekend TEVAR patients had more alcohol abuse (5.45% vs 3.37%, P = .05), drug abuse (8.41% vs 5.2%, P = .01), peripheral vascular disease (57.5% vs 52.08%, P = .04), other thyroid disorders (2.73% vs 1.09%, P = .01), renal malperfusion (43.18% vs 27.45%, P < .01) compared to the weekday TEVAR patients. On the other hand, there were fewer weekend TEVAR patients who had uncomplicated hypertension (50.91% vs 56.59%, P = .03). In addition, weekend patients were more likely to under non-elective admission among weekend patients (89.07% vs 61.63%, P < .01).
In-Hospital Outcomes of Patients Who Were Under Weekday Versus Weekend Admission in Open Repair for Type B Aortic Dissection (TBAD) Compared by Multivariable Logistic Regression.
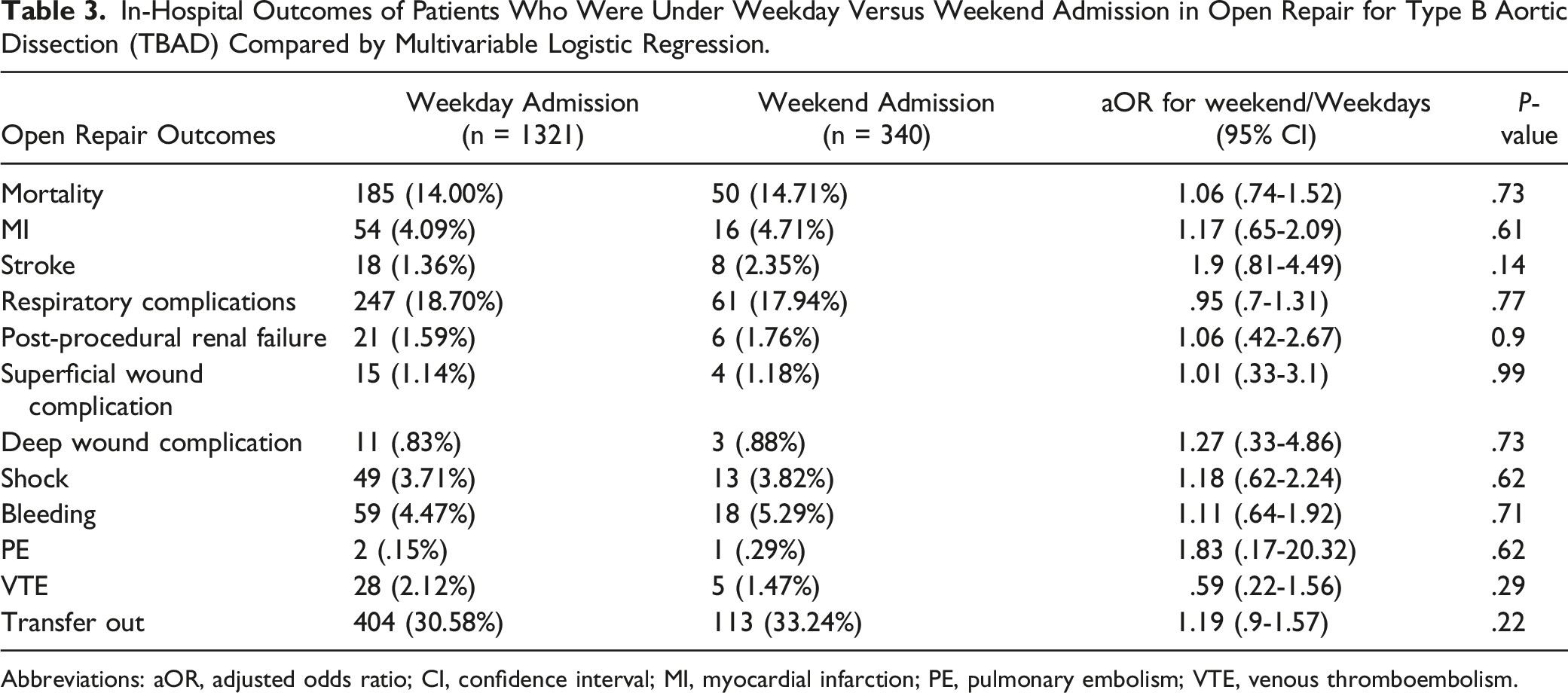
Abbreviations: aOR, adjusted odds ratio; CI, confidence interval; MI, myocardial infarction; PE, pulmonary embolism; VTE, venous thromboembolism.
Generalized Linear Model (GLM) Comparing Time From Admission to Operation, Length of Stay (LOS), and Total Hospital Charge in Patients Admitted During the Weekday Versus on the Weekend Who Underwent Open Surgery for Type B Aortic Dissection (TBAD). Mean and Standard Error (SE) are Shown.
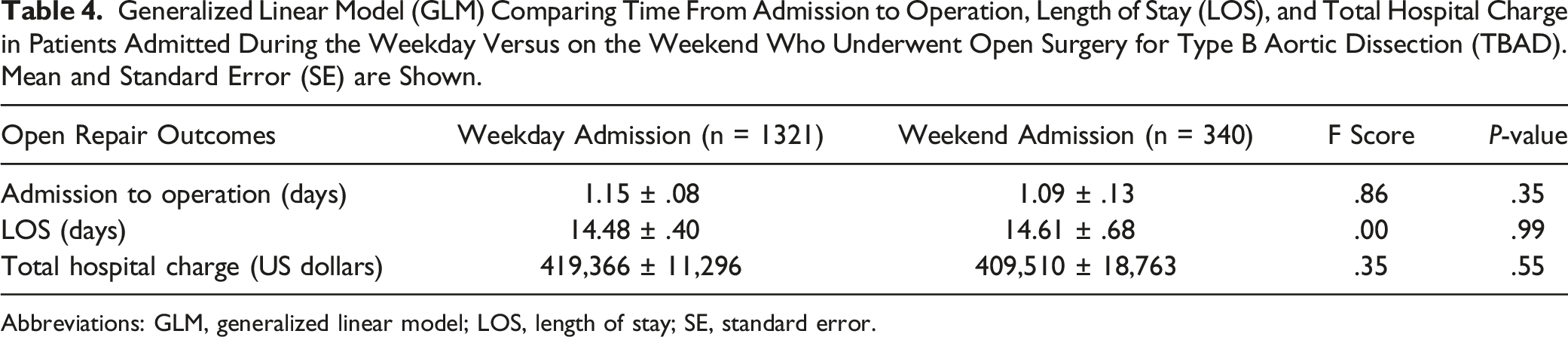
Abbreviations: GLM, generalized linear model; LOS, length of stay; SE, standard error.
In-Hospital Outcomes of Patients Who Were Under Weekday Versus Weekend Admission in Thoracic Endovascular Aortic Repair (TEVAR) for Type B Aortic Dissection (TBAD) Compared by Multivariable Logistic Regression.
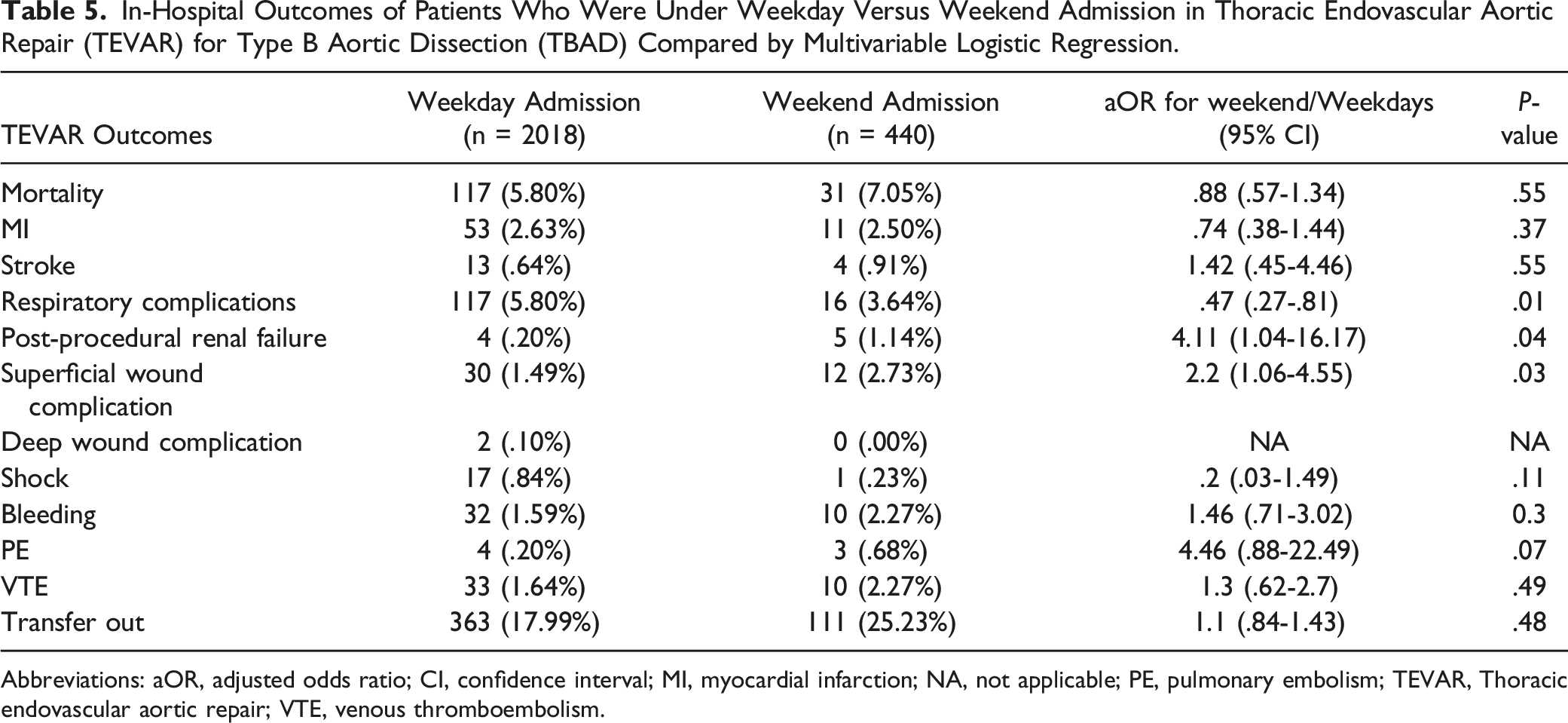
Abbreviations: aOR, adjusted odds ratio; CI, confidence interval; MI, myocardial infarction; NA, not applicable; PE, pulmonary embolism; TEVAR, Thoracic endovascular aortic repair; VTE, venous thromboembolism.
Generalized Linear Model (GLM) Comparing Time From Admission to Operation, Length of Stay (LOS), and Total Hospital Charge in Patients Admitted During the Weekday Versus on the Weekend Who Underwent Thoracic Endovascular Aortic Repair (TEVAR) for Type B Aortic Dissection (TBAD). Mean and Standard Error (SE) are Shown.
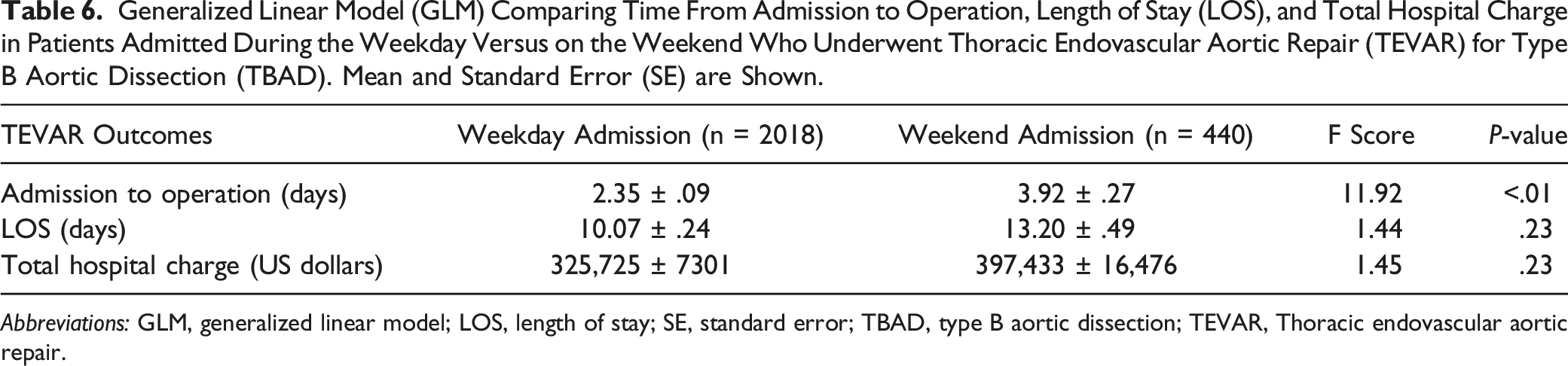
Abbreviations: GLM, generalized linear model; LOS, length of stay; SE, standard error; TBAD, type B aortic dissection; TEVAR, Thoracic endovascular aortic repair.
Discussion
This study examined the weekend admission effect on outcomes after open surgical repair or TEVAR in TBAD. There was no significant difference in open repair outcomes between weekday and weekend patients. However, in TABD patients treated with TEVAR, weekend admission was associated with higher post-procedural kidney failure and superficial wound complications but lower respiratory complications, as well as longer time from admission to operation.
In open repair for TBAD, there was no discernible difference in post-surgical mortality and morbidity, patient transfers to other hospital facilities, LOS, time until operation, or costs between patients admitted during weekdays compared to those admitted over the weekend. Open repair is typically reserved for more complex and severe TBAD cases, although surgeon and center expertise may also be a factor in some instances. In the present study, the time from admission to operation for open repair (weekday 1.15 ± .08 days, weekend 1.09 ± .13 days) was shorter than TEVAR (weekday 2.35 ± .09 days, weekend 3.92 ± .27 days) where no delay on the weekend was observed, suggesting that open repair was used in truly emergent cases that could not wait for repair. This suggests that patients who require open repair for TBAD are more likely to present with emergent conditions. Surgical procedures of an urgent nature tend not to be impacted by the weekend effect, mainly because they demand immediate attention, regardless of the day. Previous studies found that mortality rates for elective surgery patients were higher for those who had procedures later in the week and on weekends; however, this pattern was not observed for emergency surgeries.22,23 This suggests that the weekend effect might be less prominent in emergency procedures. The immediacy of these procedures requires hospitals to ensure a uniform standard of care throughout the week to effectively address life-threatening situations. Conversely, TEVAR procedures for TBAD tend to be less urgent compared to open repairs. The observation of a longer time until operation for TEVAR patients admitted on weekends aligns with this reasoning.
The findings for open repair in TBAD align with those observed in previous studies on TAAD, where no differences were found in postoperative mortality rates between patients admitted during weekdays and those admitted over the weekend.18,19 Additionally, for TAAD, patients admitted over the weekend did not experience a longer time until operation, a finding consistent with TBAD open repair cases where no delays were reported in this study. 19 Given that TAAD often manifests as an emergency requiring immediate open surgical intervention, the similar results across these 2 types of aortic dissection support the assertion that the weekend effect is less prominent in urgent, complex cases of aortic surgery.
Regarding the weekend effect on surgical complications in TBAD, earlier research mainly concentrated on mortality rates. 19 In the study by Altujjar et al, researchers found that weekend admissions of TBAD patients correlated with elevated mortality rates. However, their study did not differentiate between open and TEVAR approaches for TBAD repair. In our findings, where mortality rates for open repairs were equivalent for both weekdays (14.00%) and weekends (14.71%), and higher for TEVAR on weekends (weekday 5.80%, weekend 7.05%, although this did not meet the threshold for significance), we suspect that the elevated mortality in the weekend cohort from Altujjar’s study was likely contributed by TEVAR cases.
A key strength of this study lies in its detailed examination of major morbidities following both open repair and TEVAR for TBAD. In terms of morbidity, the study found no distinction between weekday and weekend admissions for open repairs of TBAD. This finding further reinforces the absence of observable weekend effects in the open cases. For TBAD, higher incidence of post-procedural of kidney failure (N99.0) has been observed in TEVAR patients admitted during the weekend after correcting for all pre-operative differences including higher renal malperfusion and non-elective admission in weekend patients.
Evaluating renal complications in TBAD patients is crucial. A notable proportion of those undergoing TBAD repair exhibit clinical symptoms of renal malperfusion. This includes roughly half of the patients who undergo open repair and one-third of those treated with TEVAR. This study highlights a concerning pattern of heightened of kidney failure during weekend admissions for TEVAR in TBAD. Post-operative renal complications have a strong association with long-term detrimental outcomes, such as the development of chronic kidney disease (CKD), cardiovascular disease, and mortality, which has a significant health care burden. 24 Therefore, it is crucial to address the association between weekend admission and a higher incidence of kidney failure in TEVAR.
The elevated observation of kidney failure in TEVAR for TBAD during weekend admissions may be associated with delays in diagnosis and treatment. Health care centers typically run with a decreased number of staff members over weekends, potentially affecting patient care quality; this reduction in personnel might contribute to longer reaction times during urgent situations or sporadic patient monitoring. 11 Also, diagnostic imaging or laboratory tests, including computerized tomography (CT), magnetic resonance angiogram (MRA), and CT angiography (CTA), could experience longer processing times during weekends that could potentially slow down the diagnostic or treatment processes. 10 This is confirmed by findings from this study, which noted an association between weekend admissions and longer time from admission to operation in the TEVAR cohort. The unique requirements of TEVAR, such as the use of contrast agents, can put additional strain on the kidneys and increase the risk of renal complications. Renal complications that occur post-surgery can manifest in a subtle manner where prompt diagnosis may be challenging. 24 Thus, any delays in diagnosis or intervention, which could be more likely over the weekend, can lead to an increased risk of renal complications.
Furthermore, patients who underwent TEVAR for TBAD exhibited a heightened risk of superficial wound complications. Possible contributing factors might include the expertise of the medical staff performing the procedure during weekend or disparities in post-operative care in weekend patients. The observed lower incidence of respiratory complications in patients who underwent TEVAR over the weekend requires further investigation, as the underlying cause remains unclear. However, considering the low number of such incidences, this finding could be merely incidental.
It is important to note that there was a higher number of non-elective admissions for TBAD repair over the weekend. Moreover, among TEVAR patients admitted on weekends, there was an increased prevalence of alcohol and drug abuse and peripheral vascular disease, but a reduced uncomplicated hypertension. Although these factors were accounted for in the multivariable analysis, such evidence might imply that patients admitted on weekends and weekdays represent distinct groups with differing social backgrounds. The potential biases of providers influenced by patients' social situations (eg, substance abuse) and patients’ compliance might not be entirely addressed in the analysis and could play a role in the observed disparities.
This research, while valuable, acknowledges several key limitations. The NIS, as the largest in-patient database in the US, relies predominantly on the ICD coding system. As a result, it does not capture comprehensive patient assessment and management details, such as the extent and location of the dissection, symptom onset, procedural methods, the type of graft used, the extent of the repair, and circulatory arrest time. Furthermore, the database only tracks outcomes occurring during the hospital stay and does not provide post-discharge follow-up data. Consequently, assessing the long-term prognosis following TBAD repair is beyond its scope. Additionally, the database indicates weekend admission status as a binary variable and the duration from admission to operation. Thus, it does not allow the calculation of whether the procedure occurred over the weekend or on a weekday in the subsequent week. Outcomes could be influenced by weekend operations, given that the operating room availability and equipment as well as the expertise of the staff might vary and thereby impact the results.
Despite these constraints, NIS is the largest all-payer database in the US and records data from approximately 20% of all US hospital discharges. As a result, NIS provides a more representative sample of the US patient population, making it 1 of the most comprehensive sources for examining the overall impact of the weekend effect in the US health care system. This study sets the stage for further exploration into TBAD repair outcomes in patients admitted on weekdays and weekends. It underscores the need for future research to use data sources that can capture more granular preoperative and intraoperative variables when comparing TBAD repair outcomes. Moreover, these future studies should also include patient follow-up data to evaluate long-term outcomes.
Conclusion
This research investigated the impact of weekend admission on outcomes following both open surgical repair and TEVAR for TBAD. Renal malperfusion was a common indication for TBAD repair. The study found that outcomes of open repair did not differ between patients admitted on weekdays vs weekends. However, in the case of TEVAR, weekend admissions were linked with a higher incidence of kidney failure, higher superficial wound infection, and longer time from admission to operation but lower respiratory complications. Addressing the delays associated with TEVAR procedures during weekend admissions may help reduce renal complications in TBAD. Striving to ensure prompt and efficient treatment, regardless of the day of admission, can help us achieve consistently high-quality patient care for all in TBAD repair.
Supplemental Material
Supplemental Material - Weekend Admission is Associated with Higher Kidney Failures after Thoracic Endovascular Aneurysm Repair for Stanford Type B Aortic Dissection
Supplemental Material for Weekend Admission is Associated with Higher Kidney Failures after Thoracic Endovascular Aneurysm Repair for Stanford Type B Aortic Dissection by Renxi Li, Qianyun Luo, Derrick Green, Stephen J. Huddleston in Vascular and Endovascular Surgery
Footnotes
Acknowledgments
The authors acknowledge Dr Richard Amdur, PhD, for giving statistical support for this project.
Author Contributions
conceptualization: R.L., Q.L.; methodology: R.L.; formal analysis: R.L.; investigation: R.L.; resources: R.L., D.G., S.H.; data curation: R.L.; writing (original draft): R.L., Q.L.; writing (review & editing): R.L., S.H., D.G., Q.L.; Supervision, S.H., D.G.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Patient Consent
This study was exempt from the IRB approval by The George Washington University as it analyzed retrospective, deidentified NIS data.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.